Degree of Impact of Tailor’s Bunion on Quality of Life: A Case–Control Study

 , , ,
, , ,  ,
,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
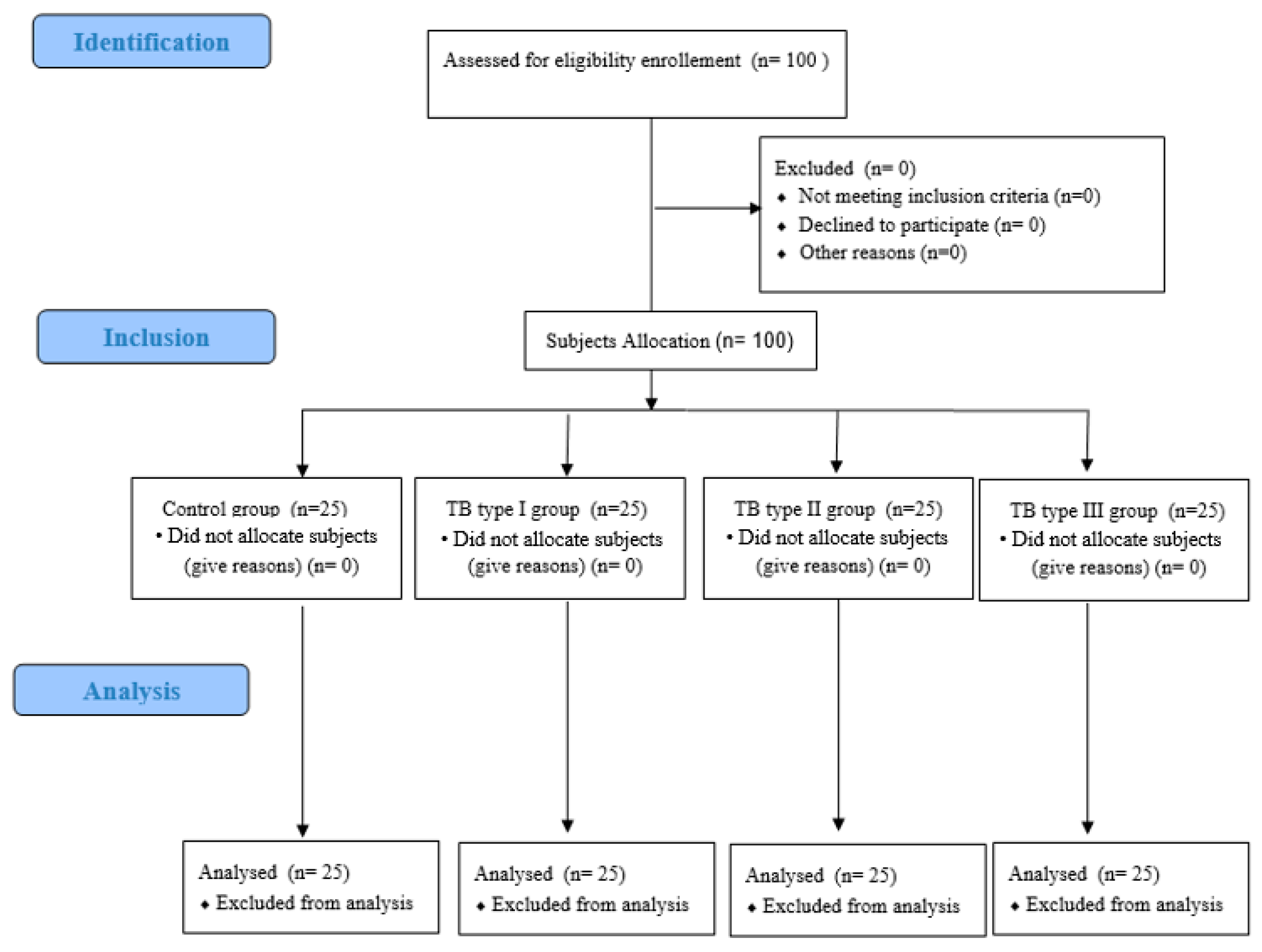
2.1. Design
2.2. Participants
2.3. Procedure and Measurements of FSHQ Results
2.4. Sample Size
2.5. Demographic and Social Descriptive Data
2.6. Statistical Analysis
3. Results
3.1. Demographic, Descriptive, and Social Data
3.2. Demographic, Descriptive, and Social Data by TB Classification
3.3. FSHQ Male and Female Distribution and TB Classification
3.4. Systematic Differences among FHSQ and TB Classification
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davies, H. Metatarsus quintus valgus. Br. Med. J. 1949, 1, 664. [Google Scholar] [CrossRef] [PubMed]
- Ceccarini, P.; Rinonapoli, G.; Nardi, A.; Bisaccia, M.; Di Giacomo, L.M.; Caraffa, A. Bunionette: Minimally Invasive and Percutaneous Techniques: A Topical Review of the Literature. Foot Ankle Spec. 2017, 10, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Caselli, M.A.; George, D.H. Foot deformities: Biomechanical and pathomechanical changes associated with aging, part I. Clin. Podiatr. Med. Surg. 2003, 20, 487–509. [Google Scholar] [CrossRef]
- Shi, G.G.; Humayun, A.; Whalen, J.L.; Kitaoka, H.B. Management of Bunionette Deformity. J. Am. Acad. Orthop. Surg. 2018, 26, e396–e404. [Google Scholar] [CrossRef] [PubMed]
- Ajis, A.; Koti, M.; Maffulli, N. Tailor’s bunion: A review. J. Foot Ankle Surg. 2005, 44, 236–245. [Google Scholar] [CrossRef]
- Golightly, Y.M.; Hannan, M.T.; Dufour, A.B.; Hillstrom, H.J.; Jordan, J.M. Foot disorders associated with overpronated and oversupinated foot Function: The johnston county osteoarthritis project. Foot Ankle Int. 2014, 35, 1159–1165. [Google Scholar] [CrossRef]
- Kitaoka, H.B.; Alexander, I.J.; Adelaar, R.S.; Nunley, J.A.; Myerson, M.S.; Sanders, M. Clinical Rating Systems for the Ankle-Hindfoot, Midfoot, Hallux, and Lesser Toes. Foot Ankle Int. 1994, 15, 349–353. [Google Scholar] [CrossRef]
- Fallat, L.M.; Buckholz, J. An analysis of the tailor’s bunion by radiographic and anatomical display. J. Am. Podiatry Assoc. 1980, 70, 597–603. [Google Scholar] [CrossRef]
- Şaylı, U.; Altunok, E.Ç.; Güven, M.; Akman, B.; Biros, J.; Şaylı, A. Prevalence estimation and familial tendency of common forefoot deformities in Turkey: A survey of 2662 adults. Acta Orthop. Traumatol. Turc. 2018, 52, 167–173. [Google Scholar] [CrossRef]
- Karasick, D. Preoperative assessment of symptomatic bunionette deformity: Radiologic findings. Am. J. Roentgenol. 1995, 164, 147–149. [Google Scholar] [CrossRef]
- Koti, M.; Maffulli, N. Current concepts review bunionette. J. Bone Jt. Surg. Ser. A 2001, 83, 1076–1082. [Google Scholar] [CrossRef] [PubMed]
- Yancey, H.A. Congenital lateral bowing of the fifth metatarsal. Report of 2 cases and operative treatment. Clin. Orthop. Relat. Res. 1969, 62, 203–205. [Google Scholar] [CrossRef] [PubMed]
- Diebold, P.F.; Bejjani, F.J. Basal osteotomy of the fifth metatarsal with intermetatarsal pinning: A new approach to tailor’s bunion. Foot Ankle 1987, 8, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Gallart, J.; González, D.; Valero, J.; Deus, J.; Serrano, P.; Lahoz, M. Biphalangeal/triphalangeal fifth toe and impact in the pathology of the fifth ray. BMC Musculoskelet. Disord. 2014, 15, 1–6. [Google Scholar] [CrossRef]
- Riskowski, J.; Dufour, A.B.; Hannan, M.T. Arthritis, foot pain and shoe wear: Current musculoskeletal research on feet. Curr. Opin. Rheumatol. 2011, 23, 148–155. [Google Scholar] [CrossRef]
- Deveci, A.; Yilmaz, S.; Firat, A.; Yildirim, A.O.; Oken, O.F.; Gulcek, M.; Ucaner, A. An overlooked deformity in patients with hallux valgus: Tailor’s Bunion. J. Am. Podiatr. Med. Assoc. 2015, 105, 233–237. [Google Scholar] [CrossRef]
- Frankel, J.P.; Turf, R.M.; King, B.A. Tailor’s bunion: Clinical evaluation and correction by distal metaphyseal osteotomy with cortical screw fixation. J. Foot Surg. 1989, 28, 237–243. [Google Scholar]
- Sakoff, M.; Levy, A.I.; Hanft, J.R. Metaphyseal osteotomy for the treatment of tailor’s bunions. J. Foot Surg. 1989, 28, 537–541. [Google Scholar]
- Hawke, F.; Burns, J. Understanding the nature and mechanism of foot pain. J. Foot Ankle Res. 2009, 2, 1. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Blettner, M.; et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (Sf-36): I. conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, M.J. Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991, 11, 195–203. [Google Scholar] [CrossRef] [PubMed]
- López, D.L.; González, L.C.; Iglesias, M.E.L.; Canosa, J.L.S.; Sanz, D.R.; Lobo, C.C.; De Bengoa Vallejo, R.B. Quality of life impact related to foot health in a sample of older people with hallux valgus. Aging Dis. 2016, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Palomo-López, P.; López-López, D.; Becerro-De-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodríguez-Sanz, D.; Fernández-Carnero, J.; Martiniano, J.; Calvo-Lobo, C. Concurrent validity of the foot health status questionnaire and study short form 36 for measuring the health-related quality of life in patients with foot problems. Medicina 2019, 55, 750. [Google Scholar]
- Garrow, J.S.; Webster, J. Quetelet’s index (W/H2) as a measure of fatness. Int. J. Obes. 1985, 9, 147–153. [Google Scholar]
- Bennett, P.J.; Patterson, C.; Wearing, S.; Baglioni, T. Development and validation of a questionnaire designed to measure foot-health status. J. Am. Podiatr. Med. Assoc. 1998, 88, 419–428. [Google Scholar] [CrossRef]
- Bennett, P.J.; Patterson, C.; Dunne, M.P. Health-related quality of life following podiatric surgery. J. Am. Podiatr. Med. Assoc. 2001, 91, 164–173. [Google Scholar] [CrossRef]
- Ferrer-Peña, R.; Calvo-Lobo, C.; Aiguadé, R.; Fernández-Carnero, J. Which Seems to Be Worst? Pain Severity and Quality of Life between Patients with Lateral Hip Pain and Low Back Pain. Pain Res. Manag. 2018, 2018, 9156247. [Google Scholar] [CrossRef]
- Coughlin, M.J. Etiology and treatment of the bunionette deformity. Instr. Course Lect. 1990, 39, 37–48. [Google Scholar]
- Benvenuti, F.; Ferrucci, L.; Guralnik, J.M.; Gangemi, S.; Baroni, A. Foot Pain and Disability in Older Persons: An Epidemiologic Survey. J. Am. Geriatr. Soc. 1995, 43, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.; Bennett, P.; Jimenez-Cebrian, A.M.; Labajos-Manzanares, M.T. The psychometric properties of the Spanish version of the Foot Health Status Questionnaire. Qual. Life Res. 2013, 22, 1739–1743. [Google Scholar] [CrossRef] [PubMed]
- Shimobayashi, M.; Tanaka, Y.; Taniguchi, A.; Kurokawa, H.; Tomiwa, K.; Higashiyama, I. Radiographic morphologic characteristics of bunionette deformity. Foot Ankle Int. 2016, 37, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Mahlknecht, P.; Kiechl, S.; Bloem, B.R.; Willeit, J.; Scherfler, C.; Gasperi, A.; Rungger, G.; Poewe, W.; Seppi, K. Prevalence and Burden of Gait Disorders in Elderly Men and Women Aged 60–97 Years: A Population-Based Study. PLoS ONE 2013, 8, e69627. [Google Scholar] [CrossRef] [PubMed]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly: A clinical guide. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef]
- Hrubina, M.; Skotak, M.; Letocha, J.; Dzupa, V. The modified scarf osteotomy in the treatment of tailor’s bunion:Midterm follow-up. Acta Orthop. Belg. 2015, 81, 57–64. [Google Scholar]
- Menz, H.B.; Gilheany, M.F.; Landorf, K.B. Foot and ankle surgery in Australia: A descriptive analysis of the Medicare Benefits Schedule database, 1997–2006. J. Foot Ankle Res. 2008, 1, 10. [Google Scholar] [CrossRef]
- Masquijo, J.J.; Willis, B.R.; Kontio, K.; Dobbs, M.B. Symptomatic bunionette deformity in adolescents: Surgical treatment with metatarsal sliding osteotomy. J. Pediatr. Orthop. 2010, 30, 904–909. [Google Scholar] [CrossRef]
- Cooper, M.T.; Granadillo, V.A.; Coughlin, M.J. The bunionette deformity—Evaluation and management. Ann. Jt. 2020, 5, 7. [Google Scholar] [CrossRef]
- Cohen, B.E.; Nicholson, C.W. Bunionette deformity. J. Am. Acad. Orthop. Surg. 2007, 15, 300–307. [Google Scholar] [CrossRef]
- López-López, D.; Vilar-Fernández, J.M.; Barros-García, G.; Losa-Iglesias, M.E.; Palomo-López, P.; Becerro-de-Bengoa-Vallejo, R.; Calvo-Lobo, C. Foot Arch Height and Quality of Life in Adults: A Strobe Observational Study. Int. J. Environ. Res. Public Health 2018, 15, 1555. [Google Scholar] [CrossRef] [PubMed]
- Palomo-López, P.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Rodríguez-Sanz, D.; Calvo-Lobo, C.; López-López, D. Impact of Hallux Valgus related of quality of life in Women. Int. Wound J. 2017, 14, 782–785. [Google Scholar] [CrossRef] [PubMed]
- López-López, D.; García-Mira, R.; Palomo-López, P.; Sánchez-Gómez, R.; Ramos-Galván, J.; Tovaruela-Carrión, N.; García-Sánchez, M. Attitude and knowledge about foot health: A spanish view. Rev. Lat. Am. Enfermagem 2017, 25, e2855. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic and Descriptive Data | Total Group n = 100 | Male n = 61 | Female n = 39 | p-Value |
|---|---|---|---|---|
| Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | ||
| Age (years) | 51.70 ± 17.78 (48.19–55.24) | 51.78 ± 19.72 (47.53–58.01) | 51.61 ± 19.72 (45.21–58.01) | <0.001 † |
| Weight (Kg) | 82.55 ± 13.60 (79.85–85.25) | 86.81 ± 10.76 (84.06–89.57) | 81.53 ± 12.78 (77.38–85.67) | 0.189 † |
| Height (cm) | 1.77 ± 0.80 (1.75–1.78) | 1.83 ± 0.52 (1.81–1.84) | 1.73 ± 0.77 (1.70–1.75) | 0.002 † |
| BMI (Kg/m2) | 26.02 ± 4.24 (25.17–26.86) | 25.92 ± 4.27 (24.06–27.76) | 27.36 ± 3.88 (26.10–28.62) | 0.113 * |
| Social Characteristics | Total Group n = 100 | Male n = 61 | Female n = 39 | p-Value | |
|---|---|---|---|---|---|
| Civil Status | Single | 23 (23%) | 13 (21.3%) | 10 (25.6%) | 0.009 |
| Divorced | 5 (5%) | 2 (3.3%) | 3 (7.7%) | ||
| Widowed | 14 (14%) | 6 (9.8%) | 8 (20.5%) | ||
| Couple | 6 (6%) | 5 (8.2%) | 1 (2.6%) | ||
| Married | 52 (52%) | 35 (57.4%) | 17 (43.6%) | ||
| Study Level | I. Primary | 17 (17%) | 11 (18%) | 6 (15.40%) | 0.041 |
| C. Primary | 21 (21%) | 14 (23%) | 7 (17.90%) | ||
| Secondary | 22 (22%) | 9 (14.80%) | 13 (33.30%) | ||
| Degree | 14 (14%) | 9 (14.80%) | 5 (12.80%) | ||
| S. Degree | 26 (26%) | 18 (29.50%) | 8 20.50%) | ||
| Professional Activity | Student | 5 (5%) | 2 (3.3%) | 3 (7.7%) | 0.031 |
| Freelance | 18 (18%) | 10 (16.4%) | 8 (20.5%) | ||
| Employed | 35 (35%) | 22 (36.1%) | 13 (33.3%) | ||
| Unemployed | 6 (6%) | 5 (8.2%) | 1 (2.6%) | ||
| Retired | 36 (36%) | 22 (3, 6.1%) | 14 (35.9%) | ||
| Demographic and Descriptive Data | Total Group n = 100 | CG n = 25 | TB1 n = 25 | TB2 n = 25 | TB3 n = 25 | p-Value |
|---|---|---|---|---|---|---|
| Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | ||
| Age (years) | 51.70 ± 17.78 (48.19–55.24) | 44.28 ± 15.53 (37.86–50.69) | 48.00 ± 15.07 (41.77–54.22) | 49.80 ± 19.21 (41.86–57.73) | 64.80 ± 14.58 (58.78–70.81) | <0.001 † |
| Weight (Kg) | 72.55 ± 13.60 (69.85–75.25) | 74.12 ± 10.94 (69.60–78.63) | 70.68 ± 14.67 (64.62–76.73) | 70.06 ± 16.30 (63.33–76.79) | 75.36 ± 13.60 (69.85–75.25) | 0.189 † |
| Height (cm) | 1.67 ± 0.80 (1.65–1.68) | 1.72 ± 0.88 (1.69–1.76) | 1.64 ± 0.73 (1.61–1.67) | 1.65 ± 0.62 (1.62–1.67) | 1.65 ± 0.69 (1.62–1.68) | 0.002 † |
| BMI (Kg/m2) | 26.02 ± 4.24 (25.17–26.86) | 25.12 ± 3.05 (23.86–26.38) | 25.89 ± 4.50 (24.03–27.75) | 25.32 ± 4.45 (23.48–27.15) | 27.74 ± 4.52 (25.87–29.61) | 0.113 * |
| Social Characteristics | Total Group n = 100 | CG n = 25 | TB1 n = 25 | TB2 n = 25 | TB3 n = 25 | p-Value | |
|---|---|---|---|---|---|---|---|
| Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | |||
| Sex | Male | 61 (61%) | 9 (36%) | 17 (68%) | 18 (72%) | 17 (68%) | 0.031 |
| Female | 39 (39%) | 16 (64%) | 8 (32%) | 7 (28%) | 8 (32%) | ||
| Civil Status | Single | 23 (23%) | 10 (40%) | 5 (20%) | 7 (28%) | 1 (4%) | 0.009 |
| Divorced | 5 (5%) | 2 (8%) | 1 (4%) | 2 (8%) | 0 (0%) | ||
| Widowed | 14 (14%) | 2 (8%) | 1 (4%) | 2 (8%) | 9 (36%) | ||
| Couple | 6 (6%) | 0 (0%) | 1 (4%) | 3 (12%) | 2 (8%) | ||
| Married | 52 (52%) | 11 (44%) | 17 (68%) | 11 (44%) | 13 (52%) | ||
| Study Level | I. Primary | 17 (17%) | 1 (4%) | 2 (8%) | 5 (20%) | 9 (36%) | 0.041 |
| C. Primary | 21 (21%) | 3 (12%) | 8 (32%) | 4 (16%) | 6 (24%) | ||
| Secondary | 22 (22%) | 10 (40%) | 2 (8%) | 6 (24%) | 4 (16%) | ||
| Degree | 14 (14%) | 3 (12%) | 5 (20%) | 4 (16%) | 2 (8%) | ||
| S. Degree | 26 (26%) | 8 (32%) | 8 (32%) | 6 (24%) | 4 (16%) | ||
| Professional activity | Student | 5 (5%) | 2 (8%) | 1 (4%) | 2 (8%) | 0 (0%) | 0.031 |
| Freelance | 18 (18%) | 6 (24%) | 6 (24%) | 4 (16%) | 2 (8%) | ||
| Employed | 35 (35%) | 10 (40%) | 11 (44%) | 11 (44%) | 3 (12%) | ||
| Unemployed | 6 (6%) | 2 (8%) | 1 (4%) | 1 (4%) | 2 (8%) | ||
| Retired | 36 (36%) | 5 (20%) | 6 (24%) | 7 (28%) | 18 (72%) | ||
| FSHQ Domains | Total Group n = 100 | Male n = 61 | Female n = 39 | p-Value |
|---|---|---|---|---|
| Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | ||
| Foot pain | 63.46 ± 27.76 (57.95–68.97) | 59.48 ± 26.67 (52.65–66.31) | 69.69 ± 28.62 (60.41–78.97) | 0.042 |
| Foot function | 77.06 ± 25.17 (72.06–82.05) | 75.81 ± 26.38 (69.06–82.57) | 79.00 ± 23.36 (71.43–86.57) | 0.517 |
| Footwear | 39.25 ± 33.42 (32.61–45.88) | 29.91 ± 29.04 (22.47–37.35) | 53.84 ± 34.93 (42.52–65.16) | 0.001 |
| Foot health | 46.37 ± 32.42 (39.94–52.80) | 40.98 ± 31.67 (32.87–49.09) | 54.80 ± 32.16 (44.38–65.23) | 0.032 |
| General health | 72.00 ± 27.81 (66.48–77.51) | 70.65 ± 28.85 (63.26–78.04) | 74.10 ± 26.33 (65.57–82.64) | 0.590 |
| Physical activity | 84.88 ± 20.25 (80.86–88.90) | 82.33 ± 22.48 (76.57–88.09) | 88.88 ± 15.60 (83.82–93.94) | 0.112 |
| Social capacity | 78.87 ± 22.93 (74.32–83.42) | 77.04 ± 24.06 (70.88–83.21) | 81.73 ± 21.04 (74.90–88.55) | 0.391 |
| Vigor | 60.43 ± 19.72 (56.52–64.35) | 56.14 ± 20.04 (51.01–61.28) | 67.14 ± 17.42 (61.49–72.79) | 0.018 |
| FSHQ Domains | Total Group n = 100 | CG n = 25 | TB1 n = 25 | TB2 n = 25 | TB3 n = 25 |
|---|---|---|---|---|---|
| Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | Mean ± SD (Range) | |
| Foot pain | 63.46 ± 27.76 (57.95–68.97) | 89.30 ± 10.46 (84.98–93.61) | 72.07 ± 21.61 (63.15–80.99) | 54.10 ± 24.02 (44.18–64.01) | 38.40 ± 22.53 (29.09–47.70) |
| Foot function | 77.06 ± 25.17 (72.06–82.05) | 94.75 ± 7.58 (91.61–97.88) | 85.25 ± 17.75 (77.91–92.58) | 67.75 ± 24.38 (57.68–77.81) | 60.50 ± 29.57 (48.29–72.70) |
| Footwear | 39.25 ± 33.42 (32.61–45.88) | 67.66 ± 26.16 (56.86–78.46) | 31.00 ± 34.06 (16.93–45.06) | 31.66 ± 30.04 (19.26–44.06) | 26.66 ± 26.89 (15.56–37.76) |
| Foot health | 46.37 ± 32.42 (39.94–52.80) | 76.90 ± 24.70 (66.70–87.09) | 46.30 ± 29.85 (33.97–58.62) | 38.70 ± 29.85 (26.37–51.02) | 23.60 ± 19.27 (15.64–31.55) |
| General health | 72.00 ± 27.81 (66.48–77.51) | 84.40 ± 22.00 (75.31–93.48) | 73.20 ± 23.75 (63.39–83.00) | 68.00 ± 30.00 (55.61–80.38) | 62.40 ± 31.12 (49.55–75.24) |
| Physical activity | 84.88 ± 20.25 (80.86–88.90) | 95.33 ± 10.10 (91.16–99.50) | 89.33 ± 14.24 (83.45–95.21) | 79.77 ± 26.19 (68.96–90.59) | 75.11 ± 20.97 (66.45–83.77) |
| Social capacity | 78.87 ± 22.93 (74.32–83.42) | 86.00 ± 19.20 (78.07–93.92) | 83.50 ± 22.16 (74.35–92.64) | 72.50 ± 26.26 (61.65–83.34) | 73.50 ± 21.74 (64.52–82.47) |
| Vigor | 60.43 ± 19.72 (56.52–64.35) | 69.25 ± 17.20 (62.14–76.35) | 61.00 ± 16.36 (54.24–67.75) | 54.00 ± 22.88 (44.55–63.44) | 57.50 ± 19.59 (49.41–65.59) |
| FSHQ Domains | Post-Hoc p | ||
|---|---|---|---|
| CG vs. TB1 | CG vs. TB2 | CG vs. TB3 | |
| Foot pain | 0.001 | <0.001 | <0.001 |
| Foot function | 0.023 | <0.001 | <0.001 |
| Footwear | 0.033 | 0.014 | 0.005 |
| Foot health | 0.002 | <0.001 | <0.001 |
| General health | 0.040 | 0.045 | 0.036 |
| Physical activity | 0.067 | 0.039 | 0.001 |
| Social capacity | 0.726 | 0.123 | 0.072 |
| Vigor | 0.125 | 0.054 | 0.096 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazoteras-Pardo, V.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.; Palomo-López, P.; López-López, D.; Calvo-Lobo, C.; Romero-Morales, C.; Casado-Hernández, I. Degree of Impact of Tailor’s Bunion on Quality of Life: A Case–Control Study. Int. J. Environ. Res. Public Health 2021, 18, 736. https://doi.org/10.3390/ijerph18020736
Mazoteras-Pardo V, Becerro-de-Bengoa-Vallejo R, Losa-Iglesias M, Palomo-López P, López-López D, Calvo-Lobo C, Romero-Morales C, Casado-Hernández I. Degree of Impact of Tailor’s Bunion on Quality of Life: A Case–Control Study. International Journal of Environmental Research and Public Health. 2021; 18(2):736. https://doi.org/10.3390/ijerph18020736
Chicago/Turabian StyleMazoteras-Pardo, Victoria, Ricardo Becerro-de-Bengoa-Vallejo, Marta Losa-Iglesias, Patricia Palomo-López, Daniel López-López, César Calvo-Lobo, Carlos Romero-Morales, and Israel Casado-Hernández. 2021. "Degree of Impact of Tailor’s Bunion on Quality of Life: A Case–Control Study" International Journal of Environmental Research and Public Health 18, no. 2: 736. https://doi.org/10.3390/ijerph18020736
APA StyleMazoteras-Pardo, V., Becerro-de-Bengoa-Vallejo, R., Losa-Iglesias, M., Palomo-López, P., López-López, D., Calvo-Lobo, C., Romero-Morales, C., & Casado-Hernández, I. (2021). Degree of Impact of Tailor’s Bunion on Quality of Life: A Case–Control Study. International Journal of Environmental Research and Public Health, 18(2), 736. https://doi.org/10.3390/ijerph18020736