
Effects of a Low-Carbohydrate High-Fat Diet Combined with High-Intensity Interval Training on Body Composition and Maximal Oxygen Uptake: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.3. Quality Assessments
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
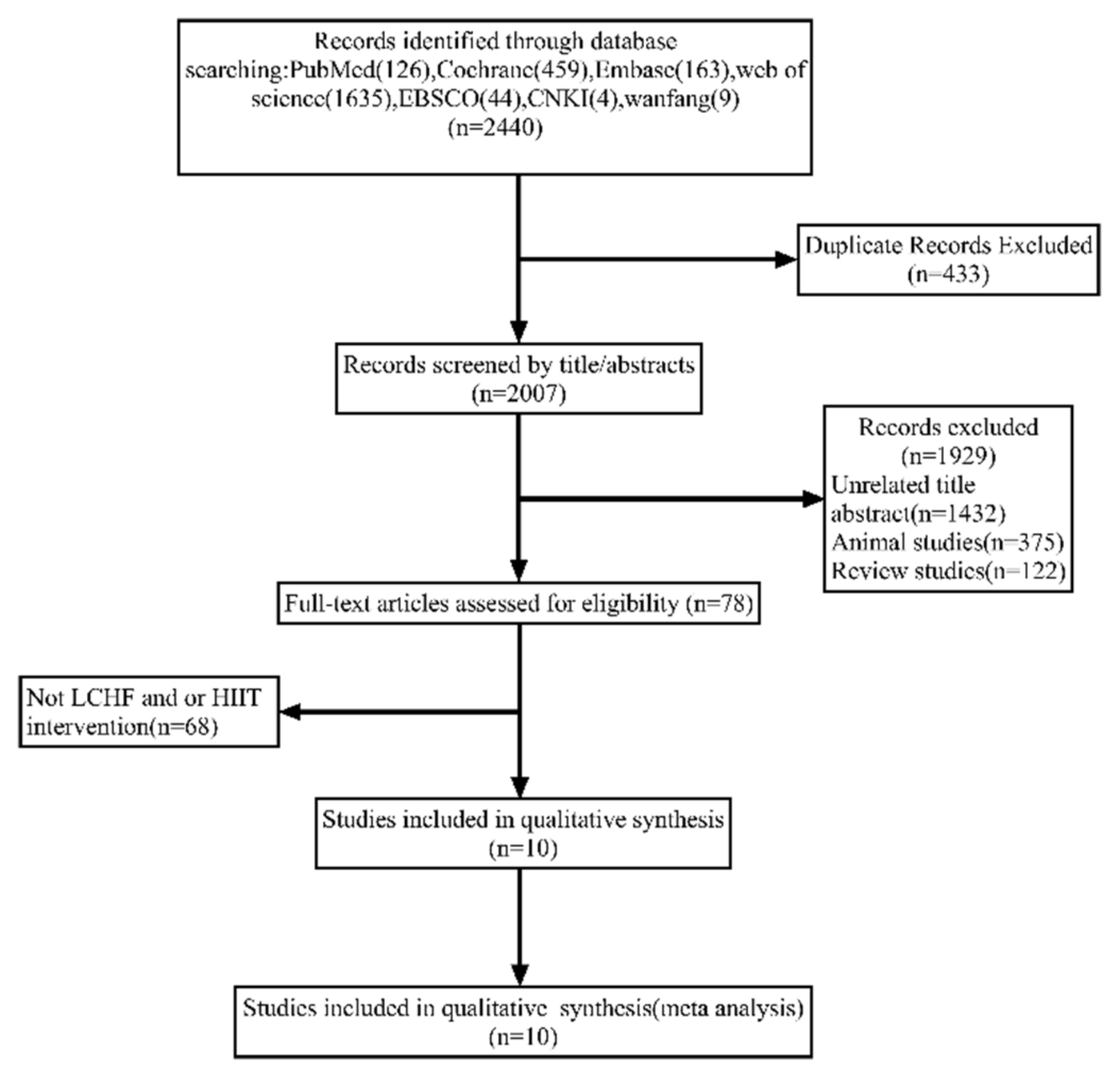
3.1. Study Selection
3.2. Characteristics of the Included Studies
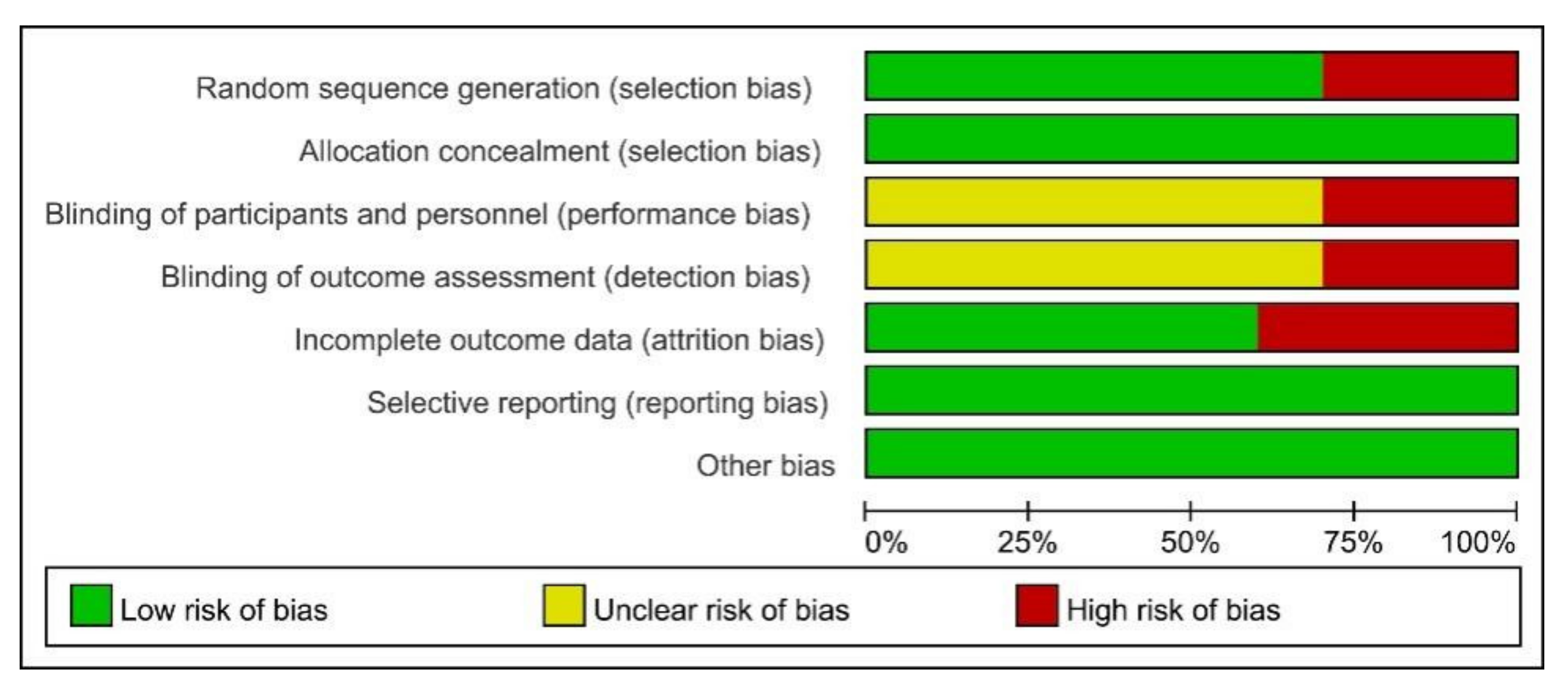
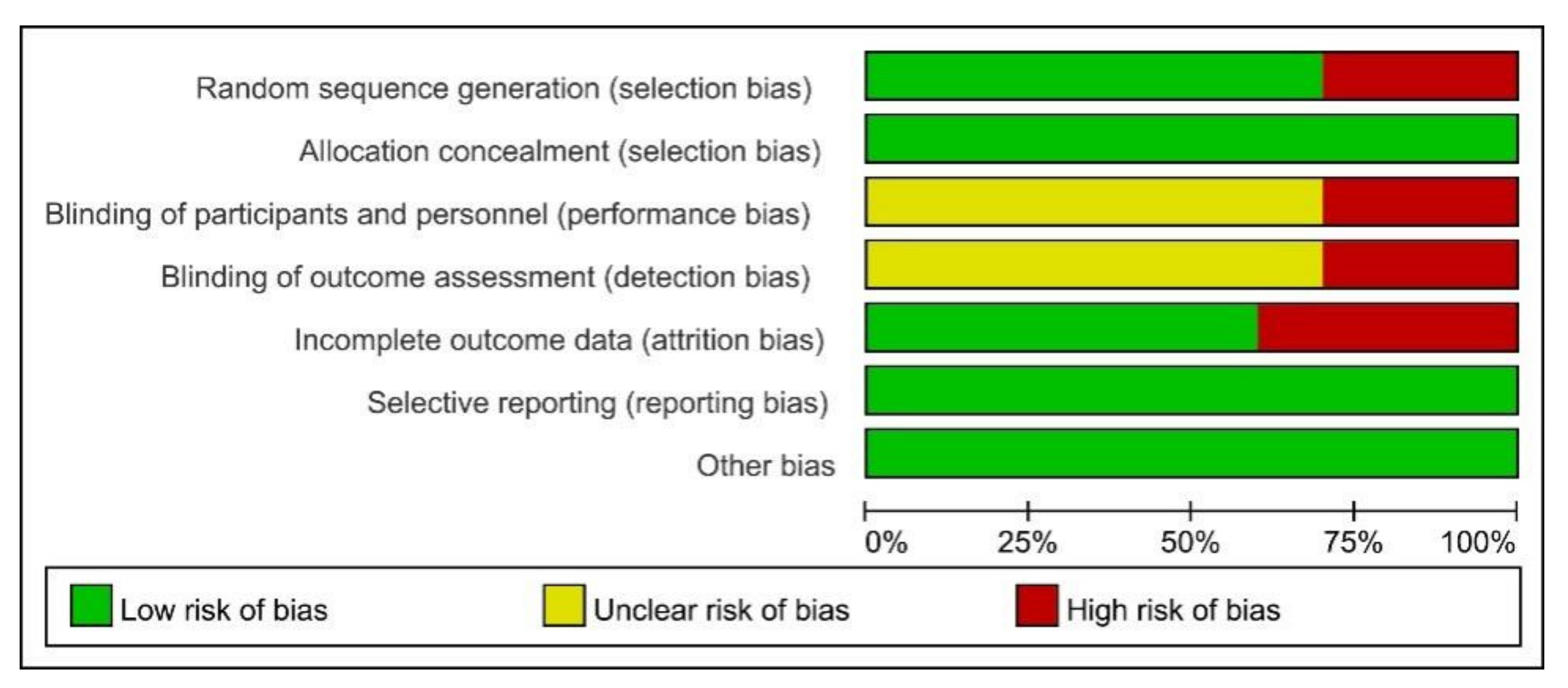
3.3. Results from Quality Assessments
3.4. Publication Bias
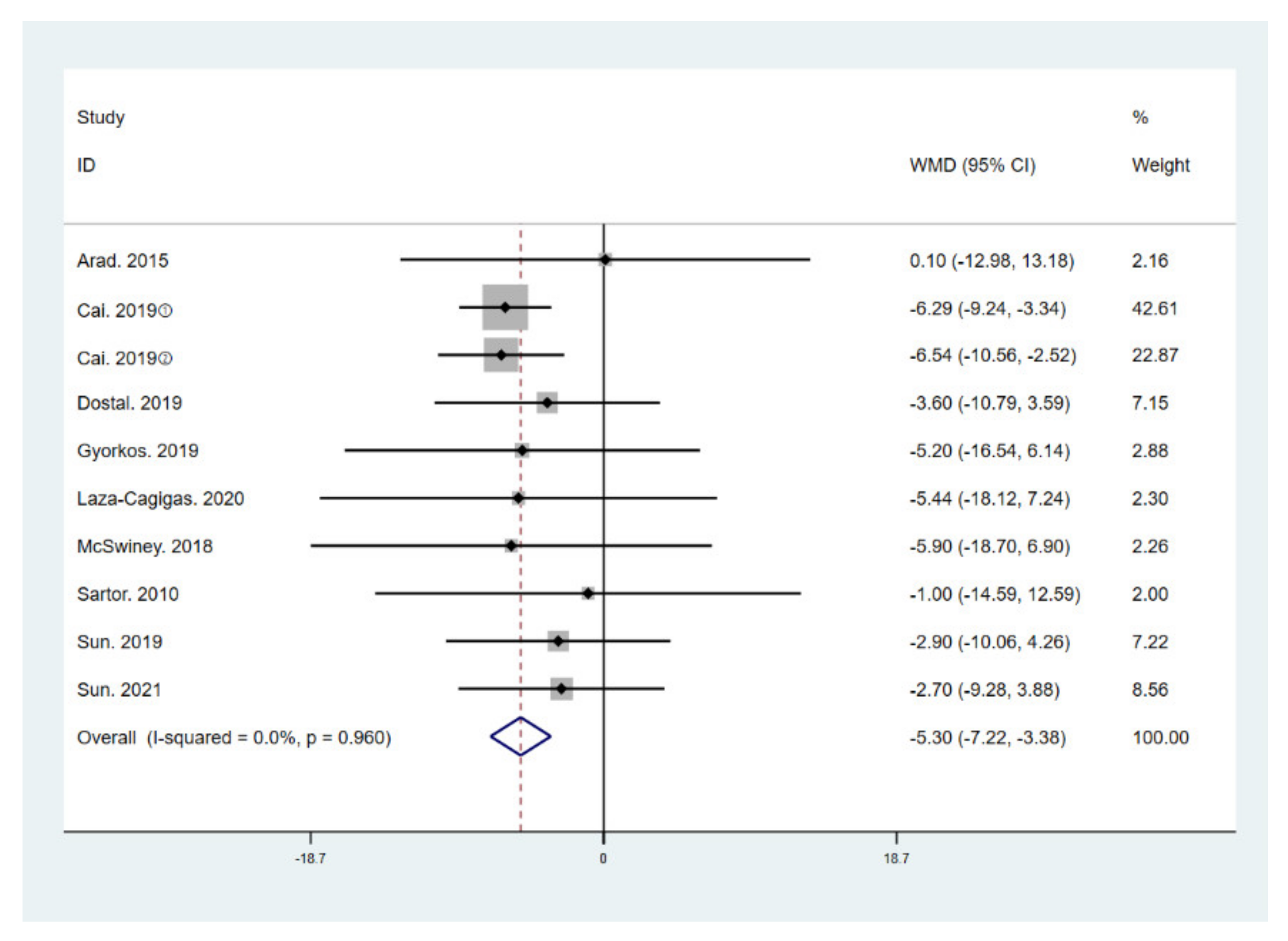
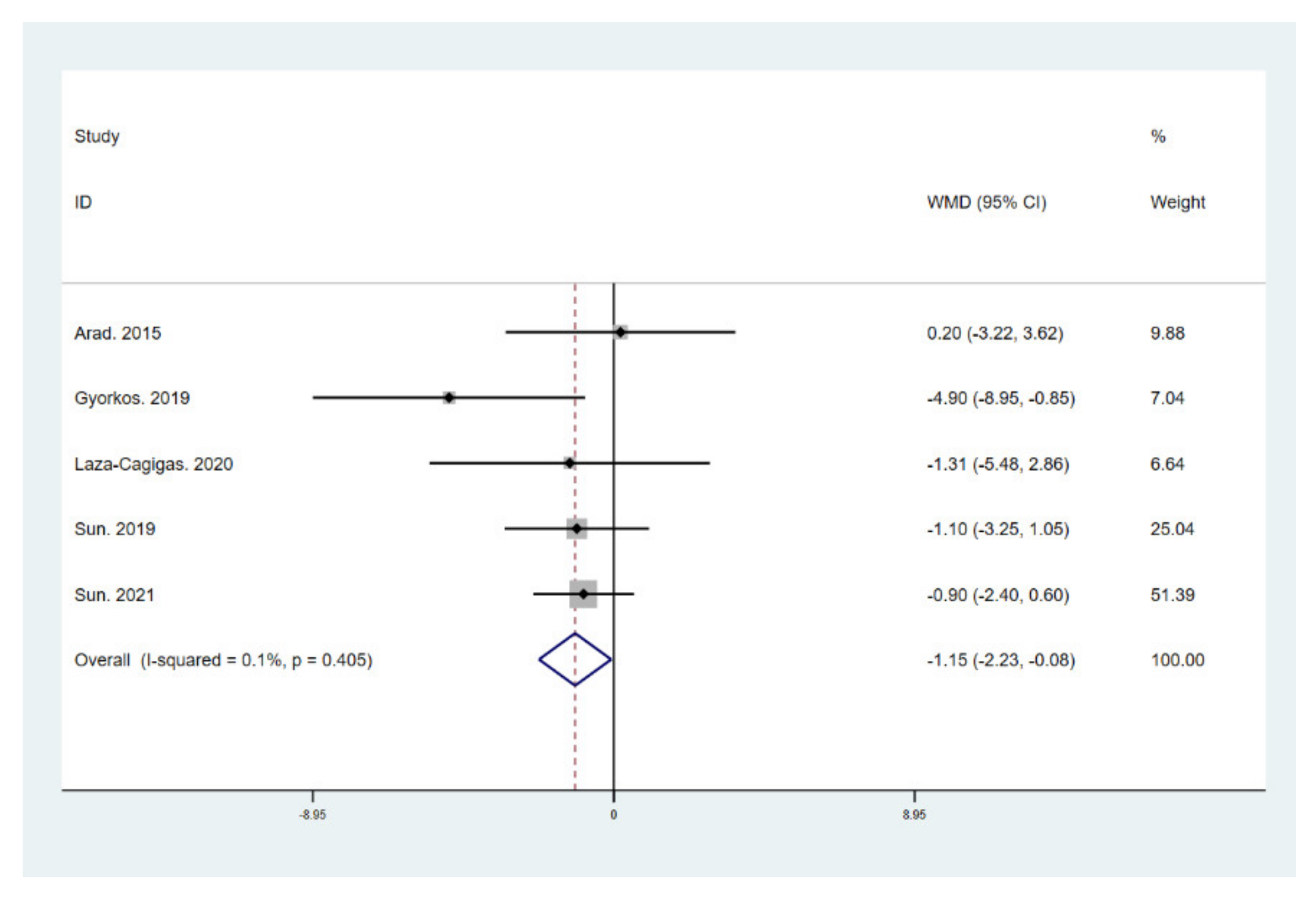
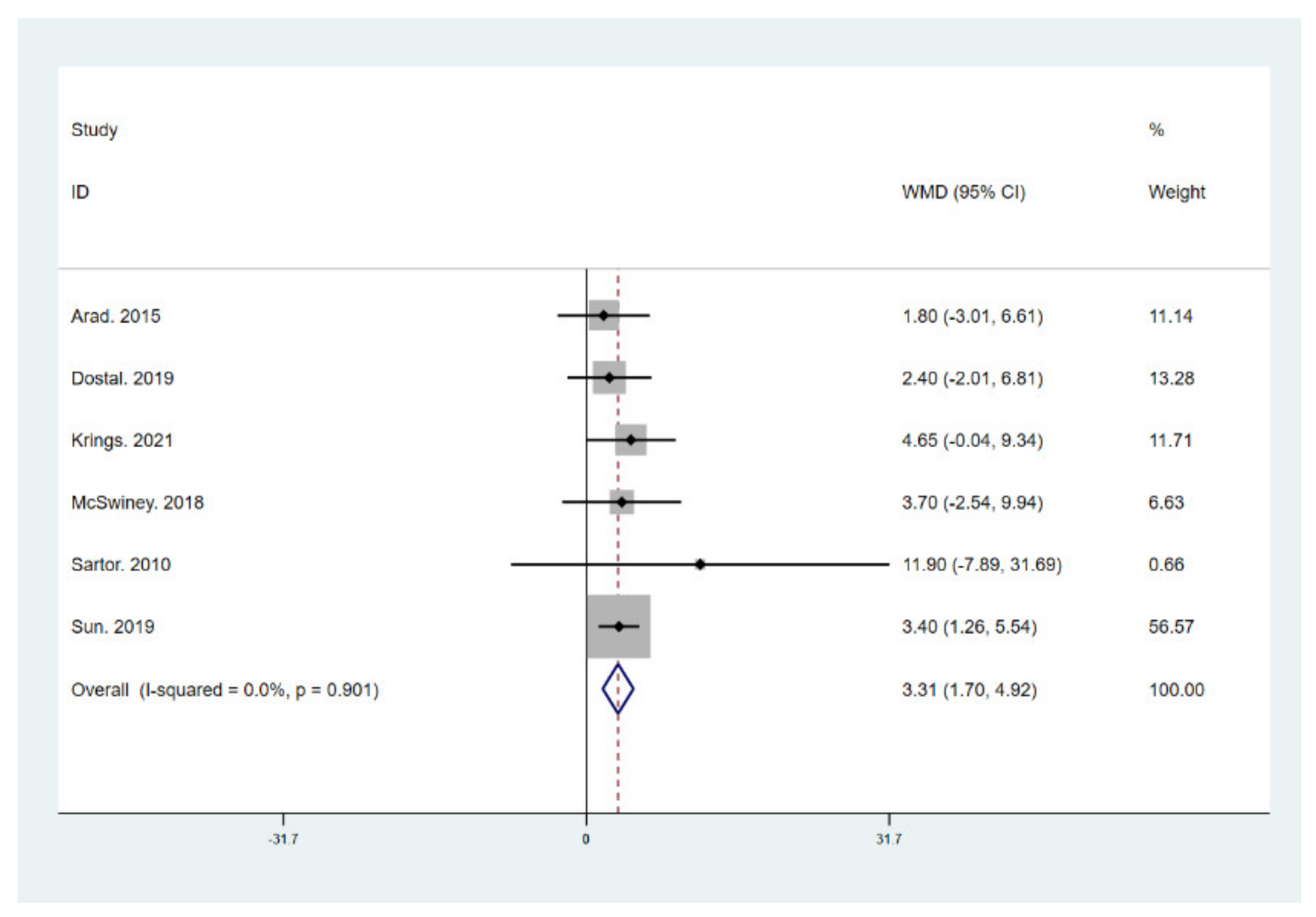
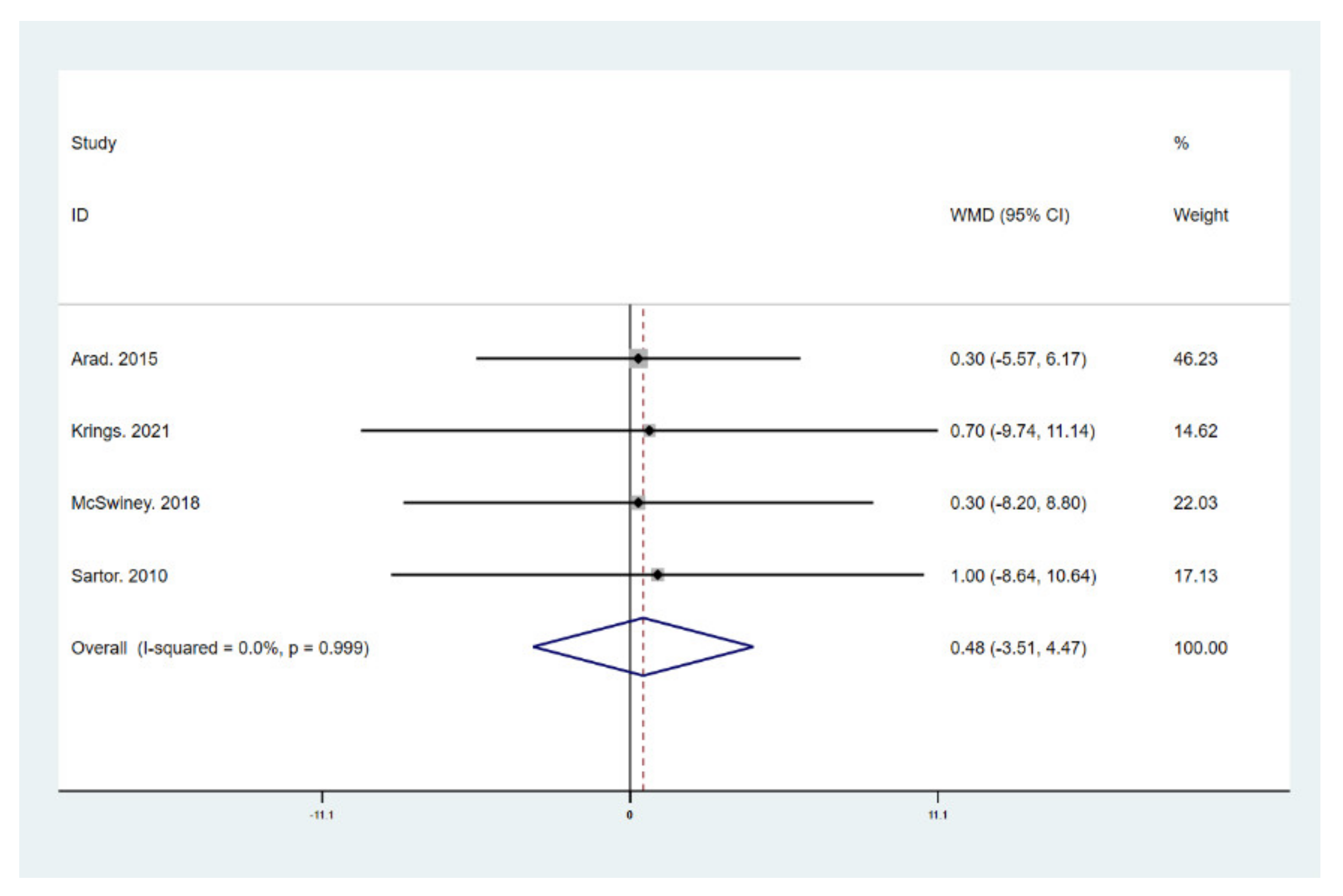
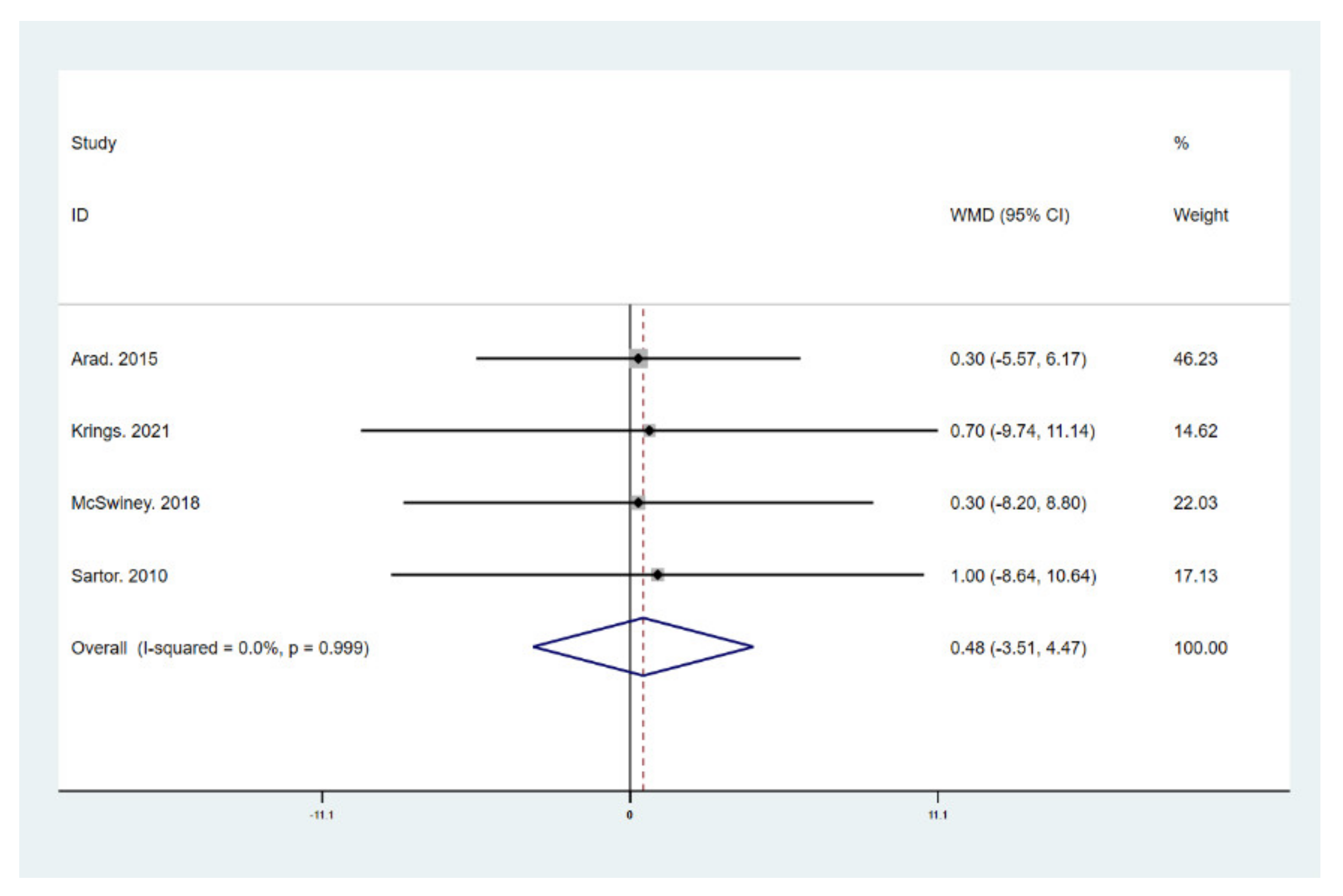
3.5. Results for Body Components and Maximal Oxygen Uptake
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burke, L.M. Re-Examining High-Fat Diets for Sports Performance: Did We Call the ‘Nail in the Coffin’ Too Soon? Sports Med. 2015, 45, S33–S49. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, S.A. Re: National, regional, and global trends in body-mass index since 1980: Systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. J. Urol. 2011, 186, 1982–1983. [Google Scholar] [CrossRef] [PubMed]
- Poirier, P.; Giles, T.D.; Bray, G.A.; Hong, Y.; Stern, J.S.; Pi-Sunyer, F.X.; Eckel, R.H. Obesity and cardiovascular disease: Pathophysiology, evaluation, and effect of weight loss: An update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation 2006, 113, 898–918. [Google Scholar]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goedecke, J.H.; Christie, C.; Wilson, G.; Dennis, S.C.; Noakes, T.D.; Hopkins, W.G.; Lambert, E.V. Metabolic adaptations to a high-fat diet in endurance cyclists. Metabolism 1999, 48, 1509–1517. [Google Scholar] [CrossRef]
- Adam-Perrot, A.; Clifton, P.; Brouns, F. Low-carbohydrate diets: Nutritional and physiological aspects. Obes. Rev. 2006, 7, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Noakes, T.; Volek, J.S.; Phinney, S.D. Low-carbohydrate diets for athletes: What evidence? Br. J. Sports Med. 2014, 48, 1077–1078. [Google Scholar] [CrossRef] [Green Version]
- Volek, J.S.; Noakes, T.; Phinney, S.D. Rethinking fat as a fuel for endurance exercise. Eur. J. Sport Sci. 2015, 15, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Yancy, W.S., Jr.; Olsen, M.K.; Guyton, J.R.; Bakst, R.P.; Westman, E.C. A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia: A randomized, controlled trial. Ann. Intern. Med. 2004, 140, 769–777. [Google Scholar] [CrossRef]
- Moreno, B.; Crujeiras, A.B.; Bellido, D.; Sajoux, I.; Casanueva, F.F. Obesity treatment by very low-calorie-ketogenic diet at two years: Reduction in visceral fat and on the burden of disease. Endocrine 2016, 54, 681–690. [Google Scholar] [CrossRef]
- Bueno, N.B.; de Melo, I.S.; de Oliveira, S.L.; da Rocha Ataide, T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2013, 110, 1178–1187. [Google Scholar] [CrossRef] [Green Version]
- Brouns, F. Overweight and diabetes prevention: Is a low-carbohydrate-high-fat diet recommendable? Eur. J. Nutr. 2018, 57, 1301–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Andrea Meira, I.; Romão, T.T.; Pires do Prado, H.J.; Krüger, L.T.; Pires, M.E.P.; da Conceição, P.O. Ketogenic Diet and Epilepsy: What We Know So Far. Front. Neurosci. 2019, 13, 5. [Google Scholar] [CrossRef] [Green Version]
- Włodarek, D. Role of Ketogenic Diets in Neurodegenerative Diseases (Alzheimer’s Disease and Parkinson’s Disease). Nutrients 2019, 11, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsharairi, N.A. The Role of Short-Chain Fatty Acids in the Interplay between a Very Low-Calorie Ketogenic Diet and the Infant Gut Microbiota and Its Therapeutic Implications for Reducing Asthma. Int. J. Mol. Sci. 2020, 21, 9580. [Google Scholar] [CrossRef] [PubMed]
- Shaw, D.M.; Merien, F.; Braakhuis, A.; Maunder, E.D.; Dulson, D.K. Effect of a Ketogenic Diet on Submaximal Exercise Capacity and Efficiency in Runners. Med. Sci. Sports Exerc. 2019, 51, 2135–2146. [Google Scholar] [CrossRef]
- Vargas-Molina, S.; Petro, J.L.; Romance, R.; Kreider, R.B.; Schoenfeld, B.J.; Bonilla, D.A.; Benitez-Porres, J. Effects of a ketogenic diet on body composition and strength in trained women. J. Int. Soc. Sports Nutr. 2020, 17, 19. [Google Scholar] [CrossRef] [Green Version]
- Vargas, S.; Romance, R.; Petro, J.L.; Bonilla, D.A.; Galancho, I.; Espinar, S.; Kreider, R.B.; Benitez-Porres, J. Efficacy of ketogenic diet on body composition during resistance training in trained men: A randomized controlled trial. J. Int. Soc. Sports Nutr. 2018, 15, 31. [Google Scholar] [CrossRef] [Green Version]
- LaFountain, R.A.; Miller, V.J.; Barnhart, E.C.; Hyde, P.N.; Crabtree, C.D.; McSwiney, F.T.; Beeler, M.K.; Buga, A.; Sapper, T.N.; Short, J.A.; et al. Extended Ketogenic Diet and Physical Training Intervention in Military Personnel. Mil. Med. 2019, 184, e538–e547. [Google Scholar] [CrossRef]
- Greene, D.A.; Varley, B.J.; Hartwig, T.B.; Chapman, P.; Rigney, M. A Low-Carbohydrate Ketogenic Diet Reduces Body Mass Without Compromising Performance in Powerlifting and Olympic Weightlifting Athletes. J. Strength Cond. Res. 2018, 32, 3373–3382. [Google Scholar] [CrossRef]
- Zdzieblik, D.; Oesser, S.; Baumstark, M.W.; Gollhofer, A.; Konig, D. Collagen peptide supplementation in combination with resistance training improves body composition and increases muscle strength in elderly sarcopenic men: A randomised controlled trial. Br. J. Nutr. 2015, 114, 1237–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ting, R.; Dugré, N.; Allan, G.M.; Lindblad, A.J. Ketogenic diet for weight loss. Can. Fam. Physician Med. Fam. Can. 2018, 64, 906. [Google Scholar]
- Kosinski, C.; Jornayvaz, F.R. Effects of Ketogenic Diets on Cardiovascular Risk Factors: Evidence from Animal and Human Studies. Nutrients 2017, 9, 517. [Google Scholar] [CrossRef]
- Jelleyman, C.; Yates, T.; O’Donovan, G.; Gray, L.J.; King, J.A.; Khunti, K.; Davies, M.J. The effects of high-intensity interval training on glucose regulation and insulin resistance: A meta-analysis. Obes. Rev. 2015, 16, 942–961. [Google Scholar] [CrossRef] [Green Version]
- Consitt, L.A.; Dudley, C.; Saxena, G. Impact of Endurance and Resistance Training on Skeletal Muscle Glucose Metabolism in Older Adults. Nutrients 2019, 11, 2636. [Google Scholar] [CrossRef] [Green Version]
- Hallsworth, K.; Thoma, C.; Hollingsworth, K.G.; Cassidy, S.; Anstee, Q.M.; Day, C.P.; Trenell, M.I. Modified high-intensity interval training reduces liver fat and improves cardiac function in non-alcoholic fatty liver disease: A randomized controlled trial. Clin. Sci. 2015, 129, 1097–1105. [Google Scholar] [CrossRef]
- Charatcharoenwitthaya, P.; Kuljiratitikal, K.; Aksornchanya, O.; Chaiyasoot, K.; Bandidniyamanon, W.; Charatcharoenwitthaya, N. Moderate-Intensity Aerobic vs. Resistance Exercise and Dietary Modification in Patients with Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. Clin. Transl. Gastroenterol. 2021, 12, e00316. [Google Scholar] [CrossRef] [PubMed]
- Dun, Y.; Smith, J.R.; Liu, S.; Olson, T.P. High-Intensity Interval Training in Cardiac Rehabilitation. Clin. Geriatr. Med. 2019, 35, 469–487. [Google Scholar] [CrossRef]
- Williams, M.A.; Stewart, K.J. Impact of strength and resistance training on cardiovascular disease risk factors and outcomes in older adults. Clin. Geriatr. Med. 2009, 25, 703–714. [Google Scholar] [CrossRef]
- Chin, E.C.; Yu, A.P.; Lai, C.W.; Fong, D.Y.; Chan, D.K.; Wong, S.H.; Sun, F.; Ngai, H.H.; Yung, P.S.H.; Siu, P.M. Low-Frequency HIIT Improves Body Composition and Aerobic Capacity in Overweight Men. Med. Sci. Sports Exerc. 2020, 52, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Cadore, E.L.; Pinto, R.S.; Bottaro, M.; Izquierdo, M. Strength and endurance training prescription in healthy and frail elderly. Aging Dis. 2014, 5, 183–195. [Google Scholar]
- Moro, T.; Marcolin, G.; Bianco, A.; Bolzetta, F.; Berton, L.; Sergi, G.; Paoli, A. Effects of 6 Weeks of Traditional Resistance Training or High Intensity Interval Resistance Training on Body Composition, Aerobic Power and Strength in Healthy Young Subjects: A Randomized Parallel Trial. Int. J. Environ. Res. Public Health 2020, 17, 4093. [Google Scholar] [CrossRef]
- Fisher, G.; Brown, A.W.; Bohan Brown, M.M.; Alcorn, A.; Noles, C.; Winwood, L.; Resuehr, H.; George, B.; Jeansonne, M.M.; Allison, D.B. High Intensity Interval—vs. Moderate Intensity—Training for Improving Cardiometabolic Health in Overweight or Obese Males: A Randomized Controlled Trial. PLoS ONE 2015, 10, e0138853. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.K.; Dorff, T.B.; Todd Schroeder, E.; Lane, C.J.; Gross, M.E.; Dieli-Conwright, C.M. Impact of resistance training on body composition and metabolic syndrome variables during androgen deprivation therapy for prostate cancer: A pilot randomized controlled trial. BMC Cancer 2018, 18, 368. [Google Scholar] [CrossRef] [PubMed]
- Shirvani, H.; Arabzadeh, E. Metabolic cross-talk between skeletal muscle and adipose tissue in high-intensity interval training vs. moderate-intensity continuous training by regulation of PGC-1α. Eat. Weight. Disord. 2020, 25, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Ashtary-Larky, D.; Bagheri, R.; Asbaghi, O.; Tinsley, G.M.; Kooti, W.; Abbasnezhad, A.; Afrisham, R.; Wong, A. Effects of resistance training combined with a ketogenic diet on body composition: A systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2021, 1–16. [Google Scholar] [CrossRef]
- Murphy, N.E.; Carrigan, C.T.; Margolis, L.M. High-Fat Ketogenic Diets and Physical Performance: A Systematic Review. Adv. Nutr. 2021, 12, 223–233. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med. Sci. Sports Exerc. 2016, 48, 543–568. [Google Scholar]
- Impey, S.G.; Hearris, M.A.; Hammond, K.M.; Bartlett, J.D.; Louis, J.; Close, G.L.; Morton, J.P. Fuel for the Work Required: A Theoretical Framework for Carbohydrate Periodization and the Glycogen Threshold Hypothesis. Sports Med. 2018, 48, 1031–1048. [Google Scholar] [CrossRef] [Green Version]
- Knuiman, P.; Hopman, M.T.; Mensink, M. Glycogen availability and skeletal muscle adaptations with endurance and resistance exercise. Nutr. Metab. 2015, 12, 59. [Google Scholar] [CrossRef] [Green Version]
- Dostal, T.; Plews, D.J.; Hofmann, P.; Laursen, P.B.; Cipryan, L. Effects of a 12-Week Very-Low Carbohydrate High-Fat Diet on Maximal Aerobic Capacity, High-Intensity Intermittent Exercise, and Cardiac Autonomic Regulation: Non-randomized Parallel-Group Study. Front. Physiol. 2019, 10, 912. [Google Scholar] [CrossRef] [Green Version]
- Durkalec-Michalski, K.; Nowaczyk, P.M.; Glowka, N.; Ziobrowska, A.; Podgorski, T. Is a Four-Week Ketogenic Diet an Effective Nutritional Strategy in CrossFit-Trained Female and Male Athletes? Nutrients 2021, 13, 864. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.Y.; Kong, Z.W.; Shi, Q.D.; Hu, M.Z.; Zhang, H.F.; Zhang, D.; Nie, J.L. Non-Energy-Restricted Low-Carbohydrate Diet Combined with Exercise Intervention Improved Cardiometabolic Health in Overweight Chinese Females. Nutrients 2019, 11, 3051. [Google Scholar] [CrossRef] [Green Version]
- Su, L.; Fu, J.; Sun, S.; Zhao, G.; Cheng, W.; Dou, C.; Quan, M. Effects of HIIT and MICT on cardiovascular risk factors in adults with overweight and/or obesity: A meta-analysis. PLoS ONE 2019, 14, e0210644. [Google Scholar] [CrossRef] [PubMed]
- Vella, C.A.; Taylor, K.; Drummer, D. High-intensity interval and moderate-intensity continuous training elicit similar enjoyment and adherence levels in overweight and obese adults. Eur. J. Sport Sci. 2017, 17, 1203–1211. [Google Scholar] [CrossRef] [PubMed]
- Astorino, T.A.; Edmunds, R.M.; Clark, A.; King, L.; Gallant, R.A.; Namm, S.; Fischer, A.; Wood, K.M. High-Intensity Interval Training Increases Cardiac Output and V O2max. Med. Sci. Sports Exerc. 2017, 49, 265–273. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Krings, B.M.; Waldman, H.S.; Shepherd, B.D.; McAllister, M.J.; Fountain, B.J.; Lamberth, J.G.; Smith, J.W. The metabolic and performance effects of carbohydrate timing in resistance trained males undergoing a carbohydrate restricted diet. Appl. Physiol. Nutr. Metab. 2021, 46, 626–636. [Google Scholar] [CrossRef]
- McSwiney, F.T.; Wardrop, B.; Hyde, P.N.; Lafountain, R.A.; Volek, J.S.; Doyle, L. Keto-adaptation enhances exercise performance and body composition responses to training in endurance athletes. Metab. Clin. Exp. 2018, 81, 25–34. [Google Scholar] [CrossRef]
- Arad, A.D.; DiMenna, F.J.; Thomas, N.; Tamis-Holland, J.; Weil, R.; Geliebter, A.; Albu, J.B. High-intensity interval training without weight loss improves exercise but not basal or insulin-induced metabolism in overweight/obese African American women. J. Appl. Physiol. 2015, 119, 352–362. [Google Scholar] [CrossRef] [Green Version]
- Sun, S.; Kong, Z.; Shi, Q.; Zhang, H.; Lei, O.K.; Nie, J. Carbohydrate Restriction with or without Exercise Training Improves Blood Pressure and Insulin Sensitivity in Overweight Women. Healthcare 2021, 9, 637. [Google Scholar] [CrossRef]
- Gyorkos, A.; Baker, M.H.; Miutz, L.N.; Lown, D.A.; Jones, M.A.; Houghton-Rahrig, L.D. Carbohydrate-restricted Diet and High-intensity Interval Training Exercise Improve Cardio-metabolic and Inflammatory Profiles in Metabolic Syndrome: A Randomized Crossover Trial. Cureus 2019, 11, e5596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sartor, F.; de Morree, H.M.; Matschke, V.; Marcora, S.M.; Milousis, A.; Thom, J.M.; Kubis, H.P. High-intensity exercise and carbohydrate-reduced energy-restricted diet in obese individuals. Eur. J. Appl. Physiol. 2010, 110, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Cai, D.; Chen, M. Epidemiological experiments on weight-loss using by ketogenic diet. J. Taishan Med. Coll. 2019, 40, 672–675. [Google Scholar]
- Laza-Cagigas, R.; Chan, S.; Sumner, D.; Rampal, T. Effects and feasibility of a prehabilitation programme incorporating a low-carbohydrate, high-fat dietary approach in patients with type 2 diabetes: A retrospective study. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Hall, K.D.; Chen, K.Y.; Guo, J.; Lam, Y.Y.; Leibel, R.L.; Mayer, L.E.; Reitman, M.L.; Rosenbaum, M.; Smith, S.R.; Walsh, B.T. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men. Am. J. Clin. Nutr. 2016, 104, 324–333. [Google Scholar] [CrossRef] [Green Version]
- Gibson, A.A.; Seimon, R.V.; Lee, C.M.; Ayre, J.; Franklin, J.; Markovic, T.P.; Caterson, I.D.; Sainsbury, A. Do ketogenic diets really suppress appetite? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 64–76. [Google Scholar] [CrossRef] [Green Version]
- Paoli, A.; Cenci, L.; Pompei, P.; Sahin, N.; Bianco, A.; Neri, M.; Caprio, M.; Moro, T. Effects of Two Months of Very Low Carbohydrate Ketogenic Diet on Body Composition, Muscle Strength, Muscle Area, and Blood Parameters in Competitive Natural Body Builders. Nutrients 2021, 13, 374. [Google Scholar] [CrossRef]
- Paoli, A. Ketogenic diet for obesity: Friend or foe? Int. J. Environ. Res. Public Health 2014, 11, 2092–2107. [Google Scholar] [CrossRef] [Green Version]
- Kephart, W.C.; Pledge, C.D.; Roberson, P.A.; Mumford, P.W.; Romero, M.A.; Mobley, C.B.; Martin, J.S.; Young, K.C.; Lowery, R.P.; Wilson, J.M. The Three-Month Effects of a Ketogenic Diet on Body Composition, Blood Parameters, and Performance Metrics in CrossFit Trainees: A Pilot Study. Sports 2018, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.M.; Lowery, R.P.; Roberts, M.D.; Sharp, M.H.; Joy, J.M.; Shields, K.A.; Partl, J.M.; Volek, J.S.; D’Agostino, D.P. Effects of Ketogenic Dieting on Body Composition, Strength, Power, and Hormonal Profiles in Resistance Training Men. J. Strength Cond. Res. 2020, 34, 3463–3474. [Google Scholar] [CrossRef]
- Paoli, A.; Rubini, A.; Volek, J.S.; Grimaldi, K.A. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013, 67, 789–796. [Google Scholar] [CrossRef] [Green Version]
- Veldhorst, M.A.; Westerterp-Plantenga, M.S.; Westerterp, K.R. Gluconeogenesis and energy expenditure after a high-protein, carbohydrate-free diet. Am. J. Clin. Nutr. 2009, 90, 519–526. [Google Scholar] [CrossRef] [Green Version]
- Fine, E.J.; Feinman, R.D. Thermodynamics of weight loss diets. Nutr. Metab. 2004, 1, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volek, J.S.; Freidenreich, D.J.; Saenz, C.; Kunces, L.J.; Creighton, B.C.; Bartley, J.M.; Davitt, P.M.; Munoz, C.X.; Anderson, J.M.; Maresh, C.M. Metabolic characteristics of keto-adapted ultra-endurance runners. Metabolism 2016, 65, 100–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Type of Study | Participants Characteristic/Age/N (Male/Female) | HIIT Intervention/Duration | Macronutrient Ratio in LCHF | Type of Diet | Macronutrient Ratio in Non-LCHF | Result of BM and BMI | Result of FM and BFP | Result of FFM | Result of VO2max |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Arad et al. 2015 [50] | United States | RCT | Overweight/obese females 20–40 years 9 (0/9) | 4 bouts of 30–60 s high-intensity cycling followed by 180–210 s recovery (24 min in total) of 3 sessions/week 14 weeks | CHO: 35% Prt: 15% Fat: 50% Energy: resting metabolic rate ×1.5 | LCHF | Not mentioned | ↔ | ↔ | ↔ | ↔ |
| Cai et al. 2019 ① [54] | China | RCT | Overweight/obese males and females 29.57 ± 3.69 years 7 (1/6) | 1 min HIIT training followed by 20 s recovery (6 times in total) of 2 sessions/week 1 month | CHO: 30 g Prt: 60 g Fat: 130 g Energy: 1500 ± 50 kcal | KD | CHO: 250 g Prt: 60 g Fat: 20 g Energy: 1500 ± 50 kcal | ↓ | - | - | - |
| Cai et al. 2019 ② [54] | China | RCT | Overweight/obese males and females 29.40 ± 3.06 years 10 (2/8) | 1 min HIIT training followed by 20 s recovery (6 times in total) of 2 sessions/week 1 month | CHO: 30 g Prt: 60 g Fat: 130 g Energy: 1500 ± 50 kcal | KD | CHO: 250 g Prt: 60 g Fat: 20 g Energy: 1500 ± 50 kcal | ↓ | - | - | - |
| Dostal et al. 2019 [41] | The Czech Republic | Non-RCT | Healthy males and females 18–35 years 12 (3/9) | 5 × 6 min sets separated by 2 min recovery (40 min in total) of 3–5 sessions/week 12 weeks | CHO: 40 ± 6 g Prt: 113 ± 24 g Fat: 149 ± 26 g Energy: 8206 ± 1322 kJ | VLCHF | CHO: 194 ± 43 g Prt: 79 ± 21 g Fat: 71 ± 17 g Energy: 7523 ± 1541 kJ | ↔ | ↔ | - | ↑ |
| Gyorkos et al. 2019 [52] | United States | RCT | Metabolic syndrome males and females 18–60 years 12 (4/9) | 60 s cycling intervals interspersed with 60 s of active recovery, and a three min cool-down (10 times in total) of 3 sessions/week 4 weeks | CHO: 51 ± 7 g Prt: 87 ± 30 g Fat: 118 ± 27 g Energy: 1590 ± 587 kcal | CRPD | CHO: 277 ± 105 g Prt: 80 ± 36 g Fat: 117 ± 31 g Energy: 2466 ± 602 kcal | ↓ | ↓ | - | ↑ |
| Krings et al. 2021 [48] | China | RCT | Healthy males 19.7 ± 1.0 years 9 (9/0) | 30 s maximal sprints interspersed with 4.5 min of active recovery (4–8 times in total) of 2 sessions/week 4 weeks | CHO: 25% Prt: 25% Fat: 50% Energy: 3051.30 ± 504.02 kcal | CRD | CHO: 298.71 ± 51.03 g Prt: 124.86 ± 35.60 g Fat: 101.14 ± 16.12 g Energy: 2637.92 ± 390.61 kcal | - | ↔ | ↔ | ↑ |
| Laza-Cagigas et al. 2020 [55] | United Kingdom | Non-RCT | Type 1 or Type 2 diabetes 63–79 years 16 (13/3) | 180 s HIIT training followed by 120 slow-intensity intervals (4 times in total) of 2 sessions/week less than 9 weeks | Not mention | LCHF | Not mention | ↓ | - | - | - |
| McSwiney et al. 2018 [49] | Ireland | Non-RCT | Endurance-trained male athletes 18–40 years 9 (9/0) | 10 sets of 1 min bouts at 70% peak power with 1 min recovery of 2 sessions/week 12 weeks | CHO: 41.1 ± 13.3 g Prt: 130.7 ± 35.8 g Fat: 259.3 ± 83.4 g Energy: 3022.3 ± 911.1 kcal | LCKD | CHO: 454.8 ± 152.0 g Prt: 110.3 ± 25.5 g Fat: 64.7 ± 39.1 g Energy: 2843.8 ± 558.4 kcal | ↓ | ↓ | ↔ | ↔ |
| Sartor et al. 2010 [53] | Greece | RCT | Obese males and females 37 ± 10 years 10 (2/8) | 4 min bouts at 90% VO2 peak with 2–3 min rest on cycle ergometers (up to 10 times) of 3 sessions/week 2 weeks | CHO: 163 ± 30 g Prt: 70.9 ± 9.8 g Fat: 63.8 ± 12.6 g (unsaturated fat), 33.5 ± 8.0 g (saturated fat) Energy: 1886 ± 345 kcal | CRD | CHO: 304 ± 57 g Prt: 91.7 ± 26.2 g Fat: 44.9 ± 17.5 g (unsaturated fat) 35.7 ± 11.8 g (saturated fat) Energy: 2363 ± 452 kcal | ↓ | ↓ | ↑ | ↑ |
| Sun et al. 2019 [43] | China | RCT | Overweight/obese females 18–30 years 18 (0/18) | 10 bouts of 6 s cycling sprints followed by 9 s passive recovery (2.5 min in total) of 5 sessions/week 4 weeks | CHO: 49 ± 17 g Prt: 109 ± 28 g Fat: 137 ± 17 g Energy: 1871 ± 246 kcal | LC | CHO: 236 ± 59 g Prt: 77 ± 23 g Fat: 84 ± 25 g Energy: 2057 ± 437 kcal | ↔ | - | - | ↔ |
| Sun et al. 2021 [51] | China | RCT | Overweight/obese females 21.4 ± 2.9 years 17 (0/17) | 10 repetitions of 6 s cycling sprints interspersed with 9 s passive recovery (2.5 min in total) of 5 sessions/week 4 weeks | CHO: 46 ± 15 g Prt: 111 ± 25 g Fat: 141 ± 18 g Energy: 1828 ± 204 kcal | LC | CHO: 241 ± 58 g Prt: 79 ± 19 g Fat: 89 ± 22 g Energy: 2071 ± 407 kcal | ↓ | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, J.; Wang, Z.; Lei, B.; Li, J.; Wang, R. Effects of a Low-Carbohydrate High-Fat Diet Combined with High-Intensity Interval Training on Body Composition and Maximal Oxygen Uptake: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 10740. https://doi.org/10.3390/ijerph182010740
Hu J, Wang Z, Lei B, Li J, Wang R. Effects of a Low-Carbohydrate High-Fat Diet Combined with High-Intensity Interval Training on Body Composition and Maximal Oxygen Uptake: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(20):10740. https://doi.org/10.3390/ijerph182010740
Chicago/Turabian StyleHu, Jing, Zhen Wang, Bingkai Lei, Junping Li, and Ruiyuan Wang. 2021. "Effects of a Low-Carbohydrate High-Fat Diet Combined with High-Intensity Interval Training on Body Composition and Maximal Oxygen Uptake: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 20: 10740. https://doi.org/10.3390/ijerph182010740
APA StyleHu, J., Wang, Z., Lei, B., Li, J., & Wang, R. (2021). Effects of a Low-Carbohydrate High-Fat Diet Combined with High-Intensity Interval Training on Body Composition and Maximal Oxygen Uptake: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(20), 10740. https://doi.org/10.3390/ijerph182010740