Depression in Children and Adolescents on the Qinghai-Tibet Plateau: Associations with Resilience and Prosocial Behavior

 , ,
, ,  , ,
, , 
Abstract
1. Introduction
2. Methods
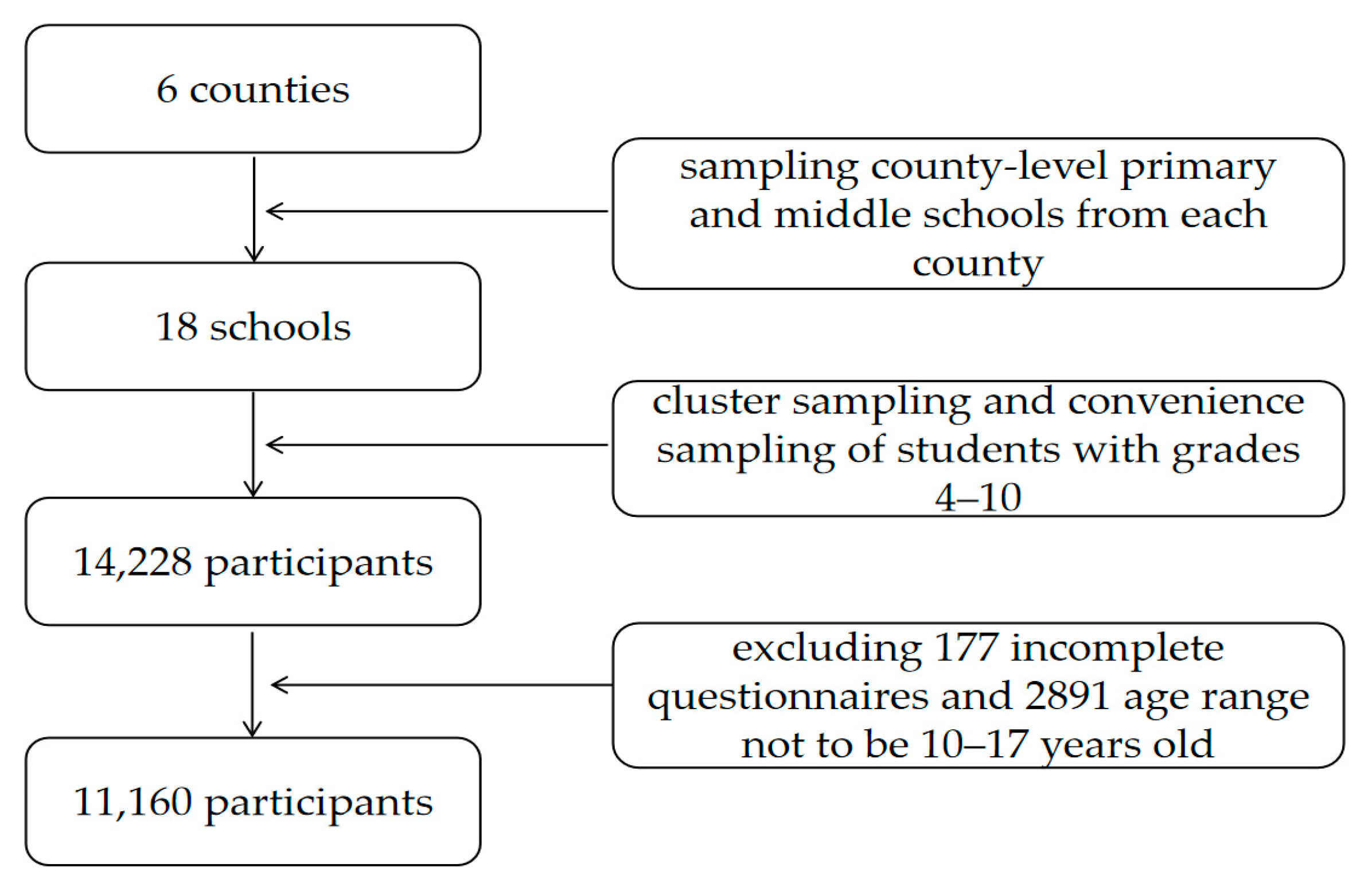
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Descriptive Analyses
3.2. Correlations between Study Variables
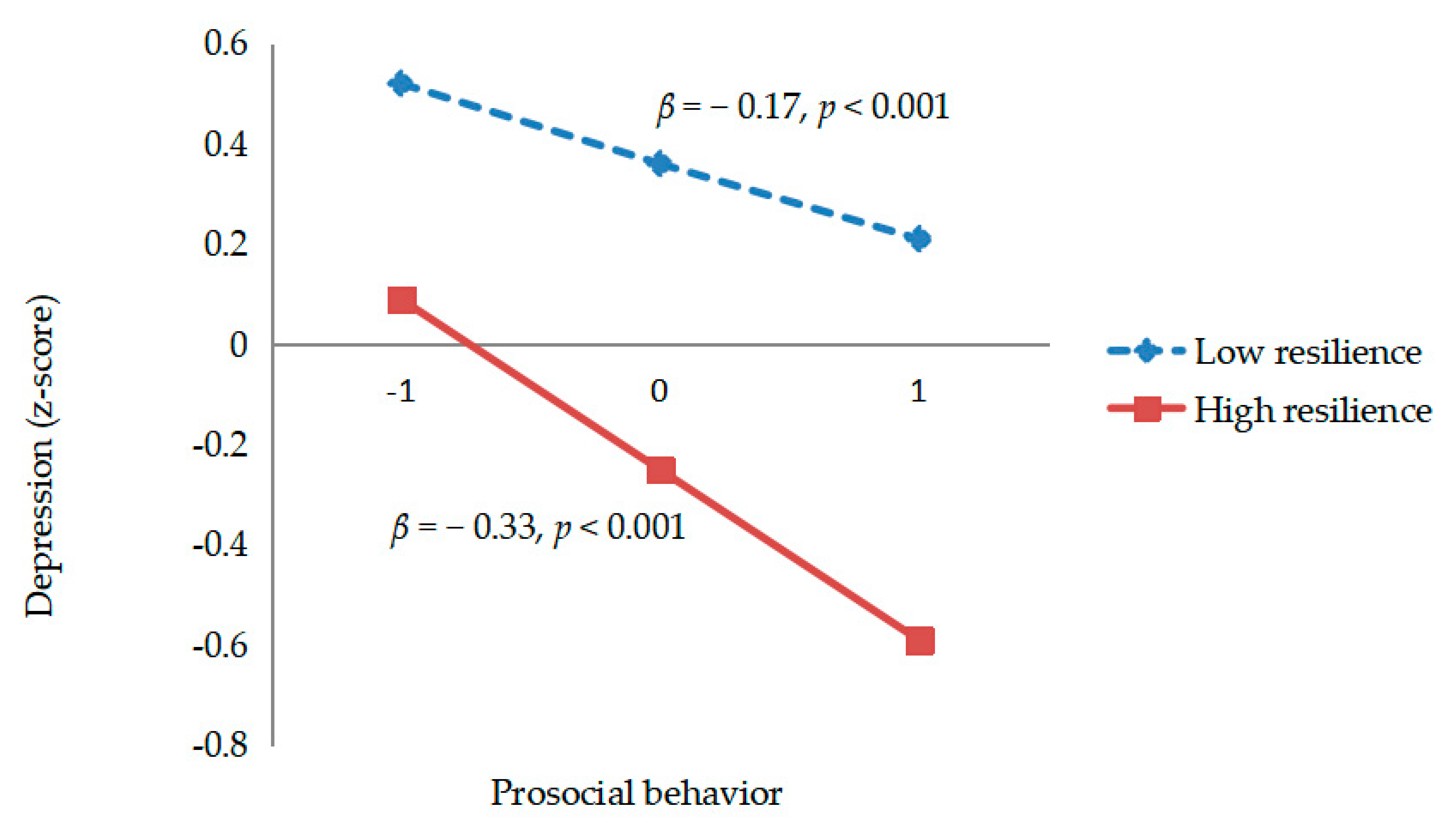
3.3. Moderating Analyses
4. Discussion
4.1. Limitations and Future Directions
4.2. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Adolescents: Health Risks and Solutions. 2018. Available online: http://www.who.int/news-room/fact-sheets/detail/adolescents-healthrisks-and-solutions (accessed on 1 May 2018).
- Roberts, R.E.; Attkisson, C.C.; Rosenblatt, A. Prevalence of psychopathology among children and adolescents. Am. J. Psychiatry 1998, 155, 715–725. [Google Scholar] [PubMed]
- Rao, W.W.; Xu, D.D.; Cao, X.L.; Wen, S.Y.; Che, W.I.; Ng, C.H.; Ungvari, G.S.; He, F.; Xiang, Y.T. Prevalence of depressive symptoms in children and adolescents in China: A meta-analysis of observational studies. Psychiatry Res. 2018, 272, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.F.; Tang, S.Q.; Ren, Z.H.; Wong, D.F.K. Prevalence of depressive symptoms among adolescents in secondary school in mainland China: A systematic review and meta-analysis. J. Affect. Disord. 2018, 245, 498–507. [Google Scholar] [CrossRef]
- DelMastro, K.; Hellem, T.; Kim, N.; Kondo, D.; Sung, Y.H.; Renshaw, P.F. Incidence of major depressive episode correlates with elevation of substate region of residence. J. Affect. Disord. 2011, 129, 376–379. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, M.; Yamanaka, G.; Yamamoto, N.; Nakaoka, T.; Okumiya, K.; Matsubayashi, K.; Otsuka, K.; Sakura, H. Depression and altitude: Cross-sectional community-based study among elderly high-altitude residents in the Himalayan regions. Cult. Med. Psychiatry 2016, 40, 1–11. [Google Scholar] [CrossRef]
- Ray, K.; Dutta, A.; Panjwani, U.; Thakur, L.; Anand, J.P.; Kumar, S. Hypobaric hypoxia modulates brain biogenic amines and disturbs sleep architecture. Neurochem. Int. 2011, 58, 112–118. [Google Scholar] [CrossRef]
- Maldonado, M.D.; Reiter, R.J.; Pérez-San-Gregorio, M.A. Melatonin as a potential therapeutic agent in psychiatric illness. Hum. Psychopharmacol. Clin. Exp. 2009, 24, 391–400. [Google Scholar] [CrossRef]
- Wei, G.; He, X.; Liu, X. The present status of mental health services in the Tibet region of China. J. Ment. Health 2004, 13, 43–46. [Google Scholar] [CrossRef]
- Chua, L.W.; Milfont, T.L.; Jose, P.E. Coping skills help explain how future-oriented adolescents accrue greater well-being over time. J. Youth Adolesc. 2015, 44, 2028–2041. [Google Scholar] [CrossRef]
- Wellhoner, M.; Lee, A.C.; Deutsch, K.; Wiebenga, M.; Weingrad, L. Maternal and child health in Yushu, Qinghai Province, China. Int. J. Equity Health. 2001, 10, 42–52. [Google Scholar] [CrossRef]
- Xie, L.; Wei, G.; Xu, Y.; Huang, Y.; Guo, W.J. Psychiatric epidemiology and mental health service in the Tibet autonomous region of the people’s republic of China. Shanghai Arch. Psychiatry 2018, 30, 127–130. [Google Scholar] [PubMed]
- Wang, J.Z.; Zhou, Y.Y.; Liang, Y.M.; Liu, Z.K. A large sample survey of Tibetan people on the Qinghai–Tibet Plateau: Current situation of depression and risk factors. Int. J. Environ. Res. Public Health 2020, 17, 289. [Google Scholar] [CrossRef] [PubMed]
- Penner, L.A.; Dovidio, J.F.; Piliavin, J.A.; Schroeder, D.A. Prosocial behavior: Multilevel perspectives. Annu. Rev. Psychol. 2005, 56, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Fehr, E.; Fischbacher, U. The nature of human altruism. Nature 2003, 425, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Dovidio, J.F.; Piliavin, J.A.; Gaertner, S.L.; Schroeder, D.A.; Clark, R.D. The arousal: Cost-reward model and the process of intervention: A review of the evidence. In Review of Personality and Social Psychology; Clark, M.S., Ed.; Prosocial Behavior; Sage Publications: Thousand Oaks, CA, USA, 1991; pp. 86–118. [Google Scholar]
- Hilbe, C.; Sigmund, K. Incentives and opportunism: From the carrot to the stick. Proc. R. Soc. B 2010, 277, 2427–2433. [Google Scholar] [CrossRef]
- Eisenberg, N.; Fabes, R.A.; Spinrad, T.L. Prosocial development. In Handbook of Child Psychology; Eisenberg, N., Ed.; Wiley: New York, NY, USA, 2006; pp. 646–718. [Google Scholar]
- Grant, A.M.; Sonnentag, S. Doing good buffers against feeling bad: Prosocial impact compensates for negative task and self-evaluations. Organ. Behav. Hum. Decis. Process. 2010, 111, 13–22. [Google Scholar] [CrossRef]
- Haroz, E.E.; Murray, L.K.; Bolton, P.; Betancourt, T.; Bass, J.K. Adolescent resilience in northern Uganda: The role of social support and prosocial behavior in reducing mental health problems. J. Res. Adolesc. 2013, 23, 138–148. [Google Scholar] [CrossRef]
- Fujiwara, T. The role of altruistic behavior in generalized anxiety disorder and major depression among adults in the united states. J. Affect. Disord. 2007, 101, 219–225. [Google Scholar] [CrossRef]
- Padilla-Walker, L.M.; Carlo, G.; Nielson, M.G. Does helping keep teens protected? longitudinal bidirectional relations between prosocial behavior and problem behavior. Child Dev. 2015, 86, 1759–1772. [Google Scholar] [CrossRef]
- Zimmer-Gembeck, M.J.; Hunter, T.A.; Pronk, R. A model of behaviors, peer relations and depression: Perceived social acceptance as a mediator and the divergence of perceptions. J. Soc. Clin. Psychol. 2007, 26, 273–302. [Google Scholar] [CrossRef]
- Teng, X.H. The harmonious relationship of barley harvest patterns and interpersonal communication of Tibetan: A case study in Xiao Shagong village of Eluo town, Chamdo county, Tibet. J. Orig. Ecol. Natl. Cult. 2015, 7, 26–31. (In Chinese) [Google Scholar]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.L.; Faulkner, B.; Wekerle, C. The relationship among internal resilience, smoking, alcohol use, and depression symptoms in emerging adults transitioning out of child welfare. Child Abus. Negl. 2013, 37, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Tugade, M.M.; Fredrickson, B.L. Resilient individuals use positive emotions to bounce back from negative emotional experiences. J. Personal. Soc. Psychol. 2004, 86, 320–333. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L. The role of positive emotions in positive psychology. The broaden-and-build theory of positive emotions. Am. Psychol. 2001, 359, 1367–1377. [Google Scholar] [CrossRef]
- Smith, B.W.; Tooley, E.M.; Christopher, P.J.; Kay, V.S. Resilience as the ability to bounce back from stress: A neglected personal resource. J. Posit. Psychol. 2010, 5, 166–176. [Google Scholar] [CrossRef]
- Fletcher, D.; Sarkar, M. Psychological resilience. Eur. Psychol. 2013, 18, 12–23. [Google Scholar] [CrossRef]
- Fischer, A.S.; Camacho, M.C.; Ho, T.C.; Whitfield-Gabrieli, S.; Gotlib, I.H. Neural markers of resilience in adolescent females at familial risk for major depressive disorder. JAMA Psychiatry 2018, 75, 493–502. [Google Scholar] [CrossRef]
- Shapero, B.G.; Farabaugh, A.; Terechina, O.; DeCross, S.; Cheung, J.C.; Fava, M.; Holt, D.J. Understanding the effects of emotional reactivity on depression and suicidal thoughts and behaviors: Moderating effects of childhood adversity and resilience. J. Affect. Disord. 2019, 245, 419–427. [Google Scholar] [CrossRef]
- Tlapek, S.M.; Auslander, W.; Edmond, T.; Gerke, D.; Schrag, R.V.; Threlfall, J. The moderating role of resiliency on the negative effects of childhood abuse for adolescent girls involved in child welfare. Child. Youth Serv. Rev. 2016, 73, 437–444. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, X.; Du, J.Z.; Zheng, X. Relationship between social support and depression, loneliness of migrant children: Resilience as a moderator and mediator. Chin. J. Clin. Psychol. 2014, 22, 512–516. (In Chinese) [Google Scholar]
- Niu, G.F.; Sun, X.J.; Tian, Y.; Fan, C.Y.; Zhou, Z.K. Resilience moderates the relationship between ostracism and depression among Chinese adolescents. Personal. Individ. Differ. 2016, 99, 77–80. [Google Scholar] [CrossRef]
- Andresen, E.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for depression in well older adults: Evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar] [CrossRef]
- Tatar, A.; Kayiran, S.; Saltukoglu, G.; Ozkut, E.; Emeksiz, M. Analysis of the Center for Epidemiological StudiesDepression Scale (CES-D) in children and adolescents fromthe perspective of item response theory. Klin. Psikofarmakol. Bul. 2013, 23, 242–253. [Google Scholar] [CrossRef]
- Khan, A.; Ahmed, R.; Burton, N.W. Prevalence and correlates of depressive symptoms in secondary school children in Dhaka city, Bangladesh. Ethn. Health 2017, 25, 34–46. [Google Scholar] [CrossRef]
- Zhou, Y.; Liang, Y.; Cheng, J.; Zheng, H.; Liu, Z. Child Maltreatment in Western China: Demographic Differences and Associations with Mental Health. Int. J. Environ. Res. Public Health 2019, 16, 3619. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Stein, M.B. Psychometric analysis and refinement of the Connor-Davidson Resilience Scale (CD-RISC): Validation of a 10-item measure of resilience. J. Trauma. Stress 2007, 20, 1019–1028. [Google Scholar] [CrossRef]
- Yu, X.; Zhang, J. Factor analysis and psychometric evaluation of the Connor-Davidson Resilience Scale (CD-RISC) with Chinese people. Soc. Behav. Persnoal. 2007, 35, 19–30. [Google Scholar] [CrossRef]
- Goodman, R.; Meltzer, H.; Bailey, V. The strengths and difficulties questionnaire: A pilot study on the validity of the self-report version. Eur. Child Adolesc. Psychiatry 1998, 7, 125–130. [Google Scholar] [CrossRef]
- El-Khodary, B.; Samara, M. The mediating role of trait emotional intelligence, prosocial behaviour, parental support and parental psychological control on the relationship between war trauma, and PTSD and depression. J. Res. Persnoal. 2019, 81, 246–256. [Google Scholar] [CrossRef]
- Du, Y.; Kou, J.; Coghill, D. The validity, reliability and normative scores of the parent, teacher and self report versions of the Strengths and Difficulties Questionnaire in China. Child Adolesc. Psychiatry Ment. Health 2008, 2, 8–22. [Google Scholar] [CrossRef] [PubMed]
- Little, R.J. A test of missing completely at random for multivariate data with missing values. J. Am. Stat. Assoc. 1988, 83, 1198–1202. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Processanalysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Miller, G.A.; Chapman, J.P. Misunderstanding analysis of covariance. J. Abnorm. Psychol. 2001, 110, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Frazier, P.A.; Tix, A.P.; Barron, K.E. Testing moderator and mediator effects in counseling psychology research. J. Couns. Psychol. 2004, 51, 115–134. [Google Scholar] [CrossRef]
- Kious, B.M.; Kondo, D.G.; Renshaw, P.F. Living High and Feeling Low: Altitude, Suicide, and Depression. Harv. Rev. Psychiatry 2018, 26, 43–55. [Google Scholar] [CrossRef]
- Sheth, C.; Ombach, H.; Olson, P.; Renshaw, P.F.; Kanekar, S. Increased anxiety and anhedonia in female rats following exposure to altitude. High Alt. Med. Biol. 2018, 19, 81–90. [Google Scholar] [CrossRef]
- Bai, L.; Woodward, A.; Zhu, C.; Liu, Q. County-level heat vulnerability of urban and rural residents in Tibet, China. Environ. Health 2016, 15, 3–13. [Google Scholar] [CrossRef]
- Davis, A.N.; Carlo, G.; Schwartz, S.J.; Unger, J.B.; Zamboanga, B.L.; Lorenzo-Blanco, E.I.; Cano, M.Á.; Baezconde-Garbanati, L.; Oshri, A.; Streit, C.; et al. The longitudinal associations between discrimination, depressive symptoms, and prosocial behaviors in U.S. Latino/a recent immigrant adolescents. J. Youth Adolesc. 2016, 45, 457–470. [Google Scholar] [CrossRef]
- Carlo, G. The development and correlates of prosocial moral behaviors. In Handbook of Moral Development; Killen, M., Smetana, J.G., Eds.; Psychology Press: New York, NY, USA, 2014. [Google Scholar]
- Betancourt, T.S.; Brennan, R.T.; Rubin-Smith, J.; Fitzmaurice, G.M.; Gilman, S.E. Sierra Leone’s former child soldiers: A longitudinal study of risk, protective factors, and mental health. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 606–615. [Google Scholar] [CrossRef]
- Schulz, A.; Becker, M.; Van der Auwera, S.; Barnow, S.; Appel, K.; Mahler, J.; Schmidt, C.O.; John, U.; Freyberger, H.J.; Grabe, H.J. The impact of childhood trauma on depression: Does resilience matter? population-based results from the study of health in Pomerania. J. Psychosom. Res. 2014, 77, 97–103. [Google Scholar] [CrossRef]
- Liu, J.J.W.; Reed, M.; Girard, T.A. Advancing resilience: An integrative, multi-system model of resilience. Personal Individ. Differ. 2017, 111, 111–118. [Google Scholar] [CrossRef]
- Donaldson, D.; Prinstein, M.J.; Danovsky, M.; Spirito, A. Patterns of Children’s Coping with Life Stress: Implications for Clinicians. Am. J. Orthopsychiatry 2000, 70, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Mandleco, B.L.; Peery, J.C. An organizational framework for conceptualizing resilience in children. J. Child Adolesc. Psychiatry Nurs. 2000, 13, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, N.; Cumberland, A.; Guthrie, I.K.; Murphy, B.C.; Shepard, S.A. Age changes in prosocial responding and moral reasoning in adolescence and early adulthood. J. Res. Adolesc. 2005, 15, 235–260. [Google Scholar] [CrossRef]
- Fabes, R.A.; Carlo, G.; Kupanoff, K.; Laible, D. Early adolescence and prosocial/moral behavior I: The role of individual processes. J. Early Adolesc. 1999, 19, 5–16. [Google Scholar] [CrossRef]
- Carlo, G.; Crockett, L.J.; Randall, B.A.; Roesch, S.C. A latent growth curve analysis of prosocial behavior among rural adolescents. J. Res. Adolesc. 2007, 17, 301–324. [Google Scholar] [CrossRef]
- Flynn, E.; Ehrenreich, S.E.; Beron, K.J.; Underwood, M.K. Prosocial behavior: Long-term trajectories and psychosocial outcomes. Soc. Dev. 2015, 24, 462–482. [Google Scholar] [CrossRef]
- Qu, Y.; Pomerantz, E.M.; Deng, C. Mothers’ goals for adolescents in the United States and China: Content and transmission. J. Res. Adolesc. 2016, 26, 126–141. [Google Scholar] [CrossRef]
- Kanacri, B.P.L.; Pastorelli, C.; Eisenberg, N.; Antonio, Z.; Caprara, G.V. The development of prosociality from adolescence to early adulthood: The role of effortful control. J. Personal 2013, 81, 302–312. [Google Scholar] [CrossRef]
- Hartling, L.M. Strengthening resilience in a risky world: It’s all about relationships. Women Ther. 2008, 31, 51–70. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sociodemographic Characteristics | Category | Frequency | % |
|---|---|---|---|
| Gender | Boys | 5419 | 48.6 |
| Girls | 5741 | 51.4 | |
| Age (years) | 10–11 | 702 | 6.3 |
| 12–13 | 2780 | 24.9 | |
| 14–15 | 4423 | 39.7 | |
| 16–17 | 3255 | 29.1 | |
| a Education level of the fathers | Never went to school | 8405 | 75.3 |
| Primary school | 1131 | 10.1 | |
| Junior high school | 887 | 7.9 | |
| High school or above | 602 | 5.4 | |
| a Education level of the mothers | Never went to school | 7758 | 69.5 |
| Primary school | 998 | 8.9 | |
| Junior high school | 777 | 7.0 | |
| High school or above | 494 | 4.4 |
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1. Depression | — | −0.45 *** | −0.40 *** | −0.08 *** | 0.02 | 0.17 *** | 0.17 *** |
| 2. Resilience | — | 0.62 *** | 0.15 *** | 0.02 | −0.25 *** | −0.22 *** | |
| 3. Prosocial behavior | — | 0.09 *** | 0.01 | −0.16 *** | −0.13 *** | ||
| 4. Age | — | −0.01 | −0.15 *** | −0.17 *** | |||
| 5. Gender | — | −0.01 | −0.01 | ||||
| 6. Education level of the fathers | — | 0.88 *** | |||||
| 7. Education level of the mothers | — | ||||||
| M | 7.51 | 38.29 | 12.70 | 14.34 | |||
| SD | 5.74 | 9.81 | 2.18 | 1.77 |
| Variables | β | SE | t | 95% (CI) |
|---|---|---|---|---|
| Prosocial behavior | −0.25 | 0.01 | −21.90 *** | (−0.27, −0.23) |
| Resilience | −0.31 | 0.01 | −28.60 *** | (−0.33, −0.29) |
| Prosocial behavior × Resilience | −0.08 | 0.01 | −9.89 *** | (−0.10, −0.07) |
| Levels of resilience | ||||
| Low (Z = −1.0) | −0.17 | 0.01 | −14.84 *** | (−0.19, −0.14) |
| High (Z = 1.0) | −0.33 | 0.02 | −20.05 *** | (−0.37, −0.30) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eli, B.; Zhou, Y.; Liang, Y.; Cheng, J.; Wang, J.; Huang, C.; Xuan, X.; Liu, Z. Depression in Children and Adolescents on the Qinghai-Tibet Plateau: Associations with Resilience and Prosocial Behavior. Int. J. Environ. Res. Public Health 2021, 18, 440. https://doi.org/10.3390/ijerph18020440
Eli B, Zhou Y, Liang Y, Cheng J, Wang J, Huang C, Xuan X, Liu Z. Depression in Children and Adolescents on the Qinghai-Tibet Plateau: Associations with Resilience and Prosocial Behavior. International Journal of Environmental Research and Public Health. 2021; 18(2):440. https://doi.org/10.3390/ijerph18020440
Chicago/Turabian StyleEli, Buzohre, Yueyue Zhou, Yiming Liang, Jin Cheng, Jiazhou Wang, Changbing Huang, Xi Xuan, and Zhengkui Liu. 2021. "Depression in Children and Adolescents on the Qinghai-Tibet Plateau: Associations with Resilience and Prosocial Behavior" International Journal of Environmental Research and Public Health 18, no. 2: 440. https://doi.org/10.3390/ijerph18020440
APA StyleEli, B., Zhou, Y., Liang, Y., Cheng, J., Wang, J., Huang, C., Xuan, X., & Liu, Z. (2021). Depression in Children and Adolescents on the Qinghai-Tibet Plateau: Associations with Resilience and Prosocial Behavior. International Journal of Environmental Research and Public Health, 18(2), 440. https://doi.org/10.3390/ijerph18020440