
Housing Instability and Depression among US Mothers Following a Nonmarital Birth

 ,
, 
Abstract
:1. Introduction
1.1. Theoretical Background
1.2. The Present Study
2. Materials and Methods
2.1. Data and Sample
2.2. Measures
2.2.1. Major Depressive Episode (MDE)
2.2.2. Cumulative Residential Moves
2.2.3. Housing Arrangements
2.2.4. Controls
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics of Mothers Unmarried at Childbirth
3.2. Cumulative Residential Moves and Housing Arrangements Following a Nonmarital Birth
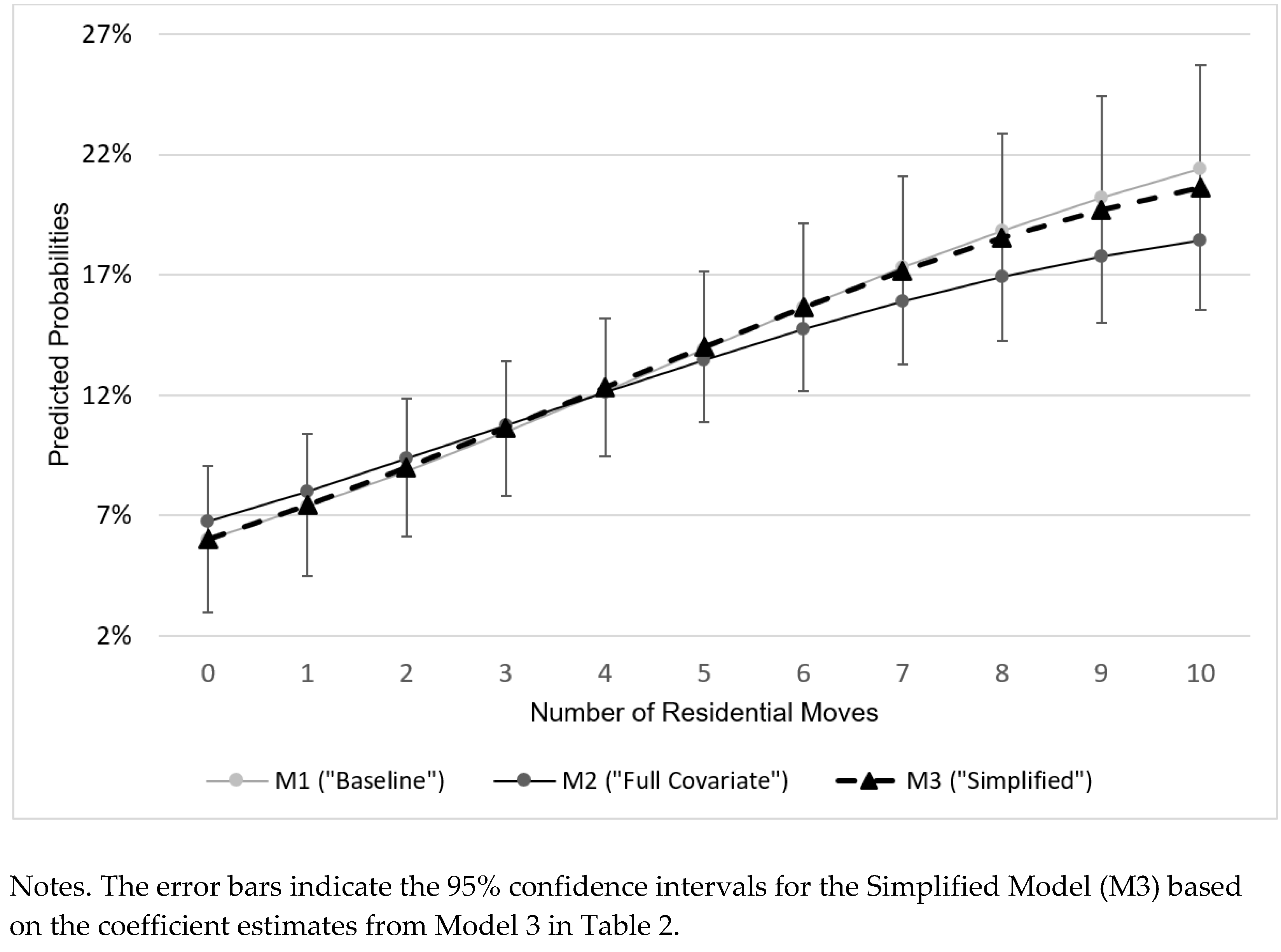
3.3. Effects of Cumulative Residential Moves on MDE among Mothers after a Nonmarital Birth
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Sociodemographic Characteristics | 0–1 Move (n = 717; 23.5%) | 2–5 Moves (n = 1473; 48.3%) | 6 + Moves (n = 862; 28.2%) | |||
|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | % | 95% CI | |
| Age at nonmarital childbirth | ||||||
| 15–19 | 3.1 | 1.8–5.5 | 13.1 | 10.0–16.9 | 24.3 | 18.7–30.9 |
| 20−29 | 44.8 | 37.0–52.9 | 57.0 | 50.6–63.1 | 64.0 | 56.6–70.8 |
| 30+ | 52.1 | 44.1–59.9 | 30.0 | 24.2–36.5 | 11.7 | 7.4–17.9 |
| Race/ethnicity | ||||||
| White | 40.0 | 32.2–48.4 | 29.4 | 23.4–36.4 | 16.7 | 12.1–22.5 |
| Black | 26.2 | 20.5–32.9 | 35.0 | 29.8–40.6 | 52.1 | 44.6–59.5 |
| Hispanic | 26.2 | 20.2–33.3 | 28.9 | 23.6–34.9 | 25.6 | 19.0–33.4 |
| Other | 7.5 | 4.2–13.0 | 6.7 | 4.1–10.7 | 5.7 | 2.4–12.8 |
| Education | ||||||
| HS or lower | 46.2 | 38.4–54.3 | 57.7 | 51.4–63.8 | 70.9 | 63.4–77.4 |
| Some college | 20.6 | 15.7–26.6 | 24.7 | 19.9–30.2 | 17.4 | 13.3–22.5 |
| College degree | 33.2 | 26.3–40.8 | 17.6 | 12.9–23.6 | 11.7 | 6.6–19.9 |
| Employment status | ||||||
| Not employed | 25.4 | 18.1–34.4 | 29.7 | 24.0–36.2 | 30.3 | 24.1–37.2 |
| Employed | 74.6 | 65.6–81.9 | 70.3 | 63.8–76.1 | 69.7 | 62.8–75.9 |
| Income to poverty ratio (YR 15) | ||||||
| 0–99% | 29.2 | 21.3–38.7 | 34.8 | 28.7–41.4 | 45.0 | 37.9–52.4 |
| 100–199% | 15.8 | 11.3–21.5 | 23.7 | 19.0–29.1 | 29.6 | 22.9–37.4 |
| 200%+ | 55.0 | 46.5–63.2 | 41.5 | 35.2–48.2 | 25.4 | 18.7–33.5 |
| Marital/cohabitation status (YR 15) | ||||||
| W/other biological parent | 67.1 | 59.9–73.7 | 42.4 | 36.1–48.9 | 21.6 | 15.9–28.6 |
| W/someone else | 6.5 | 4.1–10.0 | 21.6 | 16.8–27.4 | 29.5 | 23.5–36.4 |
| No | 26.4 | 20.4–33.4 | 36.0 | 30.6–41.8 | 48.9 | 41.5–56.3 |
| Housing Arrangement | Year 1 | Year 3 | Year 5 | Year 9 | Year 15 |
|---|---|---|---|---|---|
| Own | 43.1 (35.7–50.9) | 47.2 (39.4–55.1) | 50.8 (42.8–58.8) | 54.6 (46.2–62.8) | 56.0 (47.8–63.9) |
| Rent | 48.2 (40.1–56.4) | 44.4 (36.2–52.8) | 43.5 (35.3–52.0) | 41.7 (33.5–50.5) | 39.0 (31.1–47.6) |
| Live with family or friends | 7.9 (4.2–14.6) | 8.0 (4.2–14.7) | 5.4 (3.3–8.9) | 3.7 (2.0–6.7) | 3.6 (1.8–7.1) |
| Other | 0.7 (0.2–2.4) | 0.5 (0.2–1.1) | 0.3 (0.1–1.1) | 0.1 (0.1–0.1) | 1.4 (0.5–3.9) |
References
- Turney, K. Prevalence and correlates of stability and change in maternal depression: Evidence from the Fragile Families and Child Wellbeing Study. PLoS ONE 2012, 7, e45709. [Google Scholar] [CrossRef]
- Martin-West, S. The role of social support as a moderator of housing instability in single mother and two-parent households. Soc. Work Res. 2019, 43, 31–42. [Google Scholar] [CrossRef]
- McLanahan, S.; Percheski, C. Family structure and the reproduction of inequalities. Annu. Rev. Sociol. 2008, 34, 257–276. [Google Scholar] [CrossRef]
- McLanahan, S. Fragile families and the reproduction of poverty. Ann. Am. Acad. Pol. Soc. Sci. 2009, 621, 111–131. [Google Scholar] [CrossRef] [PubMed]
- McLanahan, S.; Beck, A.N. Parental relationships in fragile families. Future Child. 2010, 20, 17–37. [Google Scholar] [CrossRef]
- Lehrer, E.; Crittenden, K.; Norr, K.F. Depression and economic self-sufficiency among inner-city minority mothers. Soc. Sci. Res. 2002, 31, 285–309. [Google Scholar] [CrossRef]
- Povich, D.; Roberts, B.; Mather, M. Low-Income Working Mothers and State Policy: Investing for a Better Economic Future; The Working Poor Families Project: Chevy Chase, MD, USA, 2014. [Google Scholar]
- Hsueh, J.; Yoshikawa, H. Working nonstandard schedules and variable shifts in low-income families: Associations with parental psychological well-being, family functioning, and child well-being. Dev. Psychol. 2007, 43, 620–632. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.; Salas-Wright, C.P.; Vaughn, M.G. Trends in depression among low-income mothers in the United States, 2005–2015. J Affect. Disord. 2018, 235, 72–75. [Google Scholar] [CrossRef]
- Vásquez-Vera, H.; Palència, L.; Magna, I.; Mena, C.; Neira, J.; Borrell, C. The threat of home eviction and its effects on health through the equity lens: A systematic review. Soc. Sci. Med. 2017, 175, 199–208. [Google Scholar] [CrossRef]
- Burgard, S.A.; Seefeldt, K.S.; Zelner, S. Housing instability and health: Findings from the Michigan recession and recovery study. Soc. Sci. Med. 2012, 75, 2215–2224. [Google Scholar] [CrossRef]
- Pollack, C.E.; Lynch, J. Health status of people undergoing foreclosure in the Philadelphia region. Am. J. Public. Health 2009, 99, 1833–1839. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.L. Housing Instability: Toward A Better Understanding of Frequent Residential Mobility among America’s Urban Poor; Center for Housing Policy: Washington, DC, USA, 2010. [Google Scholar]
- Taylor, M.P.; Pevalin, D.J.; Todd, J. The psychological costs of unsustainable housing commitments. Psychol. Med. 2007, 37, 1027–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, L.M.; Clark, S.L. Homeplace and housing in the lives of low-income urban African American families. In African American Family Life: Ecological and Cultural Diversity; McLoyd, V.C., Hill, N.E., Dodge, K.A., Eds.; The Guilford Press: New York, NY, USA, 2005; pp. 166–210. [Google Scholar]
- Kozhimannil, K.B. Association between diabetes and perinatal depression among low-income mothers. JAMA 2009, 301, 842–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katon, J.G.; Russo, J.; Gavin, A.R.; Melville, J.L.; Katon, W.J. Diabetes and depression in pregnancy: Is there an association? J. Women’s Health 2011, 20, 983–989. [Google Scholar] [CrossRef] [PubMed]
- Amato, S.; Nobay, F.; Amato, D.P.; Abar, B.; Adler, D. Sick and unsheltered: Homelessness as a major risk factor for emergency care utilization. Am. J. Emerg. Med. 2019, 37, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Poremski, D.; Woodhall-Melnik, J.; Lemieux, A.J.; Stergiopoulos, V. Persisting barriers to employment for recently housed adults with mental illness who were homeless. J. Urban Health 2016, 93, 96–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloom, N.D.; Lasner, M.G. Affordable Housing in New York: The People, Places, and Policies that Transformed A City; Princeton University Press: Princeton, NJ, USA, 2019. [Google Scholar]
- Quigley, J.M. Just Suppose: Housing Subsidies for Low Income Renters; The Harvard Joint Center for Housing Studies: Cambridge, MA, USA, 2007. [Google Scholar]
- Teater, B.A. A qualitative evaluation of the Section 8 Housing Choice Voucher Program. Qual. Soc. Work 2011, 10, 503–519. [Google Scholar] [CrossRef]
- Berger, L.M.; Heintze, T.; Naidich, W.B.; Meyers, M.K. Subsidized housing and household hardship among low-income single-mother households. J. Marriage Fam. 2008, 70, 934–949. [Google Scholar] [CrossRef]
- Waldfogel, J.; Craigie, T.A.; Brooks-Gunn, J. Fragile families and child wellbeing. Future child. 2010, 20, 87–112. [Google Scholar] [CrossRef]
- Curtis, M.A.; Corman, H.; Noonan, K.; Reichman, N.E. Maternal depression as a risk factor for family homelessness. Am. J. Public Health 2014, 104, 1664–1670. [Google Scholar] [CrossRef]
- Suglia, S.F.; Duarte, C.S.; Sandel, M.T. Housing quality, housing instability, and maternal mental health. J. Urban Health 2011, 88, 1105–1116. [Google Scholar] [CrossRef] [Green Version]
- Davey-Rothwell, M.A.; German, D.; Latkin, C.A. Residential transience and depression: Does the relationship exist for men and women? J. Urban Health 2008, 85, 707–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, P.J.; Henry, D.B.; Marcal, K.E. Family and housing instability: Longitudinal impact on adolescent emotional and behavioral well-being. Soc. Sci. Res. 2015, 53, 364–374. [Google Scholar] [CrossRef] [PubMed]
- Gavin, A.R.; Lindhorst, T.; Lohr, M.J. The prevalence and correlates of depressive symptoms among adolescent mothers: Results from a 17-year longitudinal study. Women Health 2011, 51, 525–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conger, R.D.; Donnellan, M.B. An interactionist perspective on the socioeconomic context of human development. Annu. Rev. Psychol. 2007, 58, 175–199. [Google Scholar] [CrossRef] [Green Version]
- Conger, R.D.; Ge, X.; Elder, G.H.; Lorenz, F.O.; Simons, R.L. Economic stress, coercive family process, and developmental problems of adolescents. Child. Dev. 1994, 65, 541–561. [Google Scholar] [CrossRef]
- Conger, R.D.; Wallace, L.E.; Sun, Y.; Simons, R.L.; McLoyd, V.C.; Brody, G.H. Economic pressure in African American families: A replication and extension of the family stress model. Dev. Psychol. 2002, 38, 179–193. [Google Scholar] [CrossRef] [PubMed]
- Elder, G.H. The life course paradigm: Social change and individual development. In Examining Lives in Context: Perspectives on the Ecology of Human Development; Moen, P., Elder, G.H., Luscher, K., Eds.; American Psychological Association: Washington, DC, USA, 1995; pp. 101–139. [Google Scholar]
- Clausen, J.A. American Lives; Free Press: New York, NY, USA, 1993. [Google Scholar]
- Dannefer, D. Cumulative advantage/disadvantage and the life course: Cross-fertilizing age and social science theory. J. Gerontol. B Psychol. Sci. Soc. Sci. 2003, 58, S327–S337. [Google Scholar] [CrossRef]
- O’Rand, A.M. The precious and the precocious: Understanding cumulative disadvantage and cumulative advantage over the life course. Gerontologist. 1996, 36, 230–238. [Google Scholar] [CrossRef]
- Willson, A.E.; Shuey, K.M.; Elder, G.H. Cumulative advantage processes as mechanisms of inequality in life course health. Am. J. Sociol. 2007, 112, 1886–1924. [Google Scholar] [CrossRef]
- Knecht, M.; Wiese, B.S.; Freund, A.M. Going beyond work and family: A longitudinal study on the role of leisure in the work-life interplay. J. Organ. Behav. 2016, 37, 1061–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spini, D.; Bernardi, L.; Oris, M. Toward a life course framework for studying vulnerability. Res. Hum. Dev. 2017, 14, 5–25. [Google Scholar] [CrossRef]
- Miech, R.A.; Shanahan, M.J. Socioeconomic status and depression over the life course. J. Health Soc. Behav. 2000, 41, 162–176. [Google Scholar] [CrossRef]
- Shrira, A.; Litwin, H. The effect of lifetime cumulative adversity and depressive symptoms on functional status. J. Gerontol. B Psychol. Sci. Soc. Sci. 2014, 69, 953–965. [Google Scholar] [CrossRef] [Green Version]
- Reichman, N.E.; Teitler, J.O.; Garfinkel, I.; McLanahan, S.S. Fragile families: Sample and design. Child. Youth Serv. Rev. 2001, 23, 303–326. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Mroczek, D.; Ustun, B.; Wittchen, H.U. The World Health Organization Composite International Diagnostic Interview Short-Form (CIDI-SF). Int. J. Methods Psychiatr. Res. 1998, 7, 171–185. [Google Scholar] [CrossRef]
- Beeber, L.S.; Schwartz, T.A.; Martinez, M.I.; Holditch-Davis, D.; Bledsoe, S.E.; Canuso, R.; Lewis, V.S. Depressive symptoms and compromised parenting in low-income mothers of infants and toddlers: Distal and proximal risks. Res. Nurs. Health 2014, 37, 276–291. [Google Scholar] [CrossRef]
- Fazel, S.; Geddes, J.R.; Kushel, M. The health of homeless people in high-income countries: Descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet 2014, 384, 1529–1540. [Google Scholar] [CrossRef] [Green Version]
- Kushel, M.B.; Evans, J.L.; Perry, S.; Robertson, M.J.; Moss, A.R. No door to lock: Victimization among homeless and marginally housed persons. Arch. Intern. Med. 2003, 163, 2492–2499. [Google Scholar] [CrossRef]
- Rademacher, I.; Wiedrich, K.; McKernan, S.M.; Ratcliffe, C.; Gallagher, M. Weatering the Storm: Have IDAs Helped Low-Income Homebuyers Avoid Foreclosure? Urban Institute: Washington, DC, USA, 2010. [Google Scholar]
- Grinstein-Weiss, M.; Sherraden, M.W.; Rohe, W.; Gale, W.G.; Schreiner, M.J.; Key, C. Long-Term Follow-Up of Individual Development Accounts: Evidence from the ADD Experiment; The University of North Carolina: Chapel Hill, NC, USA, 2012. [Google Scholar]
- Oh, S.; DiNitto, D.M.; Kim, Y. Exiting poverty: A systematic review of U.S. postsecondary education and job skills training programs in the post-welfare reform era. Int. J. Sociol. Soc. Policy. in press.
- Oh, S.; DiNitto, D.M.; Powers, D.A. A longitudinal evaluation of government-sponsored job skills training and basic employment services among U.S. baby boomers with economic disadvantages. Eval. Program Plann. 2020, 82, 101845. [Google Scholar] [CrossRef] [PubMed]
- Tunstall, R. Housing. In Social Policy in A Cold Climate: Policies and Their Consequences since the Crisis; Lupton, R., Burchardt, T., Hills, J., Stewart, K., Vizard, P., Eds.; Policy Press: Bristol, UK, 2016; pp. 125–145. [Google Scholar]
- Tunstall, B. Housing and Gender: A Pre-Budget Briefing from the UK Women’s Budget Group; UK Women’s Budget Group: London, UK, 2020. [Google Scholar]

| Sociodemographic Characteristics | Married (n = 773; 54.8%) | Not Married (n = 2279; 45.2%) | AOR | 95% CI | ||
|---|---|---|---|---|---|---|
| % | 95% CI | % | 95% CI | |||
| Age | ||||||
| 15–19 | 2.5 | 1.4–4.4 | 24.1 | 19.8–29.0 | 4.98 *** | 2.19−11.35 |
| 20−29 | 51.3 | 43.5–58.9 | 55.7 | 50.5–60.7 | 0.77 | 0.44−1.35 |
| 30+ | 46.3 | 38.7–54.0 | 20.2 | 16.0–25.2 | 1.00 | - |
| Race/ethnicity | ||||||
| White | 44.7 | 37.2–52.5 | 11.0 | 8.4–14.4 | 1.00 | - |
| Black | 14.7 | 10.4–20.3 | 55.4 | 50.5–60.2 | 8.52 *** | 4.46−16.31 |
| Hispanic | 30.2 | 23.2–38.4 | 31.3 | 27.0–36.0 | 3.45 ** | 1.66−7.17 |
| Other | 10.4 | 7.0–15.3 | 2.3 | 1.4–3.8 | 4.30 ** | 1.46−12.70 |
| Education | ||||||
| HS or lower | 40.9 | 33.0–49.3 | 80.1 | 76.3–83.5 | 15.70 *** | 7.24−34.07 |
| Some college | 21.4 | 16.8–26.9 | 18.3 | 15.0–22.2 | 8.16 *** | 4.03−16.52 |
| College degree | 37.7 | 30.8–45.2 | 1.5 | 1.0–2.3 | 1.00 | - |
| Income to poverty ratio | ||||||
| 0–99% | 24.5 | 16.6–34.7 | 52.0 | 46.9–57.1 | 2.69 ** | 1.38−5.27 |
| 100–199% | 15.5 | 11.5–20.7 | 28.6 | 24.0–33.6 | 2.64 ** | 1.46−4.78 |
| 200%+ | 60.0 | 51.2–68.1 | 19.4 | 15.6–23.8 | 1.00 | - |
| Born in U.S. | ||||||
| Yes | 65.6 | 57.2–73.1 | 82.5 | 77.9–86.3 | 1.00 | - |
| No | 34.4 | 26.9–42.8 | 17.6 | 13.7–22.2 | 0.26 *** | 0.13−0.50 |
| TANF/SNAP receipt | ||||||
| Yes | 11.2 | 6.6–18.3 | 38.2 | 33.9–42.8 | 1.34 | 0.70−2.56 |
| No | 88.8 | 81.7–93.4 | 61.8 | 57.2–66.2 | 1.00 | - |
| Housing assistance receipt | ||||||
| Yes | 8.8 | 4.8–15.8 | 24.5 | 20.4–29.1 | 1.17 | 0.52−2.62 |
| No | 91.2 | 84.2–95.2 | 75.6 | 71.0–79.6 | 1.00 | - |
| Housing Arrangement | Year 1 | Year 3 | Year 5 | Year 9 | Year 15 |
|---|---|---|---|---|---|
| Own | 6.2 (4.4–8.7) | 7.9 (5.6–11.0) | 10.2 (7.5–13.7) | 14.3 (11.0–18.4) | 15.6 (13.0–18.7) |
| Rent | 61.2 (56.4–65.8) | 67.1 (62.2–71.6) | 69.5 (64.5–74.0) | 70.2 (65.4–74.6) | 71.5 (67.4–75.2) |
| Live with family or friends | 30.5 (26.3–35.0) | 23.5 (19.5–28.1) | 19.4 (15.5–23.9) | 14.7 (11.6–18.3) | 9.9 (7.7–12.7) |
| Other | 2.1 (1.0–4.1) | 1.5 (0.9–2.5) | 0.9 (0.5–1.6) | 0.9 (0.6–1.3) | 3.0 (1.8–5.1) |
| Variables | M1: Baseline Model | M2: Full Covariate Model | M3: Simplified Model | |||
|---|---|---|---|---|---|---|
| AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | |
| Key Covariates | ||||||
| No. of residential moves | 1.255 ** | 1.072–1.470 | 1.236 ** | 1.071−1.427 | 1.279 ** | 1.102−1.484 |
| No. of residential moves2 | 0.992 † | 0.982–1.002 | 0.992 * | 0.984−0.999 | 0.990 * | 0.982−0.999 |
| Parenting stress | 2.253 *** | 1.591−3.191 | 2.315 *** | 1.625−3.298 | ||
| Serious health conditions | 3.091 ** | 1.448−6.598 | 3.314** | 1.549−7.089 | ||
| Sociodemographic Controls | ||||||
| Age | ||||||
| 30–34 | 0.861 | 0.333−2.225 | ||||
| 35–44 | 0.791 | 0.346−1.808 | ||||
| 45+ | 1.000 | - | ||||
| Race/ethnicity | ||||||
| White | 1.000 | - | ||||
| Black | 0.635 | 0.358−1.127 | ||||
| Hispanic | 1.336 | 0.591−3.020 | ||||
| Other | 0.710 | 0.231−2.179 | ||||
| Born in U.S. | ||||||
| No | 0.344 | 0.084−1.403 | ||||
| Yes | 1.000 | - | ||||
| Educational attainment | ||||||
| High school or lower | 1.304 | 0.662−2.566 | ||||
| Some college | 0.870 | 0.443−1.710 | ||||
| College degree | 1.000 | - | ||||
| Marital/cohabitation status | ||||||
| W/other biological parent | 1.000 | - | ||||
| W/someone else | 1.143 | 0.542−2.410 | ||||
| No | 1.413 | 0.662−3.014 | ||||
| No. of children in household | 1.079 | 0.894−1.302 | ||||
| Income to poverty ratio | ||||||
| 0–99% | 1.059 | 0.426−2.635 | ||||
| 100–199% | 0.661 | 0.299−1.461 | ||||
| 200%+ | 1.000 | - | ||||
| Received TANF or SNAP | ||||||
| No | 1.000 | - | ||||
| Yes | 1.568 | 0.837−2.936 | ||||
| Received housing assistance | ||||||
| No | 1.000 | - | ||||
| Yes | 0.585 † | 0.330−1.037 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, S.; Zapcic, I.; Vaughn, M.G.; Salas-Wright, C.P.; Kim, Y. Housing Instability and Depression among US Mothers Following a Nonmarital Birth. Int. J. Environ. Res. Public Health 2021, 18, 10322. https://doi.org/10.3390/ijerph181910322
Oh S, Zapcic I, Vaughn MG, Salas-Wright CP, Kim Y. Housing Instability and Depression among US Mothers Following a Nonmarital Birth. International Journal of Environmental Research and Public Health. 2021; 18(19):10322. https://doi.org/10.3390/ijerph181910322
Chicago/Turabian StyleOh, Sehun, Ian Zapcic, Michael G. Vaughn, Christopher P. Salas-Wright, and Yeonwoo Kim. 2021. "Housing Instability and Depression among US Mothers Following a Nonmarital Birth" International Journal of Environmental Research and Public Health 18, no. 19: 10322. https://doi.org/10.3390/ijerph181910322
APA StyleOh, S., Zapcic, I., Vaughn, M. G., Salas-Wright, C. P., & Kim, Y. (2021). Housing Instability and Depression among US Mothers Following a Nonmarital Birth. International Journal of Environmental Research and Public Health, 18(19), 10322. https://doi.org/10.3390/ijerph181910322