
Association between Self-Perceived Social Support in the Workplace and the Presence of Depressive/Anxiety Symptoms

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Data
2.2. Main Variables
2.3. Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Milaneschi, Y.; Simmons, W.K.; van Rossum, E.F.C.; Penninx, B.W. Depression and obesity: Evidence of shared biological mechanisms. Mol. Psychiatry 2019, 24, 18–33. [Google Scholar] [CrossRef]
- Yu, M.; Zhang, X.; Lu, F.; Fang, L. Depression and risk for diabetes: A meta-analysis. Can. J. Diabetes 2015, 39, 266–272. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Ma, L. Depression and cardiovascular disease in elderly: Current understanding. J. Clin. Neurosci. 2018, 47, 1–5. [Google Scholar] [CrossRef]
- Fattouh, N.; Hallit, S.; Salameh, P.; Choueiry, G.; Kazour, F.; Hallit, R. Prevalence and factors affecting the level of depression, anxiety, and stress in hospitalized patients with a chronic disease. Perspect. Psychiatr. Care 2019, 55, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Yaribeygi, H.; Panahi, Y.; Sahraei, H.; Johnston, T.P.; Sahebkar, A. The impact of stress on body function: A review. EXCLI J. 2017, 16, 1057–1072. [Google Scholar]
- Greenberg, P.E.; Fournier, A.A.; Sisitsky, T.; Simes, M.; Berman, R.; Koenigsberg, S.H.; Kessler, R.C. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics 2021, 39, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, M.D.; Lage, M.J.; Dunayevich, E.; Russell, J.M.; Bowman, L.; Landbloom, R.P.; Levine, L.R. The cost of treating anxiety: The medical and demographic correlates that impact total medical costs. Depress. Anxiety 2005, 21, 178–184. [Google Scholar] [CrossRef]
- Chang, S.M.; Hong, J.P.; Cho, M.J. Economic burden of depression in south korea. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 683–689. [Google Scholar] [CrossRef]
- Park, K.O.; Wilson, M.G.; Lee, M.S. Effects of social support at work on depression and organizational productivity. Am. J. Health Behav. 2004, 28, 444–455. [Google Scholar] [CrossRef]
- Kim, K.W.; Park, S.J.; Lim, H.S.; Cho, H.H. Safety climate and occupational stress according to occupational accidents experience and employment type in shipbuilding industry of korea. Saf. Health Work 2017, 8, 290–295. [Google Scholar] [CrossRef]
- Zomer, E.; Rhee, Y.; Liew, D.; Ademi, Z. The health and productivity burden of depression in south korea. Appl. Health Econ. Health Policy 2021. [Google Scholar] [CrossRef] [PubMed]
- Stress, I.W. A Collective Challenge; International Labour Organisation: Geneva, Switzerland, 2016. [Google Scholar]
- Harandi, T.F.; Taghinasab, M.M.; Nayeri, T.D. The correlation of social support with mental health: A meta-analysis. Electron. Physician 2017, 9, 5212–5222. [Google Scholar] [CrossRef] [Green Version]
- Weigl, M.; Stab, N.; Herms, I.; Angerer, P.; Hacker, W.; Glaser, J. The associations of supervisor support and work overload with burnout and depression: A cross-sectional study in two nursing settings. J. Adv. Nurs. 2016, 72, 1774–1788. [Google Scholar] [CrossRef]
- Hwang, J.H.; Choi, S.; Park, H. Effects of job stress and supervisory support on depression of care givers in elderly care facilities. Korean J. Occup. Health Nurs. 2015, 24, 352–362. [Google Scholar] [CrossRef] [Green Version]
- Park, C.J.; Yook, J.H.; Kim, M.S.; Lee, D.; Lim, H.M.; Hong, Y.C. The association between quality of direct supervisor’s behavior and depressive mood in korean wage workers: The 4th korean working conditions survey. Ann. Occup. Environ. Med. 2019, 31, e16. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Kim, Y. Association of co-exposure to psychosocial factors with depression and anxiety in korean workers. J. Occup. Environ. Med. 2020, 62, e498–e507. [Google Scholar] [CrossRef] [PubMed]
- Hämmig, O. Health and well-being at work: The key role of supervisor support. SSM Popul. Health 2017, 3, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Baeriswyl, S.; Krause, A.; Elfering, A.; Berset, M. How workload and coworker support relate to emotional exhaustion: The mediating role of sickness presenteeism. Int. J. Stress Manag. 2017, 24, 52. [Google Scholar] [CrossRef]
- Age, O. Working Better with Age; OECD: Paris, France, 2019. [Google Scholar]
- Wege, N.; Li, J.; Siegrist, J. Are there gender differences in associations of effort-reward imbalance at work with self-reported doctor-diagnosed depression? Prospective evidence from the german socio-economic panel. Int. Arch. Occup. Environ. Health 2018, 91, 435–443. [Google Scholar] [CrossRef]
- Pudrovska, T.; Karraker, A. Gender, job authority, and depression. J. Health Soc. Behav. 2014, 55, 424–441. [Google Scholar] [CrossRef] [Green Version]
- Fan, Z.J.; Bonauto, D.K.; Foley, M.P.; Anderson, N.J.; Yragui, N.L.; Silverstein, B.A. Occupation and the prevalence of current depression and frequent mental distress, wa brfss 2006 and 2008. Am. J. Ind. Med. 2012, 55, 893–903. [Google Scholar] [CrossRef]
- Plaisier, I.; de Bruijn, J.G.; de Graaf, R.; ten Have, M.; Beekman, A.T.; Penninx, B.W. The contribution of working conditions and social support to the onset of depressive and anxiety disorders among male and female employees. Soc. Sci. Med. 2007, 64, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.P.; Gorenstein, C. Gender differences and disabilities of perceived depression in the workplace. J. Affect. Disord. 2015, 176, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Oliffe, J.L.; Phillips, M.J. Men, depression and masculinities: A review and recommendations. J. Men Health 2008, 5, 194–202. [Google Scholar] [CrossRef]
- Gooding, P.A.; Hurst, A.; Johnson, J.; Tarrier, N. Psychological resilience in young and older adults. Int. J. Geriatr. Psychiatry 2012, 27, 262–270. [Google Scholar] [CrossRef] [PubMed]
- Robb, C.; Haley, W.E.; Becker, M.A.; Polivka, L.A.; Chwa, H.J. Attitudes towards mental health care in younger and older adults: Similarities and differences. Aging Ment. Health 2003, 7, 142–152. [Google Scholar] [CrossRef]
- Lips-Wiersma, M.; Wright, S.; Dik, B. Meaningful work: Differences among blue-, pink-, and white-collar occupations. Career Dev. Int. 2016, 21, 534–551. [Google Scholar] [CrossRef]
- Saraç, M.; Meydan, B.; Efil, I. Does the relationship between person–organization fit and work attitudes differ for blue-collar and white-collar employees? Manag. Res. Rev. 2017, 40, 1081–1099. [Google Scholar] [CrossRef]
- Agarwal, B.; Brooks, S.K.; Greenberg, N. The role of peer support in managing occupational stress: A qualitative study of the sustaining resilience at work intervention. Workplace Health Saf. 2020, 68, 57–64. [Google Scholar] [CrossRef]
- Gilbreath, B.; Benson, P.G. The contribution of supervisor behaviour to employee psychological well-being. Work Stress 2004, 18, 255–266. [Google Scholar] [CrossRef]
- Keus van de Poll, M.; Nybergh, L.; Lornudd, C.; Hagberg, J.; Bodin, L.; Kwak, L.; Jensen, I.; Lohela-Karlsson, M.; Torgén, M.; Bergstrom, G. Preventing sickness absence among employees with common mental disorders or stress-related symptoms at work: A cluster randomised controlled trial of a problem-solving-based intervention conducted by the occupational health services. Occup. Environ. Med. 2020, 77, 454–461. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.-Y.; Hu, C. Abusive supervision and employee emotional exhaustion: Dispositional antecedents and boundaries. Group Organ. Manag. 2009, 34, 143–169. [Google Scholar] [CrossRef]
- Leung, M.-Y.; Liang, Q.; Olomolaiye, P. Impact of job stressors and stress on the safety behavior and accidents of construction workers. J. Manag. Eng. 2016, 32, 04015019. [Google Scholar] [CrossRef]
- Manuele, F.A. Reviewing heinrich: Dislodging two myths from the practice of safety. Prof. Saf. 2011, 56, 52–61. [Google Scholar]
- Forastieri, V. Prevention of psychosocial risks and work-related stress. Int. J. Labour. Res. 2016, 8, 11. [Google Scholar]
- Benavides, F.G.; Delclos, J.; Serra, C. Welfare state and public health: The role of occupational health. Gac. Sanit. 2017, 32, 377–380. [Google Scholar] [CrossRef]
- Kim, Y.S.; Rhee, K.Y.; Oh, M.J.; Park, J. The validity and reliability of the second korean working conditions survey. Saf. Health Work 2013, 4, 111–116. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Support from Colleagues | p | Support from Supervisor | p | ||
|---|---|---|---|---|---|---|
| No | Yes | No | Yes | |||
| Age | 0.012 | 0.235 | ||||
| Mean (SD) | 39.37 (9.85) | 39.74 (9.35) | 39.73 (9.76) | 39.56 (9.37) | ||
| Sex | <0.001 | <0.001 | ||||
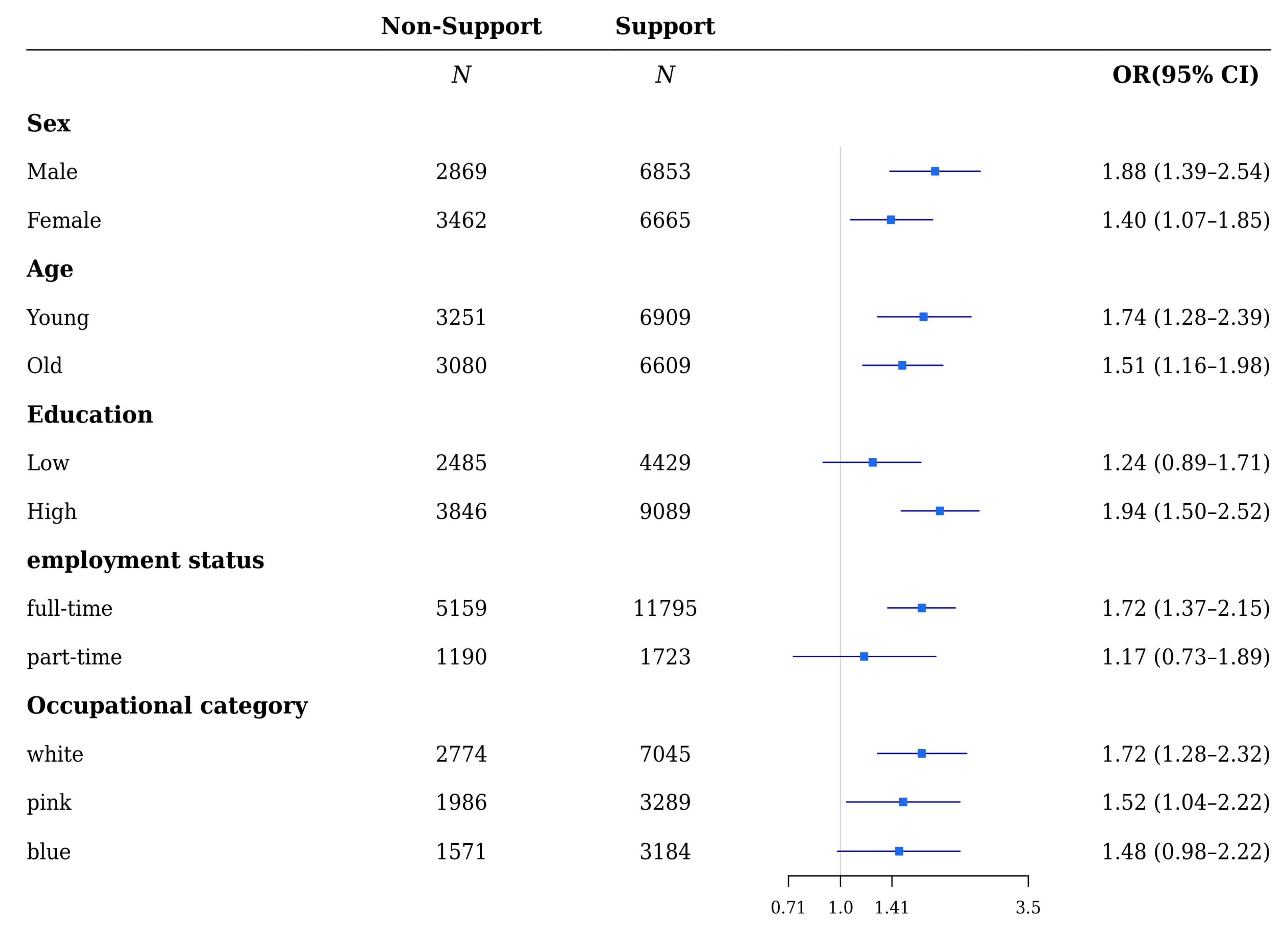
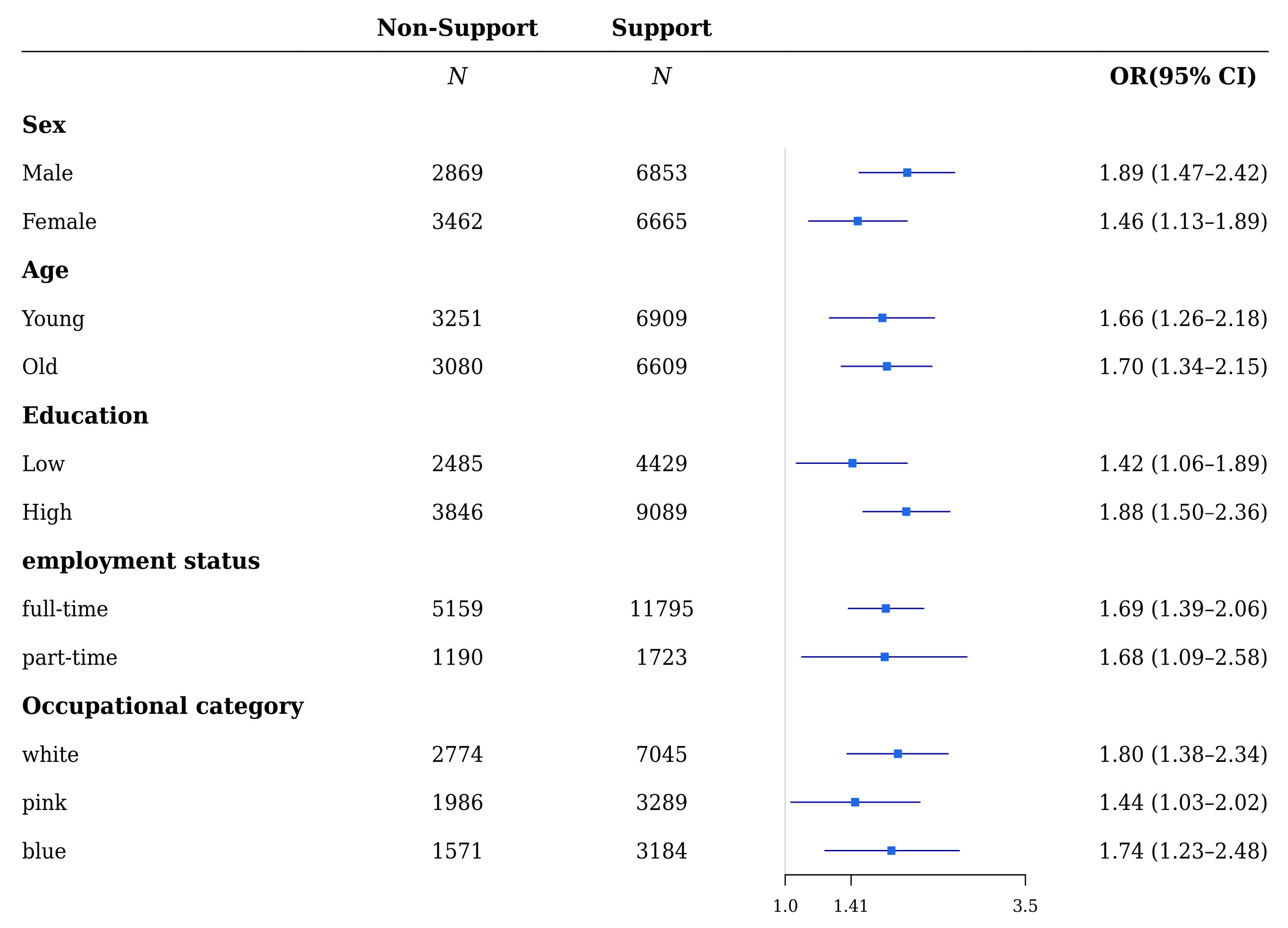
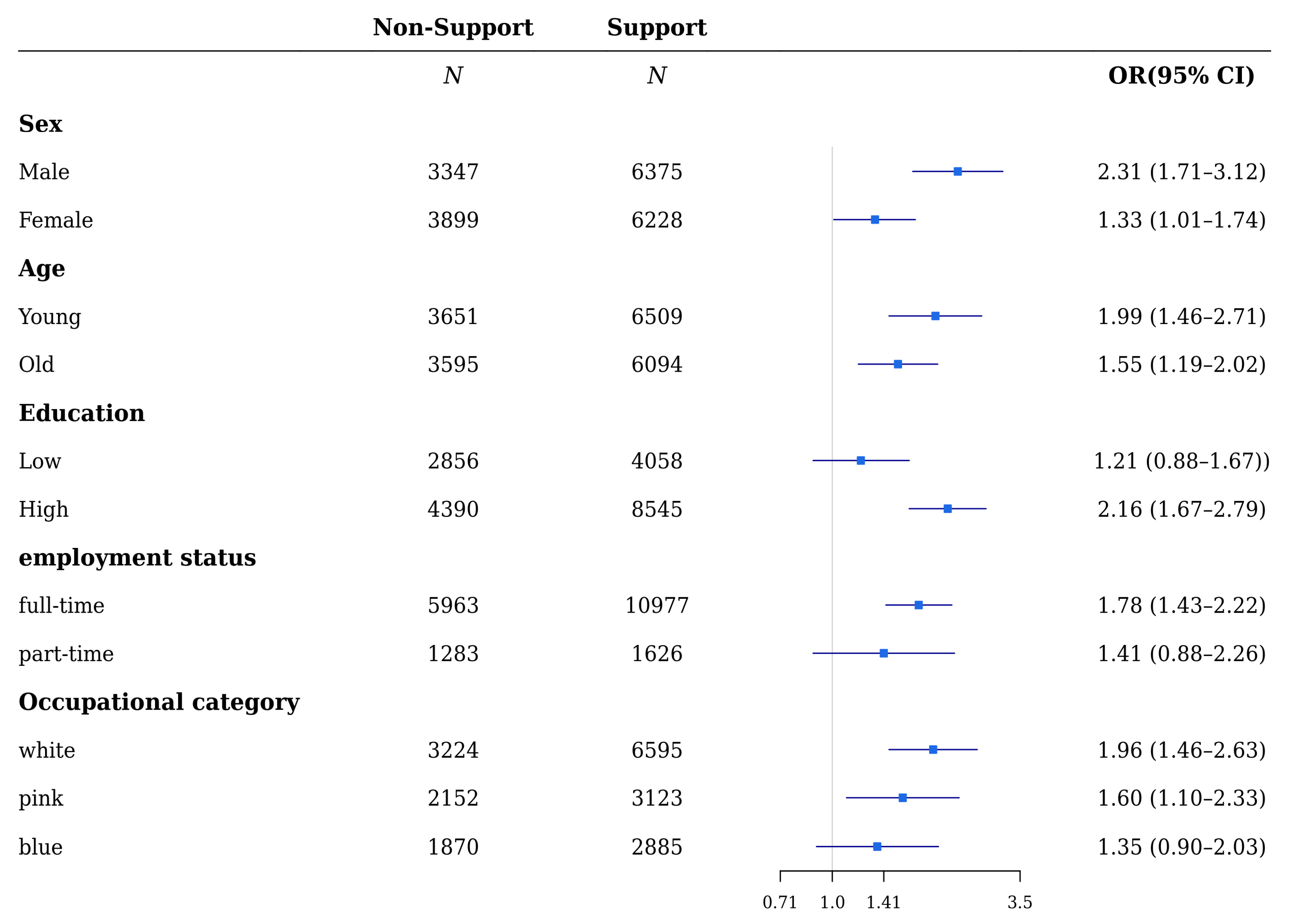
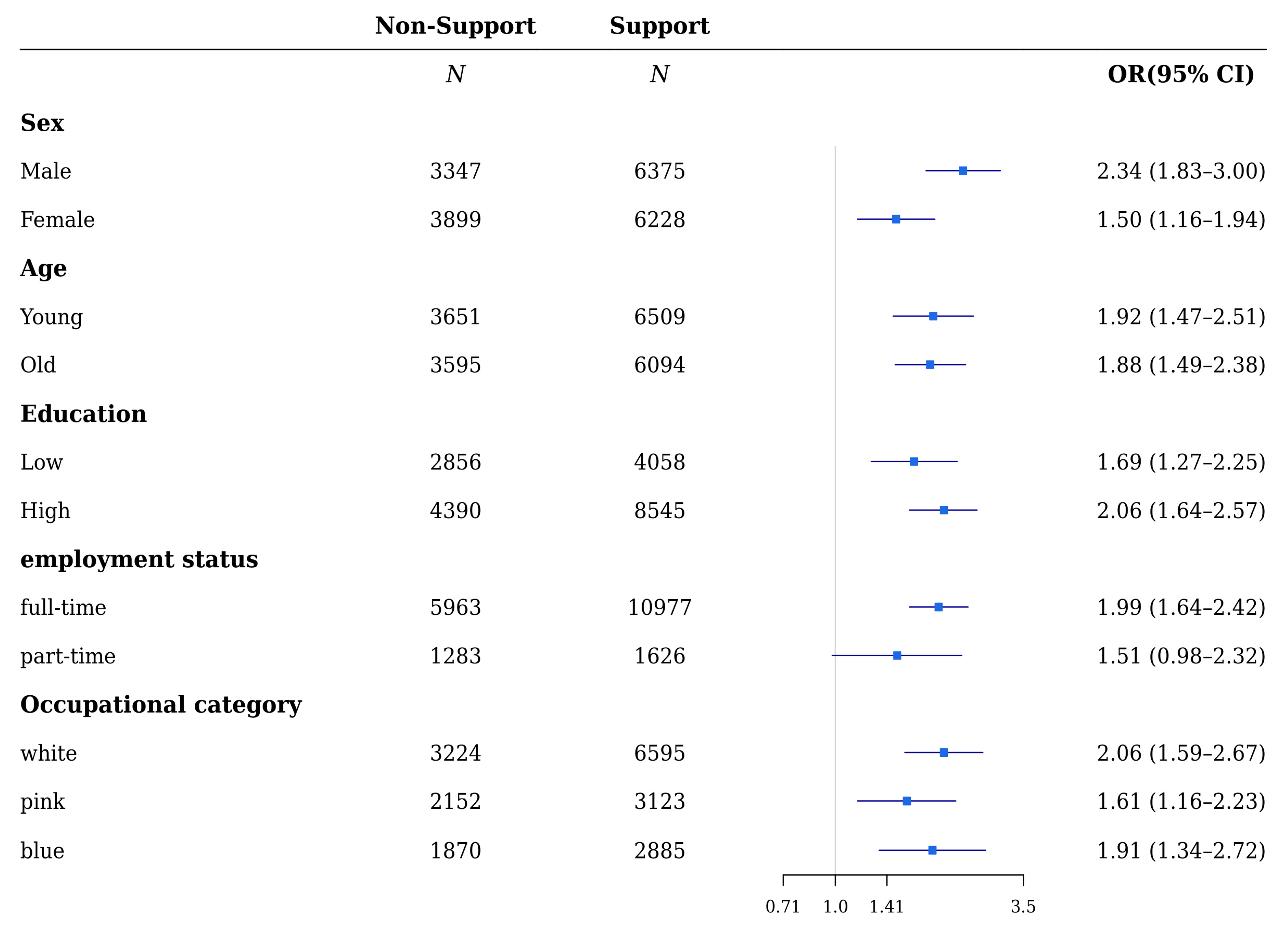
| Male | 2869 (29.51%) | 6853 (70.49%) | 3347 (34.43%) | 6375 (65.57%) | ||
| Female | 3462 (34.19%) | 6665 (65.81%) | 3899 (38.50%) | 6228 (61.50%) | ||
| Income | <0.001 | <0.001 | ||||
| Low | 1647 (40.77%) | 2393 (59.23%) | 1796 (44.46%) | 2244 (55.54%) | ||
| Low-Middle | 1766 (35.51%) | 3207 (64.49%) | 1976 (39.73%) | 2997 (60.27%) | ||
| High-Middle | 1732 (29.53%) | 4134 (70.47%) | 2039 (34.76%) | 3827 (65.24%) | ||
| High | 1186 (23.86%) | 3784 (76.14%) | 1435 (28.87%) | 3535 (71.13%) | ||
| Education | <0.001 | <0.001 | ||||
| Low | 2485 (35.94%) | 4429 (64.06%) | 2856 (41.31%) | 4058 (58.69%) | ||
| High | 3846 (29.73%) | 9089 (70.27%) | 4390 (33.94%) | 8545 (66.06%) | ||
| Employment status | <0.001 | <0.001 | ||||
| full-time | 5159 (30.30%) | 11,795 (69.63%) | 5963 (35.20%) | 10,977 (64.80%) | ||
| part-time | 1190 (40.78%) | 1723 (59.23%) | 1283 (44.10%) | 1626 (55.90%) | ||
| Work duration | <0.001 | <0.001 | ||||
| <5 year | 4208 (34.44%) | 8009 (65.56%) | 4721 (38.64%) | 7496 (61.36%) | ||
| ≥5 year | 2123 (27.82%) | 5509 (72.18%) | 2525 (33.08%) | 5107 (66.92%) | ||
| Working Hour | <0.001 | <0.001 | ||||
| ≤40 h | 3547 (30.88%) | 7939 (69.12%) | 4061 (35.36%) | 7425 (64.64%) | ||
| 41–52 h | 1958 (33.72%) | 3848 (66.28%) | 2215 (38.15%) | 3591 (61.85%) | ||
| ≥53 h | 826 (32.30%) | 1731 (67.70%) | 970 (37.94%) | 1587 (62.06%) | ||
| Shift Work | 0.209 | 0.442 | ||||
| No | 5629 (32.05%) | 11,935 (67.95%) | 6429 (36.60%) | 11,135 (63.40%) | ||
| Yes | 702 (30.72%) | 1583 (69.28%) | 817 (35.75%) | 1468 (64.25%) | ||
| Occupational category | <0.001 | <0.001 | ||||
| white-collar | 2774 (28.25%) | 7045 (71.75%) | 3224 (32.83%) | 6595 (67.17%) | ||
| pink-collar | 1986 (37.65%) | 3289 (62.35%) | 2152 (40.80%) | 3123 (59.20%) | ||
| blue-collar | 1571 (33.04%) | 3184 (66.96%) | 1870 (39.33%) | 2885 (60.67%) | ||
| Depression | <0.001 | <0.001 | ||||
| No | 6158 (31.66%) | 13,292 (68.34%) | 7046 (36.23%) | 12,404 (63.77%) | ||
| Yes | 173 (43.36%) | 226 (56.64%) | 200 (50.13%) | 199 (49.87%) | ||
| Anxiety | <0.001 | <0.001 | ||||
| No | 6105 (31.59%) | 13,223 (68.41%) | 6977 (36.10%) | 12,351 (63.90%) | ||
| Yes | 226 (43.38%) | 295 (56.62%) | 269 (51.63%) | 252 (48.37%) | ||
| Variable | Support from Colleagues | Support from Supervisor | ||
|---|---|---|---|---|
| Depression | Anxiety | Depression | Anxiety | |
| OR (95% CI) | OR (95% CI) | |||
| (Intercept) | 0.01 (0.00–0.02) | 0.01 (0.01–0.02) | 0.01 (0.00–0.02) | 0.01 (0.01–0.02) |
| Support | ||||
| Yes | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| No | 1.61 (1.31–1.97) | 1.69 (1.41–2.02) | 1.71 (1.40–2.09) | 1.91 (1.60–2.27) |
| Age | 1.02 (1.01–1.03) | 1.02 (1.01–1.03) | 1.02 (1.01–1.03) | 1.01 (1.00–1.03) |
| Sex | ||||
| Male | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Female | 1.01 (0.79–1.29) | 0.89 (0.71–1.10) | 1.01 (0.79–1.29) | 0.89 (0.72–1.11) |
| Income | ||||
| Low | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Low-Middle | 0.72 (0.53–0.97) | 0.78 (0.59–1.04) | 0.72 (0.54–0.98) | 0.79 (0.59–1.04) |
| High-Middle | 0.66 (0.47–0.91) | 0.77 (0.57–1.04) | 0.66 (0.47–0.91) | 0.77 (0.57–1.04) |
| High | 0.73 (0.50–1.07) | 1.16 (0.83–1.62) | 0.74 (0.50–1.08) | 1.18 (0.84–1.65) |
| Education | ||||
| Low | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| High | 0.99 (0.77–1.28) | 0.99 (0.79–1.24) | 1.00 (0.77–1.29) | 0.99 (0.79–1.25) |
| Employment status | ||||
| full-time | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| part-time | 1.15 (0.86–1.53) | 1.23 (0.94–1.59) | 1.16 (0.87–1.55) | 1.23 (0.95–1.60) |
| Work duration | ||||
| <5 year | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| ≥5 year | 1.03 (0.80–1.31) | 1.09 (0.87–1.35) | 1.03 (0.80–1.31) | 1.09 (0.88–1.35) |
| Working hour | ||||
| ≤40 h | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| 41–52 h | 1.17 (0.93–1.47) | 1.47 (1.21–1.79) | 1.17 (0.93–1.47) | 1.47 (1.20–1.78) |
| ≥53 h | 1.35 (0.99–1.84) | 1.32 (1.00–1.74) | 1.34 (0.98–1.83) | 1.30 (0.99–1.72) |
| Shift work | ||||
| No | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| Yes | 1.01 (0.73–1.39) | 1.21 (0.93–1.58) | 1.01 (0.73–1.38) | 1.23 (0.95–1.60) |
| Occupational category | ||||
| white-collar | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) | 1.00 (reference) |
| pink-collar | 0.90 (0.68–1.19) | 1.04 (0.81–1.33) | 0.91 (0.69–1.20) | 1.05 (0.82–1.34) |
| blue-collar | 0.90 (0.66–1.22) | 0.95 (0.73–1.24) | 0.90 (0.66–1.22) | 0.95 (0.73–1.23) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, J.; Lee, S.; Sim, J.; Kim, S.; Cho, A.; Yun, B.; Yoon, J.-H. Association between Self-Perceived Social Support in the Workplace and the Presence of Depressive/Anxiety Symptoms. Int. J. Environ. Res. Public Health 2021, 18, 10330. https://doi.org/10.3390/ijerph181910330
Oh J, Lee S, Sim J, Kim S, Cho A, Yun B, Yoon J-H. Association between Self-Perceived Social Support in the Workplace and the Presence of Depressive/Anxiety Symptoms. International Journal of Environmental Research and Public Health. 2021; 18(19):10330. https://doi.org/10.3390/ijerph181910330
Chicago/Turabian StyleOh, Juyeon, Seunghyun Lee, Juho Sim, Seunghan Kim, Ara Cho, Byungyoon Yun, and Jin-Ha Yoon. 2021. "Association between Self-Perceived Social Support in the Workplace and the Presence of Depressive/Anxiety Symptoms" International Journal of Environmental Research and Public Health 18, no. 19: 10330. https://doi.org/10.3390/ijerph181910330
APA StyleOh, J., Lee, S., Sim, J., Kim, S., Cho, A., Yun, B., & Yoon, J.-H. (2021). Association between Self-Perceived Social Support in the Workplace and the Presence of Depressive/Anxiety Symptoms. International Journal of Environmental Research and Public Health, 18(19), 10330. https://doi.org/10.3390/ijerph181910330