
Contextual Determinants of General Household Hygiene Conditions in Rural Indonesia


Abstract
:1. Introduction
2. Materials and Methods
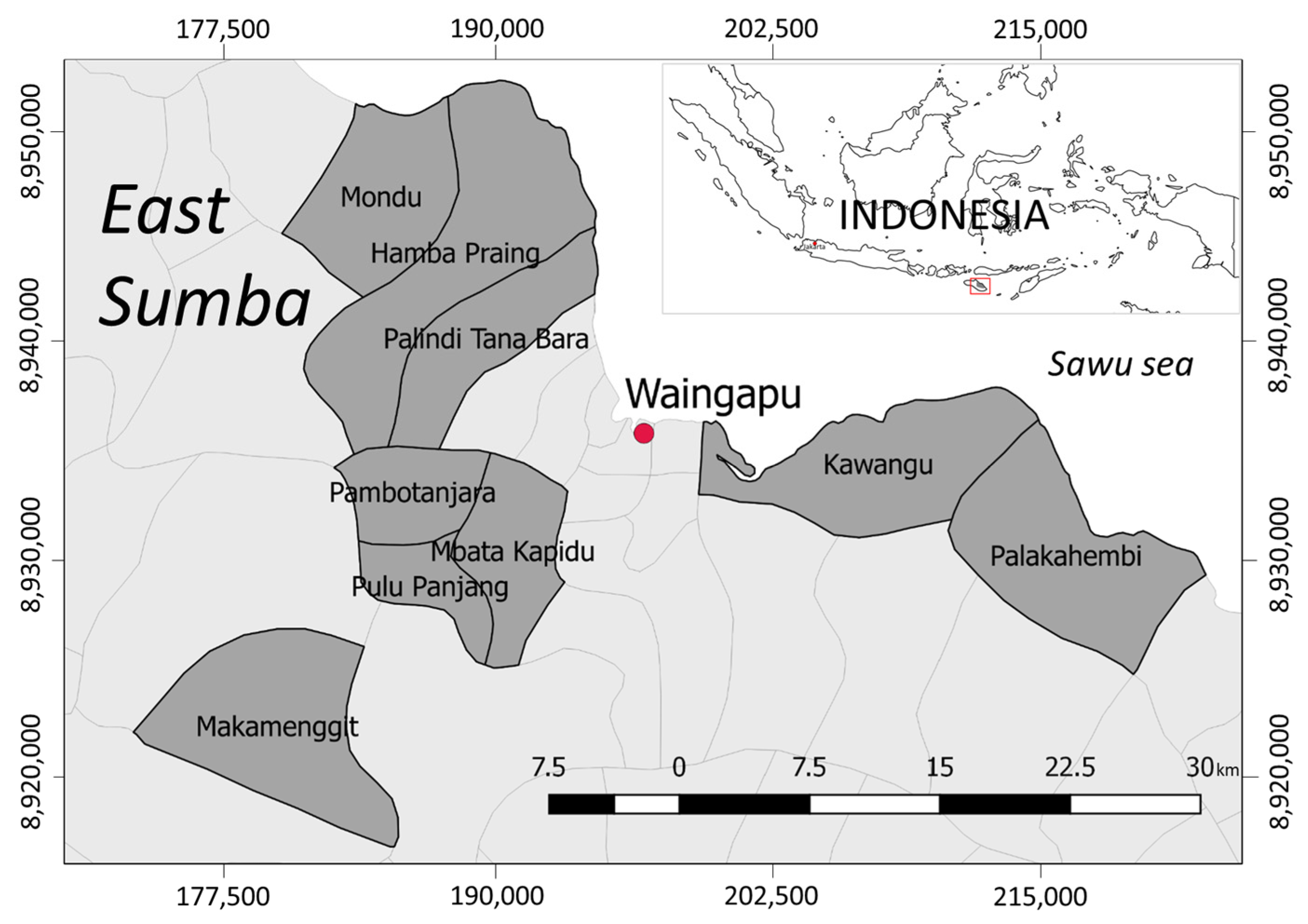
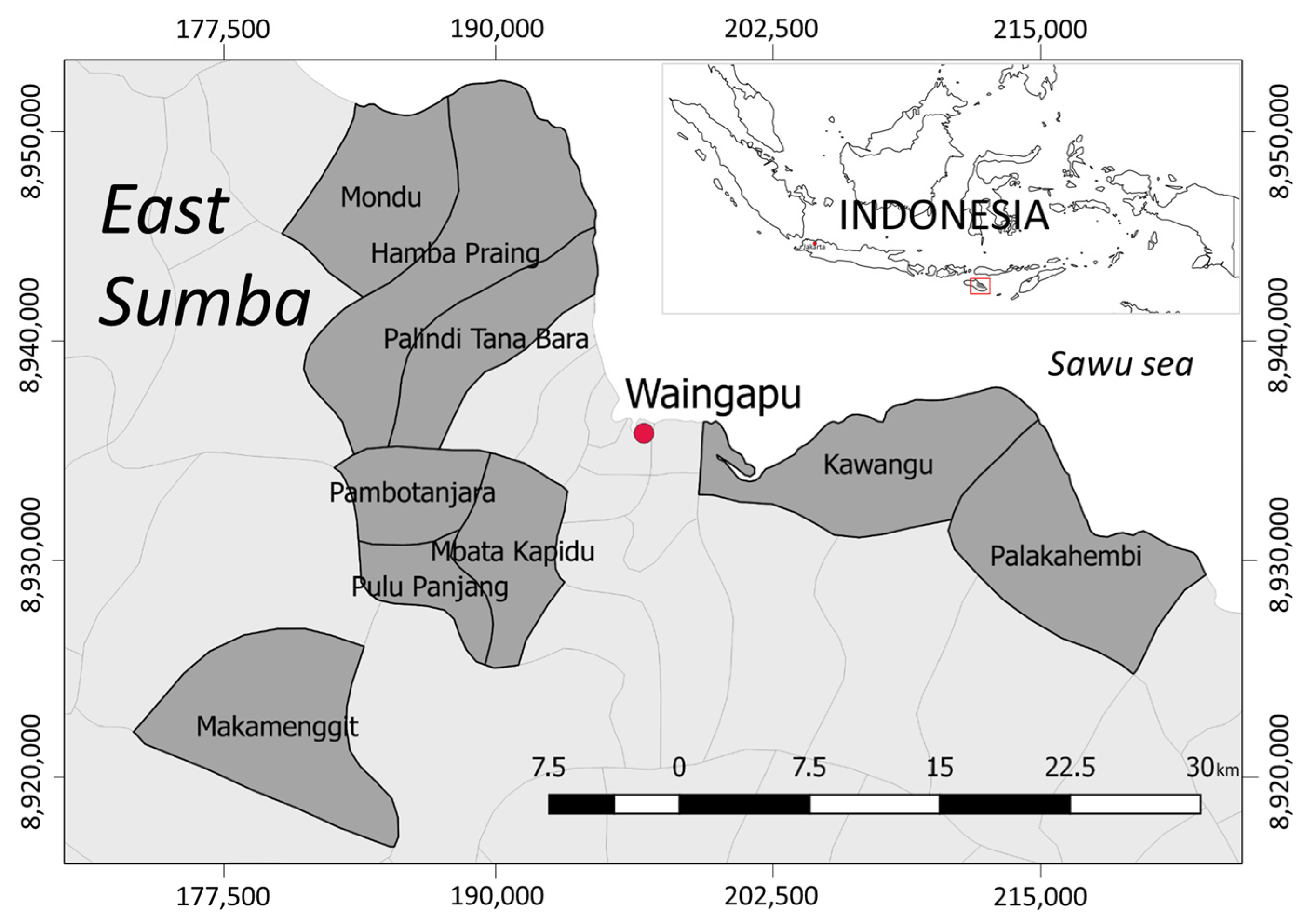
2.1. Data Collection
2.2. Contextual Determinant Variables of Household Hygiene Conditions
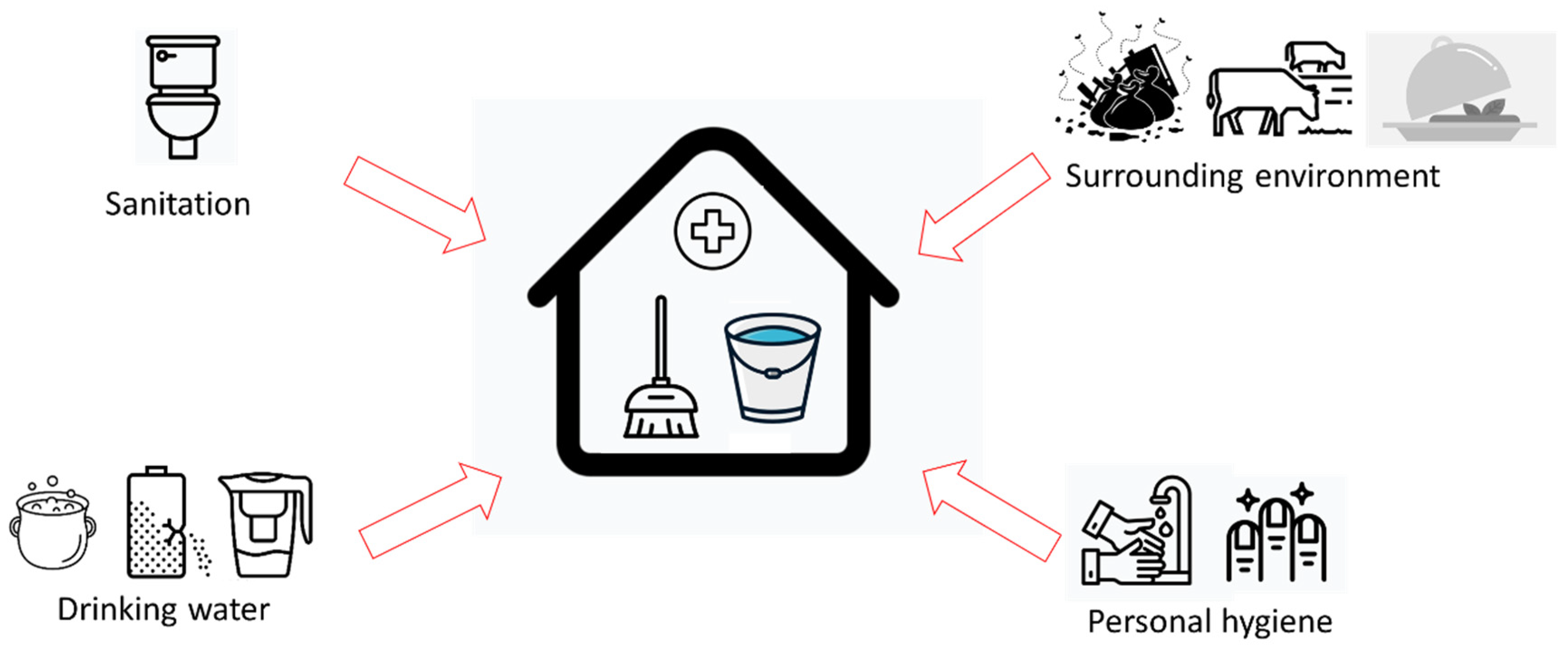
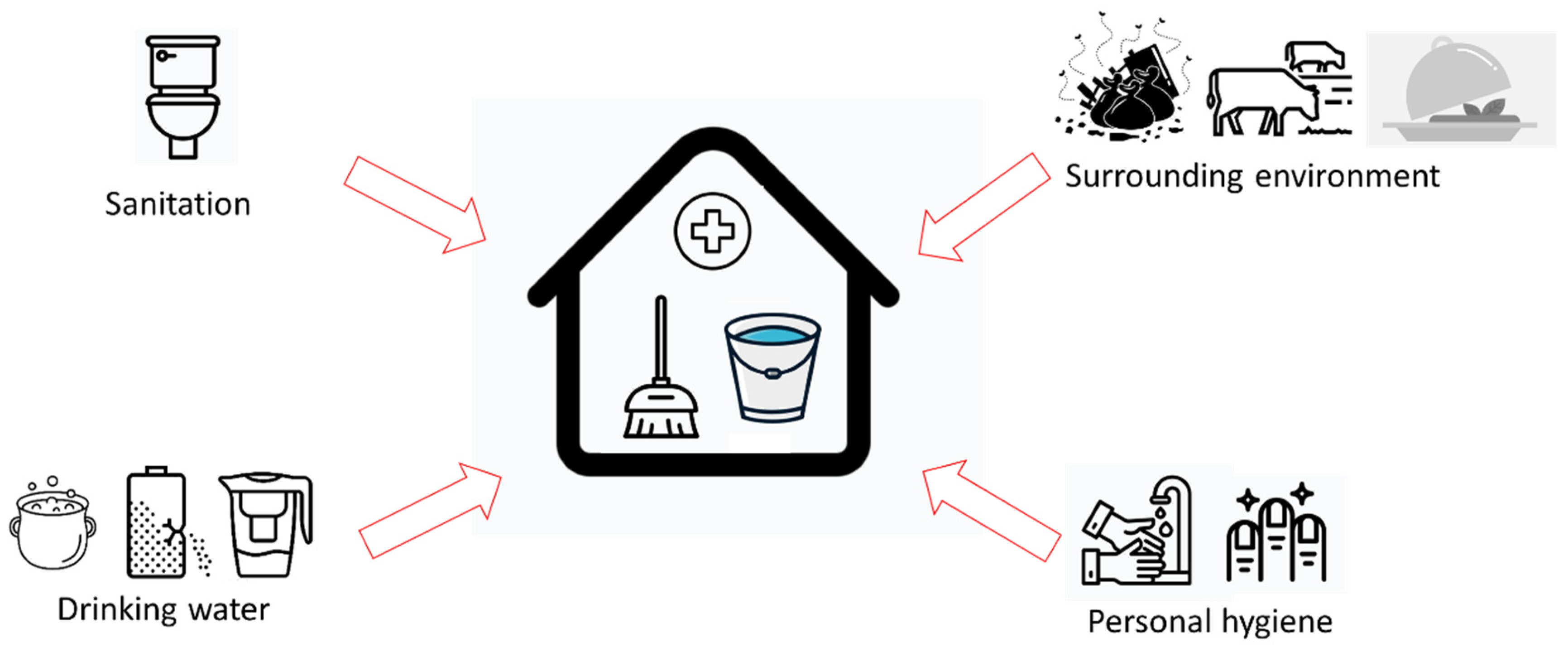
2.3. Hygiene-Related Variables
2.4. Data Analysis
3. Results
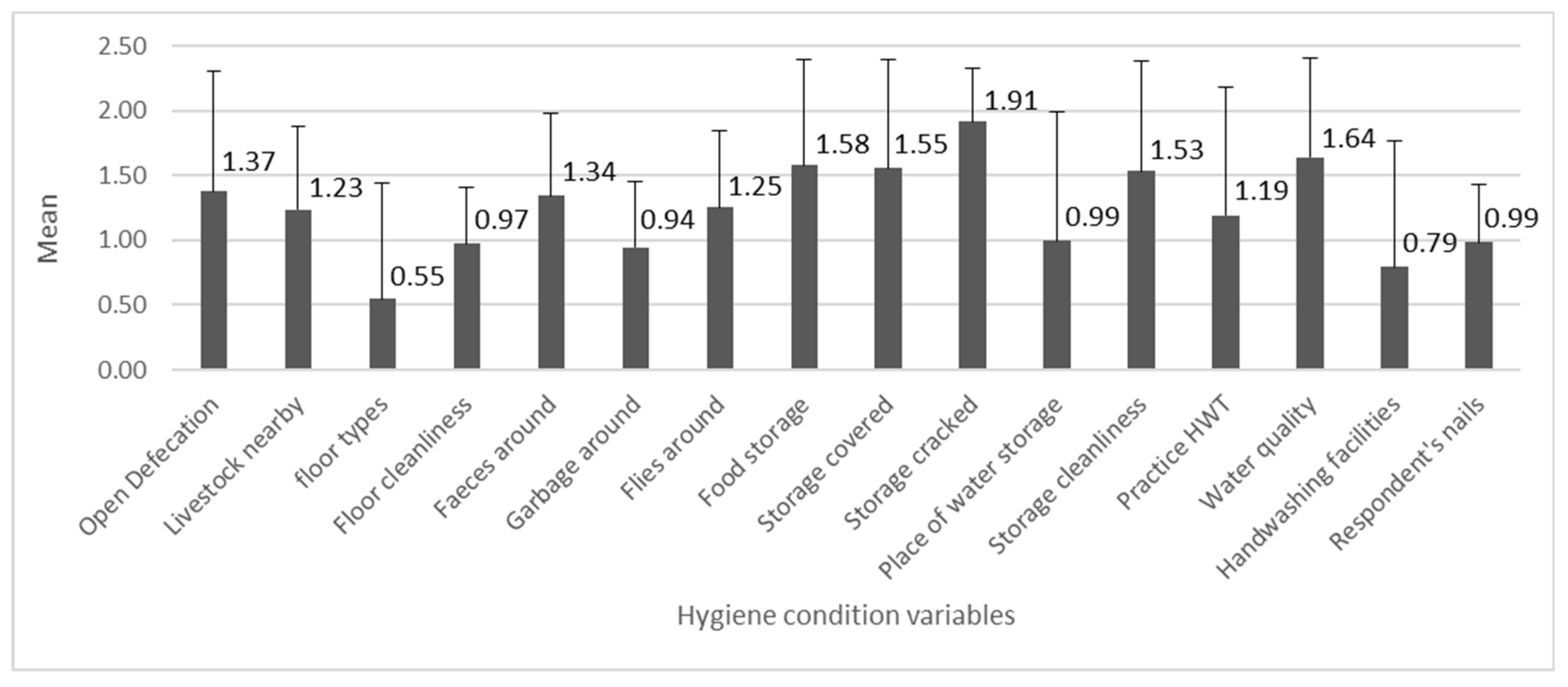
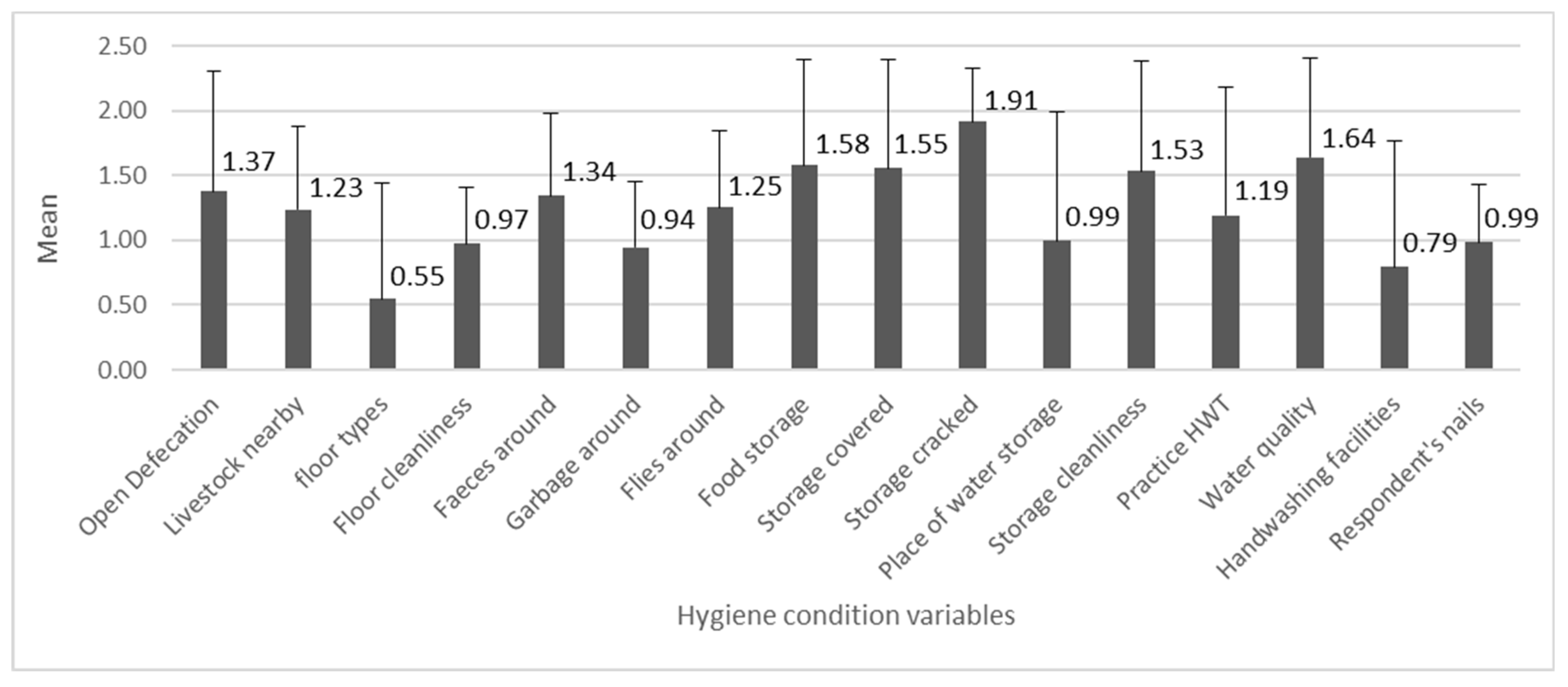
3.1. Descriptive Statistics
3.2. Hygiene Conditions and the Determinants
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wolf, J.; Hunter, P.R.; Freeman, M.C.; Cumming, O.; Clasen, T.; Bartram, J.; Higgins, J.P.T.; Johnston, R.; Medlicott, K.; Boisson, S.; et al. Impact of drinking water, sanitation and handwashing with soap on childhood diarrhoeal disease: Updated meta-analysis and meta-regression. Trop. Med. Int. Health 2018, 23, 508–525. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.C.; Stocks, M.E.; Cumming, O.; Jeandron, A.; Higgins, J.; Wolf, J.; Prüss-Ustün, A.; Bonjour, S.; Hunter, P.; Fewtrell, L.; et al. Systematic review: Hygiene and health: Systematic review of handwashing practices worldwide and update of health effects. Trop. Med. Int. Health 2014, 19, 906–916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cairncross, S.; Hunt, C.; Boisson, S.; Bostoen, K.; Curtis, V.; Fung, I.C.-H.; Schmidt, W.-P. Water, sanitation and hygiene for the prevention of diarrhoea. Int. J. Epidemiol. 2010, 39, i193–i205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cumming, O.; Cairncross, S. Can water, sanitation and hygiene help eliminate stunting? Current evidence and policy implications. Matern. Child Nutr. 2016, 12, 91–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniel, D.; Iswarani, W.P.; Pande, S.; Rietveld, L. A Bayesian Belief Network model to link sanitary inspection data to drinking water quality in a medium resource setting in rural Indonesia. Sci. Rep. 2020, 10, 18867. [Google Scholar] [CrossRef] [PubMed]
- Gundry, S.; Wright, J.; Conroy, R. A systematic review of the health outcomes related to household water quality in developing countries. J. Water Health 2004, 2, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Water Safety Planning for Small Community Water Supplies: Step-by-Step Risk Management Guidance for Drinking-Water Supplies in Small Communities; WHO: Geneva, Switzerland, 2012; Available online: http://www.who.int/iris/handle/10665/75145 (accessed on 16 July 2021). [CrossRef] [PubMed] [Green Version]
- Ercumen, A.; Mertens, A.; Arnold, B.F.; Benjamin-Chung, J.; Hubbard, A.E.; Ahmed, M.A.; Kabir, M.H.; Khalil, M.R.; Kumar, A.; Rahman, S.; et al. Effects of Single and Combined Water, Sanitation and Handwashing Interventions on Fecal Contamination in the Domestic Environment: A Cluster-Randomized Controlled Trial in Rural Bangladesh. Environ. Sci. Technol. 2018, 52, 12078–12088. [Google Scholar] [CrossRef]
- Kelly, E.R.; Cronk, R.; Kumpel, E.; Howard, G.; Bartram, J. How we assess water safety: A critical review of sanitary inspection and water quality analysis. Sci. Total Environ. 2020, 718, 137237. [Google Scholar] [CrossRef]
- WHO. Surveillance and Control of Community Supplies, Guidelines for Drinking-Water Quality, 2nd ed.; WHO: Geneva, Switzerland, 1997. [Google Scholar] [CrossRef]
- Daniel, D.; Gaicugi, J.; King, R.; Marks, S.J.; Ferrero, G. Combining Sanitary Inspection and Water Quality Data in Western Uganda: Lessons Learned from a Field Trial of Original and Revised Sanitary Inspection Forms. Resources 2020, 9, 150. [Google Scholar] [CrossRef]
- Sonego, I.L.; Mosler, H.-J. Spot-checks to measure general hygiene practice. Int. J. Environ. Health Res. 2016, 26, 554–571. [Google Scholar] [CrossRef]
- Agustina, R.; Sari, T.P.; Satroamidjojo, S.; Bovee-Oudenhoven, I.M.; Feskens, E.J.; Kok, F.J. Association of food-hygiene practices and diarrhea prevalence among Indonesian young children from low socioeconomic urban areas. BMC Public Health 2013, 13, 977. [Google Scholar] [CrossRef] [Green Version]
- Daniel, D.; Diener, A.; Van De Vossenberg, J.; Bhatta, M.; Marks, S.J. Assessing Drinking Water Quality at the Point of Collection and within Household Storage Containers in the Hilly Rural Areas of Mid and Far-Western Nepal. Int. J. Environ. Res. Public Health 2020, 17, 2172. [Google Scholar] [CrossRef] [Green Version]
- Marjadi, B.; McLaws, M.-L. Hand hygiene in rural Indonesian healthcare workers: Barriers beyond sinks, hand rubs and in-service training. J. Hosp. Infect. 2010, 76, 256–260. [Google Scholar] [CrossRef]
- Hirai, M.; Graham, J.P.; Mattson, K.D.; Kelsey, A.; Mukherji, S.; Cronin, A.A. Exploring Determinants of Handwashing with Soap in Indonesia: A Quantitative Analysis. Int. J. Environ. Res. Public Health 2016, 13, 868. [Google Scholar] [CrossRef] [Green Version]
- Dwipayanti, N.M.U.; Lubis, D.S.; Harjana, N.P.A. Public Perception and Hand Hygiene Behavior during COVID-19 Pandemic in Indonesia. Front. Public Health 2021, 9, 621800. [Google Scholar] [CrossRef]
- Akombi, B.J.; Agho, K.E.; Hall, J.J.; Wali, N.; Renzaho, A.; Merom, D. Stunting, wasting and underweight in Sub-Saharan Africa: A systematic review. Int. J. Environ. Res. Public Health 2017, 14, 863. Available online: https://www.mdpi.com/1660-4601/14/8/863/pdf (accessed on 16 July 2021). [CrossRef] [PubMed] [Green Version]
- Torlesse, H.; Cronin, A.A.; Sebayang, S.K.; Nandy, R. Determinants of stunting in Indonesian children: Evidence from a cross-sectional survey indicate a prominent role for the water, sanitation and hygiene sector in stunting reduction. BMC Public Health 2016, 16, 669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beal, T.; Tumilowicz, A.; Sutrisna, A.; Izwardy, D.; Neufeld, L.M. A review of child stunting determinants in Indonesia. Matern. Child Nutr. 2018, 14, e12617. [Google Scholar] [CrossRef] [PubMed]
- Rachmi, C.N.; Agho, K.E.; Li, M.; Baur, L. Stunting, Underweight and Overweight in Children Aged 2.0–4.9 Years in Indonesia: Prevalence Trends and Associated Risk Factors. PLoS ONE 2016, 11, e0154756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irianti, S.; Prasetyoputra, P. Rural–Urban Disparities in Access to Improved Sanitation in Indonesia: A Decomposition Approach. SAGE Open 2021, 11. [Google Scholar] [CrossRef]
- Irianti, S.; Prasetyoputra, P.; Sasimartoyo, T.P. Determinants of household drinking-water source in Indonesia: An analysis of the 2007 Indonesian family life survey. Cogent Med. 2016, 3, 1151143. [Google Scholar] [CrossRef]
- Patunru, A.A. Access to Safe Drinking Water and Sanitation in Indonesia. Asia Pac. Policy Stud. 2015, 2, 234–244. [Google Scholar] [CrossRef]
- Braveman, P.; Gottlieb, L. The Social Determinants of Health: It’s Time to Consider the Causes of the Causes. Public Health Rep. 2002, 129, 19–31. [Google Scholar] [CrossRef] [Green Version]
- Mosler, H.; Contzen, N. Systematic Behavior Change in Water Sanitation and Hygiene. A Practical Guide Using the RANAS Approach. Version 1.1. 2016, p. 99. Available online: https://research.rug.nl/en/publications/systematic-behavior-change-in-water-sanitation-and-hygiene-a-prac (accessed on 16 July 2021).
- Fitzpatrick, C.; Engels, D. Leaving no one behind: A neglected tropical disease indicator and tracers for the Sustainable Development Goals: Box 1. Int. Health 2016, 8, i15–i18. [Google Scholar] [CrossRef] [Green Version]
- Statistics of Sumba Timur Regency. Persentase Rumah Tangga Menurut Fasilitas Tempat Buang Air Besar (Persen), 2015–2017. Statistics of Sumba Timur Regency. 2018. Available online: https://sumbatimurkab.bps.go.id/indicator/154/84/1/persentase-rumah-tangga-menurut-fasilitas-tempat-buang-air-besar.html (accessed on 9 July 2021).
- BPS Statistics of East Sumba Regency. Persentase Rumah Tangga Menurut Sumber Air Utama yang Digunakan Untuk Minum di Kabupaten Sumba Timur, 2015–2017. Statistics of Sumba Timur Regency. 2018. Available online: https://sumbatimurkab.bps.go.id/dynamictable/2018/11/12/50/persentase-rumah-tangga-menurut-sumber-air-utama-yang-digunakan-untuk-minum-di-kabupaten-sumba-timur-2015-2017.html (accessed on 1 April 2021).
- Messakh, J.J.; Moy, D.L.; Mojo, D.; Maliti, Y. The linkage between household water consumption and rainfall in the semi-arid region of East Nusa Tenggara, Indonesia. IOP Conf. Ser. Earth Environ. Sci. 2018, 106, 012084. [Google Scholar] [CrossRef]
- Vel, J.A.C.; Makambombu, S. Access to Agrarian Justice in Sumba, Eastern Indonesia. Law Soc. Justice Glob. Dev. 2010, 2010, 1–22. Available online: https://warwick.ac.uk/fac/soc/law/elj/lgd/2010_1/vel_makambombu (accessed on 16 July 2021).
- Picauly, I.; Toy, S.M. Analisis Determinan dan Pengaruh Stunting Terhadap Prestasi Belajar Anak Sekolah di Kupang dan Sumba Timur, Ntt. J. Gizi dan Pangan 2013, 8, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Sungkar, S.; Pohan, A.P.N.; Ramadani, A.; Albar, N.; Azizah, F.; Nugraha, A.R.A.; Wiria, A.E. Heavy burden of intestinal parasite infections in Kalena Rongo village, a rural area in South West Sumba, eastern part of Indonesia: A cross sectional study. BMC Public Health 2015, 15, 1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- BPS Statistics of East Timur Regency. Sumba Timur in Figures 2019. 2019. Available online: http://sbdkab.go.id/sbdku/Kabupaten%20Sumba%20Barat%20Daya%20Dalam%20Angka%202019%20-%20Kominfo.pdf (accessed on 2 July 2021).
- Daniel, D.; Pande, S.; Rietveld, L. The effect of socio-economic characteristics on the use of household water treatment via psychosocial factors: A mediation analysis. Hydrol. Sci. J. 2020, 65, 2350–2358. [Google Scholar] [CrossRef]
- Daniel, D.; Pande, S.; Rietveld, L. Socio-Economic and Psychological Determinants for Household Water Treatment Practices in Indigenous–Rural Indonesia. Front. Water 2021, 3, 25. [Google Scholar] [CrossRef]
- Munamati, M.; Nhapi, I.; Misi, S. Exploring the determinants of sanitation success in Sub-Saharan Africa. Water Res. 2016, 103, 435–443. [Google Scholar] [CrossRef]
- Roma, E.; Bond, T.; Jeffrey, P. Factors involved in sustained use of point-of-use water disinfection methods: A field study from Flores Island, Indonesia. J. Water Health 2014, 12, 573–583. [Google Scholar] [CrossRef]
- Figueroa, M.; Kincaid, D. Social, Cultural and Behavioral Correlates of Household Water Treatment and Storage. Cent Publ HCI 2010-1 Heal Commun Insights, Balt Johns Hopkins Bloom Sch Public Heal Cent Commun Programs. 2010. 60p. Available online: http://ccp.jhu.edu/wp-content/uploads/Household-Water-Treatment-and-Storage-2010.pdf (accessed on 14 July 2017).
- Chittleborough, C.R.; Nicholson, A.L.; Basker, E.; Bell, S.L.; Campbell, R. Factors influencing hand washing behaviour in primary schools: Process evaluation within a randomized controlled trial. Health Educ. Res. 2012, 27, 1055–1068. [Google Scholar] [CrossRef] [Green Version]
- Behailu, B.M.; Pietilä, P.E.; Katko, T. Indigenous Practices of Water Management for Sustainable Services. SAGE Open 2016, 6, 2158244016682292. [Google Scholar] [CrossRef] [Green Version]
- Waterworth, P.; Pescud, M.; Braham, R.; Dimmock, J.; Rosenberg, M. Factors Influencing the Health Behaviour of Indigenous Australians: Perspectives from Support People. PLoS ONE 2015, 10, e0142323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubois, A.E.; Crump, J.A.; Keswick, B.H.; Slutsker, L.; Quick, R.E.; Vulule, J.M.; Luby, S.P. Determinants of Use of Household-level Water Chlorination Products in Rural Kenya, 2003–2005. Int. J. Environ. Res. Public Health 2010, 7, 3842–3852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldman, N.; Pebley, A.R.; Beckett, M. Diffusion of ideas about personal hygiene and contamination in poor countries: Evidence from Guatemala. Soc. Sci. Med. 2001, 52, 53–69. [Google Scholar] [CrossRef]
- George, C.M.; Jung, D.S.; Saif-Ur-Rahman, K.M.; Monira, S.; Sack, D.A.; Rashid, M.U.; Toslim, M.; Mustafiz, M.; Rahman, Z.; Bhuvian, S.I.; et al. Sustained Uptake of a Hospital-Based Handwashing with Soap and Water Treatment Intervention (Cholera-Hospital-Based Intervention for 7 Days [CHoBI7]): A Randomized Controlled Trial. Am. J. Trop. Med. Hyg. 2016, 94, 428–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosler, H.-J.; Kraemer, S.; Johnston, R. Achieving long-term use of solar water disinfection in Zimbabwe. Public Health 2013, 127, 92–98. [Google Scholar] [CrossRef]
- Freeman, M.C.; Trinies, V.; Boisson, S.; Mak, G.; Clasen, T. Promoting Household Water Treatment through Women’s Self Help Groups in Rural India: Assessing Impact on Drinking Water Quality and Equity. PLoS ONE 2012, 7, e44068. [Google Scholar] [CrossRef] [Green Version]
- Totouom, A.L.F.; Sikod, F.; Abba, I. Household Choice of Purifying Drinking Water in Cameroon. Environ. Manag. Sustain. Dev. 2012, 1, 101–115. [Google Scholar] [CrossRef]
- Nauges, C.; Van Den Berg, C. Perception of Health Risk and Averting Behavior: An Analysis of Household Water Consumption in Southwest Sri Lanka. Toulouse Sch. Econ. Work Pap. 2009, pp. 1–33. Available online: http://publications.ut-capitole.fr/3299/ (accessed on 10 August 2017).
- Christen, A.; Pacheco, G.D.; Hattendorf, J.; Arnold, B.F.; Cevallos, M.; Indergand, S.; Colford, J.M.; Mäusezahl, D. Factors associated with compliance among users of solar water disinfection in rural Bolivia. BMC Public Health 2011, 11, 210. [Google Scholar] [CrossRef] [Green Version]
- Houweling, T.A.; Kunst, A.; MacKenbach, J.P. Measuring health inequality among children in developing countries: Does the choice of the indicator of economic status matter? Int. J. Equity Health 2003, 2, 8. [Google Scholar] [CrossRef] [Green Version]
- Hall, N.L. Challenges of WASH in remote Australian Indigenous communities. J. Water Sanit. Hyg. Dev. 2019, 9, 429–437. [Google Scholar] [CrossRef]
- Jiménez, A.; Cortobius, M.; Kjellén, M. Water, sanitation and hygiene and indigenous peoples: A review of the literature. Water Int. 2014, 39, 277–293. [Google Scholar] [CrossRef]
- Latchmore, T.; Schuster-Wallace, C.J.; Longboat, D.R.; Dickson-Anderson, S.; Majury, A. Critical elements for local Indigenous water security in Canada: A narrative review. J. Water Health 2018, 16, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Benjamin-Chung, J.; Crider, Y.S.; Mertens, A.; Ercumen, A.; Pickering, A.J.; Lin, A.; Steinbaum, L.; Swarthout, J.; Rahman, M.; Parvez, S.M.; et al. Household finished flooring and soil-transmitted helminth and Giardia infections among children in rural Bangladesh and Kenya: A prospective cohort study. Lancet Glob. Health 2021, 9, e301–e308. [Google Scholar] [CrossRef]
- Holcomb, D.; Knee, J.; Sumner, T.; Adriano, Z.; de Bruijn, E.; Nalá, R.; Cumming, O.; Brown, J.; Stewart, J.R. Human fecal contamination of water, soil, and surfaces in households sharing poor-quality sanitation facilities in Maputo, Mozambique. Int. J. Hyg. Environ. Health 2020, 226, 113496. [Google Scholar] [CrossRef] [PubMed]
- Mathur, P. Hand hygiene: Back to the basics of infection control. Indian J. Med. Res. 2011, 134, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Ercumen, A.; Pickering, A.J.; Kwong, L.H.; Arnold, B.F.; Parvez, S.M.; Alam, M.; Sen, D.; Islam, S.; Kullmann, C.; Chase, C.; et al. Animal Feces Contribute to Domestic Fecal Contamination: Evidence from E. coli Measured in Water, Hands, Food, Flies, and Soil in Bangladesh. Environ. Sci. Technol. 2017, 51, 8725–8734. [Google Scholar] [CrossRef] [Green Version]
- Wardrop, N.A.; Hill, A.G.; Dzodzomenyo, M.; Aryeetey, G.; Wright, J.A. Livestock ownership and microbial contamination of drinking-water: Evidence from nationally representative household surveys in Ghana, Nepal and Bangladesh. Int. J. Hyg. Environ. Health 2018, 221, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Penakalapati, G.; Swarthout, J.; Delahoy, M.J.; McAliley, L.; Wodnik, B.; Levy, K.; Freeman, M.C. Exposure to Animal Feces and Human Health: A Systematic Review and Proposed Research Priorities. Environ. Sci. Technol. 2017, 51, 11537–11552. [Google Scholar] [CrossRef] [Green Version]
- Ercumen, A.; Naser, A.M.; Unicomb, L.; Arnold, B.; Colford, J.M., Jr.; Luby, S. Effects of Source- versus Household Contamination of Tubewell Water on Child Diarrhea in Rural Bangladesh: A Randomized Controlled Trial. PLoS ONE 2015, 10, e0121907. [Google Scholar] [CrossRef]
- Bamualim, A.; Livestock Production and Fire Management in East Nusa Tenggara. Fire and Sustainable Agricultural and Forestry Development in Eastern Indonesia and Northern Australia. Proceedings of an International Workshop Held at Northern Territory University, Darwin, Australia, 13–15 April 1999; pp. 69–72. Available online: https://png-data.sprep.org/system/files/Fire%20and%20Sustainable%20Agricultural%20and%20Forestry%20Development%20in%20Eastern%20Indonesia%20and%20Northern%20Australia.pdf (accessed on 16 July 2021).
- Daniel, D.; Djohan, D.; Machairas, I.; Pande, S.; Arifin, A.; Al Djono, T.P.; Rietveld, L. Financial, institutional, environmental, technical, and social (FIETS) aspects of water, sanitation, and hygiene conditions in indigenous—rural Indonesia. BMC Public Health 2021, 21, 1723. [Google Scholar] [CrossRef]
- The World Bank. Average Precipitation in Depth (mm per Year)—Indonesia; The World Bank: Washington, DC, USA, 2014; (accessed on 4 November 2019). [Google Scholar]
- Okotto-Okotto, J.; Wanza, P.; Kwoba, E.; Yu, W.; Dzodzomenyo, M.; Thumbi, S.M.; da Silva, D.T.G.; Wright, J.A. An Assessment of Inter-Observer Agreement in Water Source Classification and Sanitary Risk Observations. Expo. Health 2020, 12, 809–822. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.; Sobsey, M.D. Boiling as Household Water Treatment in Cambodia: A Longitudinal Study of Boiling Practice and Microbiological Effectiveness. Am. J. Trop. Med. Hyg. 2012, 87, 394–398. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Questions | Scale * |
|---|---|---|
| Open Defecation | What types of toilets do you have? | 2 (Open defecation or not) |
| Livestock nearby | Is there livestock around the house? | 3 (Many–few) |
| Floor types | What type of floor does the main house have? | 2 (Permanent or not) |
| Floor cleanliness | How is the cleanliness of the house floor? | 3 (Dirty–clean) |
| Feces around | Is there human or animal feces in the yard (or even inside the house)? | 3 (Many–few) |
| Garbage around | Is there garbage around the house? | 3 (Many–few) |
| Flies around | Can you see flies around the water storage container? | 3 (Many–few) |
| Food storage | How do you store cooked food? | 2 (with or without cover) |
| Storage covered | Is the water storage being covered (at that time)? | 2 (Yes or not) |
| Storage cracked | Is the container cracked? | 2 (Yes or not) |
| Place of water storage | When not in use, is the storage container kept in a place where it may become contaminated? | 2 (Yes or not) |
| Storage cleanliness | Is the inside of the container clean? | 2 (Dirty or clean) |
| Practice household water treatment (HWT) | Is the drinking water treated? | 2 (Yes or not) |
| E. coli detected | Data were from quality testing the drinking water | 2 (Yes or not) |
| Handwashing facilities | What kind of handwashing facilities does the household have? | 2 (With water and soap or not) |
| Respondent’s nails | How clean are the respondent nails? | 3 (Dirty–clean) |
| Open Defecation | Livestock Nearby | Floor Types | Floor Cleanliness | Faeces Around | Garbage Around | Flies Around | Food Storage | Storage Covered | Storage Cracked | Place of Water Storage | Storage Cleanliness | Practice HWT | Water Quality | Handwashing Facilities | Respondent’s Nails | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Open Defecation | ||||||||||||||||
| Livestock nearby | ||||||||||||||||
| Floor types | ||||||||||||||||
| Floor cleanliness | ||||||||||||||||
| Faeces around | ||||||||||||||||
| Garbage around | ||||||||||||||||
| Flies around | ||||||||||||||||
| Food storage | ||||||||||||||||
| Storage covered | ||||||||||||||||
| Storage cracked | ||||||||||||||||
| Place of water storage | ||||||||||||||||
| Storage cleanliness | ||||||||||||||||
| Practice HWT | ||||||||||||||||
| Water quality | ||||||||||||||||
| Handwashing facilities | ||||||||||||||||
| Respondent’s nails |
| Determinant Variables | B | SE | β | p Value | LB | UB |
|---|---|---|---|---|---|---|
| Constant | 20.22 | 1.31 | 0.00 | 17.65 | 22.80 | |
| Wealth | 1.03 | 0.38 | 0.23 | 0.01 | 0.29 | 1.78 |
| Access to water | −0.43 | 0.20 | −0.14 | 0.04 | −0.83 | −0.03 |
| Household time allocation | 0.06 | 0.13 | 0.03 | 0.63 | −0.19 | 0.31 |
| Local beliefs | −0.87 | 0.65 | −0.09 | 0.19 | −2.16 | 0.42 |
| Access to market | 0.93 | 0.53 | 0.10 | 0.08 | −0.11 | 1.96 |
| Access to mass media | 0.15 | 0.24 | 0.05 | 0.52 | −0.32 | 0.62 |
| Receiving WASH promotions | −0.11 | 0.78 | −0.01 | 0.89 | −1.64 | 1.42 |
| Mother’s education | −0.10 | 0.10 | −0.08 | 0.32 | −0.28 | 0.09 |
| Father’s education | 0.01 | 0.09 | 0.01 | 0.88 | −0.17 | 0.20 |
| Having children under 5-years-old | 0.00 | 0.52 | 0.00 | 1.00 | −1.02 | 1.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daniel, D. Contextual Determinants of General Household Hygiene Conditions in Rural Indonesia. Int. J. Environ. Res. Public Health 2021, 18, 11064. https://doi.org/10.3390/ijerph182111064
Daniel D. Contextual Determinants of General Household Hygiene Conditions in Rural Indonesia. International Journal of Environmental Research and Public Health. 2021; 18(21):11064. https://doi.org/10.3390/ijerph182111064
Chicago/Turabian StyleDaniel, D. 2021. "Contextual Determinants of General Household Hygiene Conditions in Rural Indonesia" International Journal of Environmental Research and Public Health 18, no. 21: 11064. https://doi.org/10.3390/ijerph182111064
APA StyleDaniel, D. (2021). Contextual Determinants of General Household Hygiene Conditions in Rural Indonesia. International Journal of Environmental Research and Public Health, 18(21), 11064. https://doi.org/10.3390/ijerph182111064