
Interest of a Joint Use of Two Diagnostic Tools of Burnout: Comparison between the Oldenburg Burnout Inventory and the Early Detection Tool of Burnout Completed by Physicians


Abstract
:1. Introduction
1.1. Definitions
1.2. Diagnostic Tools of Burnout
1.3. Evaluation of the Proportion of Healthy People and People Affected
1.4. The Comparison and the Joint Use of Diagnostic Tools
2. Materials and Methods
2.1. Objective
2.2. Procedure
2.3. Participants
2.4. Measures
2.4.1. Oldenburg Burnout Inventory (OLBI)
2.4.2. Early Detection Tool of Burnout (EDTB)
2.5. Analyses
3. Results
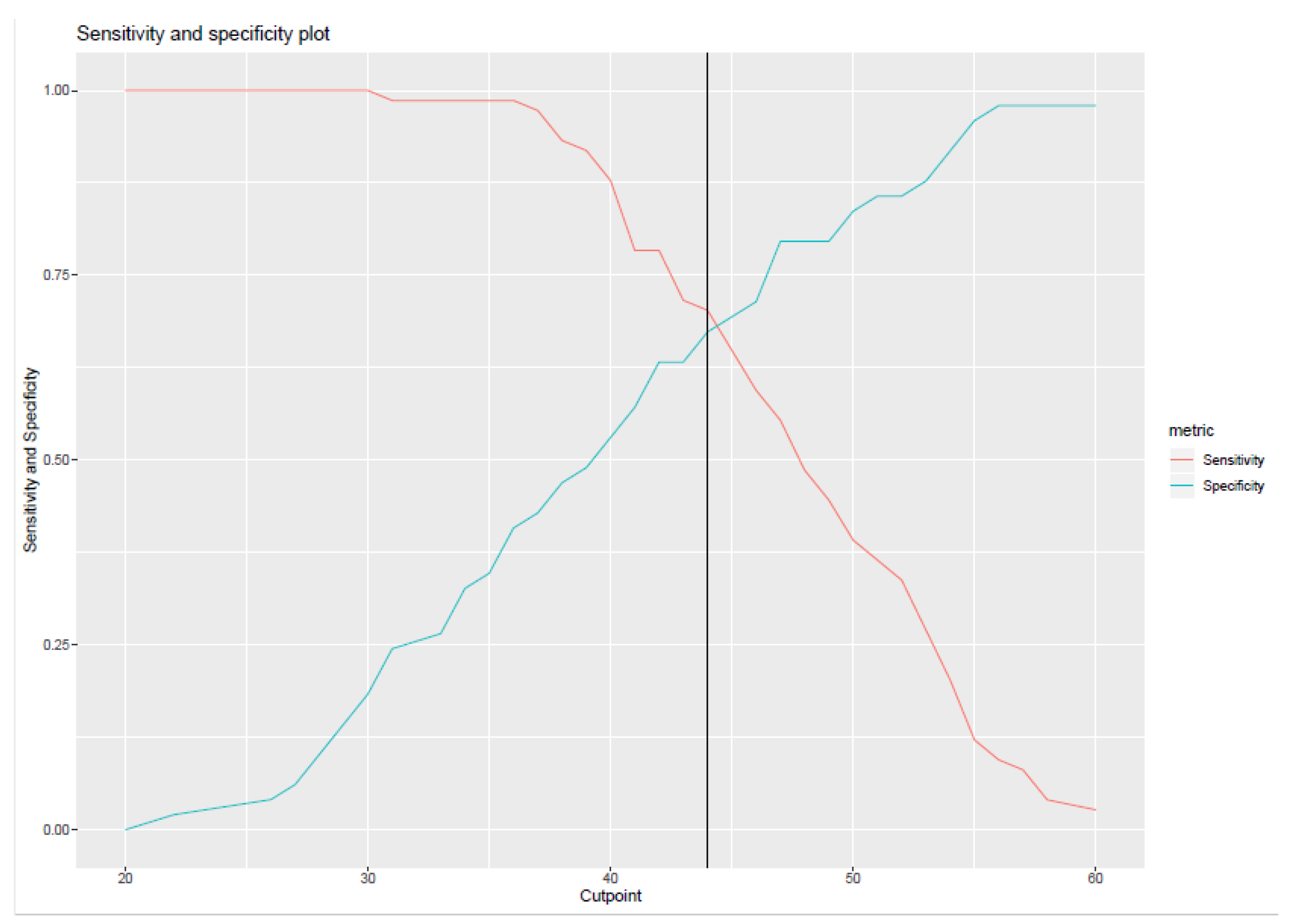
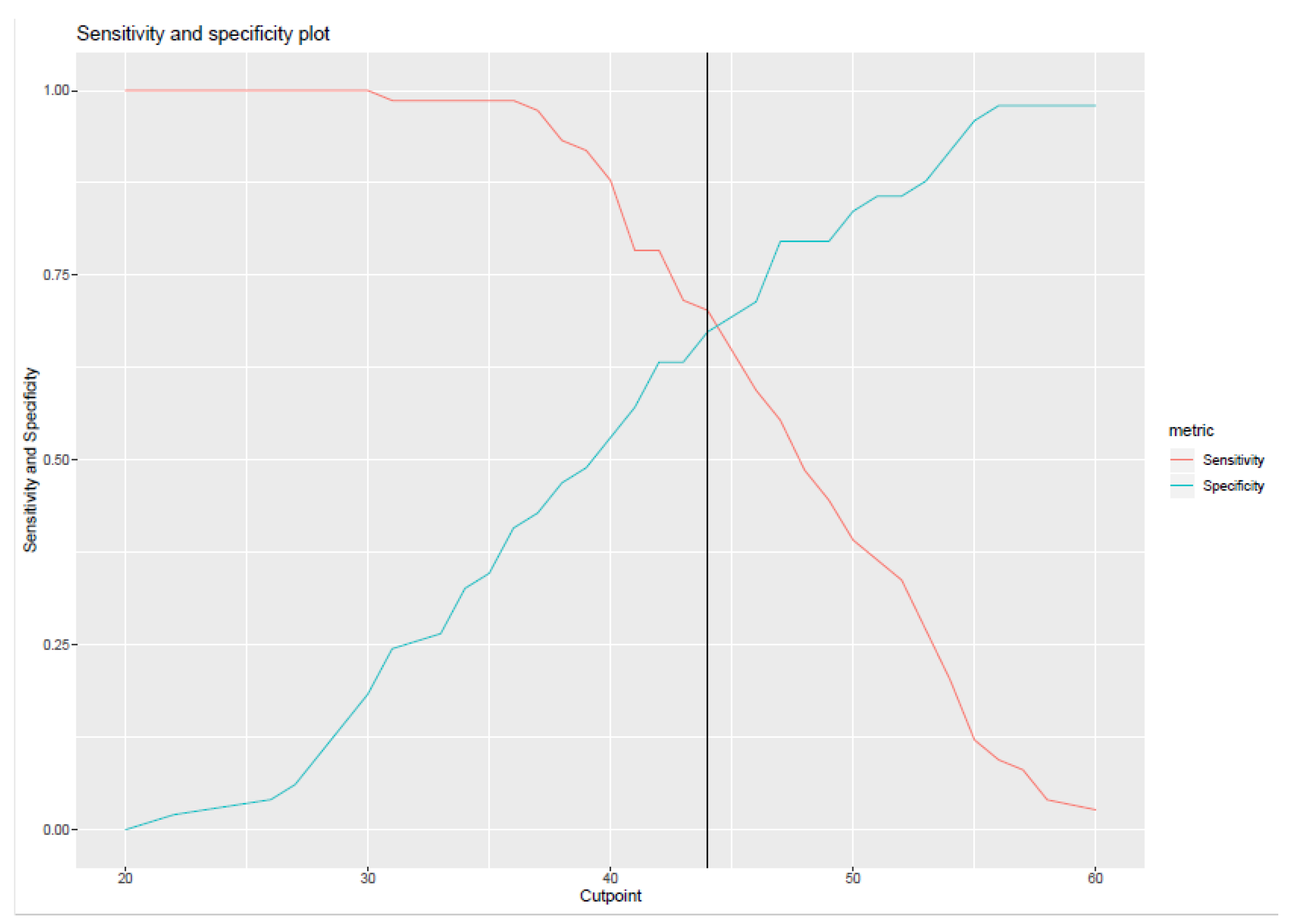
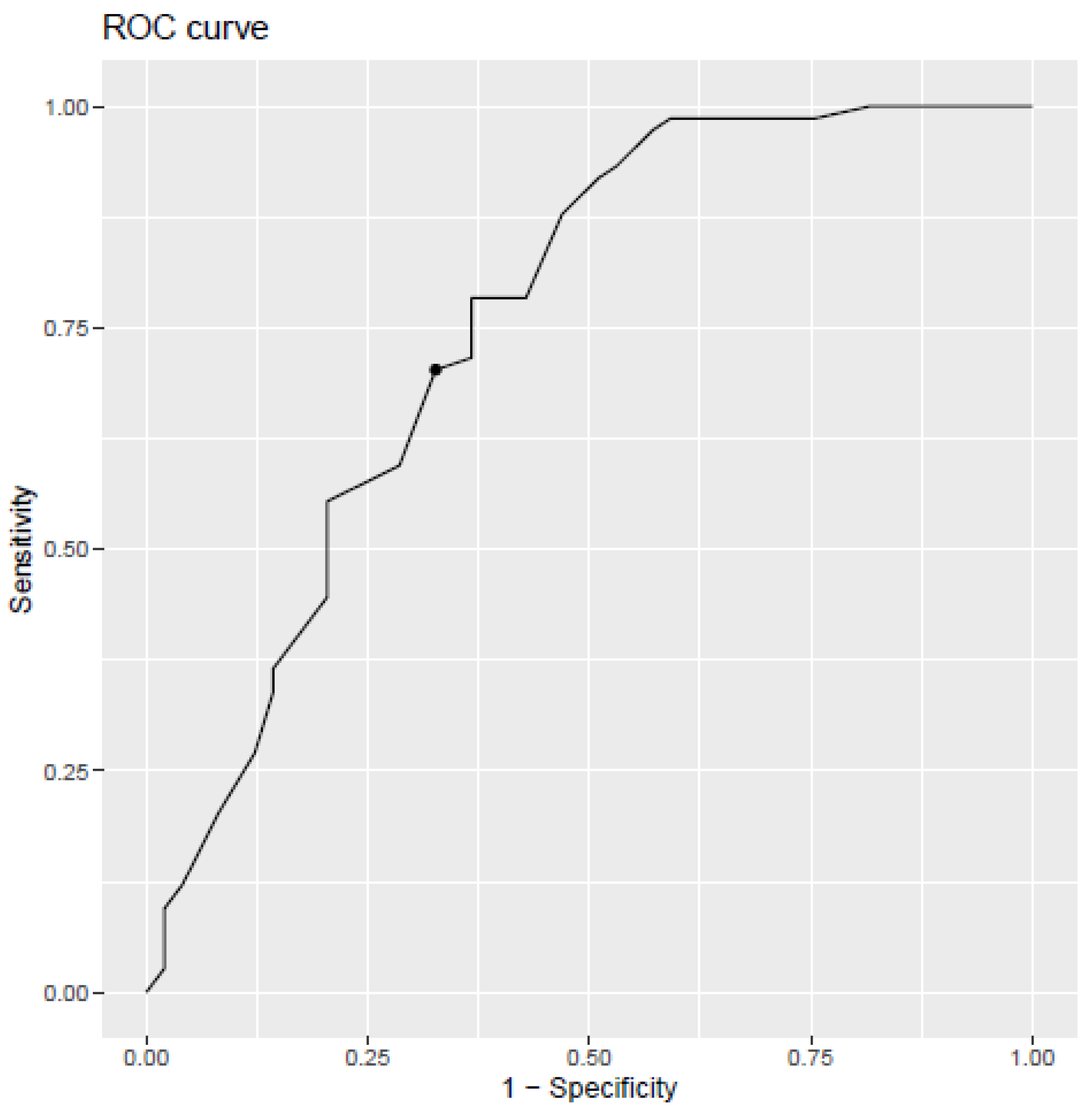
3.1. Cut-Off Score for the OLBI
3.2. Comparison between the OLBI and the EDTB
3.3. Comparison of the Clinical Judgement Made by General Practitioners (GPS) and Occupational Physicians (Ops) with the OLBI
4. Discussion
Limitations, Recommendations for Future Research, and Practical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- FPS Employment, Labour and Social Dialogue. Maladies Professionnelles. Available online: https://www.beswic.be/fr/themes/information-pour-les-medecins-traitants/maladies-professionnelles (accessed on 20 September 2021).
- National Institute for Health and Disability Insurance. Incapacité de Travail de Longue Durée: Combien de Burnouts et de Dépressions de Longue Durée? Quel Coût Pour L’assurance Indemnités? Available online: https://www.riziv.fgov.be/fr/statistiques/indemnites/Pages/incapacite-travail-longue-duree-combien-burn-outs-depressions.aspx#Une_augmentation_de_39,23_%_de_burnouts_et_de_d%C3%A9pressionde_longue_dur%C3%A9e_en_4_ans (accessed on 20 July 2021).
- Heureux, P. Le burnout à la consultation du médecin généraliste. Rev. Sect. Sci. St. De L’ucl 2018, 137, 535–539. [Google Scholar]
- Guseva Canu, I.; Mesot, O.; Györkös, C.; Mediouni, Z. Burnout Syndrome in Europe: Towards a Harmonized Approach in Occupational Health Practice and Research. Ind. Health 2019, 57, 745–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Burn-Out An “Occupational Phenomenon”: International Classification of Diseases. Available online: https://www.who.int/news/item/28-05-2019-burn-out-an-occupational-phenomenon-international-classification-of-diseases (accessed on 27 July 2021).
- Bravo, D.M.; Suárez-Falcón, J.C.; Bianchi, J.M.; Segura-Vargas, M.A.; Ruiz, F.J. Psychometric Properties and Measurement Invariance of the Maslach Burnout Inventory–General Survey in Colombia. Int. J. Environ. Res. Public Health 2021, 18, 5118. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Desart, S.; De Witte, H. Burnout Assessment Tool (BAT)—development, validity, and reliability. Int. J. Environ. Res. Public Health 2020, 17, 9495. [Google Scholar] [CrossRef]
- Guseva Canu, I.; Marca, S.; Dell’Oro, F.; Balázs, Á.; Bergamaschi, E.; Besse, C.; Bianchi, R.; Bislimovska, J.; Koscec Bjelajac, A.; Bugge, M.; et al. Harmonized Definition of Occupational Burnout: A Systematic Review, Semantic Analysis, And Delphi Consensus In 29 Countries. Scand. J. Work. Environ. Health 2020, 47, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Hansez, I.; Firket, P.; Leclercq, C. Stades du Burnout et le Type de Prévention Approprié Selon le Stade. Presented at the “Burnout: Les Clefs Pour Agir”, Bruxelles, Belgium, 12 December 2019. Available online: https://www.health.belgium.be/fr/stades-du-burnout-et-le-type-de-prevention-approprie-selon-le-stade (accessed on 17 September 2020).
- Demerouti, E.; Bakker, A.B.; Vardakou, I.; Kantas, A. The convergent validity of two burnout instruments: A multitrait-multimethod analysis. Eur. J. Psychol. Assess. 2003, 19, 12. [Google Scholar] [CrossRef]
- Guidetti, G.; Viotti, S.; Gil-Monte, P.; Converso, D. Feeling Guilty or Not Guilty. Identifying Burnout Profiles Among Italian Teachers. Curr. Psychol. 2018, 37, 769–780. [Google Scholar] [CrossRef]
- Shoman, Y.; Marca, S.C.; Bianchi, R.; Godderis, L.; van der Molen, H.F.; Guseva-Canu, I. Psychometric properties of burnout measures: A systematic review. Epidemiol. Psychiatr. Sci. 2021, 30, e8. [Google Scholar] [CrossRef]
- Abeltina, M.; Stokenberga, I.; Skudra, J.; Rascevska, M.; Kolesovs, A. Burnout Clinical Subtypes Questionnaire (BCSQ-36): Reliability and validity study in Latvia. Psychol. Health Med. 2020, 25, 1–12. [Google Scholar] [CrossRef]
- Schilling, R.; Colledge, F.; Brand, S.; Ludyga, S.; Gerber, M. Psychometric properties and convergent validity of the Shirom–Melamed burnout measure in two German-speaking samples of adult workers and police officers. Front. Psychiatry 2019, 10, 536. [Google Scholar] [CrossRef] [Green Version]
- Schaufeli, W.B.; De Witte, H.; Desart, S. Handleiding Burnout Assessment BPSEWS Tool (BAT); KU Leuven: Leuven, Belgium, 2020; Available online: https://burnoutassessmenttool.be/wp-content/uploads/2020/08/Handleiding-BAT-versie-2.0.pdf (accessed on 19 November 2020).
- Schaufeli, W.B.; De Witte, H.; Desart, S. Manual of Burnout Assessment Tool (BAT); KU Leuven: Leuven, Belgium, 2019. [Google Scholar]
- Sakakibara, K.; Shimazu, A.; Toyama, H.; Schaufeli, W.B. Validation of the Japanese Version of the Burnout Assessment Tool. Front. Psychol. 2020, 11, 1819. [Google Scholar] [CrossRef] [PubMed]
- Consiglio, C.; Mazzetti, G.; Schaufeli, W.B. Psychometric Properties of the Italian Version of the Burnout Assessment Tool (BAT). Int. J. Environ. Res. Public Health 2021, 18, 9469. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.B.; van Dierendonk, D. Utrechtse Burnout Schaal (UBOS) Handleiding (Utrecht Burnout Scale Manual); Swets & Zeitlinger: Utrecht, The Netherlands, 2000. [Google Scholar]
- Rotenstein, L.; Torre, M.; Ramos, M.; Rosales, R.; Guille, C.; Sen, S.; Mata, D. Prevalence of Burnout Among Physicians. J. Am. Med Assoc. 2018, 320, 1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, H.; Schaufeli, W. The Convergent Validity of Four Burnout Measures in A Chinese Sample: A Confirmatory Factor-Analytic Approach. Appl. Psychol. 2010, 60, 87–111. [Google Scholar] [CrossRef] [Green Version]
- Sinval, J.; Queirós, C.; Pasian, S.; Marôco, J. Transcultural Adaptation of the Oldenburg Burnout Inventory (OLBI) for Brazil and Portugal. Front. Psychol. 2019, 10, 338. [Google Scholar] [CrossRef] [PubMed]
- Grove, W.; Zald, D.; Lebow, B.; Snitz, B.; Nelson, C. Clinical Versus Mechanical Prediction: A Meta-Analysis. Psychol. Assess. 2000, 12, 19–30. [Google Scholar] [CrossRef]
- Bell, I.; Mellor, D. Clinical Judgements: Research and Practice. Aust. Psychol. 2009, 44, 112–121. [Google Scholar] [CrossRef] [Green Version]
- Hansez, I.; Mairiaux, P.; Firket, P.; Braeckman, L. Recherche Sur le Burnout au Sein de La Population Active Belge: Rapport Final [Research on Burnout in the Active Belgian Population: Final Report]; FPS Employment, Labour and Social Dialogue: Bruxelles, Belgium, 2010; Available online: https://emploi.belgique.be/sites/default/files/content/documents/Bien-%C3%AAtre%20au%20travail/Projets%20de%20recherche/rapport_final_burnout.pdf (accessed on 12 November 2020).
- Hansez, I.; Rusu, D.; Firket, P.; Braeckman, L. Evolution 2010–2018 du Burnout en Belgique et Intérêt de L’utilisation Conjointe de Deux Outils de Diagnostic; FPS Employment, Labour and Social Dialogue: Bruxelles, Belgium, 2019; Available online: https://emploi.belgique.be/sites/default/files/content/documents/Bien-%C3%AAtre%20au%20travail/Projets%20de%20recherche/burnout2019_samenvatting_van_het_onderzoek_FR.pdf (accessed on 12 November 2020).
- FPS Employment, Labour and Social Dialogue. Détection Précoce du Burnout: Outil Pour le Médecin Généraliste Burnout. Available online: https://emploi.belgique.be/fr/publications/detection-precoce-du-burnout-outil-pour-le-medecin-generaliste (accessed on 13 November 2020).
- Nahavandi, K.H. Calculating Sensitivity, Specificity and Predictive Values for Medical Diagnostic Tests. Gene Cell Tissue 2018, 5, e80270. [Google Scholar] [CrossRef]
- Hajian-Tilaki, K. The choice of methods in determining the optimal cut-off value for quantitative diagnostic test evaluation. Stat. Methods Med. Res. 2018, 27, 2374–2383. [Google Scholar] [CrossRef]
- Trevethan, R. Sensitivity, Specificity, And Predictive Values: Foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public Health 2017, 5, 307–313. [Google Scholar] [CrossRef]
- Ægisdóttir, S.; White, M.; Spengler, P.; Maugherman, A.; Anderson, L.; Cook, R.; Nichols, C.; Lampropoulos, G.; Walker, B.; Cohen, G.; et al. The Meta-Analysis of Clinical Judgment Project: Fifty-Six Years of Accumulated Research on Clinical Versus Statistical Prediction. Couns. Psychol. 2006, 34, 341–382. [Google Scholar] [CrossRef]
- van Vugt, E.; Asscher, J.; Hendriks, J.; Stams, G.; Bijleveld, C.; van der Laan, P. Assessment of Moral Judgment and Empathy in Young Sex Offenders. Int. J. Offender Ther. Comp. Criminol. 2011, 56, 986–996. [Google Scholar] [CrossRef] [Green Version]
- Kirkhus, L.; Šaltytė Benth, J.; Rostoft, S.; Grønberg, B.; Hjermstad, M.; Selbæk, G.; Wyller, T.; Harneshaug, M.; Jordhøy, M. Geriatric Assessment Is Superior to Oncologists’ Clinical Judgement in Identifying Frailty. Br. J. Cancer 2017, 117, 470–477. [Google Scholar] [CrossRef]
- Barroso, N.; Alcântara, P.; Botelho, A.; Douglas-de-Oliveira, D.; Gonçalves, P.; Flecha, O. Prevalence of Self-Reported Versus Diagnosed Dentinal Hypersensitivity: A Cross-Sectional Study and ROC Curve Analysis. Acta Odontol. Scand. 2019, 77, 219–223. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; Hoogduin, K.; Schaap, C.; Kladler, A. On the clinical validity of the Maslach Burnout Inventory and the Burnout Measure. Psychol. Health 2001, 16, 565–582. [Google Scholar] [CrossRef]
- Kleijweg, J.; Verbraak, M.; Van Dijk, M. The Clinical Utility of The Maslach Burnout Inventory in A Clinical Population. Psychol. Assess. 2013, 25, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Wickramasinghe, N.; Dissanayake, D.; Abeywardena, G. Clinical Validity and Diagnostic Accuracy Of The Maslach Burnout Inventory-Student Survey In Sri Lanka. Health Qual. Life Outcomes 2018, 16, 220. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Reed, G.; Roberts, M.; Esparza, P.; Watts, A.; Correia, J.; Ritchie, P.; Maj, M.; Saxena, S. Psychologists’ Perspectives on The Diagnostic Classification of Mental Disorders: Results from the WHO-Iupsys Global Survey. Int. J. Psychol. 2013, 48, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Bakker, A.B.; Demerouti, E. Job demands–resources theory: Taking stock and looking forward. J. Occup. Health Psy-Chology 2017, 22, 273. [Google Scholar] [CrossRef]
- Hansez, I.; Laurent, J. Création de Normes Pour la Version Francophone de L’outil « OLBI ». Unpublished work. 2018. [Google Scholar]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: http://www.R-project.org (accessed on 14 September 2021).
- Yang, S.; Berdine, G. The receiver operating characteristic (ROC) curve. Southwest Respir. Crit. Care Chron. 2017, 5, 34–36. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics 1977, 33, 363–374. [Google Scholar] [CrossRef]
- Power, M.; Fell, G.; Wright, M. Principles for High-Quality, High-Value Testing. Evid. Based Med. 2012, 18, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Mbanga, C.; Makebe, H.; Tim, D.; Fonkou, S.; Toukam, L.; Njim, T. Determinants of burnout syndrome among nurses in Cameroon. BMC Res. Notes 2018, 11, 893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen Huynh, A.; Besse, C.; Mediouni, Z.; El May, E.; Shoman, Y.; Hansez, I.; Guseva Canu, I. Diagnostic Performances of an Occupational Burnout Detection Method Designed for Healthcare Professionals. Submitted for Publication. Int. J. Environ. Res. Public Health 2021. (Under Review). [Google Scholar]
- Nguyen Huynh, A.; Béguelin, A.; Krief, P.; Marion-Veyron, R.; Mediouni, Z.; Regamey, F.; Staeger, P.; Guseva Canu, I. Repérage et prise en charge des patients en burnout par les médecins d’Unisanté [Detection and treatment of burnout by physicians of Unisanté]. Rev. Med. Suisse 2021, 17, 221–224. [Google Scholar] [PubMed]
- Salvagioni, D.; Melanda, F.; Mesas, A.; González, A.; Gabani, F.; Andrade, S. Physical, Psychological and Occupational Consequences Of Job Burnout: A Systematic Review Of Prospective Studies. PLoS ONE 2017, 12, e0185781. [Google Scholar] [CrossRef]
- Fedris. Projet Pilote Burn-Out. Available online: https://fedris.be/fr/node/2540 (accessed on 27 November 2020).
- García-Arroyo, J.; Osca Segovia, A. Effect sizes and cut-off points: A meta-analytical review of burnout in Latin American countries. Psychol. Health Med. 2018, 23, 1079–1093. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| References | Population | Reference Method | Tested Method | Test Validity of the Tested Method | |
|---|---|---|---|---|---|
| Sensitivity | Specificity | ||||
| Schaufeli et al. [35] | Netherlands workers | Clinical judgement using the ICD-10 diagnostic guidelines | MBI | 0.70 | 0.57 |
| BM | 0.60 | 0.71 | |||
| Kleijweg et al. [36] | Netherlands workers | Semi-structured interview with the mini international neuropsychiatric interview | MBI | 0.78 | 0.48 |
| Wickramasinghe et al. [37] | Sri Lankan students | Clinical judgement made by a consultant psychiatrist | MBI-SS | 0.92 | 0.93 |
| Age, mean, years (SEM *) | 44.47 (+/− 10.13) | Job tenure, mean, years (SEM) | 15.53 (+/− 10.93) |
| Genre, N | Contract, N | ||
| Men | 62 (50.40%) | Fixed-term contracts | 85 (69.10%) |
| Women | 61 (49.60%) | Open-ended contracts | 28 (22.76%) |
| Relationship status, N | Interim contracts | 7 (5.70%) | |
| Couple | 88 (71.55%) | “Did not state” | 3 (2.44%) |
| Single | 25 (20.32%) | Employment status, N | |
| “Did not state” | 10 (8.13%) | Employees | 79 (64.23%) |
| Language, N | Blue-collar workers | 28 (22.76%) | |
| French | 62 (50.40%) | Managers | 12 (9.76%) |
| Dutch | 61 (49.60%) | Self-employed | 1 (0.81%) |
| Sector, N | “Did not state” | 3 (2.44%) | |
| Private | 97 (78.86%) | Working time, N | |
| Public | 25 (20.33%) | Full-time | 40 (32.52%) |
| “Did not state” | 1 (0.81%) | Part-time | 3 (2.44%) |
| Organization size, N | “Did not state” | 80 (65.04%) | |
| <20 | 13 (10.57%) | Work disability, N | |
| 20–49 | 3 (2.44%) | Yes | 58 (47.15%) |
| 50–250 | 18 (14.64%) | No | 65 (52.85%) |
| >250 | 81 (65.85%) | ||
| “Did not state” | 8 (6.50%) |
| Method Tested | |||
|---|---|---|---|
| Positive OLBI | Negative OLBI | ||
| Reference method | Positive clinical judgement/EDTB | True Positive (TP) | False Negative (FN) |
| Negative clinical judgement/EDTB | False Positive (FP) | True Negative (TN) | |
| Reference Method | |||
|---|---|---|---|
| Positive OLBI | Negative OLBI | ||
| Method tested | Positive clinical judgement/EDTB | True Positive (TP) | False Positive (FP) |
| Negative clinical judgement/EDTB | False Negative (FN) | True Negative (TN) | |
| Positive OLBI | Negative OLBI | ||
|---|---|---|---|
| Positive clinical judgement/EDTB | Gr1 52 (42.27%) | Gr3 22 (17.89%) | 74 |
| Negative clinical judgement/EDTB | Gr2 16 (13.01%) | Gr4 33 (26.83%) | 49 |
| 68 | 55 | 123 |
| Test Validity Indicators | Tested Methods | |
|---|---|---|
| EDTB | OLBI | |
| Sensitivity | 0.76 * | 0.70 * |
| Specificity | 0.60 | 0.67 |
| Positive predictive value | 0.70 | 0.76 |
| Negative predictive value | 0.67 | 0.60 |
| Accuracy | 0.69 | 0.69 |
| Positive OLBI | Negative OLBI | ||
|---|---|---|---|
| Positive clinical judgement/EDTB | 39 (39%) | 15 (15%) | 54 |
| Negative clinical judgement/EDTB | 14 (14%) | 32 (32%) | 46 |
| 53 | 47 | 100 |
| Positive OLBI | Negative OLBI | ||
|---|---|---|---|
| Positive clinical judgement/EDTB | 14 (60.86%) | 6 (26.08%) | 20 |
| Negative clinical judgement/EDTB | 2 (0.08%) | 1 (0.04%) | 3 |
| 16 | 7 | 23 |
| All Physicians | Occ. Phys. (OPs) | Gen. Pract. (GPs) | ||||
|---|---|---|---|---|---|---|
| Method Tested | EDTB | OLBI | EDTB | OLBI | EDTB | OLBI |
| Sensitivity | 0.76 * | 0.70 * | 0.74 * | 0.72 * | 0.87 * | 0.70 * |
| Specificity | 0.60 | 0.67 | 0.68 * | 0.70 * | 0.14 | 0.33 |
| Positive predictive value | 0.70 | 0.76 | 0.72 | 0.74 | 0.70 | 0.87 |
| Negative predictive value | 0.67 | 0.60 | 0.70 | 0.68 | 0.33 | 0.14 |
| Accuracy | 0.69 | 0.69 | 0.71 | 0.71 | 0.65 | 0.65 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leclercq, C.; Braeckman, L.; Firket, P.; Babic, A.; Hansez, I. Interest of a Joint Use of Two Diagnostic Tools of Burnout: Comparison between the Oldenburg Burnout Inventory and the Early Detection Tool of Burnout Completed by Physicians. Int. J. Environ. Res. Public Health 2021, 18, 10544. https://doi.org/10.3390/ijerph181910544
Leclercq C, Braeckman L, Firket P, Babic A, Hansez I. Interest of a Joint Use of Two Diagnostic Tools of Burnout: Comparison between the Oldenburg Burnout Inventory and the Early Detection Tool of Burnout Completed by Physicians. International Journal of Environmental Research and Public Health. 2021; 18(19):10544. https://doi.org/10.3390/ijerph181910544
Chicago/Turabian StyleLeclercq, Céline, Lutgart Braeckman, Pierre Firket, Audrey Babic, and Isabelle Hansez. 2021. "Interest of a Joint Use of Two Diagnostic Tools of Burnout: Comparison between the Oldenburg Burnout Inventory and the Early Detection Tool of Burnout Completed by Physicians" International Journal of Environmental Research and Public Health 18, no. 19: 10544. https://doi.org/10.3390/ijerph181910544
APA StyleLeclercq, C., Braeckman, L., Firket, P., Babic, A., & Hansez, I. (2021). Interest of a Joint Use of Two Diagnostic Tools of Burnout: Comparison between the Oldenburg Burnout Inventory and the Early Detection Tool of Burnout Completed by Physicians. International Journal of Environmental Research and Public Health, 18(19), 10544. https://doi.org/10.3390/ijerph181910544