
Animal-Assisted Interventions for the Improvement of Mental Health Outcomes in Higher Education Students: A Systematic Review of Randomised Controlled Trials


Abstract
1. Introduction
- emotional contagion (transmitting the animal’s positive emotions onto humans)
- facilitating social interaction
- opportunities for reinforcement (by partaking in pleasurable activities and experiencing positive emotions)
- evoking expectations that participation will reduce stress (expectancy that the intervention will work)
2. Aim and Objectives
- systematically search and critically appraise the relevant published and unpublished literature on the effectiveness of AAIs, particularly AAT and AAA, in improving mental health outcomes for this particular population.
- provide evidenced-based recommendations for policy, practice and further research.
3. Methods
3.1. Protocol and Ethics
3.2. Search Strategy
3.3. Inclusion and Exclusion Criteria
- control (no-treatment, attention, usual care, or wait-list)
- validated sham treatment (where known not to be efficacious)
- other active intervention with known efficacy
- sham/alternative treatments (where efficacy is unknown)
3.4. Study Selection
3.5. Data Extraction
- study characteristics (such as design, setting and country)
- participants (including eligibility criteria, age, gender, and type of student)
- interventions (for example single/multiple sessions, species of animal, if handler present, duration and frequency of sessions as well as length of programme)
- outcomes (such as the relevant measures used, interpretation, results and time-points for measurements)
3.6. Risk of Bias Assessment and Strength of Evidence
4. Results
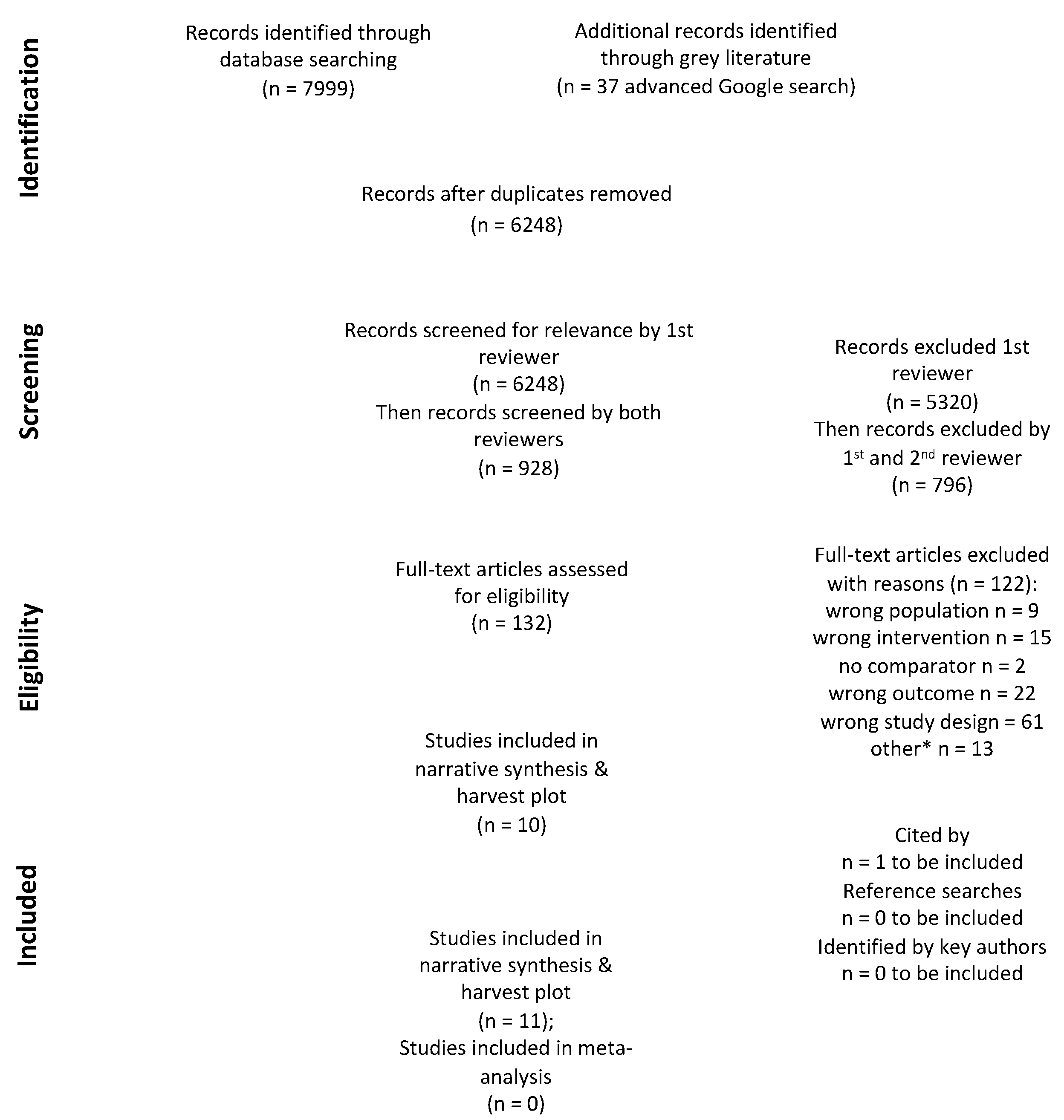
4.1. Study Selection
4.2. Study Characteristics
4.2.1. Population
4.2.2. Intervention
4.2.3. Outcomes
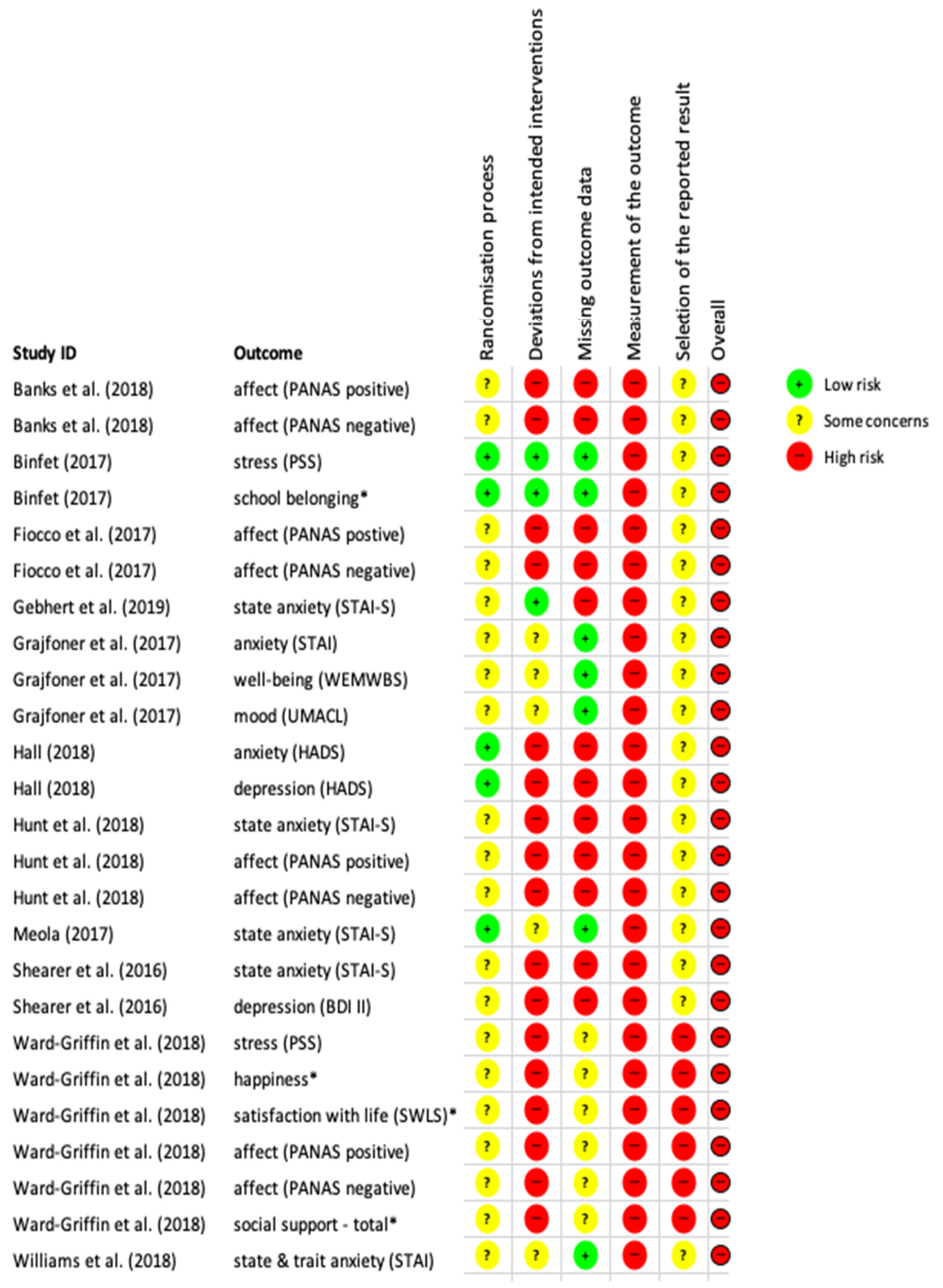
4.3. Risk of Bias Assessment
4.4. Strength of Evidence
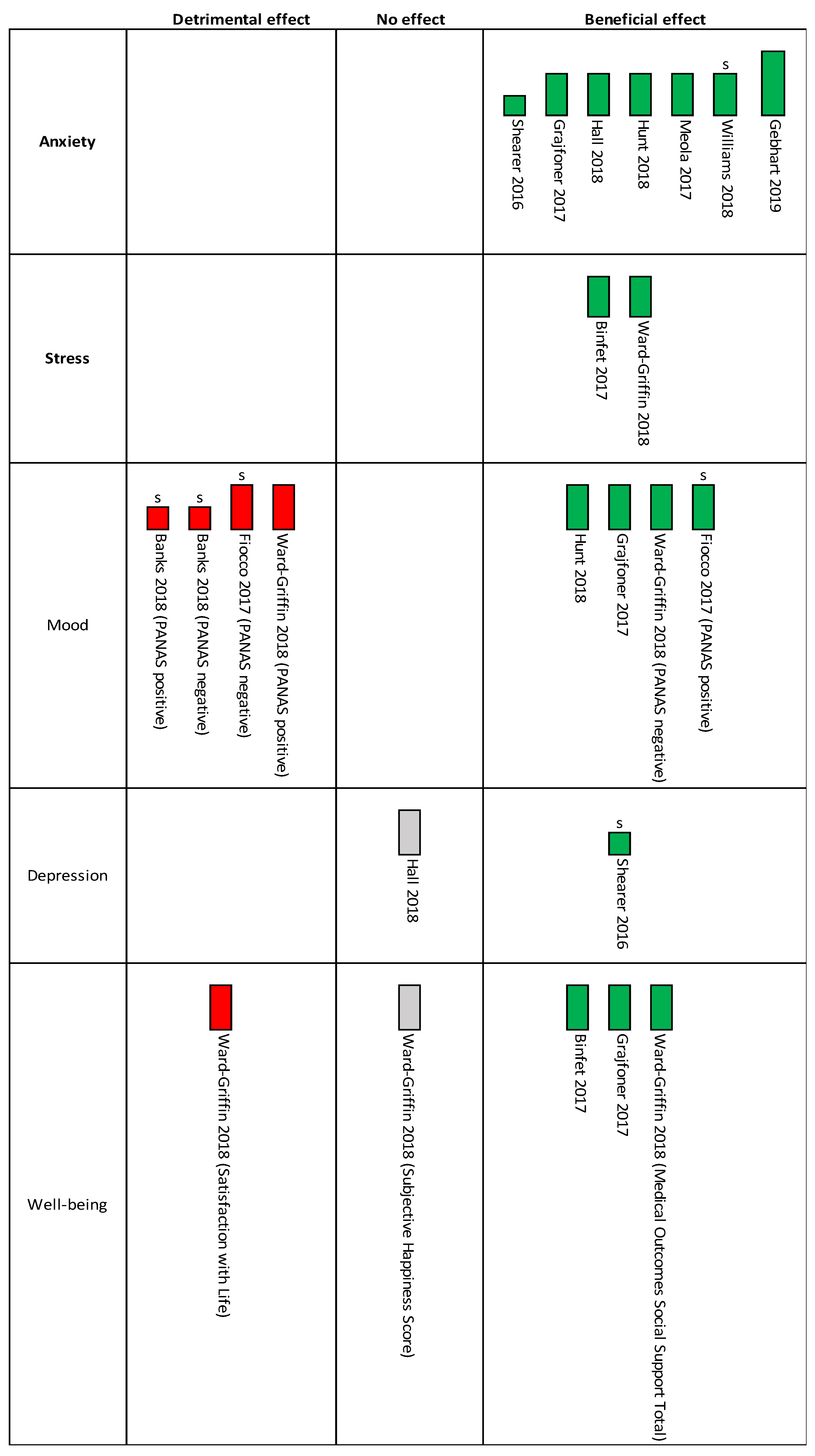
4.5. Narrative Synthesis: Interventions’ Effect
4.5.1. Primary Outcomes: Anxiety
4.5.2. Primary Outcome: Stress
4.5.3. Secondary Outcomes: Depression, Mood/Affect and Well-Being
5. Discussion
5.1. Statement of Principal Findings
5.2. Strengths and Weaknesses of the Review
5.3. Strengths and Weaknesses of the Studies
5.4. Study Meaning: Possible Mechanism and Implications for Policymakers
- time (sessions to be short)
- money (sessions to be cost-neutral for students)
- physical effort (sessions to be offered in an accessible location)
- brain cycles (process by which to attend the sessions should be easy)
- social acceptance (as offered by activities with animals)
- routine (regular sessions to be offered)
5.5. Future Research Recommendations
- Use of standardised and internationally recognised definitions when describing AAIs
- Use of sample sizes that provide adequate power
- Clarity regarding the randomisation procedure (including description of allocation, and whether concealed allocation occurred) and provision of an adequate description of the participants’ characteristics separated by group
- Clear reporting of the participants’ flow through the trial with reasons for any missing data for each respective group and at each time-point
- Use of explicit comparators to establish the relative effects of the co-interventions (e.g., appropriate attention controls)
- Adequate descriptions of the interventions implemented to facilitate replication
- Clear reporting of the outcome measurement procedure (particularly when multiple time-points or stressors are present), including any adaptations made to the scales used
- Provision of access to publicly available pre-specified statistical analysis plans by authors, including justification for choice of target differences
- Clear reporting of adverse events for both humans and animals
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAA | Animal-Assisted Activity |
| AAC | Animal-Assisted Coaching |
| AAE | Animal-Assisted Education |
| AAI | Animal-Assisted Intervention |
| AAT | Animal-Assisted Therapy |
| ADHD | Attention Deficit Hyperactivity Disorder |
| ANOVA | analysis of variance |
| ANCOVA | analysis of covariance |
| BDI-II | Beck Depression Inventory II |
| DO | dog only |
| EALS | equine-assisted learning supervision |
| EPPI | Evidence for Policy and Practice Information |
| ESRC | Economic and Social Research Council |
| FBM | Fogg Behavioural Model |
| F/up | follow-up |
| HADS | Hospital Anxiety and Depression Scale |
| HEI | higher education institute |
| HO | handler only |
| IAHAIO | International Association of Human-Animal Interaction Organizations |
| IQR | interquartile range |
| IRB | Institutional Review Boards |
| MANCOVA | multivariate analysis of covariance |
| MANOVA | multivariate analysis of variance |
| MeSH | Medical Subject Headings |
| MOS Social Support Scale | Medical Outcomes Study Social Support Scale |
| NR | not reported |
| NS | not significant |
| PANAS | Positive and Negative Affect Schedule |
| PASAT | Paced Auditory Serial Addition Task |
| PICOS | Population, Intervention, Comparator, Outcome, Study design |
| PSS | Perceived Stress Scale |
| RCT | randomised controlled trial |
| SART | Sustained Attention to Response Task |
| SD | standard deviation |
| SES | socioeconomic status |
| SSS | student support services |
| STAI | State-Trait Anxiety Inventory |
| SWLS | Satisfaction with Life Score |
| TIDieR | template for intervention description and replication |
| UMACL | University of Wales Institute of Science & Technology Mood Adjective Checklist |
| UWIST | University of Wales Institute of Science & Technology |
| WAIQ Scale-IV | Wechsler Adult Intelligence Scale-IV |
| WEMWBS | Warwick-Edinburgh Mental Well-being Scale |
| Yrs | years |
Appendix A
- (1)
- [Student$ or pupil$ or undergrad$ or postgrad$ or graduat$ or freshm?n* or sophomor$ or junior$ or senior$ or learner$ or scholar$ or apprentic$ or classmate$].ti.kw.ab
- (2)
- [junior$ or senior$] adj1 year$].ti,kw,ab.
- (3)
- Exp students/
- (4)
- [colleg$ or universit$ or school$ or conservator$ or classroom$ or apprenticeship$ or facult$].ti,kw,ab.
- (5)
- [[educat$ or graduat$ or undergrad$ or academ$ or junior$ or senior$ or postsecondary$ or ‘post secondary$’] adj1 [school$ or colleg$ or universit$ or institut$ or setting$ or facult$ or establish$ or program$]].ti,kw,ab.
- (6)
- [[seminar$ or lectur$] adj1 [room$ or theatre$]].ti,kw,ab
- (7)
- Exp schools/
- (8)
- Exp “internship and residency”/
- (9)
- Exp faculty/
- (10)
- Exp nursing faculty practice/
- (11)
- Exp education, nonprofessional/
- (12)
- Exp education, predental/
- (13)
- Exp education, premedical/
- (14)
- Exp education, professional/
- (15)
- Exp inservice training/
- (16)
- Exp international educational exchange/
- (17)
- Exp “academies and institutes”/
- (18)
- 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17
- (19)
- “human$ animal$ interact$’.ti,ab,kw.
- (20)
- Exp bonding, human-pet/
- (21)
- ‘human$ animal$ bond$’.ti,ab,kw.
- (22)
- Exp animal assisted therapy/
- (23)
- [[animal$ or pet$ or dog$ or canine$ or hound$ or pooch$ or pup$ or cat$ or feline$ or kitt$ or equine$ or horse$ or hippo$ or pony$ or foal$ or riding$ or ‘guinea$ pig$’ or rabbit$ or bunn$ or ferret$ or hamster$ or rodent$ or mammal$ or bird$ or cow$ or pig$ or sheep$ or lamb$ or dolphin$ or aquatic$ or fish$ or marine$ or reptile$] adj5 [therap$ or intervent$ or activit$ or psychotherap$ or interact$ or visit$ or program$]].ti,kw,ab.
- (24)
- Exp equine-assisted therapy/
- (25)
- 19 or 20 or 21 or 22 or 23 or 24
- (26)
- Exp resilience, psychological/
- (27)
- [Anxiet$ or anxious$ or worr$ or concern$ or apprehens$ or nervous$ or fear$ or distress$ or panic$ or neuros$ or apath$ or mood$ or dread$ or terror$ or phobia$ or irritable$].ti,ab,kw.
- (28)
- Exp psychological distress/
- (29)
- Exp stress, psychological/
- (30)
- Exp stress disorder, traumatic/
- (31)
- Exp stress, physiological/
- (32)
- [Stress$ or burnout$ or burn-out$ or ‘burn out’].ti,ab,kw.
- (33)
- [Depress$ or sad$ or sorr$ or unhapp$ or grie$ or lone$ or happ$ or dysthymia$].ti,kw,ab.
- (34)
- [Internali? adj1 [disorder$ or symptom$ or behavio$]].ti,ab,kw.
- (35)
- [Self$ adj/1 [esteem$ or accept$ or confiden$ or concept$]].ti,ab,kw.
- (36)
- [[Emotion$ or mental$] adj/1 [health$ or illness$ or wellbeing or well-being or ‘well being]’ or cop$ or stress$ or burnout or burn-out or ‘burn out’ or resilien$]].ti,ab,kw
- (37)
- Exp emotions/
- (38)
- Exp depression/
- (39)
- Exp mental health/
- (40)
- Exp self concept/
- (41)
- Exp mood disorders
- (42)
- Exp anxiety disorders
- (43)
- 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42
- (44)
- 18 and 25 and 43
- (1)
- [[animal$ or pet$ or dog$ or canine$ or hound$ or pooch$ or pup$ or cat$ or feline$ or kitt$ or equine$ or horse$ or hippo$ or pony$ or foal$ or riding$ or ‘guinea$ pig$’ or rabbit$ or bunn$ or ferret$ or hamster$ or rodent$ or mammal$ or bird$ or cow$ or pig$ or sheep$ or lamb$ or dolphin$ or aquatic$ or fish$ or marine$ or reptile$] adj5 [therap$ or intervent$ or activit$ or psychotherap$ or interact$ or visit$ or program$]].tw.
- (2)
- “human$ animal$ interact$”.tw.
- (3)
- “human$ animal$ bond$”.tw.
- (4)
- Exp interspecies interaction/
- (5)
- Exp animal assisted therapy/
- (6)
- 1 or 2 or 3 or 4 or 5
- (7)
- [college$ or universit$ or school$ or conservator$ or classroom$ or apprenticeship$ or faculty$].tw.
- (8)
- [[educat$ or graduat$ or undergraduat$ or academ$ or junior$ or senior$ or postsecondary$ or “postsecondary$”] adj1 [school$ or colleg$ or universit$ or institut$ or setting$ or facult$ or establish$ or program$]].tw.
- (9)
- [[seminar$ or lectur$] adj1 [room$ or theatre$]].tw.
- (10)
- [high$ adj1 educat$].tw.
- (11)
- Exp colleges/
- (12)
- Exp schools/
- (13)
- Exp classrooms/
- (14)
- Exp apprenticeship/
- (15)
- Exp higher education/
- (16)
- Exp academic settings/
- (17)
- Exp educational programs/
- (18)
- Exp college environment/
- (19)
- Exp educational degrees/
- (20)
- Exp nursing education/
- (21)
- Exp educational placement/
- (22)
- Exp adult education/
- (23)
- Exp academic environment/
- (24)
- Exp campuses/
- (25)
- [student$ or pupil$ or undergrad$ or postgrad$ or graduat$ or freshm?n* or sophomor$ or junior$ or senior$ or learner$ or scholar$ or apprentic$ or classmate$].tw.
- (26)
- [[junior$ or senior$] adj1 year$].tw.
- (27)
- Exp student/
- (28)
- Exp classmates/
- (29)
- 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28
- (30)
- [anxiet$ or anxious$ or worr$ or concern$ or apprehens$ or nervous$ or fear$ or distress$ or panic$ or neuros$ or apath$ or mood$ or dread$ or terror$ or phobia$ or irritable$].tw
- (31)
- [depress$ or sad$ or sorr$ or unhapp$ or grie$ or lone$ or happ$ or dysthymia$].tw.
- (32)
- [stress$ or burnout or burn-out or “burn out”].tw.
- (33)
- [[emotion$ or mental$] adj1 [health$ or illness$ or wellbeing or well-being or “well-being” or cop$ or stress$ or burnout or burn-out or “burn-out” or resilien$]].tw.
- (34)
- [internali? adj1 [disorder$ or symptom$ or behavio$]].tw.
- (35)
- [self adj1 [esteem$ or accept$ or confiden$ or concept$]].tw.
- (36)
- Exp emotions/
- (37)
- Exp anxiety disorders/
- (38)
- Exp neurosis/
- (39)
- Exp irritability/
- (40)
- Exp affective disorders/
- (41)
- Exp well being/
- (42)
- Exp anhedonia/
- (43)
- Exp mental health/
- (44)
- Exp emotional adjustment/
- (45)
- Exp “resilience [psychological]”/
- (46)
- Exp coping behaviour/
- (47)
- Exp internalization/
- (48)
- Exp self-esteem/
- (49)
- Exp self-perception/
- (50)
- Exp self-concept/
- (51)
- Exp stress
- (52)
- 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 0r 51
- (53)
- 6 and 29 and 52
- (1)
- “human$ animal$ interact$”.ti,ab,kw.
- (2)
- “human$ animal$ bond$”. ti,ab,kw.
- (3)
- [[animal$ or pet$ or dog$ or canine$ or hound$ or pooch$ or pup$ or cat$ or feline$ or kitt$ or equine$ or horse$ or hippo$ or pony$ or foal$ or riding$ or ‘guinea$ pig$’ or rabbit$ or bunn$ or ferret$ or hamster$ or rodent$ or mammal$ or bird$ or cow$ or pig$ or sheep$ or lamb$ or dolphin$ or aquatic$ or fish$ or marine$ or reptile$] adj5 [therap$ or intervent$ or activit$ or psychotherap$ or interact$ or visit$ or program$]].ti,ab,kw.
- (4)
- Exp animal assisted therapy/
- (5)
- Exp human-animal bond/
- (6)
- 1 or 2 or 3 or 4 or 5
- (7)
- [colleg$ or universit$ or school$ or conservator$ or classroom$ or apprenticeship$ or facult$].ti,ab,kw.
- (8)
- [[seminar$ or lectur$] adj1 [room$ or theatre$]].ti,ab,kw.
- (9)
- [high$ adj1 educat$].ti.ab.kw.
- (10)
- [[educat$ or graduat$ or undergraduat$ or academ$ or junior$ or senior$ or postsecondary$ or “post secondary$”] adj1 [school$ or colleg$ or universit$ or institut$ or setting$ or facult$ or establish$ or program$]].ti,ab,kw.
- (11)
- Exp university/
- (12)
- Exp college/
- (13)
- Exp school/
- (14)
- Exp school health service/
- (15)
- Exp apprenticeship/
- (16)
- Exp adult education/
- (17)
- Exp doctoral education/
- (18)
- Exp education program/
- (19)
- Exp in service training/
- (20)
- Exp medical education/
- (21)
- Exp masters education/
- (22)
- Exp paramedical education
- (23)
- Exp postdoctoral education/
- (24)
- Exp postgraduate education/
- (25)
- Exp teacher training/
- (26)
- 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25
- (27)
- [student$ or pupil$ or undergrad$ or postgrad$ or graduat$ or freshm?n* or sophomor$ or junior$ or senior$ or learner$ or scholar$ or apprentic$ or classmate$].ti,ab,kw.
- (28)
- [[junior$ or senior$] adj1 year$].ti,ab,kw.
- (29)
- Exp student/
- (30)
- Exp graduate/
- (31)
- 27 or 28 or 29 or 30
- (32)
- [anxiet$ or anxious$ or worr$ or concern$ or apprehens$ or nervous$ or fear$ or distress$ or panic$ or neuros$ or apath$ or mood$ or dread$ or terror$ or phobia$ or irritable$].ti,ab,kw.
- (33)
- [depress$ or sad$ or sorr$ or unhapp$ or grie$ or lone$ or happ$ or dysthymia$].ti,ab,kw.
- (34)
- [stress$ or burnout or burn-out or “burn out”].ti,ab,kw.
- (35)
- [[emotion$ or mental$] adj1 [health$ or illness$ or wellbeing or well-being or “well-being” or cop$ or stress$ or burnout or burn-out or “burn-out” or resilien$]].ti,ab,kw.
- (36)
- [internali? adj1 [disorder$ or symptom$ or behavio$].ti,ab,kw.
- (37)
- [self$ adj1 [esteem$ or accept$ or confiden$ or concept$]].ti,ab,kw
- (38)
- Exp emotion/
- (39)
- Exp anxiety disorder/
- (40)
- Exp neurosis/
- (41)
- Exp affect/
- (42)
- Exp mood disorder/
- (43)
- Exp stress/
- (44)
- Exp temperament/
- (45)
- Exp emotional disorder/
- (46)
- Exp wellbeing/
- (47)
- Exp coping behaviour/
- (48)
- Exp psychological resilience/
- (49)
- Exp mental health/
- (50)
- Exp self concept/
- (51)
- 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50
- (52)
- 26 or 31
- (53)
- 6 and 51 and 52
- (1)
- [Anxiet* or anxious* or worr* or concern* or apprehens* or nervous* or fear* or distress* or panic* or neuros* or apath* or mood* or dread* or terror* or phobia* or irritable*]:ti,ab,kw
- (2)
- [Depress* or sad* or sorr* or unhapp* or grie* or lone* or happ* or dysthymia*]:ti.ab.kw
- (3)
- [Stress* or burnout or burn-out or [burn NEXT out]]:ti,ab,kw
- (4)
- [[Emotion* or mental*] NEAR/1 [health* or illness* or wellbeing or well-being or [well NEXT being] or cop* or stress* or burnout or burn-out or [burn NEXT out] or resilien*]]:ti,ab,kw
- (5)
- [[Internali? NEAR/1 [disorder* or symptom* or behavio*]]]:ti,ab,kw
- (6)
- [Self* NEAR/1 [esteem* or accept* or confiden* or concept*]]:ti,ab,kw
- (7)
- MeSH descriptor: [Anxiety] explode all trees
- (8)
- MeSH descriptor: [Anxiety Disorders] explode all trees
- (9)
- MeSH descriptor: [Emotions] explode all trees
- (10)
- MeSH descriptor: [Emotional Adjustment] explode all trees
- (11)
- MeSH descriptor: [Expressed Emotion] explode all trees
- (12)
- MeSH descriptor: [Mood Disorders] explode all trees
- (13)
- MeSH descriptor: [Depression] explode all trees
- (14)
- MeSH descriptor: [Trauma and Stressor Related Disorders] explode all trees
- (15)
- MeSH descriptor: [Stress, Psychological] explode all trees
- (16)
- MeSH descriptor: [Affective Symptoms] explode all trees
- (17)
- MeSH descriptor: [Mental Health] explode all trees
- (18)
- MeSH descriptor: [Resilience, Psychological] explode all trees
- (19)
- MeSH descriptor: [Self Concept] explode all trees
- (20)
- OR #1-#19
- (21)
- [student* or pupil* or undergrad* or postgrad* or graduat* or freshm?n* or sophomor* or junior* or senior* or learner* or scholar* or apprentic* or classmate*]:ti,ab,kw
- (22)
- [[junior* or senior*] NEAR/1 year*].ti,ab,kw
- (23)
- MeSH descriptor: [Students] explode all trees
- (24)
- OR #21-#23
- (25)
- [colleg* or universit*or school* or conservator* or classroom* or apprenticeship* or facult*]:ti,ab,kw
- (26)
- [[educat* or graduat* or undergraduat* or academ* or junior* or senior* or postsecondary* or [post NEXT secondary*]] NEAR/1 [school* or colleg* or universit* or institut* or setting* or facult* or establish* or program*]]:ti,ab,kw
- (27)
- [[seminar* or lectur*] NEAR/1 [room* or theatre*]]:ti,ab,kw
- (28)
- [high* NEAR/1 educat*]:ti.ab.kw
- (29)
- MeSH descriptor: [College Fraternities and Sororities] explode all trees
- (30)
- MeSH descriptor: [Universities] explode all trees
- (31)
- MeSH descriptor: [Schools] explode all trees
- (32)
- MeSH descriptor: [Clinical Clerkship] explode all trees
- (33)
- MeSH descriptor: [Educational, nonprofessional] explode all trees
- (34)
- MeSH descriptor: [Educational, professional] explode all trees
- (35)
- MeSH descriptor: [Educational, predental] explode all trees
- (36)
- MeSH descriptor: [Educational, premedical] explode all trees
- (37)
- MeSH descriptor: [International Educational Exchange] explode all trees
- (38)
- MeSH descriptor: [Inservice Training] explode all trees
- (39)
- MeSH descriptor: [Academies and Institutes] explode all trees
- (40)
- OR #25-39
- (41)
- [human* NEXT animal* NEXT interact*].ti,ab,kw
- (42)
- [human* NEXT animal* NEXT bond*].ti,ab,kw
- (43)
- MeSH descriptor: [Bonding, Human-Pet] explode all trees
- (44)
- MeSH descriptor: [Animal Assisted Therapy] explode all trees
- (45)
- MeSH descriptor: [Equine-assisted therapy] explode all trees
- (46)
- [[[animal* or pet* or dog* or canine* or hound* or pooch* or pup* or cat* or feline* or kitt* or equine* or horse* or hippo* or pony* or foal* or riding* or [guinea* NEAR pig*] or rabbit* or bunn* or ferret* or hamster* or rodent* or mammal* or bird* or cow* or pig* or sheep* or lamb* or dolphin* or aquatic* or fish* or marine* or reptile*] NEAR/5 [therap* or intervent* or activit* or psychotherap* or interact* or visit* or program*]]]:ti,ab,kw
- (47)
- OR #41-#46
- (48)
- #24 OR #40
- (49)
- #47 AND #48 AND #20
- 1st search: [“animal assisted therapy” OR “pet therapy”] AND [university OR college] AND [anxiety OR stress]
- 2nd search: [“human animal interaction” OR “animal assisted intervention”] AND [university OR college] AND [anxiety OR stress]
- 3rd search: [“animal assisted therapy” OR “pet therapy”] AND [undergraduate OR postgraduate] AND [anxiety OR stress]
- 4th search: [“human animal interaction” OR “animal assisted intervention”] AND [undergraduate OR postgraduate] AND [anxiety OR stress]
Appendix B
- (1)
- anxiety was worse after the intervention (as expected due to the stressor) but not by as much as the control group
- (2)
- no change seen after the intervention, but anxiety was worse in the control group
- (3)
- anxiety was better after the intervention and better than the control group

{kind=link}
{kind=link}
{kind=link}
| Interpretation | Requirements |
|---|---|
| Without a stressor | |
| Beneficial | Post-intervention assessment shows improvement in scores (direction relative to the measure used) compared to pre-assessment and better than control |
| No | Post-intervention assessment:
|
| Detrimental | Post-intervention assessment shows worsening in scores (direction relative to the measure used) compared to pre-assessment and worse than control |
| With a stressor (either before the post-assessment or present during post-assessment, e.g., occurring prior to an exam) | |
| Beneficial | Post-intervention assessment shows:
|
| Detrimental | Post-intervention assessment shows worsening in scores (direction relative to the measure used) compared to pre-assessment as would be expected due to stressor and worse than control |
Appendix C
| References of Excluded Studies from Full Manuscript Search | Reason Excluded |
|---|---|
| Adamle et al. [93] | wrong study design |
| Adams et al. [94] | wrong study design |
| Adams et al. [95] | wrong study design |
| Alonso [96] | criteria for inter-library loan not met |
| Anderson [97] | wrong outcome measures |
| Anonymous [98] | criteria for inter-library loan not met |
| Anonymous [99] | wrong study design |
| Ashton [100] | wrong study design |
| Baghain et al. [101] | wrong study design |
| Bajorek [102] | wrong outcomes |
| Barker et al. [103] | wrong outcomes |
| Barker et al. [104] | wrong outcomes |
| Barker et al. [105] | wrong study design |
| Barlow et al. [106] | wrong intervention |
| Basil et al. [107] | wrong study design |
| Behnke et al. [108] | wrong study design |
| Bell [2] | wrong study design |
| Beutler et al. [109] | wrong study design |
| Biery [110] | criteria for inter-library loan not met |
| Binfet et al. [111] | wrong study design |
| Binfet et al. [112] | wrong study design |
| Binfet et al. [113] | no comparator |
| Bjick [114] | wrong study design |
| Blender [115] | wrong intervention |
| Brelsford et al. [13] | wrong population |
| Broeyer et al. [116] | criteria for inter-library loan not met |
| Buttelmann et al. [117] | wrong study design |
| Chakales et al. [118] | wrong study design |
| Chramouleeswaran et al. [119] | wrong population |
| Cieslak [120] | wrong outcomes |
| ClinicalTrials.gov [121] | wrong intervention |
| ClinicalTrials.gov [122] | wrong outcomes |
| ClinicalTrials.gov [123] | wrong outcomes |
| ClinicalTrials.gov [124] | not included as trial still ongoing |
| Colarelli et al. [125] | wrong intervention |
| Coleman et al. [126] | wrong outcomes |
| Crago et al. [127] | wrong study design |
| Crossman et al. [6] | wrong study design |
| Crossman et al. [36] | wrong study design |
| Crump et al. [21] | wrong study design |
| Daltry et al. [34] | wrong study design |
| Delgado et al. [128] | wrong study design |
| Dell et al. [129] | wrong study design |
| Dhooper et al. [130] | wrong study design |
| Dluzynski [131] | wrong outcomes |
| Duffey T [132] | wrong study design |
| Flaherty [133] | wrong intervention |
| Folse et al. [134] | wrong study design |
| Frederick [135] | wrong population |
| Frederick et al. [136] | wrong population |
| Friedmann et al. [137] | wrong outcomes |
| Gonzalez-Ramirez et al. [138] | wrong outcomes |
| Goodkind et al. [139] | wrong population |
| Gress [140] | criteria for inter-library loan not met |
| Haggerty et al [141] | wrong study design |
| Hammer et al. [142] | wrong study design |
| Hemingway et al. [143] | wrong study design |
| Henry [144] | wrong intervention |
| House et al. [145] | wrong study design |
| Ishimura et al. [146] | wrong intervention |
| Jarolmen et al. [147] | wrong outcomes |
| Johnson [148] | wrong study design |
| King [149] | wrong study design |
| Kobayashi et al. [150] | wrong outcomes |
| Kronholz et al. [151] | wrong study design |
| Kuzara et al. [152] | wrong outcomes |
| Lacoff et al. [153] | wrong study design |
| Lauriente et al. [154] | wrong study design |
| Lephart et al. [155] | wrong study design |
| Linden [156] | criteria for inter-library loan not met |
| Litwiller et al. [157] | wrong study design |
| Machova et al. [158] | wrong study design |
| Malakoff [159] | wrong population |
| Manor [160] | criteria for inter-library loan not met |
| Marino [161] | wrong study design |
| Matsuura et al. [162] | wrong intervention |
| McArthur et al. [163] | wrong study design |
| McCrindle [164] | criteria for inter-library loan not met |
| McDonald et al. [165] | wrong intervention |
| Merritt [166] | criteria for inter-library loan not met |
| Morrison [15] | wrong study design |
| Morgan [167] | wrong study design |
| Muckle et al. [168] | wrong study design |
| Muellmann et al. [169] | wrong study design |
| Nocentini et al. [170] | wrong study design |
| Pendry et al. [171] | wrong outcomes |
| Pendry et al. [172] | wrong outcomes |
| Pendry et al. [173] | wrong outcomes |
| Pendry et al. [174] | wrong outcomes |
| Pendry et al. [175] | wrong intervention |
| Perry et al. [176] | wrong study design |
| Picard [177] | wrong intervention |
| Polking et al. [178] | wrong study design |
| Quinn et al. [179] | wrong study design |
| Ralston et al. [180] | wrong study design |
| Renne et al. [181] | wrong study design |
| Robino et al. [182] | wrong study design |
| Robson [183] | wrong study design |
| Rose [184] | wrong study design |
| Sanford [185] | wrong study design |
| Silas et al. [186] | wrong study design |
| Sola-Perkins [187] | wrong population |
| Stewart et al. [188] | wrong intervention |
| Stewart et al. [189] | wrong study design |
| Straatman et al. [190] | wrong intervention |
| Swan [191] | criteria for inter-library loan not met |
| Taylor et al. [192] | wrong study design |
| Thelwell [193] | wrong intervention |
| Thew [194] | wrong outcomes |
| Tobin [195] | wrong population |
| Tomaszewska et al. [196] | wrong study design |
| Trammell [197] | wrong outcomes |
| Turner et al. [198] | wrong study design |
| Voelpel et al. [199] | wrong study design |
| Walsh [200] | wrong study design |
| Wheeler et al. [201] | wrong intervention |
| Williams et al. [202] | wrong outcomes |
| Wilson [203] | not available due to COVID-19 |
| Wilson [204] | not available due to COVID-19 |
| Wood et al [205] | no comparator |
| Young [206] | wrong reporting of outcomes |
| Zents et al. [207] | wrong population |
Appendix D. Summary of the Theoretical Frameworks and Results
- mechanism of action was stated and directly linked back to the intervention’s development before implementation; or
- proposal was offered for the intervention’s mechanism of action on the outcomes before the intervention was implemented; or
- mechanism of action was stated with a pre-specified assessment to distinguish the different co-interventions’ relative effects
- Grajfoner et al. [37] suggested that a benefit of dog-assisted interventions is “encouraging students to perceive counseling services as more accessible” & “therapy dogs represent a source of comfort, acceptance & de-stress” ([37] p. 2) with the study aimed to work out the relative influence of the dogs.
- Fiocco et al. [73] discussed the presence of therapy animal may act as a buffer of stress with no further expansion.
- Hall [75] applied Kolcaba’s Midrange Theory of Comfort [208] from patients to students. Suggested that students who reach transcendence (highest level of comfort) “would be empowered to rise above the challenges of nursing education” ([75] p. 203). Stating how & why dogs could help with achieving transcendence was not explicitly included.
- Hunt et al. [76] described the intervention of interest initially as a placebo control and in the discussion theorized the role of social support, community & sense of belonging.
- Shearer et al. [77] described the intervention of interest as an active control and in the discussion considered unconditional positive regard & social environment.
- Ward-Griffin et al. [78] suggested that therapy animals may act as a source of social support with no further expansion.
- Williams et al. [79] reported that therapy animals are trained to provide comfort, affection & can be calming with no further expansion.
- Banks et al. [72] discussed the benefits of canine interaction, for example the cognitive changes with reducing mind wandering & increasing sustained attention but did not explore how & why mental health outcomes would be improved.
| Anxiety as measured by: |
| STAI (regardless of subscale): negative change = anxiety decreases |
| HADS-anxiety subscale: negative change = anxiety decreases |
| Stress as measured by: |
| PSS: negative change = stress decreases |
| Depression as measured by: |
| BDI II: negative change = depression decreases |
| HADS-depression subscale: negative change = depression decreases |
| Mood/affect as measured by: |
| PANAS positive: negative change = positive mood decreases |
| PANAS negative: negative change = negative mood decreases |
| UMACL (depends on subscale): inference in paper was positive change = mood increases |
| Well-being as measured by: |
| WEMWBS: positive change = mental well-being increases |
| Subjective Happiness Scale: positive change = happiness increases |
| Total social support: positive change = total levels of support increases |
| SWLS (based on brackets): 5–9 = extremely dissatisfied; 15–19 = slightly dissatisfied; 20 = neutral; 21–25 = slightly satisfied; 26–30 = satisfied and as both groups in the same bracket that a negative score = satisfaction with life decreases |
| Author & Year | Sample Size | Outcome | Findings with Effect Measures & Statistical Test Used by Authors | p Value | Evidence Strength | Vote Count | Conclusions |
|---|---|---|---|---|---|---|---|
| Banks [72] 2018 | Randomised: n = 56 (n = 29 dog; n = 27 no-treatment control) Analysed: unclear | PANAS positive PANAS negative | Mean change after stressor; calculation by review. Positive mood (PANAS positive): Treatment: −4.51 No-treatment control: −3.48 Negative mood (PANAS negative): Treatment: 0.21 No-treatment control:−0.82 Mixed modal ANOVAs for change over time & if moderated by condition | Mood: PANAS positive: p > 0.05 (NS) for condition or time × condition PANAS negative: p > 0.05 (NS) for time, condition, time x condition | Overall weight: low | Mood (with stressor): PANAS positive & negative: Detrimental | Measurement occurred after a 10-min group free interaction single AAA session with a stressor applied before measurement (& sessions occurred during exam week). NS reduction in positive mood for both groups when condition or condition × time reviewed (treatment more than control). NS slight worsening of negative mood for treatment group. Where NS, no power calculation so unable to say if no true effect or if underpowered. |
| Binfet [35] 2017 | Randomised: n = 163 Analysed: n = 155 (n = 81therapy dog; n = 74 no-treatment control e.g., studying) | PSS Sense of Belonging in School | Mean change (SD) Stress (PSS): Treatment: −0.17 (0.03) No-treatment control: 0.02 (0.04) Well-being proxy (School belonging): Treatment: 0.1 (0.03) No-treatment control: −0.05 (0.03) Used MANCOVA controlling for gender (inferred same approach with ANCOVA) | ANCOVA over time: treatment group vs. control Immediate: Stress: p < 0.001 Well-being: p = 0.002 (<0.05) 2-week f/up: NS | Overall weight: medium | Stress: Beneficial Well-being: Beneficial | Compared to control, statistical significance with improved scores were shown for both perceived stress (reduced) & school belonging (increased) for the treatment group (a 20-min group free interaction single AAT session). NS difference between the two groups at 2-week follow-up but no power calculation so unable to say if truly ‘no effect’ or if underpowered. |
| Fiocco [73] 2017 | Randomised: n = 61 (n = 31 dog; n = 30 no-treatment control) Analysed: unclear | PANAS positive PANAS negative | Mean change inferred post minus pre after stressor (SD) Positive mood (PANAS positive): Treatment: −0.35 (6.66) No-treatment control: −4.37 (7.15) Negative mood (PANAS negative): Treatment: 2.29 (5.62) No-treatment control: 0.6 (6.1) ANCOVA controlling for baseline effect | Mood: PANAS positive p = 0.08 (NS) PANAS negative p = 0.61 (NS) | Overall weight: medium | Mood (with stressor): PANAS positive: Beneficial PANAS negative: Detrimental | For this individual free interaction 10-min single AAA session and subsequent stressor: Positive mood reduces (NS) for both but was worse for control. Negative mood was worse (NS) for both groups but more so for treatment group. Where NS, no power calculation so unable to say if no true effect or if underpowered. |
| Gebhart [74] 2019 | Randomised: n = 72 Analysed: n = 57 (n = 12 therapy dog; n = 15 no-treatment control (unstructured free hour); n = 14 body percussion; n = 16 mandala painting) | STAI-S | Median change trends reported as relevant results only presented in graphs Anxiety (STAI-S): Normal day: Treatment: reduction No-treatment control: small increase Prior to exam (stressor): Treatment: small reduction No-treatment control: an increase Wilcoxon signed-rank tests | Anxiety: Normal day p < 0.01 for therapy dog; NS for control Exam day p = NS for both therapy dog & control | Overall weight: high | Anxiety (without stressor): Beneficial | On a normal day (after two structured group AAT interventions lasting 45–60 min of unknown time between sessions) a statistically significant reduction in anxiety was found in therapy dog group. On an exam day (after three structured group AAT interventions lasting 45–60 min of unknown time between sessions) NS difference in anxiety was found in both therapy dog & control group. Where NS, no power calculation so unable to say if no true effect or if underpowered. |
| Grajfoner [37] 2017 | Randomised: Unclear; n = 132 recruited Analysed: n = 132 (n = 45 dog with handler; n = 46 handler only (HO) & n = 41 dog only (DO)) | STAI WEMWBS UMACL | Mean change (SD NR) Anxiety (STAI): Treatment: −13.73 HO attention control: −2.02 Well-being (WEMWBS): Treatment: 2.36 HO attention control: −0.94 Mood (UMACL): Treatment: 2.62 HO attention control: −0.026 MANOVA across 3 groups with condition as between-participants factor & f/up Bonferroni tests | Anxiety: p < 0.001 Well-being: p < 0.001 Mood: NS (exact p value NR) | Overall weight: medium | Anxiety: Beneficial Well-being: Beneficial Mood: Beneficial | A free interaction 20-min single group AAA session demonstrated: (1) anxiety scores reduced for both dog with handler & control groups which was statistically significant in favour of the dog with handler group (2) statistically significant improvement in well-being in favour of the dog with handler group (3) NS significant improvement in mood (increased in dog with handler group with reduction in control) Where NS, no power calculation so unable to say if no true effect or if underpowered. |
| Hall [75] 2018 | Randomised: Unclear; n = 109 recruited Analysed: n = 77 (n = 41 dog; n = 36 no-treatment control) | HADS | Mean change; calculation by review Anxiety (HADS anxiety): Treatment: −2.68 No-treatment control: −1.67 Independent t-test on pre- then post-scores by authors Depression (HADS depression): non-normal distribution & only given mean; Treatment: −0.93; No-treatment control: −1.55 | Anxiety: p = 0.076 (NS) between pre-scores for control & dog. p = 0.008 between post-scores for control & dog Depression: NR (non-normal distribution) | Overall weight: medium | Anxiety: Beneficial Depression: No effect | A mixture of group/individual dog AAA sessions with free interaction & numerous opportunities to interact over 15–16 weeks, showed a statistically significant reduction in anxiety in favour of dogs on post-score (not controlled for pre-score; however, if evenly randomised can be appropriate [209]). Caution: depression scores not normally distributed (only means provided personal communication [81]). Appears to reduce in both groups: more in control group. |
| Hunt [76] 2018 | Randomised: n = 119 Analysed: Unclear regarding final number analysed: (study break with dog; no-treatment control; mindfulness training alone; yoga alone; combined mindfulness & yoga training) | STAI-S PANAS positive PANAS negative | Mean change trends from baseline to after 1st session reported as relevant results only presented in graphs. Authors only report statistical results for after stressor. Anxiety (STAI-S): Treatment: reduction No-treatment control: an increase Positive mood (PANAS positive): Means NR Negative mood (PANAS negative): Treatment: reduction No-treatment control: no change Repeated measure ANOVA of condition across time & after each time-point; then pairwise comparisons | Anxiety (dog vs. control): No stressor: NS p = 0.07 by 4th session Stressor: anxiety higher p < 0.05 Mood: No stressor: PANAS positive: NS; PANAS negative: control worse mood over time than dog group (p ≤ 0.01); but NS by 4th session. Stressor: NS (p < 0.1) | Overall weight: medium | Anxiety: Beneficial Mood: PANAS positive: unable to assess PANAS negative: Beneficial | Group AAA sessions with free interaction of NR length once a week for 4 weeks with a dog (with games, icebreakers & snacks) demonstrated: (1) anxiety levels reduced for dog group compared to control (statistical significance only reported for 4th session = NS) (2) Control had statistically significant worse negative mood over time compared to dog group but not by 4th session After a stressor (1–3 weeks after interventions had finished), dog group had statistically significant worsening of anxiety levels & NS higher negative mood compared to control. Positive mood was NR. Where NS, no power calculation so unable to say if no true effect or if underpowered. |
| Meola [80] 2017 | Randomised: n = 20 Analysed: n = 19 (unclear split between EALS & control) | STAI-S | Mean change; calculation by review Anxiety (STAI): Treatment: −0.16 No-treatment control: 0.09 Split plot MANOVA for pre- & post-test | Anxiety: p = 0.274 (NS) | Overall weight: medium | Anxiety: Beneficial | Individual 1-h structured AAT/AAE session with a horse demonstrated a small reduction in anxiety when measured up to 1 month after intervention (NS but underpowered). |
| Shearer [77] 2016 | Randomised: n = 74 Analysed: Numbers analysed vary at each time-point: ‘destress with dog’; no-treatment control; mindfulness meditation | STAI-S BDI II | Mean change; calculation by review Anxiety (STAI-S): No stressor: (1st session minus pre) Treatment: −15.25 No-treatment control: −3.5 With stressor (post minus pre): Treatment: 3.1 No-treatment control: 1.79 Depression (BDI II): interpreted as with stressor Treatment: −1.58; No-treatment control: −0.47 Repeated-measures ANOVA change over time, then planned comparisons (paired sample t-tests) | Anxiety: No stressor: control significantly different (p = NR) across time for anxiety when compared to dog group. Stressor: NS Depression: No stressor NR Stressor: NS | Overall weight: low | Anxiety: Beneficial Depression: Beneficial | Group free interaction AAA sessions with a dog including games & snacks lasting for 1 h/week for 4 weeks had statistically significant lower anxiety scores than control. After a stressor (1–2 weeks after interventions finished), anxiety levels increased in both groups but greater in treatment group (NS). Depression scores decreased in both groups with treatment group reducing more (NS) than control. Where NS, no power calculation so unable to say if no true effect or if underpowered. |
| Ward-Griffin [78] 2018 | Randomised: n = 357 Analysed: n = 246 (n = 122 dog; n = 124 wait-list control) | PSS PANAS positive PANAS negative SWLS Subjective Happiness Scale Medical Outcomes Social Support | Mean change; calculated by review Stress (PSS): Treatment: −0.11; Wait-list control: 0.06 Positive mood (PANAS positive): Treatment: −0.52; Wait-list control:−0.44 Negative mood (PANAS negative): Treatment: −0.5; Wait-list control: −0.27 Well-being proxies: Satisfaction with life (SWLS): Treatment: −0.08; Wait-list control: 0.03 Subjective Happiness Scale: Treatment: −0.01; Wait-list control: −0.03 Total Social Support: Treatment: 0.1; Wait-list control: −0.03 Repeated measures ANOVA (effect of time x condition) | Effect of time x condition p = 0.007 negative mood; p = 0.031 stress; p = 0.032 total social support (gender as a fixed factor no significant interaction between condition, time & gender) p values otherwise NS | Overall weight: medium | Stress: Beneficial Mood positive: Detrimental Mood negative: Beneficial Well-being: SWLS: Detrimental Happiness: No effect Total Social Support: Beneficial | Group free interaction single AAA session with dogs lasting up to 90 min with outcomes measured up to 24 h after delivery, had statistically significant reduction in stress, negative mood & amelioration of total social support compared to control. Positive mood reduced for both groups & slightly more in treatment group (NS). Well-being: Satisfaction with Life: both groups were in the extremely dissatisfied category at baseline. Scores reduced in dog (NS) & did not change category. Happiness levels essentially did not change. Total social support significantly increased in treatment group. Where NS, no power calculation so unable to say if no true effect or if underpowered. |
| Williams [79] 2018 | Randomised: n = 39 Analysed: n = 37 (n = 19 dog & n = 18 no-treatment control e.g., studying) | STAI-S&T | Mean change; calculation by review Anxiety (STAI-S&T): Treatment: 2.95 No-treatment control: 16.33 2-way mixed ANOVA, independent t-tests & Wilcoxon signed rank | Anxiety: p = 0.008 control had more anxiety than treatment group on exam day | Overall weight: medium | Anxiety (with stressor): Beneficial | For a 12-min inferred individual single AAA session delivered prior to an exam, anxiety levels increased for both groups with control having statistically significant higher levels of anxiety than dog. |
References
- Thorley, C. Not by Degrees: Not by Degrees: Improving Student Mental Health in UK’s Universities; IPPR: London, UK, 2017; Available online: https://www.ippr.org/publications/not-by-degrees (accessed on 2 February 2020).
- Bell, A. Paws for a Study Break: Running an Animal-Assisted Therapy Program at the Gerstein Science Information Centre. Partnership Can. J. Libr. Inf. Pr. Res. 2013, 8, 1. [Google Scholar] [CrossRef]
- Hughes, G.; Spanner, L. The University Mental Health Charter; Student Minds: Leeds, UK, 2019. [Google Scholar]
- Bethlehem, J. Applied Survey Methods: A Statistical Perspective Applied Survey Methods. 2009. Available online: http://www.applied-survey-methods.com/weight.html (accessed on 22 July 2020).
- Campbell, D. UK students waiting up to three months for mental health care. Guardian 2019, 11, 243. [Google Scholar]
- Crossman, M.K.; Kazdin, A.E. Animal visitation programs in colleges and universities: An efficient mode for reducing student stress. In Handbook on Animal-Assisted Therapy: Foundations and Guidelines for Animal-Assisted Interventions, 4th ed.; Fine, A.H., Ed.; Elsevier Science & Technology: Alpharetta, GA, USA, 2015; pp. 333–337. [Google Scholar]
- American Veterinary Medical Association (AVMA). Animal-assisted interventions: Definitions. 2020. Available online: https://www.avma.org/policies/animal-assisted-interventions-definitions (accessed on 26 January 2020).
- International Association of Human-Animal Interaction (IAHAIO). The IAHAIO Definitions for Animal-Assisted Intervention and Guidelines for Wellness of Animals Involved in AAIs. 2018. Available online: https://iahaio.org/wp/wp-content/uploads/2018/04/iahaio_wp_updated-2018-final.pdf (accessed on 4 May 2020).
- The Society for Companion Animal Studies (SCAS). Animal Assisted Interventions: SCAS Code of Practice for the UK. 2019. Available online: http://www.scas.org.uk/wp-content/uploads/2019/08/SCAS-AAI-Code-of-Practice-August-2019.pdf (accessed on 5 May 2020).
- Kamioka, H.; Okada, S.; Tsutani, K.; Park, H.; Okuizumi, H.; Handa, S.; Oshio, T.; Park, S.-J.; Kitayuguchi, J.; Abe, T.; et al. Effectiveness of animal-assisted therapy: A systematic review of randomized controlled trials. Complement. Ther. Med. 2014, 22, 371–390. [Google Scholar] [CrossRef]
- Nimer, J.; Lundahl, B. Animal-Assisted Therapy: A Meta-Analysis. Anthrozoös 2007, 20, 225–238. [Google Scholar] [CrossRef]
- Bert, F.; Gualano, M.R.; Camussi, E.; Pieve, G.; Voglino, G.; Siliquini, R. Animal assisted intervention: A systematic review of benefits and risks. Eur. J. Integr. Med. 2016, 8, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Brelsford, V.L.; Meints, K.; Gee, N.R.; Pfeffer, K. Animal-Assisted Interventions in the Classroom—A Systematic Review. Int. J. Environ. Res. Public Health 2017, 14, 669. [Google Scholar] [CrossRef] [PubMed]
- Shen, R.Z.; Xiong, P.; Chou, U.I.; Hall, B.J. “We need them as much as they need us”: A systematic review of the qualitative evidence for possible mechanisms of effectiveness of animal-assisted intervention (AAI). Complement. Ther. Med. 2018, 41, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Morrison, M.L. Health Benefits of Animal-Assisted Interventions. Complement. Health Pr. Rev. 2007, 12, 51–62. [Google Scholar] [CrossRef]
- Odendaal, J.; Meintjes, R. Neurophysiological Correlates of Affiliative Behaviour between Humans and Dogs. Veter-J. 2003, 165, 296–301. [Google Scholar] [CrossRef]
- Polheber, J.P.; Matchock, R.L. The presence of a dog attenuates cortisol and heart rate in the Trier Social Stress Test compared to human friends. J. Behav. Med. 2014, 37, 860–867. [Google Scholar] [CrossRef]
- Stasi, M.; Amati, D.; Costa, C.; Resta, D.; Senepa, G.; Scarafioiti, C.; Aimonino, N.; Molaschi, M. Pet-therapy: A trial for institutionalized frail elderly patients. Arch. Gerontol. Geriatr. 2004, 38, 407–412. [Google Scholar] [CrossRef]
- Lai, N.M.; Chang, S.M.W.; Ng, S.S.; Tan, S.L.; Chaiyakunapruk, N.; Stanaway, F. Animal-assisted therapy for dementia. Cochrane Database Syst. Rev. 2019, 11. [Google Scholar] [CrossRef]
- Ein, N.; Li, L.; Vickers, K. The effect of pet therapy on the physiological and subjective stress response: A meta-analysis. Stress Health 2018, 34, 477–489. [Google Scholar] [CrossRef]
- Crump, C.; Derting, T.L. Effects of pet therapy on the psychological and physiological stress levels of first-year female undergraduates. N. Am. J. Psychol. 2015, 17, 575–590. [Google Scholar]
- Beck, A.M. The biology of the human-animal bond. Anim. Front. 2014, 4, 32–36. [Google Scholar] [CrossRef]
- Bartley, M. Health Inequalities: An Introduction to Theories, Concepts and Methods, 2nd ed.; Blackwell Publishing Ltd.: Cambridge, UK, 2004. [Google Scholar]
- Cobb, S. Social Support as a Moderator of Life Stress. Psychosom. Med. 1976, 38, 300–314. [Google Scholar] [CrossRef]
- Fine, A.H.; Beck, A.M. Understanding Our Kinship with Animals: Input for Health Care Professionals Interested in the Human–Animal Bond. In Handbook on Animal-Assisted Therapy: Foundations and Guidelines for Animal-Assisted Interventions, 4th ed.; Fine, A.H., Ed.; Elsevier Science & Technology: Philadelphia, PA, USA, 2015; pp. 3–10. [Google Scholar]
- Wilson, E. Biophilia: The Human Bond with Other Species; Harvard University Press: Cambridge, MA, USA, 1986. [Google Scholar]
- Hudson, B.; Ogden, J.; Whiteley, M. Randomized controlled trial to compare the effect of simple distraction interventions on pain and anxiety experienced during conscious surgery. Eur. J. Pain 2015, 19, 1447–1455. [Google Scholar] [CrossRef]
- Newcastle University. Bessie Gives Students Time to Paws for Thought; Newcastle University Press Office. 2019. Available online: https://www.ncl.ac.uk/press/articles/latest/2019/10/borrowbessie/ (accessed on 28 January 2020).
- Spencer, C. Dogs help relieve Swansea students’ exam stress. BBC News. 2019. Available online: https://www.bbc.co.uk/news/uk-wales-47074779 (accessed on 5 May 2020).
- Coughlan, S. Stress-busting dogs on university staff. BBC News. 2019. Available online: https://www.bbc.co.uk/news/education-48097050 (accessed on 5 May 2020).
- University of Sheffield. Pet Therapy Day 2018. 2018. Available online: https://www.sheffield.ac.uk/sss/news/pet-therapy-2018-1.804532 (accessed on 5 May 2020).
- Newcastle University. Wellbeing Initiatives: Borrow Bessie. 2020. Available online: https://www.ncl.ac.uk/wellbeing/newseventsandprojects/initiatives/#borrowbessie (accessed on 11 May 2020).
- Reynolds, J.A.; Rabschutz, L. Studying for Exams Just Got More Relaxing—Animal-Assisted Activities at the University of Connecticut Library. Coll. Undergrad. Libr. 2011, 18, 359–367. [Google Scholar] [CrossRef]
- Daltry, R.M.; Mehr, K.E. Therapy Dogs on Campus: Recommendations for Counseling Center Outreach. J. Coll. Stud. Psychother. 2015, 29, 72–78. [Google Scholar] [CrossRef]
- Binfet, J.-T. The Effects of Group-Administered Canine Therapy on University Students’ Wellbeing: A Randomized Controlled Trial. Anthrozoös 2017, 30, 397–414. [Google Scholar] [CrossRef]
- Crossman, M.K.; Kazdin, A.E.; Knudson, K. Brief Unstructured Interaction with a Dog Reduces Distress. Anthrozoös 2015, 28, 649–659. [Google Scholar] [CrossRef]
- Grajfoner, D.; Harte, E.; Potter, L.M.; McGuigan, N. The Effect of Dog-Assisted Intervention on Student Well-Being, Mood, and Anxiety. Int. J. Environ. Res. Public Health 2017, 14, 483. [Google Scholar] [CrossRef] [PubMed]
- Parbery-Clark, C.; McColl, E.; Tanner, L. Animal-Assisted Interventions for the Improvement of Mental Health Outcomes in Higher Education Students: Prospero Form. 2020. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=186541 (accessed on 26 June 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Page, M.J.; Welch, V.A. Cochrane Handbook of Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Cummins, I. The Impact of Austerity on Mental Health Service Provision: A UK Perspective. Int. J. Environ. Res. Public Health 2018, 15, 1145. [Google Scholar] [CrossRef]
- Hart, L.A.; Yamamoto, M. Recruiting Psychosocial Health Effects of Animals for Families and Communities: Transition to Practice. In Handbook on Animal-Assisted Therapy: Foundations and Guidelines for Animal-Assisted Interventions, 4th ed.; Fine, A.H., Ed.; Elsevier Science & Technology: Philadelphia, PA, USA, 2015; pp. 53–72. [Google Scholar]
- American Veterinary Medical Association (AVMA). Service Animals. 2020. Available online: https://www.avma.org/resources-tools/avma-policies/service-animals (accessed on 15 July 2020).
- The Society for Companion Animal Studies (SCAS). Therapy/Assistance Dogs. 2013. Available online: http://www.scas.org.uk/animal-assisted-interventions/therapy-assistance-dogs/ (accessed on 15 July 2020).
- American Veterinary Medical Association (AVMA). Service, Emotional Support and Therapy Animals. 2020. Available online: https://www.avma.org/resources-tools/animal-health-welfare/service-emotional-support-and-therapy-animals (accessed on 15 July 2020).
- Department for Education. Further Education Courses and Funding. 2020. Available online: https://www.gov.uk/further-education-courses (accessed on 21 June 2020).
- Animal Assisted Intervention International (AAII). Animal Assisted Intervention International Standards of Practice: Animal Assisted Intervention International (AAII). 2019. Available online: https://aai-int.org/wp-content/uploads/2019/02/AAII-Standards-of-Practice.pdf (accessed on 4 May 2020).
- Animal Assisted Intervention International (AAII). Animal Assisted Intervention. 2020. Available online: https://aai-int.org/aai/animal-assisted-intervention/ (accessed on 24 April 2020).
- Santaniello, A.; Die, F.; Carratu, R.C.; Amato, A.; Fioretti, A.; Menna, L.F. Methodological and terminalogical issues in animal-assisted interventions: An umbrella reviews of systematic reviews. Animals 2020, 10, 759. [Google Scholar] [CrossRef] [PubMed]
- Horn, B.; Balk, J.; Gold, J.I. Revisiting the Sham: Is It all Smoke and Mirrors? Evidence-Based Complement. Altern. Med. 2011, 2011, 842767. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; CPP Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 386–396. [Google Scholar] [CrossRef]
- Nightline Association. Depressed, Anxious, Lonely and Homesick: Study Reveals Darker Side to Student Life. 2013. Available online: https://www.nightline.ac.uk/2013/06/depressed-anxious-lonely-and-homesick-study-reveals-darker-side-to-student-life/ (accessed on 11 May 2020).
- The Insight Network. University Student Mental Health Survey 2018, London. 2019. Available online: https://uploads-ssl.webflow.com/561110743bc7e45e78292140/5c7d4b5d314d163fecdc3706_Mental%20Health%20Report%202018.pdf (accessed on 15 January 2020).
- The Insight Network. University Student Mental Health Survey 2020, London. 2020. Available online: https://www.diginbox.com/go/files/Mental%20Health%20Report%202019.pdf (accessed on 11 May 2020).
- Anxiety and Depression Association of America (ADAA). Understanding the Facts: Stress: Anxiety and Depression Association of America (ADAA). 2018. Available online: https://adaa.org/understanding-anxiety/related-illnesses/stress (accessed on 24 April 2020).
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding randomised controlled trials. Arch. Dis. Child. 2005, 90, 840–844. [Google Scholar] [CrossRef]
- Petticrew, M.; Roberts, H. Systematic Reviews in the Social Sciences: A Practical Guide; Blackwell LTD.: Oxford, UK, 2006. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Haar, M. Random.org: Randomness and Integrity Services Ltd. 1998. Available online: https://www.random.org/analysis/ (accessed on 29 May 2020).
- Grossetta Nardini, H.K.; Wang, L. The Yale MeSH Analyzer; Internet; Cushing/Whitney Medical Library: New Haven, CT, USA, 2017; Available online: http://mesh.med.yale.edu/ (accessed on 17 March 2020).
- Reuters, T. Endnote X9 Thomson Reuters. J. Electron. Resour. Med Libr. 2019, 10, 1691963. [Google Scholar]
- Hoffman, T.; Glasziou, P.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; Lamb, S.E. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]
- Whiting, P.; Savovic, J.; Higgin, J.; Caldwell, D.; Reeves, B.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R. Robis: Tool to Assess Risk of Bias in Systematic Reviews—Guidance on How to Use ROBIS. 2015. Available online: https://www.bristol.ac.uk/media-library/sites/social-community-medicine/robis/robisguidancedocument.pdf (accessed on 1 January 2020).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- RoB2 Development Group. Revised Cochrane Risk-of-Bias Tool for Randomized Trials (RoB2). 2019. Available online: https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials (accessed on 24 April 2020).
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the conduct of narrative synthesis in systematic reviews. In A Product from the ESRC Methods Programme; Lancaster Universit: Lancaster, UK, 2006. [Google Scholar] [CrossRef]
- Gough, D. Weight of Evidence: A framework for the appraisal of the quality and relevance of evidence. Res. Pap. Educ. 2007, 22, 213–228. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Banks, J.B.; McCoy, C.; Trzcinski, C. Examining the impact of a brief human-canine interaction on stress and attention. Hum.-Anim. Interact. Bull. 2018, 6, 1. [Google Scholar]
- Fiocco, A.J.; Hunse, A.M. The Buffer Effect of Therapy Dog Exposure on Stress Reactivity in Undergraduate Students. Int. J. Environ. Res. Public Health 2017, 14, 707. [Google Scholar] [CrossRef]
- Gebhart, V.; Buchberger, W.; Klotz, I.; Neururer, S.; Rungg, C.; Tucek, G.; Zenzmaier, C.; Perkhofer, S. Distraction-focused interventions on examination stress in nursing students: Effects on psychological stress and biomarker levels. A randomized controlled trial. Int. J. Nurs. Pr. 2019, 26, e12788. [Google Scholar] [CrossRef]
- Hall, D. Nursing Campus Therapy Dog: A Pilot Study. Teach. Learn. Nurs. 2018, 13, 202–206. [Google Scholar] [CrossRef]
- Hunt, M.; Al-Braiki, F.; Dailey, S.; Russell, R.; Simon, K. Mindfulness Training, Yoga, or Both? Dismantling the Active Components of a Mindfulness-Based Stress Reduction Intervention. Mindfulness 2018, 9, 512–520. [Google Scholar] [CrossRef]
- Shearer, A.; Hunt, M.; Chowdhury, M.; Nicol, L. Effects of a brief mindfulness meditation intervention on student stress and heart rate variability. Int. J. Stress Manag. 2016, 23, 232–254. [Google Scholar] [CrossRef]
- Ward-Griffin, E.; Klaiber, P.; Collins, H.K.; Owens, R.L.; Coren, S.; Chen, F.S. Petting away pre-exam stress: The effect of therapy dog sessions on student well-being. Stress Health 2018, 34, 468–473. [Google Scholar] [CrossRef]
- Williams, C.; Emond, K.; Maynord, K.; Simpkins, J.; Stumbo, A.; Terhaar, T. An animal-assisted intervention’s influence on graduate students’ stress and anxiety prior to an examination. OALib 2018, 05, e4831. [Google Scholar] [CrossRef]
- Meola, C. The Effects of an Equine Assisted Learning Supervision Intervention on Counselors’-in-Training Performance Anxiety, Counseling Self-Efficacy, and Supervisory Working Alliance. Ph.D. Thesis, East Carolina University, Greene County, NC, USA, 2017. Dissertation Abstracts International: Section B: The Sciences and Engineering. [Google Scholar]
- Hall, D. Nursing campus therapy dog: A pilot study. Sci. Driect 2018, 5, 142. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Cochrane Handbok for Systematic Reviews of Interventions; John Wiley and Sons: Chichester, UK, 2016. [Google Scholar]
- de Bruin, M. Risk of bias in randomised controlled trials of health behaviour change interventions: Evidence, practices and challenge. Psychol. Health 2015, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Barratt, H.; Kirwan, M.; Shantikumar, S. Biases and Confounding: Health Knowledge. 2018. Available online: https://www.healthknowledge.org.uk/public-health-textbook/research-methods/1a-epidemiology/biases (accessed on 24 July 2020).
- Gosall, N.; Gosall, G. The Doctor’s Guide to Critical Appraisal, 4th ed.; Pastest Ltd.: Cheshire, UK, 2015. [Google Scholar]
- O’Haire, M.E.; Guérin, N.A.; Kirkham, A.C. Animal-Assisted Intervention for trauma: A systematic literature review. Front. Psychol. 2015, 6, 1121. [Google Scholar] [CrossRef] [PubMed]
- Walmsley, A.L.E.; Brown, M.C. What is power? Statistics Teacher. 2017. Available online: https://www.statisticsteacher.org/2017/09/15/what-is-power/ (accessed on 24 July 2020).
- Fogg, B.J. A behavior model for persuasive design—Persuasive 09. In Proceedings of the 4th International Conference on Persuasive Technology, Claremont, CA, USA, 26–29 April 2009; pp. 1–7. [Google Scholar]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.; Fitzpatrick, R.; Haines, A.; Kinmonth, A.L.; Sandercock, P.; Spiegelhalter, D.; Tyrer, P. Framework for design and evaluation of complex interventions to improve health. BMJ 2000, 321, 694–696. [Google Scholar] [CrossRef] [PubMed]
- Bonell, C.; Jamal, F.; Melendez-Torres, G.; Cummins, S. ‘Dark logic’: Theorising the harmful consequences of public health interventions. J. Epidemiol. Community Health 2015, 69, 95–98. [Google Scholar] [CrossRef]
- Adamle, K.N.; Riley, T.A.; Carlson, T. Evaluating college interest in pet therapy. J. Am. Coll. Health. 2009, 57, 545–548. [Google Scholar] [CrossRef]
- Adams, A.C.; Sharkin, B.S.; Bottinelli, J.J. The role of pets in the lives of college students: Implications for college counsellors. J. College Stud. Psychother. 2017, 31, 306–324. [Google Scholar] [CrossRef]
- Adams, T.; Clark, C.; Crowell, V.; Duffy, K.; Green, M. The mental health benefits of having dogs on college campuses. Mod. Psychol. 2017, 22, 7. [Google Scholar]
- Alonso, Y. Effects of pets on human health: Is there a correlation? Gesundheitswesen 1999, 61, 45–49. [Google Scholar] [PubMed]
- Anderson, D. The Effect of Animal-Assisted Therapy on Nursing Student Anxiety. Ph.D. Thesis, University of Kansas, Lawrence, KS, USA, 2018. Dissertation Abstracts International Section: Humanities and Social Sciences. [Google Scholar]
- Anonymous. DM-style program caters to behavioral needs of college students. Dis Manag Advis. 2004, 10, 55–56. [Google Scholar]
- Anonymous. Dog therapy helps reduce stress in students. Vet. Rec. 2019, 184, 541. [Google Scholar] [CrossRef]
- Ashton, L. Intrigued about equine modalities. J. Psychosoc. Nurs. Ment. Health Serv. 2011, 49, 16. [Google Scholar] [CrossRef]
- Baghain, N.; Sari, A.A.; Shati, M.; Fallahzadeh, H. Evaluation of students’ mental and social health promotion educational programs: A systematic review. J. Edu. Health Promot. 2019, 8, 258. [Google Scholar] [CrossRef]
- Bajorek, K. The effects of pet therapy on undergraduate nursing students’ perceived stress and exam performance. Honors Thesis, Western Michigan University, Kalamazoo, MI, USA, 2014. [Google Scholar]
- Barker, S.; Barker, T.; McCain, N.L.; Schubert, C.M. A randomized cross-over exploratory study of the effect of visiting therapy dogs on college student stress before final exams. Anthrozoös 2016, 29, 35–46. [Google Scholar] [CrossRef]
- Barker, S.; Barker, R.T.; McCain, N.L.; Schubert, C.M. The effect of a canine-assisted activity on college student perceptions of family supports and current stressors. Anthrozoös 2017, 30, 595–606. [Google Scholar] [CrossRef]
- Barker, S.; Barker, R.T.; Schubert, C. Therapy dogs on campus: A counseling outreach activity for college students preparing for final exams. J. Coll. Couns. 2017, 20, 278–288. [Google Scholar] [CrossRef]
- Barlow, R.; DeMarni Cromer, L.; Caron, H.P.; Freyd, J.J. Comparison of normative and diagnosed dissociation on attachment to companion animals and stuffed animals. Psychol Trauma. 2012, 4, 501–506. [Google Scholar] [CrossRef]
- Basil, B.; Mathews, M. Human and animal health: Strengthening the link—Methodological concerns about animal facilitated therapy with dolphins. BMJ 2005, 331, 1407. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Behnke, M.; Olson, S. Knowing is half the battle. Lab. Anim. 2019, 48, 69–70. [Google Scholar] [CrossRef]
- Beutler, L.E.; Crago, M. Psychotherapy Research: An International Review of Programmatic Studies; American Psychological Association: Washington, DC, USA, 1991. [Google Scholar]
- Biery, M.J. Riding and the handicapped. Vet. Clin. N. Am. Small Anim. Pract. 1985, 15, 345–354. [Google Scholar] [CrossRef]
- Binfet, J.-T.; Passmore, H.-A. Hounds and homesickness: The effects of an animal-assisted therapeutic intervention for first-year university students. Anthrozoös 2016, 29, 441–454. [Google Scholar] [CrossRef]
- Binfet, J.-T.; Passmore, H.-A.; Cebry, A.; Struik, K.; Mckay, C. Reducing university students’ stress through a drop-in canine-therapy program. J. Ment. Health. 2018, 27, 197–204. [Google Scholar] [CrossRef]
- Binfet, J.-T.; Trotman, M.L.; Henstock, H.D.; Silas, H. J Reducing the affective filter: Using Canine Assisted Therapy to support international university students’ English language development. BC TEAL J. 2016, 1, 18. [Google Scholar] [CrossRef]
- Bjick, M. The Effects of a Therapy Animal on College Student Stress and Arousal. In Social Work Master’s Clinical Research Paper; St Catherine University & University of St. Thomas: St. Paul, MN, USA, 2013. [Google Scholar]
- Blender, J.A. A Multimodal Investigation of the Use of Animal-Assisted Therapy in a Clinical Interview. Ph.D. Thesis, University of Rochester, Rochester, NY, USA, 2010. Dissertation Abstracts International: Section B: The Sciences and Engineering. [Google Scholar]
- Broeyer, L.; Chanson, P.F.; Durrenberger, Y. Educational meetings: “crisis intervention”. “Catastrophe … that concerns me”. Krankenpfl.—Soins Infirm. 1990, 83, 70–71. [Google Scholar]
- Buttelmann, D.; Rompke, A.-K. Anxiety-reducing effect: Dog, fish and plant in direct comparison. Anthrozoös 2014, 27, 267–277. [Google Scholar] [CrossRef]
- Chakales, P.A.; Locklear, J.; Wharton, T. Medicine and Horsemanship: The Effects of equine-assisted activities and therapies on stress and depression in medical students. Cureus 2020, 12, e6896. [Google Scholar] [CrossRef]
- Chramouleeswaran, S.; Russell, P.S. Complementary psychosocial interventions in child and adolescent psychiatry: Pet assisted therapy. Indian J. Psychol. Med. 2014, 36, 4–8. [Google Scholar] [CrossRef]
- Cieslak, E.J. Animal-Assisted Therapy and the Development of an Early Working Alliance: The Use of Dogs in Therapy with Young Adults. Ph.D. Thesis, University of Wisconsin-Madison, Madison, WI, USA, 2001. Dissertation Abstracts International: Section B: The Sciences and Engineering. [Google Scholar]
- ClinicalTrials.gov. National Library of Medicine. Identifier: NCT02758886. Pet Your Stress Away Study. 2016. Available online: https://clinicaltrialsgov/show/NCT02758886 (accessed on 31 July 2020).
- ClinicalTrials.gov. National Library of Medicine. Identifier: NCT03704779. Effectiveness of a Multimodal Mindfulness Program to Alleviate Graduate Student Stress. 2018. Available online: https://clinicaltrialsgov/show/NCT03704779 (accessed on 31 July 2020).
- ClinicalTrials.gov. National Library of Medicine. Identifier: NCT03530943. Pet Partners for Promotion of Academic Life Skills. 2018. Available online: https://clinicaltrialsgov/show/NCT03530943 (accessed on 31 July 2020).
- ClinicalTrials.gov. National Library of Medicine. Identifier: NCT04200612. The Therapeutic Effects of Equine-Assisted Psychotherapy. 2019. Available online: https://clinicaltrialsgov/show/NCT04200612 (accessed on 31 July 2020).
- Colarelli, S.M.; McDonald, A.; Christensen, M.S.; Honts, C. A companion dog increases prosocial behavior in work groups. Anthrozoös. 2017, 30, 77–89. [Google Scholar] [CrossRef]
- Coleman, J.A.; Green, B.; Garthe, R.C.; Worthington, E.L.; Barker, S.; Ingram, K.M. The Coleman Dog Attitude Scale (C-DAS): Development, refinement, validation, and reliability. Appl. Anim. Behav. Sci. 2016, 176, 77–86. [Google Scholar] [CrossRef]
- Crago, L.; Leeder, J. Animal magic. University & College Counselling. 2014. Available online: https://17d8607e-a6ae-496b-96bd-48b9899bdf1a.filesusr.com/ugd/f89e47_3f02c88da55949deb740c5dae5b72407.pdf (accessed on 31 July 2020).
- Delgado, C.; Toukonen, M.; Wheeler, C. Effect of canine play interventions as a stress reduction strategy in college students. Nurse Educ. 2018, 43, 149–153. [Google Scholar] [CrossRef]
- Dell, C.A.; Chalmers, D.; Gillett, J.; Rohr, B.; Nickel, C.; Campbell, L.; Hanoski, R.; Haguerud, J.; Husband, A.; Stephenson, C.; et al. PAWSing student stress: A pilot evaluation study of the St. John Ambulance Therapy Dog program on three university campuses in Canada. Can. J. Couns. Psychother. 2015, 49, 332–359. [Google Scholar]
- Dhooper, M.K. Animal-Assisted Therapy: The Effects of the Presence of a Trained Therapy Dog on Group Anxiety Management Training. Ph.D. Thesis, University of South Dakota, Vermillion, SD, USA, 2003. Dissertation Abstracts International: Section B: The Sciences and Engineering. [Google Scholar]
- Dluzynski, J.L. A Quantitative Assessment of Test Anxiety and Human-Animal Interaction in College Students. Psy.D. Dissertation, ProQuest Dissertations Publishing. Michigan School of Professional Psychology, Farmington Hills, MI, USA, 2017. [Google Scholar]
- Duffey, T. Letter from the editor. J. Creat. Ment. Health. 2014, 9, 317. [Google Scholar] [CrossRef]
- Flaherty, L.T. School-based interventions as part of the therapeutic alliance. Adolesc. Psychiatry. 2012, 2, 105–106. [Google Scholar]
- Folse, E.B.; Minder, C.C.; Aycock, M.J.; Santana, R.T. Animal-assisted therapy and depression in adult college students. Anthrozoös 1994, 7, 188–194. [Google Scholar] [CrossRef]
- Frederick, K.E. Understanding the Impact of Equine-Assisted Learning on Levels of Hope in at-Risk Adolescents. Ph.D. Thesis, Baylor University, Waco, TX, USA, 2012. Dissertation Abstracts International Section A: Humanities and Social Sciences. [Google Scholar]
- Frederick, K.E.; Ivey Hatz, J.; Lanning, B. Not Just Horsing Around: The Impact of Equine-Assisted Learning on Levels of Hope and Depression in At-Risk Adolescents. Community Ment. Health J. 2015, 51, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, E.; Locker, B.Z.; Lockwood, R. Perception of animals and cardiovascular responses during verbalization with an animal present. Anthrozoös 1993, 6, 115–134. [Google Scholar] [CrossRef]
- Gonzalez-Ramirez, M.T.; Landaverde-Molina, O.D.; Morales-Rodriguez, D.; Landero-Hernandez, R. Speech anxiety management workshop assisted by therapy dogs. Ansiedad y Estres. 2016, 22, 5–10. [Google Scholar]
- Goodkind, J.; LaNoue, M.; Lee, C.; Freeland, L.; Freund, R. Feasibility, acceptability, and initial findings from a community-based cultural mental health intervention for American Indian youth and their families. J. Community Psychol. 2012, 40, 381–405. [Google Scholar] [CrossRef] [PubMed]
- Gress, K. Animals helping people. People helping animals. Interview by Shirley A. Smoyak. J. Psychosoc. Nurs. Ment. Health Serv. 2003, 41, 18–25. [Google Scholar]
- Haggerty, J.; Mueller, M. Animal-assisted stress reduction programs in higher education. Innov. High. Educ. 2017, 42, 379–389. [Google Scholar] [CrossRef]
- Hammer, C.J.; Bach-Gorman, A.R.; Berg, E.L. Equine-assisted counseling as an intervention for undergraduate female college students experiencing anxiety. J. Equine Vet Sc. 2019, 76, 118. [Google Scholar] [CrossRef]
- Hemingway, A.; Carter, S.; Callaway, A.; Kavanagh, E.; Ellis, S. An exploration of the mechanism of action of an equine-assisted intervention. Animals 2019, 9, 303. [Google Scholar] [CrossRef]
- Henry, C. The Psychological and Physiological Effects of Using a Therapy Dog in Mindfulness Training. Ph.D. Thesis, Utah State University, Logan, UT, USA, 2013. [Google Scholar]
- House, L.A.; Neal, C.; Backels, K. A doggone way to reduce stress: An animal assisted intervention with college students. Coll. Stud. J. 2018, 52, 199–204. [Google Scholar]
- Ishimura, I.; Komazawa, A. Positive psychological resources among Japanese university students with deep depression and anxiety: A study of flow experience and strength-awareness. Int. J. Psychiatry Clin. Pract. 2012, 16, 30–31. [Google Scholar]
- Jarolmen, J.; Patel, G. The effects of animal-assisted activities on college students before and after a final exam. J. Creat. Ment. Health. 2018, 13, 264–274. [Google Scholar] [CrossRef]
- Johnson, R.A. Promoting one health: The University of Missouri Research Center for Human/Animal Interaction. Mo Med. 2013, 110, 197–200. [Google Scholar] [PubMed]
- King, C.A. The Relationship between Human-Canine Attachment and College Adjustment. Ph.D. Thesis, Northern Illinois University, DeKalb, IL, USA, 2012. Dissertation Abstracts International Section A: Humanities and Social Sciences. [Google Scholar]
- Kobayashi, A.; Yamaguchi, Y.; Ohtani, N.; Ohta, M. The effects of touching and stroking a cat on the inferior frontal gyrus in people. Anthrozoös 2017, 30, 473–486. [Google Scholar] [CrossRef]
- Kronholz, J.F.; Freeman, V.F.; Mackintosh, R.C. Animal-Assisted Therapy: Best practices for college counseling. Ideas and Research You Can Use: VISTAS. 2015. Available online: https://www.counseling.org/docs/default-source/vistas/article_7525cd23f16116603abcacff0000bee5e7.pdf?sfvrsn=bbdb432c_8 (accessed on 31 July 2020).
- Kuzara, S.; Pendry, P.; Gee, N.R. Exploring the handler-dog connection within a university-based Animal-Assisted Activity. Animals 2019, 9, 402. [Google Scholar] [CrossRef] [PubMed]
- Lacoff, S.L.; Boris, M. Levinson: A Historical Perspective. A Focus on His Work Involving Animal-Assisted Psychotherapy. Doctoral Thesis, Miami Institute of Psychology, Miami, FL, USA, 1999. Dissertation Abstracts International: Section B: The Sciences and Engineering. [Google Scholar]
- Lauriente, T.; Kopp, D. Therapy Dogs on Campus: An Exploration of How Dog Therapy Services Affect Undergraduate Students’ Stress Levels. Ph.D. Thesis, Thompson River’s University, Kamloops, BC, Canada, 2018. [Google Scholar]
- Lephart, S.P.; Jennings, C.; Hamilton, A.N.C.; Hoellein, A.R. The paws that refresh us: Can animal-assisted therapy have an effect on exam performance in medical students? Glob. Adv. Health Med. 2018, 7, 203–204. [Google Scholar]
- Linden, M. Recognition and treatment of work-related anxieties. Psychother. Psychosom. 2013, 82, 56–57. [Google Scholar]
- Litwiller, F.; White, C.; Hamilton-Hinch, B.; Gilbert, R. The impacts of recreation programs on the mental health of postsecondary students in North America: An integrative review. Leis. Sci. 2018. [Google Scholar] [CrossRef]
- Machova, K.; Prochazkova, R.; Vadronova, M.; Souckova, M.; Prouzova, E. Effect of dog presence on stress levels in students under psychological strain: A pilot study. IJERPH 2020, 17, 2286. [Google Scholar] [CrossRef]
- Malakoff, M. Effects of Animal-Assisted Therapy on Students with Emotional and Behavioral Disorders. Ph.D. Thesis, Alliant International University, San Diego, CA, USA, 2009. Dissertation Abstracts International: Section B: The Sciences and Engineering. [Google Scholar]
- Manor, W. Directions for the human-animal bond in the nursing education curriculum. Holist. Nursing Prac. 1991, 5, 64–71. [Google Scholar] [CrossRef]
- Marino, L. Construct Validity of Animal-Assisted Therapy and Activities: How Important Is the Animal in AAT? Anthrozoös 2012, 25, s139–s151. [Google Scholar] [CrossRef]
- Matsuura, A.; Nagai, N.; Funatsu, A.; Irimajiri, M.; Yamazaki, A.; Hodate, K. Comparison of the short-term effects of horse trekking & exercising with a riding simulator on autonomic nervous activity. Anthrozoös 2011, 24, 65–77. [Google Scholar]
- McArthur, A.D.; Syrnyk, C. On-campus animal-assisted therapy events: Post-secondary students’ reactions and mood. Soc. Anim. J. Hum. Anim. Stud. 2018, 26, 616–632. [Google Scholar] [CrossRef]
- McCrindle, C.M. Companion animal health education programmes in schools. J. S. Afr. Vet. Assoc. 1996, 67, 102. [Google Scholar]
- McDonald, S.; McDonald, E.; Roberts, A. Effects of novel dog exposure on college students’ stress prior to examination. North Am. J. Psycho. 2017, 19, 477–484. [Google Scholar]
- Merritt, A.E. The effect of a Structured Work Experience Fish Management Program on the self-concept of college students (dissertation). Diss. Abstr. Int. Sect. A Humanit. Soc. Sci. 1990, 50, 3854. Available online: https://www.proquest.com/openview/80378d84f8cf87403caf7d776ed3d17f/1?pq-origsite=gscholar&cbl=18750&diss=y (accessed on 31 July 2020).
- Morgan, B.M. Stress management for college students: An experiential multi-modal approach. J. Creat. Ment. Health. 2017, 12, 276–288. [Google Scholar] [CrossRef]
- Muckle, J.; Lasikiewicz, N. An exploration of the benefits of animal-assisted activities in undergraduate students in Singapore. Asian J. Soc. Psychol. 2017, 20, 75–84. [Google Scholar] [CrossRef]
- Muellmann, S.; Landgraf-Rauf, K.; Brand, T.; Zeeb, H.; Pischke, C.R. Effectiveness of School-based Interventions for the Prevention and/or Reduction of Psychosocial Problems among Children and Adolescents: A Review of Reviews. Gesundheitswesen 2017, 79, 252–260. [Google Scholar] [PubMed]
- Nocentini, S.; Novelli, C.; Campani, D. Animal assisted therapy, 4 paws and 2 feet: 6 steps toward a different future. J. Intellec. Disabil. Res. 2015, 59, 35–36. [Google Scholar]
- Pendry, P.; Vandagriff, J.L. Animal Visitation Program (AVP) Reduces Cortisol Levels of University Students: A Randomized Controlled Trial. AERA Open 2019, 5, 2332858419852592. [Google Scholar] [CrossRef]
- Pendry, P.; Carr, A.M.; Gee, N.R.; Vandagriff, J.L. Randomized Trial Examining Effects of Animal Assisted Intervention and Stress Related Symptoms on College Students’ Learning and Study Skills. IJERPH 2020, 17, 1909. [Google Scholar] [CrossRef] [PubMed]
- Pendry, P.; Kuzara, S.; Gee, N.R. Evaluation of undergraduate students’ responsiveness to a 4-week university-based Animal-Assisted Stress Prevention Program. IJERPH 2019, 16, 3331. [Google Scholar] [CrossRef] [PubMed]
- Pendry, P.; Kuzara, S.; Gee, N.R. Characteristics of student-dog interaction during a meet-and-greet activity in a university-based Animal Visitation Program. Anthrozoös 2020, 33, 53–69. [Google Scholar] [CrossRef]
- Pendry, P.; Carr, A.; Roeter, S.M.; Vandgriff, J.L. Experimental trial demonstrates effects of animal-assisted stress prevention program on college students’ positive and negative emotion. HAIB 2018, 6, 81–97. [Google Scholar]
- Perry, R. The benefits of human-animal interaction on college campuses. Bachelor Thesis, Worcester Polytechnic Institute, Worcester, MA, USA, 2017. [Google Scholar]
- Picard, M.J. Study of the Effect of Dogs on College Students’ Mood and Anxiety; Honors College, The University of Maine: Orono, ME, USA, 2015. [Google Scholar]
- Polking, A.K.; Cornelius-White, J.H.D.; Stout, T.L. Doggone good? Potential benefits of Assistance Animals for students on college campuses. JPED 2017, 30, 237–250. [Google Scholar]
- Quinn, B.L.; Peters, A. Strategies to reduce nursing student test anxiety: A literature review. J. Nurs. Educ. 2017, 56, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Ralston, S.L. Rutgers Young Horse Teaching and Research Program: Undergraduate student outcomes. J. Anim. Sci. 2012, 90, 4671–4676. [Google Scholar] [CrossRef][Green Version]
- Renne, K.G. Effects of therapy dogs on participants’ anxiety in group discussion. In The Research and Scholarship Symposium; 13 Cedarville University: Cedarville, OH, USA, 2018. [Google Scholar]
- Robino, A.E.; Corrigan, V.K.; Anderson, B.; Werre, S.; Farley, J.P.; Marmagas, S.W.; Buechner-Maxwell, V. College Student mental health in an Animal-Assisted Intervention Program: A preliminary study. J. Creat. Ment. Health 2020, 16, 49–58. [Google Scholar] [CrossRef]
- Robson, H.A. Equine Assisted Psychotherapy: A Critical Review of the Literature. Ph.D. Thesis, Saybrook University, Pasadena, CA, USA, 2016. Dissertation Abstracts International: Section B: The Sciences and Engineering. [Google Scholar]
- Rose, J.F. Therapy horses school nurses in emotional fitness. RN 2008, 71, 18–20. [Google Scholar] [PubMed]
- Sanford, M.D. Campus Tails: An on-Campus Therapy-Dog Pilot Program and Feasibility Study. Ph.D. Thesis, Antioch University New England, Keene, NH, USA, 2015. Dissertation Abstracts International: Section B: The Sciences and Engineering. [Google Scholar]
- Silas, H.J.; Binfet, J.-T.; Ford, A.T. Therapeutic for all? Observational assessments of therapy canine stress in an on-campus stress-reduction program. J. Vet. Behav. 2019, 32, 6–13. [Google Scholar] [CrossRef]
- Sola-Perkins, B. The Impact of the Use of a Professional Therapy Dog on the Sense of School Belongingness and Class Attendance of Students in a Truant’s Alternative and Optional Education Program. Ed.D. Dissertation, Edgewood College, Madison, WI, USA, 2019. Dissertation Abstracts International Section A: Humanities and Social Sciences. [Google Scholar]
- Stewart, A.; Strickland, O. A companion animal in a work simulation: The roles of task difficulty and prior companion-animal guardianship in state anxiety. Soc. Anim. J. Hum. Anim. Stud. 2013, 21, 249–265. [Google Scholar] [CrossRef]
- Stewart, L.A.; Dispenza, F.; Parker, L.; Chang, C.Y.; Cunnien, T. A pilot study assessing the effectiveness of an Animal-Assisted Outreach Program. J. Creat. Ment. Health 2014, 9, 332–345. [Google Scholar] [CrossRef]
- Straatman, I.; Hanson, E.K.; Endenburg, N.; Mol, J.A. The influence of a dog on male students during a stressor. Anthrozoös 1997, 10, 191–197. [Google Scholar] [CrossRef]
- Swan, A.M. Close encounters of the canine kind: The use of dogs as “canine co-therapists” in psychotherapy. Aust. N. Z. J. Psychiatry 2011, 45, A55. [Google Scholar]
- Taylor, L.E.; Shaw, J.M. Interspecies encounter: Documenting the benefits of incorporating fine arts into the Equine Studies curriculum. J.Equine Vet. Sci. 2017, 52, 120. [Google Scholar] [CrossRef]
- Thelwell, E.L.R. Paws for Thought: A Controlled Study Investigating the Benefits of Interacting with a House-Trained Dog on University Students Mood and Anxiety. Animals 2019, 9, 846. [Google Scholar] [CrossRef]
- Thew, K.R. The Effect of Interaction with a Therapy Dog on College Student Stress Levels as Measured by Physiological Indicators. Ph.D. Thesis, Washington State University, Pullman, WA, USA, 2018. Dissertation Abstracts International: Section B: The Sciences and Engineering. [Google Scholar]
- Tobin, K.M. The Relationship between Equine-Assisted Psychotherapy and Client-Therapist Attachment on Symptom Reduction. Ph.D. Thesis, Walden University, Minneapolis, MN, USA, 2020. Dissertation Abstracts International Section A: Humanities and Social Sciences. [Google Scholar]
- Tomaszewska, K.; Bomert, I.; Wilkiewicz-Wawro, E. Feline-assisted therapy: Integrating contact with cats into treatment plans. Pol. Ann. Med. 2017, 24, 283–286. [Google Scholar] [CrossRef]
- Trammell, J.P. The effect of therapy dogs on exam stress and memory. Anthrozoös 2017, 30, 607–621. [Google Scholar] [CrossRef]
- Turner, K.; McCarthy, V.L. Stress and anxiety among nursing students: A review of intervention strategies in literature between 2009 and 2015. Nurse Educ. Pract. 2017, 22, 21–29. [Google Scholar] [CrossRef]
- Voelpel, P.; Escallier, L.; Fullerton, J.; Abitbol, L. Interaction between veterans and horses: Perceptions of benefits. J. Psychosoc. Nurs. Ment. Health Serv. 2018, 56, 7–10. [Google Scholar] [CrossRef]
- Walsh, F. Human-animal bonds I: The relational significance of companion animals. Fam. Process. 2009, 48, 462–480. [Google Scholar] [CrossRef]
- Wheller, E.A.; Faulkner, M.E. The “pet effect”: Physiological calming in the presence of canines. Soc. Anim. J. Hum. Anim. Stud. 2015, 23, 425–438. [Google Scholar] [CrossRef]
- Williams, C.L.; Dagnan, E.; Miner, K.M.; Sells, P. The Effect of an Animal-Assisted Intervention on Physiological Measures of Stress and Anxiety in Graduate Professional Physical Therapy Students. OALib J. 2018, 5, 1–16. [Google Scholar] [CrossRef]
- Wilson, C.C. Physiological responses of college students to a pet. J. Nerv. Ment. Dis. 1987, 175, 606–612. [Google Scholar] [CrossRef]
- Wilson, C.C. The pet as an anxiolytic intervention. J. Nerv. Ment. Dis. 1991, 179, 482–489. [Google Scholar] [CrossRef]
- Wood, E.; Ohlsen, S.; Thompson, J.; Hulin, J.; Knowles, L. The feasibility of brief dog-assisted therapy on university students stress levels: The PAwS study. J. Ment. Health 2018, 27, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Young, J.S. Pet therapy: Dogs de-stress students. JCN 2012, 29, 217–221. [Google Scholar] [CrossRef]
- Zents, C.E.; Fisk, A.K.; Lauback, C.W. Paws for intervention: Perceptions about the use of dogs in schools. J. Creat. Ment. Health 2017, 12, 82–98. [Google Scholar] [CrossRef]
- Kolcaba, K. Evolution of the mid range theory of comfort for outcomes research. Nurs. Outlook 2001, 49, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Health Knowledge. Continuous Outcomes. 2020. Available online: https://www.healthknowledge.org.uk/interactive-learning/fae/making-sense-of-results/outcome-measures/continuous-outcomes (accessed on 30 July 2020).



| Inclusion | Exclusion |
|---|---|
| Population: Students in higher education (defined as post-secondary education leading to a degree). OR A description of an equivalent/use of terms known to be associated with higher education. Rationale: Definition of higher education and represents a population exposed to significant stress. If stressor present, had to be an aspect of study, training, education or be student-specific. Rationale: student-specific stressor. | Population: Students who all have an established diagnosed condition/disorder (such as autism or ADHD). Rationale: could substantially affect the clinical heterogeneity of the populations being compared. |
| Intervention: AAI—particularly AAT and AAA. OR Live animal considered/called a therapy animal (OR animal had training AND assessment or evaluation/certification), a therapeutic goal/aim was identified, and the outcomes of interest were evaluated. Rationale: Key elements of AAI (including AAT and AAA); evaluation of relevant outcomes was required to assess results. | Intervention: Not involving a live animal. Rationale: AAIs involve live animals. Participants’ own pets/companion/support/assistance/service animals. Rationale: Likely to represent potential confounders/effect modifiers and not consistent with definitions of AAI, AAT or AAA. |
| Comparator: A comparison group required. Rationale: comparators are required to evaluate intervention’s effectiveness. | Comparator: No comparator. |
| Outcome: Psychological using published or established standardised measures: Primary outcomes: effect on anxiety and/or stress. Secondary outcomes: effect on depression, mood/affect and well-being. Rationale: Represent important measures of mental health and well-being. | Outcome: Physiological. Rationale: Often used as proxy measures for psychological states but not directly related to psychological outcomes. Educational/or academic. Rationale: Focus is on mental health and well-being, not performance. |
| Study: RCT and other types of randomisation. Rationale: RCT represents gold standard for measuring effectiveness. | Study: all non-randomised. Rationale: prone to effects of confounding & to ensure feasibility of review due to time/resources constraints. |
| First Author, Year & Country | Participants | Intervention | Comparator | Outcomes | |||
|---|---|---|---|---|---|---|---|
| Characteristics | Theoretical Framework Articulated | Description of Intervention | Type of AAI & Delivery | Tools Used | Time-Points | ||
| Banks [72] 2018 USA | University students with some recruited from psychology department (76.8% female) Mean age 20.05 (SD 3.38) Year of study, type of graduate, ethnicity, health status or SES NR | No | Group (free interaction) with as many dogs as wanted (student: dog ratio NR) for 10 min single session during mid-term exam week Various breeds (e.g., Beagle, Golden Retrievers, German Shepherds) | AAA Handler | No-treatment control | PANAS—positive & negative | Pre & post stressor (SART & letter/ pattern comparison) |
| Binfet [35] 2017 Canada | First-year university undergraduate students taking psychology classes (78% female) Mean age 18.85 (SD 2.65) Ethnicity: 57% Caucasian; 15% Chinese; 9% Mixed-Race Health status or SES NR | Yes | Group (free interaction) 3–4 student: 1 therapy dog/handler for 20 min single session Various breeds including pure-bred & mixed (which breeds NR) | AAT * Handler | No-treatment control (“business as usual” control = studying) | PSS Sense of Belonging in School | Pre, post, & then follow-up after 2 weeks |
| Fiocco [73] 2017 Canada | Undergraduate university students (77.1% female) Mean age 21.02 (SD 5.5) Ethnicity: 37.7% Caucasian; 8.2% Black/African American; 54.1% Other Year of study, health status or SES NR | Partial | Individual (free interaction as long as participant remained seated) with a dog for 10 min single session Various breeds of different ages & sizes/breed (e.g., Irish Setter, Schnoodle, Greyhound, King Charles Spaniel) | AAA Unclear if handler present | No-treatment control (sitting for 10 min) | PANAS—positive & negative | Pre, post AAA & then after stressor (PASAT) |
| Gebhart [74] 2019 Austria | First-year students at nursing school (77% female) Median age 20 (IQR 19–22) Type of graduate not clearly specified; health status, ethnicity or SES NR | Partial | Group interaction (structured with different tasks, playing & interacting with dogs) student: dog/handler ratio implied 3 students: 1 therapy dogs/handler for 45–60 min for 3 sessions (time interval between sessions NR) | AAT Handler | No-treatment control unstructured free hour; music therapy (body percussion) & mandala painting | STAI-S | Pre & post normal day Pre & post exam day |
| Grajfoner [37] 2017 Scotland | University students (64.4.% female) Mean age 21.6 (SD 3.4) Year of study, type of graduate, health status, ethnicity or SES NR | Yes | Group (free interaction) ~6 students: 1 dog/handler ratio for 20 min single session Various breeds (e.g., Labrador, Lhasa Apso, Golden Retriever) | AAA Handler | Handler only (HO) & dog only (DO) (handler present; no interaction) | STAI WEMWBS UMACL | Pre & post |
| Hall [75] 2018 USA | Level 2 community college associate degree nursing programme Gender, age, year of study, type of graduate or health status, ethnicity or SES NR (only demographics of the course) | Partial | Mix of group or individual session (free interaction) with numerous opportunities to interact with dog. Dog on campus minimum twice a week, visited students at various locations & on exam days for 30 min pre-exams. Intensity, length & frequency of sessions NR Standard Poodle | AAA Handler (unclear if always present) | No-treatment control | HADs—anxiety & depression | Pre & post (which is after 15–16 weeks from start of intervention) |
| Hunt [76] 2018 USA | Undergraduate students enrolled in psychology courses (74% female) Mean age 19.3 (SD NR) & ≥18 yrs old Ethnicity: 52% non-Hispanic White; 27% Asian/Asian-American; 9% Hispanic/Latino; 5% Black/African American, 4% Multiracial, 2% Indian; 1% Arab Year of study, health status or SES NR | Partial | Group interaction (free interaction) with a dog plus interactive games, icebreakers & snacks student: dog ratio not clearly stated but implied 12–14 students: 1 dog of unclear length for once/week for 4 sessions Golden Retriever | AAA Unclear if handler present | No-treatment control; mindfulness training alone; yoga alone; or mindfulness training with yoga | STAI-S PANAS—positive & negative | Pre & post every session & once 1–3 weeks after completion of AAA with stressor (WAIS-IV IQ test) |
| Meola [80] 2017 USA | University students enrolled on accredited counselling program (85% female) Mean age 30.8 (SD NR) Ethnicity: 85.7% Caucasian; 9.5% African American Year of study, type of graduate (some Masters & PhD but NR for all), health status, or SES NR | Yes | Individual (structured & tailored) equine-assisted learning supervision (EALS) session with a horse with 3 different activities: for 1-h single session | AAT/AAE Handler (who was also an instructor/ facilitator) | No-treatment control | STAI-S | Pre & then post up to one month after intervention |
| Shearer [77] 2016 USA | Undergraduate university students in psychology courses (57% female) Ethnicity: 43% Asian; 41% Caucasian; 7% Hispanic; 3% African American; 3% Other; 1% Native American; 1% Pacific Islander; 1% unidentified. Year of study, health status, age or SES NR | Partial | Group session (free interaction) with a dog plus games & snacks students: dog ratio not clearly specified but implied 12–13 students: 1 dog for 1 h/week for 4 weeks | AAA Facilitator | No-treatment control (added in 2nd phase) or mindfulness meditation | STAI-S BDI II | Pre & then post each session for 4 weeks & then once 1–2 weeks after completion of AAA with stressor (WAIS-IV) |
| Ward-Griffin [78] 2018 Canada | University students enrolled in introductory psychology classes (78% female) Mean age 19.4 (SD 3.73) 45.5% first-year students; others NR Type of graduate, health status, ethnicity or SES NR | Partial | Group session (free interaction) with dogs. student to dog ratio not clearly specified with 7–12 dogs present with handlers for up to 90 min single session during mid-term exam season (on average participants spent 30 min in the space) | AAA Handler | Wait-list control | PSS PANAS—positive & negative SWLS Subjective Happiness Scale Medical Outcomes Study Social Support Scale | Pre & within 24 h of AAA |
| Williams [79] 2018 USA | University graduate students in pharmacy/physical therapy (63.2% female) Mean age 24.42 (SD NR) Year of study, health status, ethnicity, or SES NR | Partial | Not clearly specified but inferred as individual free interaction (as long as no active running & playing) with a dog for 12 min single session prior to exam | AAA Handler | No-treatment control (“business as usual” control = quiet time studying) | STAI-S & T | Pre & post (but before an exam) |
| Study | Trustworthiness (A) | Appropriateness (B) | Relevance (C) | Overall Weight (D) |
|---|---|---|---|---|
| Banks et al. [72] | Low | High | High | Low |
| Binfet [35] | Medium | High | High | Medium |
| Fiocco et al. [73] | Medium | High | High | Medium |
| Gebhart et al. [74] | High | High | High | High |
| Grajfoner et al. [37] | Medium | High | High | Medium |
| Hall [75] | Medium | High | High | Medium |
| Hunt et al. [76] | Medium | High | High | Medium |
| Meola [80] | Medium | High | High | Medium |
| Shearer et al. [77] | Low | High | High | Low |
| Ward-Griffin et al. [78] | Medium | High | High | Medium |
| Williams et al. [79] | Medium | High | High | Medium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parbery-Clark, C.; Lubamba, M.; Tanner, L.; McColl, E. Animal-Assisted Interventions for the Improvement of Mental Health Outcomes in Higher Education Students: A Systematic Review of Randomised Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 10768. https://doi.org/10.3390/ijerph182010768
Parbery-Clark C, Lubamba M, Tanner L, McColl E. Animal-Assisted Interventions for the Improvement of Mental Health Outcomes in Higher Education Students: A Systematic Review of Randomised Controlled Trials. International Journal of Environmental Research and Public Health. 2021; 18(20):10768. https://doi.org/10.3390/ijerph182010768
Chicago/Turabian StyleParbery-Clark, Charlotte, Marvellas Lubamba, Louise Tanner, and Elaine McColl. 2021. "Animal-Assisted Interventions for the Improvement of Mental Health Outcomes in Higher Education Students: A Systematic Review of Randomised Controlled Trials" International Journal of Environmental Research and Public Health 18, no. 20: 10768. https://doi.org/10.3390/ijerph182010768
APA StyleParbery-Clark, C., Lubamba, M., Tanner, L., & McColl, E. (2021). Animal-Assisted Interventions for the Improvement of Mental Health Outcomes in Higher Education Students: A Systematic Review of Randomised Controlled Trials. International Journal of Environmental Research and Public Health, 18(20), 10768. https://doi.org/10.3390/ijerph182010768