Playing Non-Professional Football in COVID-19 Time: A Narrative Review of Recommendations, Considerations, and Best Practices




Abstract
1. Introduction
Experimental Approach to the Problem
2. Method
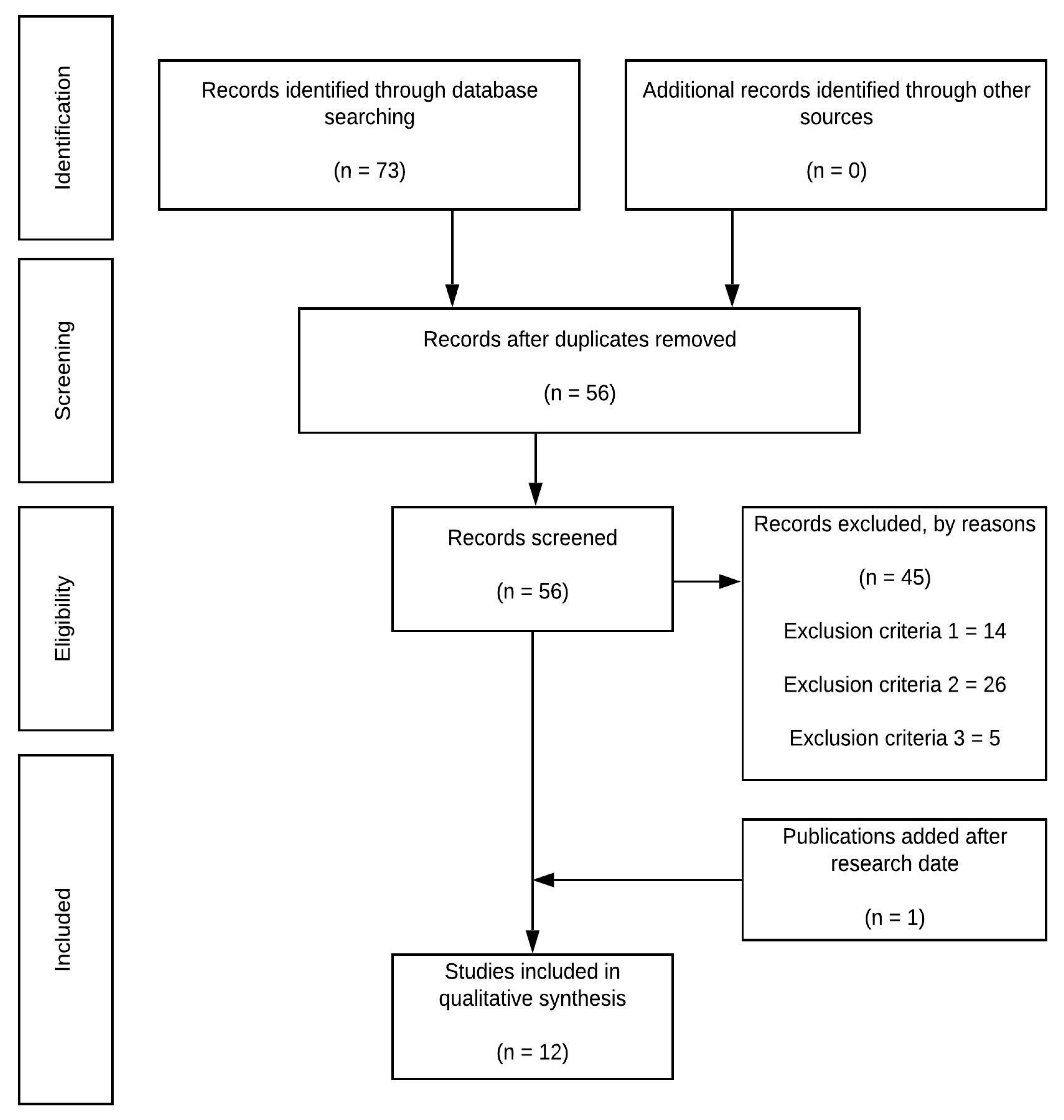
2.1. Data Sources
2.2. Data Selection
2.3. Data Collecting
3. Results
3.1. Assessment of Methodological Quality
3.2. Study Characteristics
4. Discussion
4.1. Training Load Management
4.2. Medical Considerations
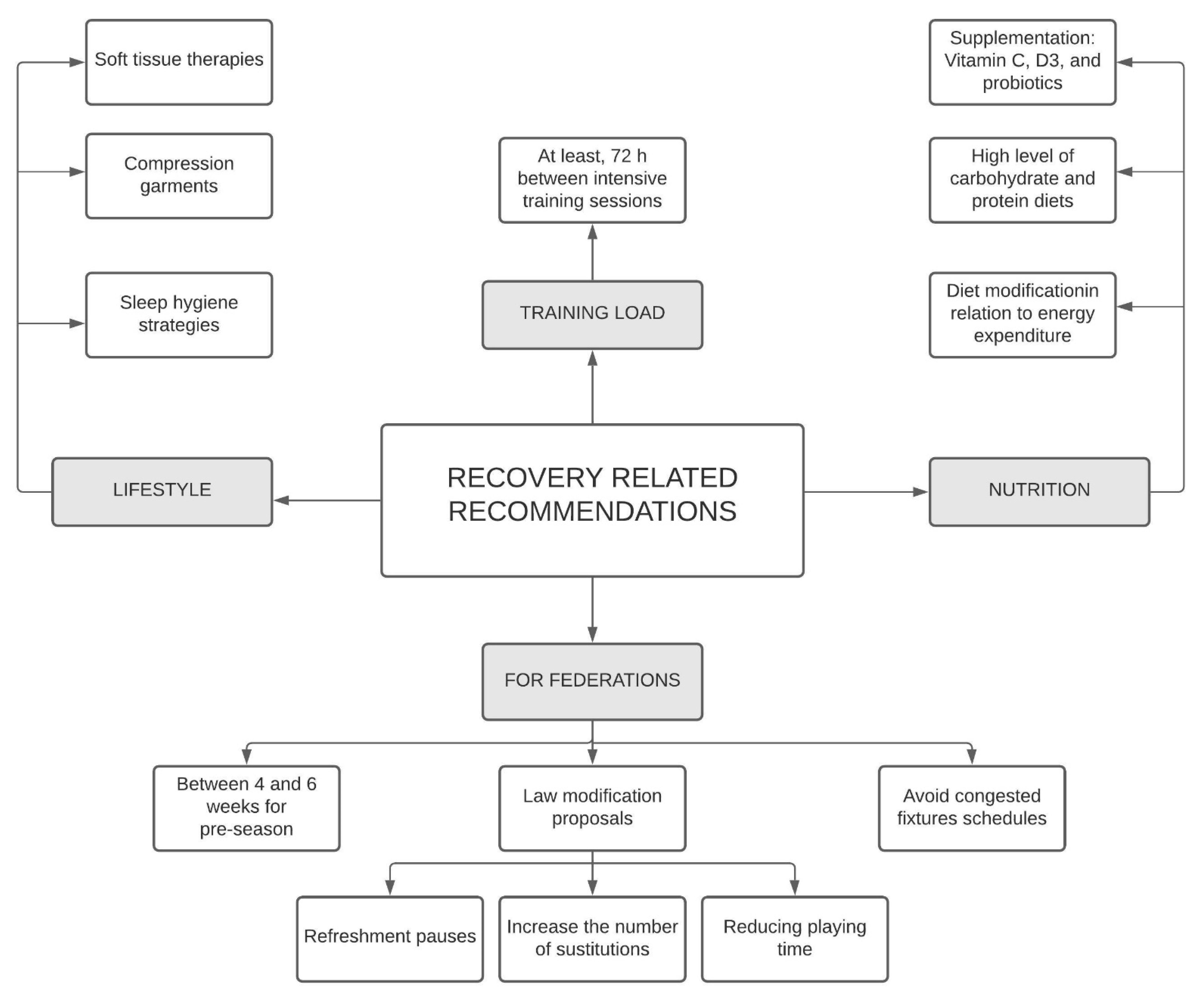
4.3. Recovery Recommendations
5. Certainties, Speculations, and Future Lines of Investigation
5.1. Training Load Management
5.2. Medical Issues
5.3. Recovery Related Issues
6. Study Limits
7. Practical Applications
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bisciotti, G.N.; Eirale, C.; Corsini, A.; Baudot, C.; Saillant, G.; Chalabi, H. Return to Football Training and Competition after Lockdown Caused by the COVID-19 Pandemic: Medical Recommendations. Biol. Sport 2020, 37, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, B.; Anderson, L.; Anglem, N.; Armstrong, S.; Baker, S.; Beable, S.; Burt, P.; Coleman, L.; Doughty, R.; Edwards, T.; et al. Medical Considerations for Supporting Elite Athletes during the Post-Peak Phase of the New Zealand COVID-19 Pandemic: A New Zealand Sporting Code Consensus. NZMA 2020, 133, 10. [Google Scholar]
- Primorac, D.; Matišić, V.; Molnar, V.; Bahtijarević, Z.; Polašek, O. Pre-Season Football Preparation in the Era of COVID-19: Croatian Football Association Model. J. Glob. Health 2020, 10, 010352. [Google Scholar] [CrossRef] [PubMed]
- Eirale, C.; Bisciotti, G.; Corsini, A.; Baudot, C.; Saillant, G.; Chalabi, H. Medical Recommendations for Home-Confined Footballers’ Training during the COVID-19 Pandemic: From Evidence to Practical Application. Biol. Sport 2020, 37, 203–207. [Google Scholar] [CrossRef]
- Guerrero-Calderón, B. The Effect of Short-Term and Long-Term Coronavirus Quarantine on Physical Performance and Injury Incidence in High-Level Soccer. Soccer Soc. 2020, 1–11. [Google Scholar] [CrossRef]
- Jukic, I.; Calleja-González, J.; Cos, F.; Cuzzolin, F.; Olmo, J.; Terrados, N.; Njaradi, N.; Sassi, R.; Requena, B.; Milanovic, L.; et al. Strategies and Solutions for Team Sports Athletes in Isolation Due to COVID-19. Sports 2020, 8, 56. [Google Scholar] [CrossRef]
- Mon-López, D.; García-Aliaga, A.; Ginés Bartolomé, A.; Muriarte Solana, D. How Has COVID-19 Modified Training and Mood in Professional and Non-Professional Football Players? Physiol. Behav. 2020, 227, 113148. [Google Scholar] [CrossRef]
- Stokes, K.A.; Jones, B.; Bennett, M.; Close, G.L.; Gill, N.; Hull, J.H.; Kasper, A.M.; Kemp, S.P.T.; Mellalieu, S.D.; Peirce, N.; et al. Returning to Play after Prolonged Training Restrictions in Professional Collision Sports. Int. J. Sports Med. 2020, 41, 895–911. [Google Scholar] [CrossRef]
- Smith, V.; Devane, D.; Begley, C.M.; Clarke, M. Methodology in Conducting a Systematic Review of Systematic Reviews of Healthcare Interventions. BMC Med. Res. Methodol. 2011, 11, 15. [Google Scholar] [CrossRef]
- Impellizzeri, F.M.; Franchi, M.V.; Sarto, F.; Meyer, T.; Coutts, A.J. Sharing Information Is Probably More Helpful than Providing Generic Training Recommendations on Return to Play after COVID-19 Home Confinement. Sci. Med. Footb. 2020, 4, 169–170. [Google Scholar] [CrossRef]
- Zabetakis, I.; Lordan, R.; Norton, C.; Tsoupras, A. COVID-19: The Inflammation Link and the Role of Nutrition in Potential Mitigation. Nutrients 2020, 12, 1466. [Google Scholar] [CrossRef] [PubMed]
- Messina, G.; Polito, R.; Monda, V.; Cipolloni, L.; Di Nunno, N.; Di Mizio, G.; Murabito, P.; Carotenuto, M.; Messina, A.; Pisanelli, D.; et al. Functional Role of Dietary Intervention to Improve the Outcome of COVID-19: A Hypothesis of Work. IJMS 2020, 21, 3104. [Google Scholar] [CrossRef] [PubMed]
- Jain, V.K.; Lal, H.; Patralekh, M.K.; Vaishya, R. Fracture Management during COVID-19 Pandemic: A Systematic Review. J. Clin. Orthop. Trauma 2020, 11, S431–S441. [Google Scholar] [CrossRef] [PubMed]
- Gentil, P.; Jimenez, A.; Mayo, X.; Pereira, E.G.; Alcaraz, P.; Bianco, A.; Paoli, A.; Papeschi, J.; Junior, L.C.C. Resistance Training Safety during and after the SARS-Cov-2 Outbreak: Practical Recommendations. Biomed Res. Int. 2020, 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.G.; Hull, J.H.; Rogers, J.; Pollock, N.; Dodd, M.; Haines, J.; Harris, S.; Loosemore, M.; Malhotra, A.; Pieles, G.; et al. Cardiorespiratory Considerations for Return--to--play in Elite Athletes after COVID-19 Infection: A Practical Guide for Sport and Exercise Medicine Physicians. Br. J. Sports Med. 2020, 54, 1157–1161. [Google Scholar] [CrossRef]
- Bentlage, E.; Ammar, A.; How, D.; Ahmed, M.; Trabelsi, K.; Chtourou, H.; Brach, M. Practical Recommendations for Maintaining Active Lifestyle during the COVID-19 Pandemic: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 6265. [Google Scholar] [CrossRef]
- Dove, J.; Gage, A.; Kriz, P.; Tabaddor, R.R.; Owens, B.D. COVID-19 and Review of Current Recommendations for Return to Athletic Play. Sports Med. 2020, 103, 15–20. [Google Scholar]
- Herrero-Gonzalez, H.; Martín-Acero, R.; Del Coso, J.; Lalín-Novoa, C.; Pol, R.; Martín-Escudero, P.; De la Torre, A.I.; Hughes, C.; Mohr, M.; Biosca, F.; et al. Position Statement of the Royal Spanish Football Federation for the Resumption of Football Activities after the COVID-19 Pandemic (June 2020). Br. J. Sports Med. 2020, 54, 1133–1134. [Google Scholar] [CrossRef]
- Mohr, M.; Nassis, G.P.; Brito, J.; Randers, M.B.; Castagna, C.; Parnell, D.; Krustrup, P. Return to Elite Football after the COVID-19 Lockdown. Manag. Sport Leis. 2020, 1–9. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Castagna, C.; Bizzini, M.; Leguizamon, A.P.; Pizzi, A.; Torquati, R.; Póvoas, S. Considerations and Best Practices for Elite Football Officials Return to Play after COVID-19 Confinement. Manag. Sport Leis. 2020, 1–8. [Google Scholar] [CrossRef]
- Sarto, F.; Impellizzeri, F.M.; Spörri, J.; Porcelli, S.; Olmo, J.; Requena, B.; Suarez-Arrones, L.; Arundale, A.; Bilsborough, J.; Buchheit, M.; et al. Impact of Potential Physiological Changes Due to COVID-19 Home Confinement on Athlete Health Protection in Elite Sports: A Call for Awareness in Sports Programming. Sports Med. 2020, 50, 1417–1419. [Google Scholar] [CrossRef] [PubMed]
- Nassis, G.P.; Massey, A.; Jacobsen, P.; Brito, J.; Randers, M.B.; Castagna, C.; Mohr, M.; Krustrup, P. Elite Football of 2030 Will Not Be the Same as That of 2020: Preparing Players, Coaches, and Support Staff for the Evolution. Scand. J. Med. Sci. Sports 2020, 30, 962–964. [Google Scholar] [CrossRef] [PubMed]
- Huyghe, T.; Bird, S.; Calleja-González, J.; Alcaraz, P.E. Season Suspension and Summer Extension: Unique Opportunity for Professional Team-Sport Athletes and Support Staff During and Following the COVID-19 Crisis. Front. Sports Act. Living 2020, 2, 98. [Google Scholar] [CrossRef]
- Wong, A.Y.-Y.; Ling, S.K.-K.; Louie, L.H.-T.; Law, G.Y.-K.; So, R.C.-H.; Lee, D.C.-W.; Yau, F.C.-F.; Yung, P.S.-H. Impact of the COVID-19 Pandemic on Sports and Exercise. Asia-Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2020, 22, 39–44. [Google Scholar] [CrossRef]
- Carmody, S.; Ahmad, I.; Gouttebarge, V.; Malhotra, A.; Glover, D.; Massey, A. Infographics. Football-Specific Strategies to Reduce COVID-19 Transmission. Br. J. Sports Med. 2020, 54, 1362–1364. [Google Scholar] [CrossRef]
- Delgado-Bordonau, J.L.; Mendez-Villanueva, A. Tactical Periodization: Mourinho’s Best-Kept Secret? Soccer Nscaa J. 2012, 57, 29–34. [Google Scholar]
- Tarragó, J.R.; Massafret-Marimón, M.; Seirul·lo, F.; Cos, F. Entrenamiento En Deportes de Equipo: El Entrenamiento Estructurado En El FCB. Apunts 2019, 103–114. [Google Scholar] [CrossRef]
- Pons Alcalá, E.; Martin Garcia, A.; Guitart Trench, M.; Guerrero Hernández, I.; Ramon Tarragó, J.; Seirul·lo Vargas, F.; Cos Morera, F. Entrenamiento en deportes de equipo: El entrenamiento optimizador en el Fútbol Club Barcelona. Apunts 2020, 4, 55–66. [Google Scholar] [CrossRef]
- Clemente, F.M.; Seerden, G.; van der Linden, C.M.I. Quantifying the Physical Loading of Five Weeks of Pre-Season Training in Professional Soccer Teams from Dutch and Portuguese Leagues. Physiol. Behav. 2019, 209, 112588. [Google Scholar] [CrossRef]
- Sarmento, H.; Marcelino, R.; Anguera, M.T.; CampaniÇo, J.; Matos, N.; LeitÃo, J.C. Match Analysis in Football: A Systematic Review. J. Sports Sci. 2014, 32, 1831–1843. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, D.; da Silva, C.D.; Hill-Haas, S.; Wong, D.P.; Natali, A.J.; De Lima, J.R.P.; Filho, M.G.B.B.; Marins, J.J.C.B.; Garcia, E.S.; Karim, C. Heart Rate Monitoring in Soccer: Interest and Limits During Competitive Match Play and Training, Practical Application. J. Strength Cond. Res. 2012, 26, 2890–2906. [Google Scholar] [CrossRef] [PubMed]
- Bangsbo, J. Physiological demands of football. Sports Sci. Exch. 2014, 27, 6. [Google Scholar]
- Drust, B.; Reilly, T.; Cable, N.T. Physiological Responses to Laboratory-Based Soccer-Specific Intermittent and Continuous Exercise. J. Sports Sci. 2000, 18, 885–892. [Google Scholar] [CrossRef] [PubMed]
- McAloon, C.; Collins, Á.; Hunt, K.; Barber, A.; Byrne, A.W.; Butler, F.; Casey, M.; Griffin, J.; Lane, E.; McEvoy, D.; et al. Incubation Period of COVID-19: A Rapid Systematic Review and Meta-Analysis of Observational Research. BMJ Open 2020, 10, e039652. [Google Scholar] [CrossRef]
- Filetti, C.; Ruscello, B.; D’Ottavio, S.; Fanelli, V. A Study of Relationships among Technical, Tactical, Physical Parameters and Final Outcomes in Elite Soccer Matches as Analyzed by a Semiautomatic Video Tracking System. Percept. Mot. Ski. 2017, 124, 601–620. [Google Scholar] [CrossRef]
- Coutinho, D.; Gonçalves, B.; Santos, S.; Travassos, B.; Wong, D.P.; Sampaio, J. Effects of the Pitch Configuration Design on Players’ Physical Performance and Movement Behaviour during Soccer Small-Sided Games. Res. Sports Med. 2019, 27, 298–313. [Google Scholar] [CrossRef]
- Coutinho, D.; Santos, S.; Gonçalves, B.; Travassos, B.; Wong, D.P.; Schöllhorn, W.; Sampaio, J. The Effects of an Enrichment Training Program for Youth Football Attackers. PLoS ONE 2018, 13, e0199008. [Google Scholar] [CrossRef]
- Gonçalves, B.; Santos, S.; Mateus, N.; Sampaio, J.; Leite, N.; Silva, A. Individual and Collective Creativity in Young Footballers. Egitania Sci. 2015, 8, 33. [Google Scholar]
- Santos, S.; Jiménez, S.; Sampaio, J.; Leite, N. Effects of the Skills4Genius Sports-Based Training Program in Creative Behavior. PloS ONE 2017, 12, e0172520. [Google Scholar] [CrossRef]
- Santos, S.; Coutinho, D.; Gonçalves, B.; Schöllhorn, W.; Sampaio, J.; Leite, N. Differential Learning as a Key Training Approach to Improve Creative and Tactical Behavior in Soccer. Res. Q. Exerc. Sport 2018, 89, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, B.; Mendes, R.; Folgado, H.; Figueiredo, P.; Travassos, B.; Barros, H.; Campos-Fernandes, A.; Beckert, P.; Brito, J. Can Tracking Data Help in Assessing Interpersonal Contact Exposure in Team Sports during the COVID-19 Pandemic? Sensors 2020, 20, 6163. [Google Scholar] [CrossRef] [PubMed]
- van Doreman, N.; Bushmaker, T.; Morris, D. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Hughes, D.; Saw, R.; Perera, N.K.P.; Mooney, M.; Wallett, A.; Cooke, J.; Coatsworth, N.; Broderick, C. The Australian Institute of Sport Framework for Rebooting Sport in a COVID-19 Environment. J. Sci. Med. Sport 2020, 23, 639–663. [Google Scholar] [CrossRef]
- Barker-Davies, R.M.; O’Sullivan, O.; Senaratne, K.P.P.; Baker, P.; Cranley, M.; Dharm-Datta, S.; Ellis, H.; Goodall, D.; Gough, M.; Lewis, S.; et al. The Stanford Hall Consensus Statement for Post-COVID-19 Rehabilitation. Br. J. Sports Med. 2020, 54, 949–959. [Google Scholar] [CrossRef]
- Lodi, E.; Scavone, A.; Carollo, A.; Guicciardi, C.; Reggianini, L.; Savino, G.; Modena, M.G. Ripresa dell’attività sportiva in seguito a pandemia COVID-19. Come comportarsi? G. Ital. Cardiol. 2020, 21, 9. [Google Scholar]
- Meyer, T.; Mack, D.; Donde, K.; Harzer, O.; Krutsch, W.; Rössler, A.; Kimpel, J.; von Laer, D.; Gärtner, B.C. Successful Return to Professional Men’s Football (Soccer) Competition after the COVID-19 Shutdown: A Cohort Study in the German Bundesliga. Br. J. Sports Med. 2021, 55, 62–66. [Google Scholar] [CrossRef]
- Gleeson, M. Immune Function and Exercise. Eur. J. Sport Sci. 2004, 4, 52–66. [Google Scholar] [CrossRef]
- Mortatti, A.L.; Moreira, A.; Aoki, M.S.; Crewther, B.T.; Castagna, C.; de Arruda, A.F.S.; Filho, J.M. Effect of Competition on Salivary Cortisol, Immunoglobulin A, and Upper Respiratory Tract Infections in Elite Young Soccer Players. J. Strength Cond. Res. 2012, 26, 1396–1401. [Google Scholar] [CrossRef]
- Moreira, A.; Mortatti, A.L.; Arruda, A.F.S.; Freitas, C.G.; de Arruda, M.; Aoki, M.S. Salivary IgA Response and Upper Respiratory Tract Infection Symptoms During a 21-Week Competitive Season in Young Soccer Players. J. Strength Cond. Res. 2014, 28, 467–473. [Google Scholar] [CrossRef]
- Lopes, R.F.; Minuzzi, L.G.; Figueiredo, A.J.; Gonçalves, C.; Tessitore, A.; Capranica, L.; Teixeira, A.M.; Rama, L. Upper Respiratory Symptoms (URS) and Salivary Responses across a Season in Youth Soccer Players: A Useful and Non-Invasive Approach Associated to URS Susceptibility and Occurrence in Young Athletes. PLoS ONE 2020, 15, e0236669. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, P.; Nassis, G.P.; Brito, J. Within-Subject Correlation Between Salivary IgA and Measures of Training Load in Elite Football Players. Int. J. Sports Physiol. Perform. 2019, 14, 847–849. [Google Scholar] [CrossRef] [PubMed]
- Morgans, R.; Owen, A.; Doran, D.; Drust, B.; Morton, J.P. Prematch Salivary Secretory Immunoglobulin A in Soccer Players From the 2014 World Cup Qualifying Campaign. Int. J. Sports Physiol. Perform. 2015, 10, 401–403. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.L.; Morgans, R.; Kavanagh, R.; Djaoui, L. Salivary IgA and Pre-Training Wellness Status across an International Soccer Qualifying and Finals Campaign (Euro 2016). Int. J. Sports Sci. Coach. 2018, 13, 794–803. [Google Scholar] [CrossRef]
- Fredericks, S. Changes in Salivary Immunoglobulin A (IgA) Following Match-Play and Training among English Premiership Footballers. Med. J. Malays. 2012, 67, 5. [Google Scholar]
- Peñailillo, L.; Maya, L.; Niño, G.; Torres, H.; Zbinden-Foncea, H. Salivary Hormones and IgA in Relation to Physical Performance in Football. J. Sports Sci. 2015, 33, 2080–2087. [Google Scholar] [CrossRef]
- Page, R.M.; Marrin, K.; Brogden, C.M.; Greig, M. Physical Response to a Simulated Period of Soccer-Specific Fixture Congestion. J. Strength Cond. Res. 2019, 33, 1075–1085. [Google Scholar] [CrossRef]
- Putlur, P.; Foster, C.; Miskowski, J.A.; Kane, M.K.; Burton, S.E.; Scheett, T.P.; McGuigan, M.R. Alteration of Immune Function in Women Collegiate Soccer Players and College Student. J. Sports Sci. Med. 2004, 3, 234–243. [Google Scholar]
- Nakamura, D.; Akimoto, T.; Suzuki, S.; Kono, I. Daily Changes of Salivary Secretory Immunoglobulin A and Appearance of Upper Respiratory Symptoms during Physical Training. Sports Med. Phys. Fit. 2006, 46, 152–157. [Google Scholar]
- Besedovsky, L.; Lange, T.; Haack, M. The Sleep-Immune Crosstalk in Health and Disease. Physiol. Rev. 2019, 99, 1325–1380. [Google Scholar] [CrossRef]
- Gonçalves, B.; Esteves, P.; Folgado, H.; Ric, A.; Torrents, C.; Sampaio, J. Effects of Pitch Area-Restrictions on Tactical Behavior, Physical, and Physiological Performances in Soccer Large-Sided Games. J. Strength Cond. Res. 2017, 31, 2398–2408. [Google Scholar] [CrossRef] [PubMed]
- Moreira, A.; Arsati, F.; Cury, P.R.; Franciscon, C.; de Oliveira, P.R.; de Araújo, V.C. Salivary Immunoglobulin A Response to a Match in Top-Level Brazilian Soccer Players. J. Strength Cond. Res. 2009, 23, 1968–1973. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.L.; Wong, D.P.; Dunlop, G.; Groussard, C.; Kebsi, W.; Dellal, A.; Morgans, R.; Zouhal, H. High-Intensity Training and Salivary Immunoglobulin A Responses in Professional Top-Level Soccer Players: Effect of Training Intensity. J. Strength Cond. Res. 2016, 30, 2460–2469. [Google Scholar] [CrossRef] [PubMed]
- Olthof, S.; Frencken, W.; Lemmink, K. A Match-Derived Relative Pitch Area Facilitates the Tactical Representativeness of Small-Sided Games for the Official Soccer Match. J. Strength Cond. Res. 2019, 33, 523–530. [Google Scholar] [CrossRef]
- Vitale, J.A.; La Torre, A.; Banfi, G.; Bonato, M. Acute Sleep Hygiene Strategy Improves Objective Sleep Latency Following a Late-Evening Soccer-Specific Training Session: A Randomized Controlled Trial. J. Sports Sci. 2019, 37, 2711–2719. [Google Scholar] [CrossRef]
- Nédélec, M.; Halson, S.; Delecroix, B.; Abaidia, A.-E.; Ahmaidi, S.; Dupont, G. Sleep Hygiene and Recovery Strategies in Elite Soccer Players. Sports Med. 2015, 45, 1547–1559. [Google Scholar] [CrossRef]
- Bonato, M.; Merati, G.; La Torre, A.; Saresella, M.; Marventano, I.; Banfi, G.; Vitale, J.A. Effect of Acute Sleep Hygiene on Salivary Cortisol Level Following A Late Night Soccer-Specific Training Session. J. Sports Sci. Med. 2020, 19, 235–236. [Google Scholar]



{kind=link}
{kind=link}
| Reference | Recommendations about? | Training Sessions (See Table 2) | Medical Issues (See Table 3) | Recovery Strategies (See Figure 2) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aerobic Training | Anaerobic Training | Speed/Strength/Neuromuscular Training | Ball Drills | Injury Prevention Programs/Issues | Social Issues | Hygiene Issues | Test | Nutritional | Wellness | Training Load | Federation Issues | ||
| Bisciotti et al. [1] | TL management Injury prevention | Intensity progression (from aerobic to anaerobic training) | Three phases: power production; plyometric; repeated sprints | For joints: multicomponent prevention programs. For neuromuscular control: Single leg exercises | Pre competition medical assessment | ||||||||
| 10 sessions At 70–75% Slow rhythmic | Stimulation of fast twitch fibers. At 50–85% High rhythmic | ||||||||||||
| Mohr et al. [19] | TL management | Progressiveness of loading From moderate to high intensity, combined with basic power training | Warm up with ball circuit Specificity (SSG) | 3–5 weeks pre competition period | 2 m of social distance at initial stage | Carbohydrate enrichment diet | Proper sleep Compression garments | Avoid exhaustive TL | Reduce playing time Increase substitutions | ||||
| Castagna et al. [21] | TL management Guide safe | Maximal and submaximal test Consider the ideal worst match scenario to prepare match psychological and physiological demands Weekly TL progression < 10–20% | Social distancing | Sanitized VAR rooms | Repeated test PCMA | 24–48 h recovery time post session | Reduce match duration (30-40 min/half) | ||||||
| Herrero-González et al. [18] | TL management Safety | Phase 1: individualized test (power, endurance, joint mobility and body composition). Phase 2: football specific games including power, endurance, high-intensity intermittent exercise capacity and speed | Football specific training phase | Pre training Temperature Respiratory and cardiovascular screening | 72 h between matches | 4-6 weeks before competition Refreshment pauses Increase the number of substitutions | |||||||
| Sarto et al. [22] | Awareness in sport programming | Improve physiological and mental functions Involve all stakeholders in the decisions Ensure recovery, specially, during congested fixtures | Allow prolonged pre-season | ||||||||||
| Nassis et al. [23] | TL management | The use of technology for real time feedback Positional and individual variability in fatigue and recovery patterns should be established | |||||||||||
| High-intensity bouts with emphasis not only on the number of bouts but also on the density too (i.e., number of high-intensity efforts within 1–2 min) | |||||||||||||
| Hamilton et al. [2] | TL management Safety | Multi-disciplinary planning for reintroduction of training volume and intensity, taking into consideration both individual and squad-based factors | Consider squad-based factors | Open areas Face mask | Alcohol based cleaning products | Triage Temperature NSAID when managing URTI | Adapt diet to a new energy expenditure Consume protein regularly | Sleep quality low mood Soft tissue recovery strategy | Well organized TL | ||||
| Stokes et al. [8] | TL management Safety | Six-week training blocks. Assess with RPE and other indicators of reduced cardiopulmonary function. Progression through small increments in intensity (e.g., speed, distance kicked/passed, player numbers) and volume (e.g., nº repetitions, duration, nº of player). Introduction of randomization, reaction time, fatigue and decision making | Symptom free for 7 days and return no sooner than day 10 | ||||||||||
| From SGG with small areas to greater | |||||||||||||
| Huyghe et al. [24] | TL management and recovery | Consider a preliminary baseline with reduced loads upon return to competition | |||||||||||
| 2/4 weeks of unstructured, low impact, and low volume activities. 50/30/20/10 rule | Near competition HIIT (87–97% peak HR) | Nutrition education. Carbohydrate ingestion. Quercetin-rich foods | |||||||||||
| Wong et al. [25] | TL recovery and safety | Physical distancing | Clean equipment, surfaces. Avoid contact | Temperature Declare FTOCC status | 72 h between matches high intensity sessions | ||||||||
| Carmody et al. [26] | Safety | Read COVID-19 guidelines | Educate players. Installation disinfection. No sharing of thingsFace mask. | Any person with symptoms should be at home for, at least, 14 days | |||||||||
| Primorac et al. [3] | Training phases Safety | Return to physical activity in 4 phases: (1) training in small groups (< 5 players); (2) training of the entire team; (3) national league competitions; (4) international competitions | 5 m physical distance. Training outdoors.Go home in the same transport | No sharing | Negative consecutive two PCR pharyngeal swabs over a 5-day interval | ||||||||
| Phase 1 | Phase 2 | Phase 3 | |||
|---|---|---|---|---|---|
| Sub-Phase 1 (1st Week) | Sub-Phase 1 (3rd Week) | Sub-Phase 1 (5th Week) | |||
| Conditional Dimension | Technic/Tactic Dimension | Conditional Dimension | Technic/Tactic Dimension | Conditional Dimension | Technic/Tactic Dimension |
| 1. Aerobic adaptation (low intensity). 2. Maintain speed and endurance. | Individual ball drills | 1. Aerobic-anaerobic training (moderate). 1.1. Intermittent exercise 1. 2. Speed and endurance production. 3. Selective stimulation of the fast twitch fibers. 4. Plyometric training 1. | High-intensity ball drills 1 | 1. Aerobic-anaerobic training (high-intensity). 1.1. Repeated sprint ability 2. 2. Speed training. | High intensity ball drills 2 |
| 1. Aerobic to anaerobic training (from low to moderate). 2. Maintenance and production of speed and endurance. | 1. Aerobic-anaerobic training (from moderate to high). 1.1. Intermittent exercise 2. 1.2. Repeated sprint ability 1. 2. From speed and endurance production to speed training. 3. Selective stimulation of the fast twitch fibers. 4. Plyometric training 2. 5. Repeated sprint ability. | RETURN TO PLAYING FOOTBALL | |||
| INDIVIDUAL TRAINING PHYSICAL DISTANCING | GROUP TRAINING FOOTBALL-SPECIFIC TRAINING DRILLS | ||||
| General Recommendations | ||
|---|---|---|
| ||
| Pre-Training | During Training | After Training |
|
|
|
| Education | Planning to Return to Match Officials | After Confinament |
Educate player in:
|
| Re-training could start after COVID-19 pre-competitive medical assessment:
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rico-González, M.; Pino-Ortega, J.; Ardigò, L.P. Playing Non-Professional Football in COVID-19 Time: A Narrative Review of Recommendations, Considerations, and Best Practices. Int. J. Environ. Res. Public Health 2021, 18, 568. https://doi.org/10.3390/ijerph18020568
Rico-González M, Pino-Ortega J, Ardigò LP. Playing Non-Professional Football in COVID-19 Time: A Narrative Review of Recommendations, Considerations, and Best Practices. International Journal of Environmental Research and Public Health. 2021; 18(2):568. https://doi.org/10.3390/ijerph18020568
Chicago/Turabian StyleRico-González, Markel, José Pino-Ortega, and Luca Paolo Ardigò. 2021. "Playing Non-Professional Football in COVID-19 Time: A Narrative Review of Recommendations, Considerations, and Best Practices" International Journal of Environmental Research and Public Health 18, no. 2: 568. https://doi.org/10.3390/ijerph18020568
APA StyleRico-González, M., Pino-Ortega, J., & Ardigò, L. P. (2021). Playing Non-Professional Football in COVID-19 Time: A Narrative Review of Recommendations, Considerations, and Best Practices. International Journal of Environmental Research and Public Health, 18(2), 568. https://doi.org/10.3390/ijerph18020568