
Estimation of Life Expectancy for Dependent Population in a Multi-State Context


Abstract
1. Introduction
2. The Dependency in Spain
- Degree I. Moderate dependency: a person who needs help to perform various basic activities of daily living, at least once a day or periodically and/or limited support for his/her personal autonomy. People who were classified within this grade must have a score between 25 and 49.99 points.
- Degree II. Severe dependency: a person who needs help to perform various basic activities of daily living two or three times a day, but he/she does not need/want the permanent help from a caregiver or when he/she needs extensive support services for his/her personal autonomy. People who were classified within this grade must have a score between 50 and 74.99 points.
- Degree III. Major dependency: a person who needs help with various basic activities of daily living several times a day and/or needs continued assistance from another person due to his/her total loss of physical, mental, intellectual, or sensorial autonomy. People who were classified within this grade must have a score between 75 and 100 points.
3. Data
- Spanish Social Security life table for retired persons who receive a permanent annuity for disability. They were published in the State Official Gazette of 28 December 2005. This table provides information on the entire population with permanent disability, whether or not they are dependents. This table is elaborated for ages between 16 and 108 years old, both included. From now on, they are identified as .
- Life table for the general population. The PERM/F table for the year 2000 was used for this purpose, with particular reference to the year 2008. There is a life table for men and another for women. However, there is not a table for the whole population.
- Spanish population structure by age and sex in 2008. This information was taken from the INE.
- National Survey on Disability, Personal Autonomy, and Dependency (EDAD database: Encuesta sobre, Discapacidad, Autonomía personal y Situaciones de Dependencia), conducted by the Spanish National Institute of Statistics (INE) in 2008 in collaboration with the IMSERSO (Institute for the Elderly and Social Services) and the ONCE (Spanish National Organisation for Blind people). Two-stage, stratified sampling proportional to the size of each Autonomous Community was used. It collects information from more than 260,000 people living at home plus 11,000 in residential homes. Each of the 271,000 participants in the survey represents a certain number of people. This number is captured in what is called the elevation factor, so that the sum of all the factors equals the total Spanish population at the time of the survey. The interviews were carried out both with the people affected and with their relatives and/or carers. Self-perceived disability is the core concept of EDAD. It is captured by means of a set of questions that allow the assessment of possible difficulties in performing activities of daily living (hereafter ADLs). EDAD is one of the largest national survey studies on the topics of health, disability, and care in Europe. Although the name of EDAD 2008 refers to Dependency, the registers included therein only collect information on all of the disabilities included in the ICF 2001 classification (International Classification of Functioning, Disability and Health). The change from data referring to disability to other data referring to dependency was carried out considering the requirements of the current legislation in Spain. An explanation of the process followed can be found in [35].
4. Steps in the Estimation Process
- as the probabilities of death are known for each age by sex but not for the whole population at each age, the first step is to estimate what the probability of death is for each age from the information contained in the life tables for each sex. This was done by calculating a weighted average probability of death estimated for each age, , no matter what the sex of the individual. For this purpose, the set of from the life tables of the general population for each sex are used, that is, and (from now on, the superscripts M and F refer to male and female, respectively. As it was indicated in Section 3, the PERM/F-2000 tables are elaborated by sex but not for the whole population). In addition to these probabilities for each age, weighting factors are required. They are identified as and . They are obtained from the structure figures of the general population in 2008 by age and sex, so that: where is the total of the population with age x and belonging to sex i and is the total population with age x, whatever their sex were. So, the average is obtained as:
- the death probability for each sex at each age in general population, is then compared with the estimated average probability at that age. This provides a measure of the divergence between sex-specific and overall mortality for each age. This difference will be captured in a coefficient, called , calculated as follows:It must be said that the coefficients change with age and that there are two coefficients per each age.
- finally, once the former coefficients were calculated, the probabilities of death of the permanently disabled population are estimated for each sex as follows:
- the estimated survival probabilities are obtained using this set of as . Then, the values for can be obtained as . The profiles can be seen in Figure 1:
- A1: this ratio is equal to when the scale B is equal to the average, i.e., . This case is denoted as .
- A2: this ratio tends to unity in the case where there is no dependence ().
- A3: this ratio is assumed to be less than unity. In the absence of statistical information, 10 values are assumed, denoted henceforth as k, from 0.8 to 0.98, with steps of 0.02.
- A4: finally, the definitive reduction depends both on the scale for each degree and on age, so that the higher the scale, and therefore the more intense the dependency, the greater the reduction in the probability of survival.
- . In this case, the two extreme situations occur when B values are and 100. As it was previously indicated when the scale is equal to the average, then r is equal to . From this point, the ratio decreases as the scale increases until it becomes equal to when the scale reaches 100 points. Therefore, when the scale reaches that maximum point, the largest variation of the scale and then, , it follows that . So, for any change equal to , it follows that . According to this, the final ratio, , is equal to , that is:
- . In this case, the two extreme situations occur when B values are 0 and . In the first case there is no dependence. We call the ratio in this case and its definition is explained later. Therefore, as B increases from 0 to , the ratio goes from to . Therefore, for any value of B between these two extremes, changes in r is equal to , so that the final ratio, , is equal to . The value of remains to be determined. This ratio is associated with a situation without dependence. This would make it equal to unity. However, to consider the different scenarios of intensity of this contingency, the effect of assuming different scenarios of intensity in the loss of survival in this group was subtracted from this unit value, so that the value taken for is . The first bracket refers to the loss associated with suffering this contingency, whereas the second one reflects the intensity of the loss.
- the final probability of passing from state i to j at age x and still being alive at , , is equal to where refers to the probability of being alive at age x.
- the final probability of passing from state i at age x to be dead at age , is obtained as
- as there is no improvement in the state of the dependency suffered then .
- finally and obviously, .
- firstly, the matrix is obtained for the age of 50 years old, and a given scenario k, is taken as the origin of the process
- assuming that the transition matrices for each age are reflecting Markov homogeneous chains, then:These are the matrices used to estimate the needed to obtain the life expectancies.
- for each age, degree, sex, and scenario, the are obtained as the horizontal sum in the matrices of the probabilities of passing from a certain state to a state other than death.
- finally, the life expectancies at a certain degree, age, scenario, and sex are obtained as:
5. Results
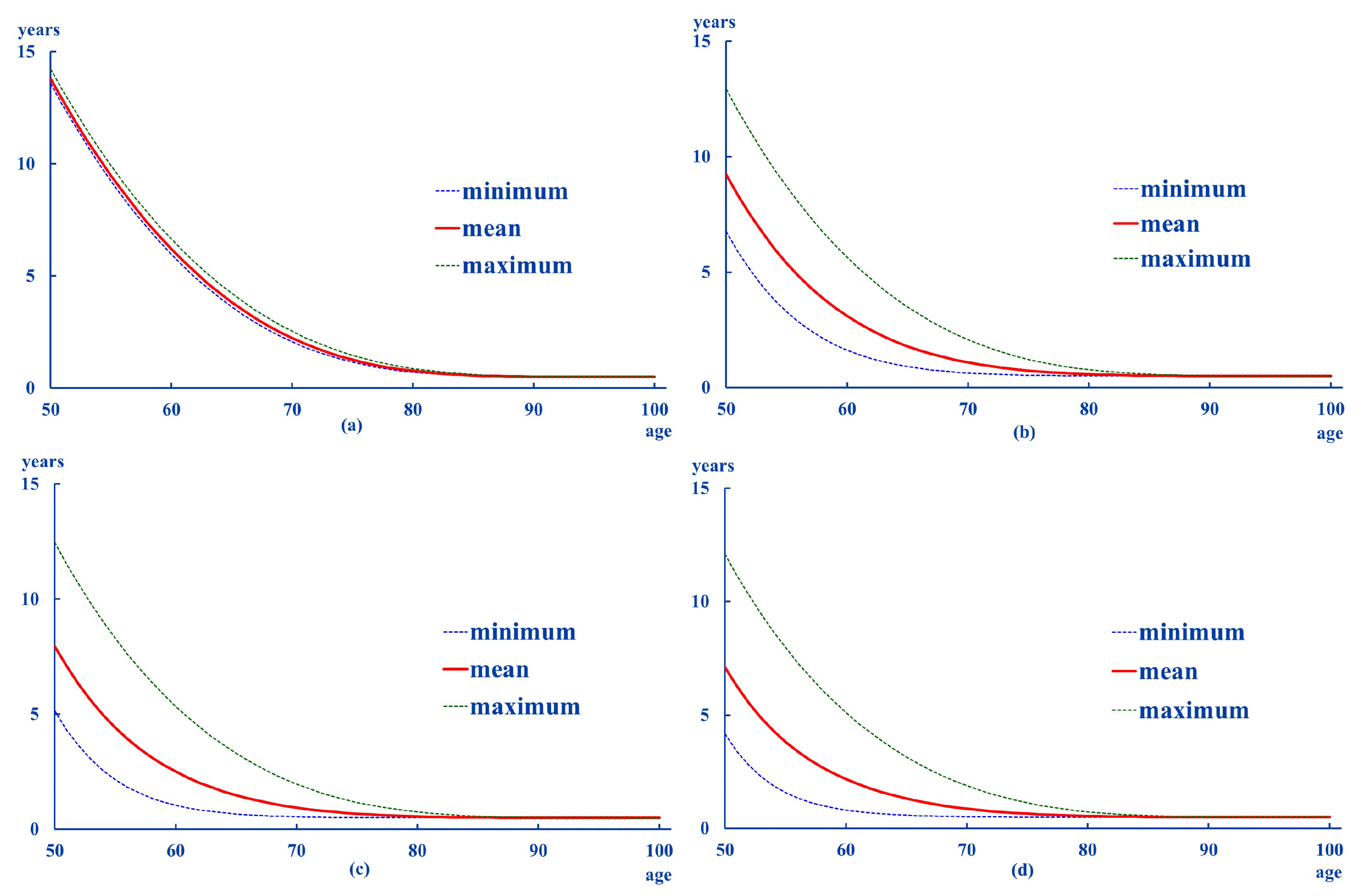
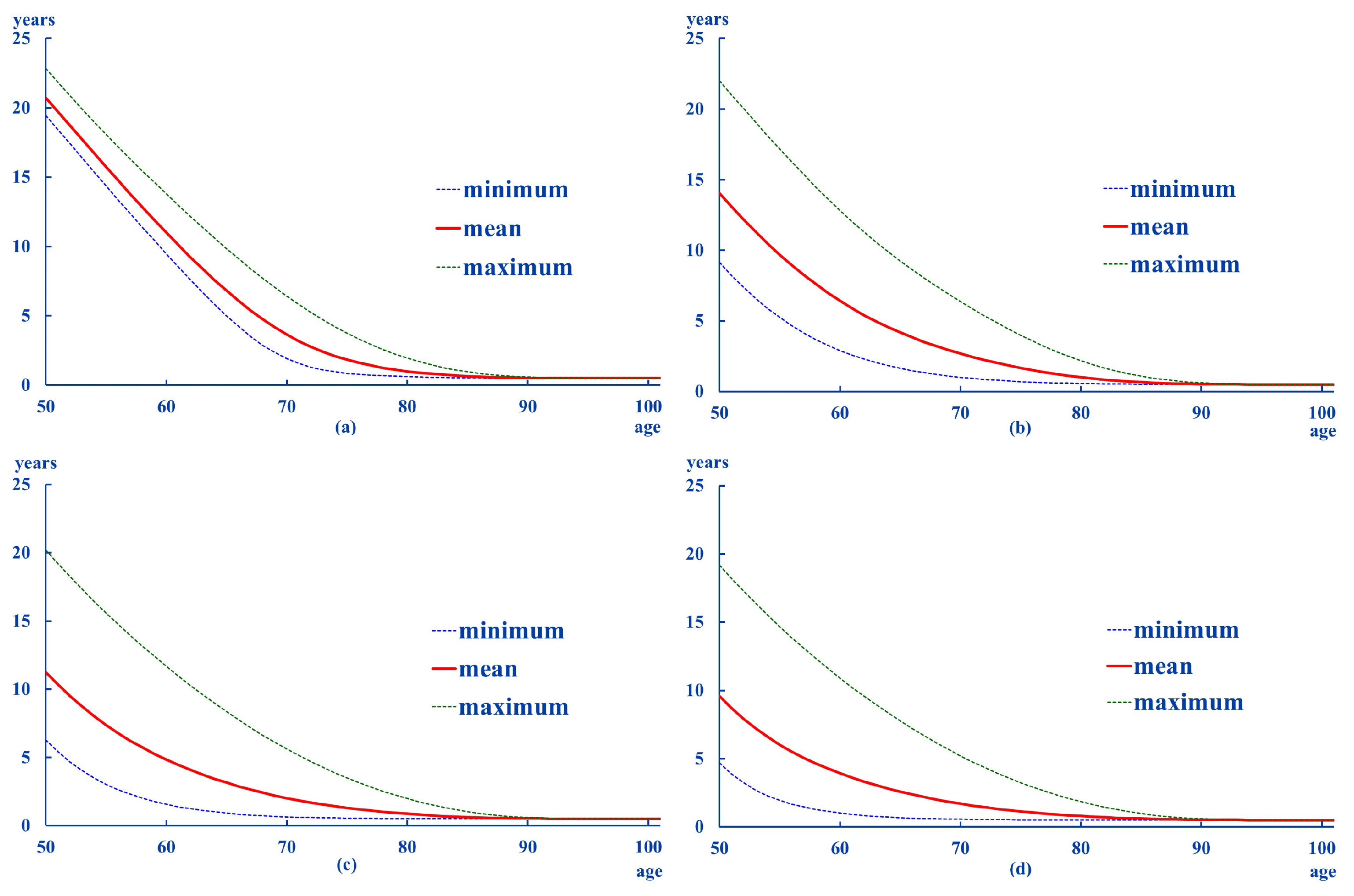
- average life expectancies are higher in women than in men, as it happens in the general population.
- except for Degree 0, the age at which the is less than one year of life is 8 to 10 years higher in women than in men. This difference becomes smaller as the intensity of dependency increases.
- the distances from the mean to the extremes are larger for women than for men. This pattern is also registered in the standard deviations of these differences.
- in general, the results suggest greater and more dispersed distances in the high ranges (maximum–average).
- low degrees (0 and 1) show a relative stability in the transition probabilities, whatever the age considered. As for the probabilities associated with Degree II, there is a transfer to Degree III. This pattern can be seen in all the ages analyzed in women, whereas it can be seen from the age of 60 onwards in men.
- according to these results, it is most likely to remain at the Degree they were at the initial age. This pattern is more likely in men beginning in Degrees I and II. However, if their situation worsens, it is most likely to end at Degree III. This is more likely in women beginning in Degree II.
6. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. Word Population Prospects; Technical Report; United Nations, Department of Economics and Social Affairs: New York, NY, USA, 2019. [Google Scholar]
- Leeson, G. The importance of Demography. Popul. Ageing 2011, 4, 1–4. [Google Scholar] [CrossRef]
- Vaupel, J.; Kohler, H. Demography and its relation to other disciplines. In Position of Demography among Other Disciplines; Pavlic, Z., Ed.; Department of Demography and Geodemography, Charles University in Prague, Faculty of Sciences: Prague, Czech Republic, 2000; pp. 19–26. [Google Scholar]
- Wachter, K. The past, Present and Future of Demography and the role of the Max Planck Institute of Demography. Demogr. Res. 2003, 9, 69–80. [Google Scholar] [CrossRef]
- Kovacheva, P. Life tables—Key parameters and relationships between them. Int. Math. Forum 2017, 12, 469–479. [Google Scholar] [CrossRef]
- Fried, L.; Tangen, C.; Walston, J.; Newman, A.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med Sci. 2001, 56, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.; Rockwood, K. Frailty in eldely people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Swiss Re. Long Term Care Data Pack; Technical Report; Swiss Re: London, UK, 1999. [Google Scholar]
- Fries, J. Aging, natural death and the compression of morbidity. N. Engl. J. Med. 1980, 303, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Manton, K. Changing concepts of morbidity and mortality in the elderly population. Milbank Meml. Found. Q. Health Soc. 1982, 62, 183–244. [Google Scholar] [CrossRef]
- Gruenberg, E. The failure of success. Milbank Meml. Found. Q. Health Soc. 1977, 55, 3–24. [Google Scholar] [CrossRef]
- Kramer, J. The rising pandemic of mental disorders and associated chronic diseases and disabilities. Acta Psychiatr. Scaninavica 1980, 62, 382–397. [Google Scholar] [CrossRef]
- Karlsson, N.; Carstensen, J.; Gjesdal, S.; Alexanderson, K. Mortality in relation to disability pension: Findings from a12-year prospective population-based cohort study in Sweden. Scand. J. Public Health 2007, 35, 341–347. [Google Scholar] [CrossRef]
- Majer, I.; Nusselder, W.; Mackenbach, J.; Klijs, B.; van Baal, P. Mortality risk associated with disability: A population-based record linkage study. Am. J. Public Health 2011, 101, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Lauer, E.; McCallion, P. Mortality of People with Intellectual and Developmental Disabilities from Select US State Disability Service Systems and Medical Claims Data. J. Appl. Res. Intellect. Disabil. 2015, 28, 394–405. [Google Scholar] [CrossRef]
- Park, J.M.; Oh, U.; Roh, B.R.; Moon, Y. Disparities in mortality by disability: An 11-year follow-up study of 1 million individuals. Int. J. Public Health 2017, 62, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Llibre, J.; López, A.; Valhuerdi, A.; Guerra, M.; Llibre-Guerra, J.; Sánchez, Y.; Bosch, R.; Zayas, T.; Moreno, C. Frailty, Dependency and Mortality Predictors in a Cohort of Cuban Older Adults. Medicc Rev. 2014, 16, 24–30. [Google Scholar]
- Nakazawa, A.; Nakamura, K.; Kitamura, K.; Yoshizawa, Y. Association between activities of daily living and mortality among institutionalized elderly adults in Japan. J. Epidemiol. 2012, 22, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Hong, G. Predictive Factors of Mortality in Older Adult Residents of Long-Term Care Facilities. J. Nurs. Res. 2020, 28, e82. [Google Scholar] [CrossRef]
- Lopes, H.; Mateus, C.; Rosati, N. Impact of long term care and mortality risk in community care and nursing homes population. Arch. Gerontol. Geriatr. 2018, 76, 160–168. [Google Scholar] [CrossRef]
- Crimmins, E.; Hayward, M.; Saito, Y. Changing mortality and the morbidity rate and the health status and the life expectancy of the older population. Demography 1994, 31, 159–175. [Google Scholar] [CrossRef]
- Crimmins, E.; Hayward, M.; Saito, Y. Differentials in active life expectancy in the older population of the United States. J. Gerontol. Ser. B 1996, 51, 111–120. [Google Scholar] [CrossRef]
- Crimmins, E.; Hayward, M.; Hagedron, A.; Saito, Y.; Brouard, N. Change in disability free life expectancy for Americans 70 years old and older. Demography 2009, 46, 627–646. [Google Scholar] [CrossRef]
- Crimmins, E. Trends in the health of the elderly. Annu. Rev. Public Health 2004, 25, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Cruz, S.; Saito, Y.; Natividad, J. Active Life Expectancy and Functional Health Transition among Filipino Older People. Can. Stud. Popul. 2007, 34, 29–47. [Google Scholar] [CrossRef][Green Version]
- Haberman, S.; Pitacco, E. Actuarial Models for Disability Insurance; Chapman and Hall: London, UK; Cambridge University Press: Boca Ratón, FL, USA, 1999. [Google Scholar]
- Olivieri, A.; Ferri, S. Rischi demografici nelle assicurazioni Long Term Care. Diritto ed Economia dell’Assicurazione 2002, 3-4, 583–610. [Google Scholar]
- Martikäinen, P.; Moustgaard, H.; Einiö, E.; Murphy, M. Life Expectancy in Long-Term Institutional Care by Marital Status: Multistate Life Table Estimates for Older Finnish Men and Women. J. Gerontol. Ser. B 2013, 62, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Balasubramaniyan, S.; Mohananchandran, N. Changes in Health Expectancies: A Multi State Lifetable Model. Demogr. India 2015, 44, 119–135. [Google Scholar]
- Gobbens, R.; van der Ploeg, T. The Prediction of Mortality by Disability Among Dutch Community-Dwelling Older People. Clin. Interv. Ageing 2020, 15, 1897–1906. [Google Scholar] [CrossRef]
- Aspell, N.; O’Sullivan, M.; O’Shea, E.; Irving, K.; Duffy, C.; Gorman, R.; Warters, A. Predicting admission to long-term care and mortality among community-based, dependent older people in Ireland. Int. J. Geriatr. Psychiatry 2019, 34, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Millán-Calenti, J.; Tubío, J.; Pita-Fernández, S.; González-Abraldes, I.; Lorenzo, T.; Fernández-Arruty, T.; Maseda, A. Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch. Gerontol. Geriatr. 2010, 50, 306–310. [Google Scholar] [CrossRef]
- Albarrán, I.; Alonso, P.; Bolancé, C. Comparación de los baremos español, francés y alemán para medir la dependencia de las personas con discapacidad y sus prestaciones. Rev. Espa Nola Salud Pública 2009, 83, 379–392. [Google Scholar] [CrossRef][Green Version]
- Zueras, P.; Rentería, E. Trends in disease-free life expectancy at age 65 in Spain: Diverging patterns by sex, region and disease. PLoS ONE 2020, 15, e0240923. [Google Scholar] [CrossRef]
- Albarrán, I.; Alonso, P. La población dependiente en España: Estimación del número y del coste asociado a su cuidado. Estud. Econ. 2009, 36, 127–163. [Google Scholar] [CrossRef]
- Albarrán, I.; Alonso-González, P.; Grané, A. Long term care insurance pricing in Spanish population: A functional data approach. Eur. J. Financ. 2020, 26, 258–276. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean-Minimum | Maximum-Mean | |||||
|---|---|---|---|---|---|---|
| Mean | x for e < 1 | Mean | Standard Deviation | Mean | Standard Deviation | |
| Degree 0 | 3.29 | 77 | 0.11 | 0.10 | 0.21 | 0.18 |
| Degree I | 1.93 | 70 | 0.64 | 0.82 | 1.11 | 1.28 |
| Degree II | 1.65 | 69 | 0.66 | 0.89 | 1.25 | 1.51 |
| Degree III | 1.48 | 68 | 0.64 | 0.90 | 1.31 | 1.62 |
| Mean-Minimum | Maximum-Mean | |||||
|---|---|---|---|---|---|---|
| Mean | x for e < 1 | Mean | Standard Deviation | Mean | Standard Deviation | |
| Degree 0 | 5.02 | 79 | 0.81 | 0.72 | 1.43 | 1.19 |
| Degree I | 3.33 | 80 | 1.55 | 1.70 | 2.91 | 2.88 |
| Degree II | 2.60 | 78 | 1.43 | 1.66 | 3.05 | 3.15 |
| Degree III | 2.19 | 76 | 1.30 | 1.57 | 3.12 | 3.31 |
| x = 50 | x = 60 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| D 0 | D I | D II | D III | D 0 | D I | D II | D III | ||
| D 0 | 0.56 | 0.00 | 0.14 | 0.29 | D 0 | 0.56 | 0.00 | 0.15 | 0.29 |
| D I | 0.00 | 0.56 | 0.13 | 0.31 | D I | 0.00 | 0.57 | 0.12 | 0.31 |
| D II | 0.00 | 0.00 | 0.78 | 0.22 | D II | 0.00 | 0.00 | 0.80 | 0.20 |
| D III | 0.00 | 0.00 | 0.00 | 1.00 | D III | 0.00 | 0.00 | 0.00 | 1.00 |
| x = 70 | x = 80 | ||||||||
| D 0 | D I | D II | D III | D 0 | D I | D II | D III | ||
| D 0 | 0.55 | 0.01 | 0.15 | 0.30 | D 0 | 0.52 | 0.02 | 0.15 | 0.31 |
| D I | 0.00 | 0.53 | 0.14 | 0.33 | D I | 0.00 | 0.52 | 0.14 | 0.34 |
| D II | 0.00 | 0.00 | 0.71 | 0.29 | D II | 0.00 | 0.00 | 0.69 | 0.31 |
| D III | 0.00 | 0.00 | 0.00 | 1.00 | D III | 0.00 | 0.00 | 0.00 | 1.00 |
| x = 50 | x = 60 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| D 0 | D I | D II | D III | D 0 | D I | D II | D III | ||
| D 0 | 0.68 | 0.04 | 0.12 | 0.16 | D 0 | 0.67 | 0.04 | 0.12 | 0.16 |
| D I | 0.00 | 0.48 | 0.18 | 0.34 | D I | 0.00 | 0.49 | 0.19 | 0.33 |
| D II | 0.00 | 0.00 | 0.60 | 0.40 | D II | 0.00 | 0.00 | 0.59 | 0.41 |
| D III | 0.00 | 0.00 | 0.00 | 1.00 | D III | 0.00 | 0.00 | 0.00 | 1.00 |
| x = 70 | x = 80 | ||||||||
| D 0 | D I | D II | D III | D 0 | D I | D II | D III | ||
| D 0 | 0.66 | 0.05 | 0.12 | 0.17 | D 0 | 0.63 | 0.05 | 0.12 | 0.19 |
| D I | 0.00 | 0.47 | 0.18 | 0.35 | D I | 0.00 | 0.43 | 0.18 | 0.39 |
| D II | 0.00 | 0.00 | 0.58 | 0.42 | D II | 0.00 | 0.00 | 0.54 | 0.46 |
| D III | 0.00 | 0.00 | 0.00 | 1.00 | D III | 0.00 | 0.00 | 0.00 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albarrán Lozano, I.; Alonso-González, P.J.; Núñez-Velázquez, J.J. Estimation of Life Expectancy for Dependent Population in a Multi-State Context. Int. J. Environ. Res. Public Health 2021, 18, 11162. https://doi.org/10.3390/ijerph182111162
Albarrán Lozano I, Alonso-González PJ, Núñez-Velázquez JJ. Estimation of Life Expectancy for Dependent Population in a Multi-State Context. International Journal of Environmental Research and Public Health. 2021; 18(21):11162. https://doi.org/10.3390/ijerph182111162
Chicago/Turabian StyleAlbarrán Lozano, Irene, Pablo J. Alonso-González, and José Javier Núñez-Velázquez. 2021. "Estimation of Life Expectancy for Dependent Population in a Multi-State Context" International Journal of Environmental Research and Public Health 18, no. 21: 11162. https://doi.org/10.3390/ijerph182111162
APA StyleAlbarrán Lozano, I., Alonso-González, P. J., & Núñez-Velázquez, J. J. (2021). Estimation of Life Expectancy for Dependent Population in a Multi-State Context. International Journal of Environmental Research and Public Health, 18(21), 11162. https://doi.org/10.3390/ijerph182111162