Abstract
This study compared the response of a 9-week cycling training on ventilatory efficiency under two conditions: (i) Combined with respiratory muscle training (RMT) using a new nasal restriction device (FeelBreathe) (FB group) and (ii) without RMT (Control group). Eighteen healthy elite cyclists were randomly separated into the FB group (n = 10) or Control group (n = 8). Gas exchange was measured breath by breath to measure ventilatory efficiency during an incremental test on a cycloergometer before (Pre) and after (Post) the nine weeks of training. The FB group showed higher peak power (Δ (95%HDI) (0.82 W/kg (0.49, 1.17)), VO2max (5.27 mL/kg/min (0.69, 10.83)) and VT1 (29.3 W (1.8, 56.7)) compared to Control at PostFINAL. The FB group showed lower values from Pre to PostPRE in minute ventilation (VE) (−21.0 L/min (−29.7, −11.5)), Breathing frequency (BF) (−5.1 breaths/min (−9.4, −0.9)), carbon dioxide output (VCO2) (−0.5 L/min (−0.7, −0.2)), respiratory equivalents for oxygen (EqO2) (−0.8 L/min (−2.4, 0.8)), heart rate (HR) (−5.9 beats/min (−9.2, −2.5)), respiratory exchange ratio (RER) (−0.1 (−0.1, −0.0) and a higher value in inspiratory time (Tin) (0.05 s (0.00, 0.10)), expiratory time (Tex) (0.11 s (0.05, 0.17)) and end-tidal partial pressure of CO2 (PETCO2) (0.3 mmHg (0.1, 0.6)). In conclusion, RMT using FB seems to be a new and easy alternative ergogenic tool which can be used at the same time as day-to-day training for performance enhancement.
1. Introduction
Respiratory muscle training (RMT) has been considered as an effective method to improve the inspiratory muscle strength and performance of athletes of endurance sports [1,2,3,4,5]. Indeed, several studies performed specifically with cyclists have shown that RMT causes physiological adaptations with improvements in the respiratory system, the peak power developed and the time trial performance, both in elite and amateur cyclists [6,7,8,9,10]. However, the RMTs performed in these previous studies have been in static position at rest. Thus, it has not been possible to address the possible additive effect of RMT and exercise at the same time in these previous studies.
Functional RMT while cycling has been investigated previously using 3 different devices: (i) Power Breathe Kinetic KH1 [11]; (ii) Training Mask v2.0 [12]; and (iii) FeelBreathe nasal strips [13]. Using the Power Breathe Kinetic KH1 to RMT while performing stationary cycling increased the electromyography activity in the diaphragm [6]. Despite these results, it should be noted that participants in this study with Power Breathe performed a “static” exercise and, therefore, not a specific cycling training exercise. The use of Training Mask v2.0 while performing 6 weeks of high-intensity cycle ergometer training resulted in improvements in ventilatory threshold, power output at ventilatory threshold, respiratory compensation threshold, and power output at the intensity of respiratory compensation threshold [12]. However, the training mask should be used only part-time during the training season as it could cause inadequate hyperventilation and psychological discomfort [14].
Recently, a new nasal ventilatory flow restriction and filtering device, called FeelBreathe (FB), has been designed, developed and patented to increase nasal airflow resistance [15]. A previous study with elite cyclists has shown that FB used for 10 min on cycle ergometer at 50% of VO2peak causes acute effects in lung ventilation, gas exchange and heart rate during exercise, with improvements on ventilatory efficiency, which could be a target of RMT in sport performance. However, the chronic effect of FB combined with aerobic training in cyclists is unknown [13].
Therefore, the aim of this study was to analyze the additive effect of RMT using FB while performing a specific cycling training plan on different cardiorespiratory variables. We hypothesized, based on the previous results, that the FB group will obtain higher benefits in terms of ventilatory efficiency and peak power developed compared to exercise group without FB without changes on VO2 uptake after the period of training.
2. Materials and Methods
2.1. Subjects
Twenty healthy elite cyclists from two sport clubs in Chiclana de la Frontera (Cádiz, Spain) voluntary participated in this study (mean ± SD, age: 36 ± 10, weight: 71.7 ± 6.7 kg, height: 1.75 ± 0.06 m). All the cyclists had participated in regional and national championships during the last 5 years at least. One of them dropped out the training plan due to illness and another one due to disagreements with the club’s coach, which led to a final sample of eighteen completing the study.
All of the participants were informed of the aims of the study and requirements during the first experimental session. In addition, they signed a written informed consent in accordance with the Declaration of Helsinki. The study protocol and design were approved by the Ethics Committee University Hospital Puerta del Mar (Date: 22 December 2015).
2.2. Training Program
The training plan of this study was directed and controlled by a national cycling coach daily. The training intervention lasted 9 weeks, and one group combined the exercise with RMT at the same time as using the FB device (FB group), and another group trained without any airflow restriction (CG group). The training was carried out at the Moreno Periñan velodrome (Chiclana, Cádiz, Spain) and on the road. The distances and slopes of the roads were controlled for the preparation of the training. Physiological evaluations were before (Pre) and after (Post) the training program to evaluate breathing efficiency through gas exchange.
FB was manufactured for the present study in three models, 4, 5 and 6 mm of ventilatory flow restriction, which produce different levels of air restriction and inspiratory effort. FB has been authorized by the Spanish Agency for Medicines and Health Products (AEMPS No. Exp: 521/15/EC, Spain) (Figure 1). The use of this device during exercise has been used in previous investigations, both in athletes [13] and in patients with COPD [16,17].
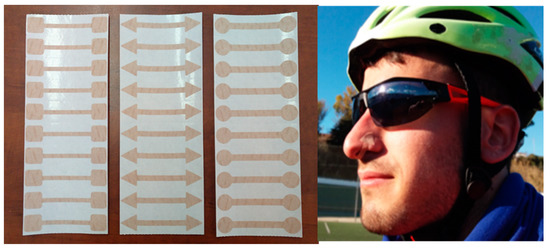
Figure 1.
FeelBreathe (FB) devices of 4, 5 and 6 mm arranged in sheets of 10 units. FB placement mode under the nostrils.
Participants were randomly assigned to either the cycling training combined with FB (FB, n = 10) or control group without FB (Control, n = 8). Both groups were matched by age and VO2max. All participants were instructed to avoid changes in their diet or physical activity while they were following the training plan. The training intensity was set based on the heart rate corresponding to the lactate threshold (HRlactate): (i) Regenerative (<75% HRlactate); A0 (75–90% HRlactate); A1 (90–95% HRlactate); A2 (95–100% HRlactate); A3 (100–105% HRlactate); A4 (105% HRlactate—HRpeak). Both groups completed a volume of 144 h of training during the 9 weeks of intervention, with similar intensity and duration adapted to each athlete (Regenerative: ~42/43% of total training time, A0: ~36/38%, A1: ~8/9%, A2: ~8%, A3: ~3%, A4: ~1%).
The participants of the FB group were instructed on how to place the FB device correctly. During the first 2 weeks, all the participants used the 4 mm FB device model, increasing the width of the device to the 5 mm FB model for the next 4 weeks and to 6 mm FB during the last 3 weeks of training.
2.3. Measurements
At the Andalusian Center for Sports Medicine (Bahía Sur, San Fernando, Spain), pre and post training tests were performed on all participants. During the testing day, resting tests were done with measurement of weight and height, blood pressure, cardiopulmonary auscultation, baseline spirometry (Cardinal Health Spirometer, D-97204 Hoechberg, Germany) and a twelve-lead resting electrocardiogram (Mortara R-SCRIBETM 5, Milwaukee, USA). Moreover, maximal inspiratory pressure (MIP) (Micro RPM of Micro Medical, Chatham, Kent, UK) was measured according to American Thoracic Society (ATS) protocol, choosing the highest value of the 3 efforts with a lower than 5% difference [18].
After that, all participants completed an incremental test on a cycle ergometer (Cardgirus Bikemarc SL, Barcelona, Spain). This test consisted of a stepwise protocol of 30 watt increments every minute with constant revolutions per minute of 80–85 rpm, as used previously [19,20]. The incremental test continued until exhaustion or until the cadence was not maintained. Gas exchange and ventilatory variables were recorded during the incremental test using a gas analyzer (Jaeger-CareFusion modelo MasterScreen CPX). The oxygen consumption (VO2), carbon dioxide output (VCO2), Breathing frequency (BF), tidal volume (Vt), inspiratory tidal volume (VTin), expiratory tidal volume (VTex), inspiratory time (Tin), expiratory time (Tex), duty cycle (TiTot), minute ventilation (VE), respiratory equivalents for oxygen (EqO2) and carbon dioxide (EqCO2), end-tidal partial pressure of O2 (PETO2) and CO2 (PETCO2), and respiratory exchange ratio (RER) were registered in a breath-by-breath manner and averaged by 10 s. Moreover, two dependent evaluators assessed VT1 from visual inspection of (1) the first disproportionate increase in VE; (2) an increase in VE/VO2 with no increase in VE/VCO2 (i.e., the ventilatory equivalents); (3) an increase in PETO2 with no consequent fall in PETCO2, and (4) V-slope plot. VT2 was determined from visual inspection of (1) the second disproportionate increase in VE, (2) the first systematic decrease in PETCO2, and (3) the first systematic increase in VE/VCO2.
Rating of Perceived Exertion (RPE) was detected using the Borg Scale CR 0–10 [21]. One minute after the end of exercise, MIP were repeated post-exercise. After the 9-week training program, all post-tests were performed in the same order and conditions of the pre-test. The evaluators who performed the tests were blind to which individual they were evaluating since they did not participate in the training sessions.
3. Statistical Analysis
Values are reported as mean ± standard deviation. For cardiorespiratory variables analyses, three values were obtained corresponding to three different temporal points in the incremental test: The maximum value recorded at the pre-training test (Pre), the value obtained at the post-training test at the same time as the maximum value at the pre-training test (PostPRE) was obtained, and the maximum value recorded at the post-training test (PostFINAL) (Figure 2).
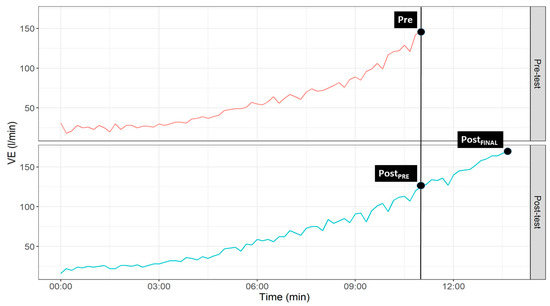
Figure 2.
Graphical representation of temporal points selected for statistical analyses.
Within- and between-group differences were assessed using a Bayesian hierarchical regression model. All hyperparameters in the model followed a weakly informative prior distribution (i.e., a prior distribution that encoded enough information to restrict the plausible range of values of the parameter space but still left a wide range of values to be covered) [22]. Inference was performed based on the 95% highest density interval (95%HDI), which contains a range of values where we can be 95% certain that the true value lies given the data at hand and the model fitted. The null value in our analysis is 0, so if this number is not inside the 95%HDI then we can reject that value for practical purposes [23]. Bayesian estimation of the parameters was obtained by using the package brms for the R programming language [24]. All parameters estimated showed a good convergence with values of = 1 and number of effective sample size > 1000. Further details about the analysis can be found in the supplemental file S1, while the code and the dataset to replicate it are stored in https://github.com/JorgeDelro/cyclists_PE.
4. Results
No significant differences were found between FB and CG groups at the baseline (Table 1).

Table 1.
Participant’s baseline characteristics by group.
Regarding within-group differences, the FB group (Table 2) obtained a lower value from Pre to PostPRE in VE (Δ (95%HDI) = −21.0 L/min (−29.7, −11.5)), BF (−5.1 breaths/min (−9.4, −0.9)), VCO2 (−0.5 L/min (−0.7, −0.2)), EqO2 (−0.8 L/min (−2.4, 0.8)), HR (−5.9 beats/min (−9.2, −2.5)) and RER (−0.1 (−0.1, −0.0) and a higher value in Tin (0.05 s (0.00, 0.10)), Tex (0.11 s (0.05, 0.17)) and PETCO2 (0.3 mmHg (0.1, 0.6)). Additionally, the FB group (Table 2) increased the peak power from Pre to PostFINAL (0.7 W/kg (0.5, 0.9)), VT1 (21.0 W (9.6, 32.4)) and VT2 (17.7 W (0.7, 36.2)). The Control group (Table 3) reached a lower value from Pre to PostPRE in VCO2 (−0.2 L/min (−0.5, −0.0)) and HR (−4.6 beats/min (−7.7, −1.1)) and a higher value in VT2 (21.0 W (9.6, 32.4)).
Table 2.
Average of the maximum value obtained by the Feelbreathe group (FB) in each variable at the pre-training test (Pre-Value), value obtained in the post-training test at the same moment that the maximum in the pre-training test was obtained (PostPRE-Value), and maximum obtained at the post-training test (PostFINAL-Value). Percentage of change (%Change), increment (Δ), and 95% HDI are reported from Pre to PostPRE and from Pre to PostFINAL.
Table 3.
Average of the maximum value obtained by the control group (CG) in each variable at the pre-training test (Pre-Value), value obtained in the post-training test at the same moment that the maximum in the pre-training test was obtained (PostPRE-Value), and maximum obtained at the post-training test (PostFINAL-Value). Percentage of change (%Change), increment (Δ), and 95% HDI are reported from Pre to PostPRE and from Pre to PostFINAL.
Between-group differences for breathing conditions (Table 4) showed a difference in VT2 (7.69 mL/kg/min (1.86, 13.27)) at Pre; in BF (−10.73 breath/min (−19.7, −2.13)), tin (0.10 s (−0.00, −0.20)), tex (0.19 s (0.09, 0.30)) and PETCO2 (0.56 mmHg (0.15, 0.97)) at PostPRE; in Peak power (0.82 W/kg (0.49, 1.17)), VO2max (5.27 mL(kg/min (0.69, 10.83)) and VT1 (29.3 W (1.8, 56.7)) at PostFINAL; in VCO2 (−371.7 L/min (−732.9, −10.2)), tex (0.14 s (0.01, 0.27)), titot (−2.49% (−4.10, −0.85)) and PETO2 (−0.51 mmHg (−0.99, −0.03)) of Δ at PostPRE; in Peak power (0.58 W/kg (0.23, 0.92)) and HR (5.0 beats/min (3.5, 9.6)) of Δ at PostFINAL.
Table 4.
Between-group differences for breathing conditions at the pre-training test (Pre), at the value obtained in the post-training test at the same moment that the maximum in the pre-training test was obtained (PostPRE), at the maximum value obtained at the post-training test (PostFINAL), and between increments at PostPRE (Δ PostPRE) and PostFINAL (Δ PostFINAL).
Within-group differences were found pre-test and pre-training vs. pre-test and post-training in MIP for FB (30.5 cmH2O (18.1, 43.0)) and CG (15.4 cmH2O (2.6, 27.7) and in RPE post-training vs. pre-training for the control group (0.7 (0.1–1.4)) (Table 5).
Table 5.
Within-group pre- and post-test differences in MIP and RPE values.
Finally, no significant between-group differences were found in the increments in MIP or RPE values (Table 6).
Table 6.
Between-group differences in the increments in MIP and RPE values.
5. Discussion
The main finding of the present study was that the ventilatory efficiency and the breathing pattern were improved after the exercise training program in the FB group at the maximum intensity reached in the Pre-test (PostPRE) but not in the control group. FB showed improvements in the time trial and hence in the maximum peak of power developed in the maximum test but without changes in the VO2max compared to pre-training values, while the Control group remained unchanged. This could be explained in part by the higher VO2max and VT1 in the FB compared to the Control group after the training program at maximum values (PostFINAL). Moreover, VT2 showed similar values between conditions after intervention despite the Control group beginning with higher values at Pre. Therefore, only the combination of cyclist training with RMT and FB optimized the breathing pattern such that it could improve performance. To our knowledge, this is the first study which has analyzed the benefits on ventilatory efficiency and breathing pattern in elite cyclists after 9 weeks of traditional endurance training combined with respiratory muscle training at the same time as FB is used.
In agreement with our results, RMT has been documented to improve performance in a wide range of exercise modalities including running, cycling, swimming and rowing [3]. In a study by Holm et al. [7], where 20 trained cyclists and triathletes underwent aerobic training of the respiratory muscles, a significant improvement (of 4.75%) was observed in the time trial as well as in the endurance of the respiratory muscles compared to the control group, but without changes in VO2max. In agreement, McEntire et al. [25], showed that specific training of respiratory muscles through the use of Power Breathe at 15% of MIP in cyclists improved physical performance (18% Exercise Group vs. 10% control group), also without changes in VO2max, RPE or dyspnea. In that sense, our study found that the FB group improved 14.3% in the time trial after intervention, while the Control group remained unchanged (~3%) and without any effect on VO2max in both groups.
The observed gain in the time trial performance in these studies, without an increase in VO2max, may be due to an improvement on ventilatory efficiency. In concordance, our results showed improvements only in FB group at PostPRE moment with significant reductions in VE, BF, VCO2, EqO2, Vt/Ti and RER values and with significant increments in Tin, Tex and PETCO2 values at the same maximum intensity of Pre-moment.
Minute VE was reduced by 13.8% in a moderate intensity exercise in hypoxic condition after only four weeks of inspiratory muscle training (IMT), which means a reduction of the physiological demand of exercise [26]. Similar reduction in VE (15%) was observed only in the FB group in our study at the PostPRE moment. Moreover, it was only in the FB group that the BF dropped ~12%, which can indicate, together with a longer inspiratory time (~9.8%), that there has been a correct training of the respiratory muscles, which are then able to obtain slower and deeper breaths. This, together with a reduction in EQO2 of −8.6% without changes in EQCO2, leads us to a lower dynamic hyperinflation and greater ventilatory efficiency with a similar oxygen uptake with lower ventilation. This physiologic phenomenon triggered a lower heart frequency (~3.5%) and RER (~6.6%) at the same intensity moment, therefore showing an improvement in cardiovascular performance, lower cardiac output and higher energy efficiency. Moreover, FB causes nasal inspirations and mouth exhalations during training sessions, improving the humidification, heating and filtering of the air as it represents a normal mechanism of heat and moisture exchange in the respiratory tract [27].
All changes on ventilatory parameters in FB group after the intervention lead to the improvement of both VT1 and VT2 thresholds (~13.2 and 6.3%; respectively), which are relevant factors for performance and metabolic flexibility during exercise. In fact, a shift to the right of ventilatory thresholds means a better use of fat as an energy source, saving energy from muscle glycogen, preventing fatigue and improving the trial time and the peak of power developed. Despite the fact that the FB group improved the peak of maximum power after training, the subjective perception of effort remained unchanged. Hence, RMT with FB combined with aerobic training may improve the efficiency of oxygen delivery, transport and utilization for fat oxidation during exercise. The group that trained without FB only improved the VT2, but this could be due in part to the fact that this group begun the intervention with lower values in Pre-moment compared to the FB group. However, the magnitude of the Pre-Post change was similar for VT2 between groups, but not for VT1, where the FB group obtained greater improvements.
Furthermore, one of the most important variables to quantify respiratory performance is the MIP. Enright el al. [28] showed that, after 8 weeks of IMT, there was a significant increase in MIP from 142 to 193 cmH2O. In agreement, another study conducted with cyclists demonstrated that IMT for 10 weeks improved MIP by 34% and test time to exhaustion [29]. Moreover, Archiza et al. [30] found that 6 weeks of pressure-threshold IMT improved running time to exhaustion and repeated sprint ability in soccer players. In our study, the FB group showed a significant increase in MIP of 30.5 cmH2O, while that of the CG group was only 15.4 cmH2O. However, no significant between-groups differences were found in the increments of MIP. Moreover, the FB group started from a lower average baseline, which may be responsible for the steeper increase. Nonetheless, the higher effect found in MIP at Pre vs. Pre and the positive change showed from pre-test to post-test either pre- and post-training (negative for CG group) make us claim that further studies are necessary to confirm the ergogenic effect of FB on MIP.
Thus, RMT has been proposed as an ergogenic aid for performance enhancement in training protocols [3]. In this sense, recent studies have been shown the positive effect of training the respiratory muscles at the same time as exercise [12] and not doing so in static situations as is usually done [1,31]. This is, without doubt, one of the biggest advantages of FB.
6. Conclusions
FB is a new and easy device for respiratory muscle training that can be used during the practice of physical exercise. It also could be used while performing most daily tasks unlike other devices for IMT, which have to be used in static position. Moreover, FB is a valid and useful alternative to the training mask since it could be easier and, especially, more comfortable. Hence, FB could be incorporated into the training of this type of athlete as a further stimulus to training with the goal of improving both the specific and respiratory muscles.
Supplementary Materials
The following are available online at https://www.mdpi.com/1660-4601/18/2/777/s1. File S1: Effect of a training programme using a nasal inspiratory restriction device in elite cyclists.
Author Contributions
All authors played a role in the content and writing of the manuscript. J.L.G.-M., J.G.P.-G. and J.R.F.-S. were the principal investigators and contributed the original idea for the study. J.L.G.-M., C.V.-P., J.G.P.-G. and A.A.-M. had input into the study design and con-duct of the study; J.L.G.-M., J.R.-N., E.O.-G., J.H.-J. and R.A.-M. collected the data; J.R.F.-S. per-formed data analysis; J.L.G.-M., J.G.P.-G., J.R.F.-S. E.O.-G., and J.H.-J. interpreted the data and wrote the manuscript. Each one of the authors has read and become responsible for any of the aspects of the study included in the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of University Hospital Puerta del Mar (Date: 22 December 2015).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data is stored in https://github.com/JorgeDelro/cyclists_PE.
Acknowledgments
Special thanks are due to the Center for Sports Medicine (Cádiz, Spain) for the help and collaboration received. The authors wish to thank all the individuals who contributed or took part in the study. No potential conflict of interest was reported by the authors. This study was performed without any funding sources.
Conflicts of Interest
The authors declare no conflict of interest.
References
- HajGhanbari, B.; Yamabayashi, C.; Buna, T.R.; Coelho, J.D.; Freedman, K.D.; Morton, T.A.; Palmer, S.A.; Toy, M.A.; Walsh, C.; Sheel, A.W.; et al. Effects of respiratory muscle training on performance in athletes: A systematic review with meta-analyses. J. Strength Cond. Res. 2013, 27, 1643–1663. [Google Scholar] [CrossRef]
- Illi, S.K.; Held, U.; Frank, I.; Spengler, C.M. Effect of respiratory muscle training on exercise performance in healthy individuals: A systematic review and meta-analysis. Sports Med. 2012, 42, 707–724. [Google Scholar] [CrossRef]
- Shei, R.J. Recent advancements in our understanding of the ergogenic effect of respiratory muscle training in healthy humans: A systematic review. J. Strength Cond. Res. 2018, 32, 2665–2676. [Google Scholar] [CrossRef] [PubMed]
- Jurić, I.; Labor, S.; Plavec, D.; Labor, M. Inspiratory muscle strength affects anaerobic endurance in professional athletes. Arh. Hig. Rada Toksikol. 2019, 70, 42–48. [Google Scholar] [CrossRef]
- Sales, A.T.; Fregonezi, G.A.; Ramsook, A.H.; Guenette, J.A.; Lima, I.N.; Reid, W.D. Respiratory muscle endurance after training in athletes and non-athletes: A systematic review and meta-analysis. Phys. Ther. Sport 2016, 17, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Hellyer, N.J.; Folsom, I.A.; Gaz, D.V.; Kakuk, A.C.; Mack, J.L.; Ver Mulm, J.A. Respiratory muscle activity during simultaneous stationary cycling and inspiratory muscle training. J. Strength Cond. Res. 2015, 29, 3517–3522. [Google Scholar] [CrossRef]
- Holm, P.; Sattler, A.; Fregosi, R.F. Endurance training of respiratory muscles improves cycling performance in fit young cyclists. BMC Physiol. 2004, 4, 9. [Google Scholar] [CrossRef]
- Johnson, M.A.; Sharpe, G.R.; Brown, P.I. Inspiratory muscle training improves cycling time-trial performance and anaerobic work capacity but not critical power. Eur. J. Appl. Physiol. 2007, 101, 761–770. [Google Scholar] [CrossRef]
- McMahon, M.E.; Boutellier, U.; Smith, R.M.; Spengler, C.M. Hyperpnea training attenuates peripheral chemosensitivity and improves cycling endurance. J. Exp. Biol. 2002, 205, 3937–3943. [Google Scholar]
- Romer, L.M.; McConnell, A.K.; Jones, D.A. Effects of inspiratory muscle training upon recovery time during high intensity, repetitive sprint activity. Int. J. Sports Med. 2002, 23, 353–360. [Google Scholar] [CrossRef]
- Caine, M.P.; McConnell, A.K. Development and evaluation of a pressure threshold inspiratory muscle trainer for use in the context of sports performance. Sports Eng. 2000, 3, 149–159. [Google Scholar] [CrossRef]
- Porcari, J.P.; Probst, L.; Forrester, K.; Doberstein, S.; Foster, C.; Cress, M.L.; Schmidt, K. Effect of wearing the elevation training mask on aerobic capacity, lung function, and hematological variables. J. Sports Sci. Med. 2016, 15, 379–386. [Google Scholar] [PubMed]
- González-Montesinos, J.L.; Ponce-González, J.G.; Vicente-Campos, D.; López-Chicharro, J.; Fernández-Santos, J.D.R.; Vaz-Pardal, C.; Costa-Sepúlveda, J.L.; Conde-Caveda, J.; Castro-Piñero, J. Efectos de un dispositivo de restricción ventilatoria nasal sobre la ventilación pulmonar e intercambio gaseoso durante el ejercicio en personas sanas. Nutr. Hosp. 2016, 33, 130. [Google Scholar] [CrossRef] [PubMed]
- Granados, J.; Gillum, T.L.; Castillo, W.; Christmas, K.M.; Kuennen, M.R. “Functional” respiratory muscle training during endurance exercise causes modest hypoxemia but overall is well tolerated. J. Strength Cond. Res. 2016, 30, 755–762. [Google Scholar] [CrossRef]
- Gonzalez-Montesinos, J.L.; Arnedillo-Muñoz, A.; Vaz-Pardal, C.; Fernandez-Santos, J. Dispositivo Para El Entrenamiento de La Musculatura Respiratoria. Utility Model U201930922, 6 August 2019. [Google Scholar]
- Arnedillo, A.; Gonzalez-Montesinos, J.L.; Fernandez-Santos, J.R.; Vaz-Pardal, C.; España-Domínguez, C.; Ponce-González, J.G.; Cuenca-García, M. Effects of a rehabilitation programme with a nasal inspiratory restriction device on exercise capacity and quality of life in COPD. Int. J. Environ. Res. Public Health 2020, 17, 3669. [Google Scholar] [CrossRef]
- Gonzalez-Montesinos, J.L.; Arnedillo, A.; Fernandez-Santos, J.R.; Vaz-Pardal, C.; García, P.A.; Castro-Piñero, J.; Ponce-González, J.G. A new nasal restriction device called feelbreathe (®) improves breathing patterns in chronic obstructive pulmonary disease patients during exercise. Int. J. Environ. Res. Public Health 2020, 17, 4876. [Google Scholar] [CrossRef]
- American Thoracic Society; European Respiratory Society. ATS/ERS statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 2002, 166, 518–624. [Google Scholar] [CrossRef]
- Ponce-González, J.G.; Rodríguez-Garcia, L.; Losa-Reyna, J.; Guadalupe-Grau, A.; Rodriguez-Gonzalez, F.G.; Díaz-Chico, B.N.; Dorado, C.; Serrano-Sanchez, J.A.; Calbet, J.A.L. Androgen receptor gene polymorphism influence fat accumulation: A longitudinal study from adolescence to adult age. Scand. J. Med. Sci. Sports 2016, 26, 1313–1320. [Google Scholar] [CrossRef]
- Ponce-González, J.G.; Guadalupe-Grau, A.; Rodríguez-González, F.G.; Torres-Peralta, R.; Morales-Alamo, D.; Rodríguez-García, L.; Díaz-Chico, B.N.; López Calbet, J.A.; Dorado, C. Androgen receptor gene polymorphisms and maximal fat oxidation in healthy men. A longitudinal study. Nutr. Hosp. 2017, 34, 1089–1098. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Gelman, A.; Simpson, D.; Betancourt, M. The prior can generally only be understood in the context of the likelihood. Entropy 2017, 19, 555. [Google Scholar] [CrossRef]
- Kruschke, J.K. Rejecting or accepting parameter values in bayesian estimation. Adv. Methods Pract. Psychol. Sci. 2018, 1, 270–280. [Google Scholar] [CrossRef]
- Bürkner, P.-C. Brms: An R package for bayesian multilevel models using stan. J. Stat. Softw. 2017, 80. [Google Scholar] [CrossRef]
- McEntire, S.J.; Smith, J.R.; Ferguson, C.S.; Brown, K.R.; Kurti, S.P.; Harms, C.A. The effect of exercise training with an additional inspiratory load on inspiratory muscle fatigue and time-trial performance. Respir. Physiol. Neurobiol. 2016, 230, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Lomax, M.; Massey, H.C.; House, J.R. Inspiratory muscle training effects on cycling during acute hypoxic exposure. Aerosp. Med. Hum. Perform. 2017, 88, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C. Humidification in the upper respiratory tract: A physiological overview. Intensive. Crit. Care Nurs. 1996, 12, 27–32. [Google Scholar] [CrossRef]
- Enright, S.; Chatham, K.; Baldwin, J.; Griffiths, H. The effect of fixed load incremental inspiratory muscle training in the elite athlete: A pilot study. Phys. Ther. Sport 2000, 1, 1–5. [Google Scholar] [CrossRef]
- Gething, A.D.; Williams, M.; Davies, B. Inspiratory resistive loading improves cycling capacity: A placebo controlled trial. Br. J. Sports Med. 2004, 38, 730–736. [Google Scholar] [CrossRef]
- Archiza, B.; Andaku, D.K.; Caruso, F.C.R.; Bonjorno, J.C.; Oliveira, C.R.; Ricci, P.A.; Amaral, A.C.D.; Mattiello, S.M.; Libardi, C.A.; Phillips, S.A.; et al. Effects of inspiratory muscle training in professional women football players: A randomized sham-controlled trial. J. Sports Sci. 2018, 36, 771–780. [Google Scholar] [CrossRef]
- Shei, R.J.; Chapman, R.F.; Gruber, A.H.; Mickleborough, T.D. Respiratory effects of thoracic load carriage exercise and inspiratory muscle training as a strategy to optimize respiratory muscle performance with load carriage. Springer Sci. Rev. 2017, 5, 49–64. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).