
Awareness, Knowledge and Risky Behaviors of Sexually Transmitted Diseases among Young People in Greece

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
Ethics Approval
2.2. Data Collection and Processing
2.3. Evaluation of Knowledge Score
2.4. Data Management
2.5. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics of Respondents
3.2. Sexual-Risk Associated Knowledge
3.3. Evaluation of Sexual Behavior-Associated Risk
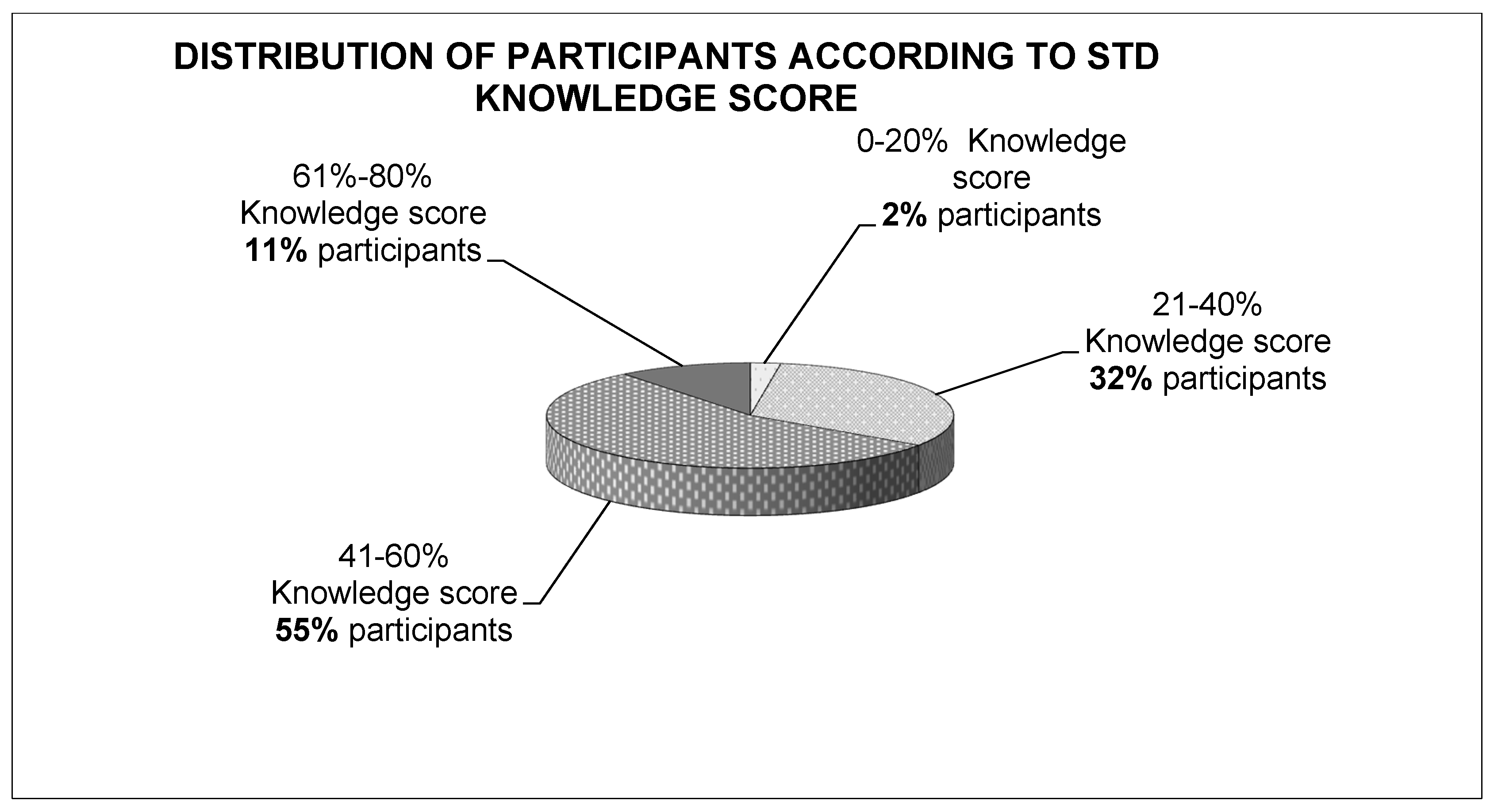
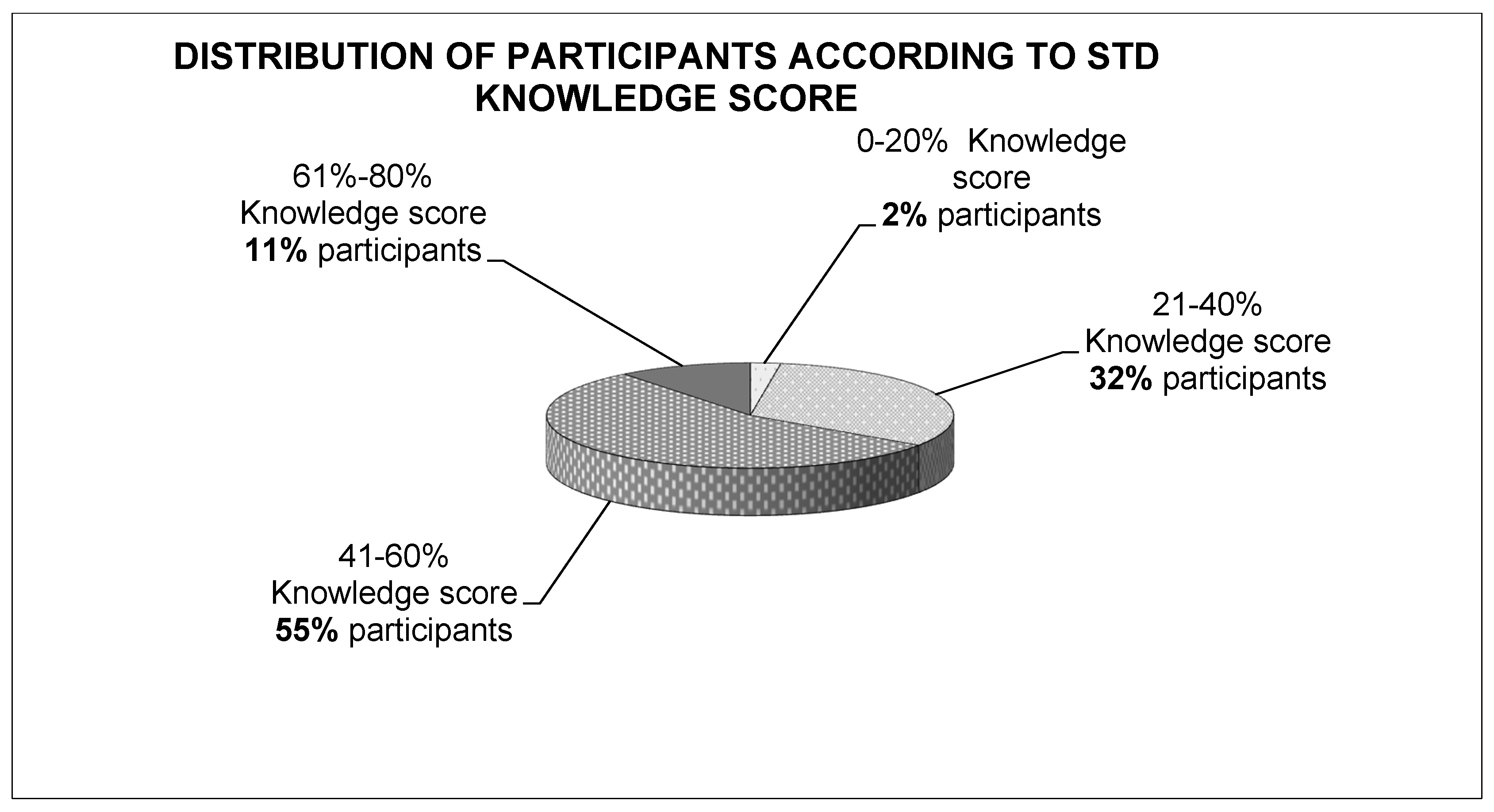
3.4. Assessment of STD Knowledge Score
3.5. Unifactorial Associations of Knowledge Score with Socio-Demographic Characteristics
3.6. Multifactorial Associations of Knowledge Score with Socio-Demographic Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Newman, L.; Rowley, J.; Hoorn, S.v.; Wijesooriya, N.S.; Unemo, M.; Low, N.; Stevens, G.; Gottlieb, S.; Kiarie, J.; Temmerman, M. Global Estimates of the Prevalence and Incidence of Four Curable Sexually Transmitted Infections in 2012 Based on Systematic Review and Global Reporting. PLoS ONE 2015, 10, e0143304. [Google Scholar] [CrossRef] [Green Version]
- Rowley, J.; Hoorn, S.V.; Korenromp, E.; Low, N.; Unemo, M.; AbuRaddad, L.J.; Chico, R.M.; Smolak, A.; Newman, L.; Gottlieb, S.; et al. Chlamydia, Gonorrhoea, Trichomoniasis and Syphilis: Global Prevalence and Incidence Estimates. 2016. Available online: https://www.who.int/bulletin/volumes/97/8/18-228486.pdf (accessed on 7 August 2021).
- Sexually Transmitted Infections (STIs). Available online: https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis) (accessed on 7 August 2021).
- Korenromp, E.L.; Rowley, J.; Alonso, M.; Mello, M.B.; Wijesooriya, N.S.; Mahiané, S.G.; Ishikawa, N.; Le, L.-V.; Newman-Owiredu, M.; Nagelkerke, N.; et al. Global burden of maternal and congenital syphilis and associated adverse birth outcomes—Estimates for 2016 and progress since 2012. PLoS ONE 2019, 14, e0211720. [Google Scholar] [CrossRef]
- WHO|Global Health Sector Strategy on Sexually Transmitted Infections, 2016–2021. Available online: https://www.who.int/reproductivehealth/publications/rtis/ghss-stis/en/ (accessed on 7 August 2021).
- Juliana, N.C.A.; Omar, A.M.; Pleijster, J.; Aftab, F.; Uijldert, N.B.; Ali, S.M.; Ouburg, S.; Sazawal, S.; Morré, S.A.; Deb, S.; et al. The Natural Course of Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, and Mycoplasma genitalium in Pregnant and Post-Delivery Women in Pemba Island, Tanzania. Microorganisms 2021, 9, 1180. [Google Scholar] [CrossRef]
- World Health Organization. Department of Child and Adolescent Health and Development. World Health Organization, Child and Adolescent Health and Development Progress Report 2009; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Bekker, L.-G.; Johnson, L.; Wallace, M.; Hosek, S. Building our youth for the future. J. Int. AIDS Soc. 2015, 18, 20027. [Google Scholar] [CrossRef] [PubMed]
- Vanable, P.A.; Carey, M.P.; Brown, J.L.; DiClemente, R.J.; Salazar, L.F.; Brown, L.K.; Romer, D.; Valois, R.F.; Hennessy, M.; Stanton, B.F. Test–Retest Reliability of Self-Reported HIV/STD-Related Measures Among African-American Adolescents in Four U.S. Cities. J. Adolesc. Health 2009, 44, 214–221. [Google Scholar] [CrossRef] [Green Version]
- Siracusano, S.; Silvestri, T.; Casotto, D. Sexually Transmitted Diseases: Epidemiological and Clinical Aspects in Adults. Urol. J. 2014, 81, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Sieving, R.E.; O’Brien, J.R.G.; Saftner, M.A.; Argo, T.A. Sexually Transmitted Diseases Among US Adolescents and Young Adults: Patterns, Clinical Considerations, and Prevention. Nurs. Clin. N. Am. 2019, 54, 207–225. [Google Scholar] [CrossRef] [PubMed]
- Downing-Matibag, T.M.; Geisinger, B. Hooking Up and Sexual Risk Taking Among College Students: A Health Belief Model Perspective. APA PsycNet 2009, 19, 1196–1209. [Google Scholar] [CrossRef]
- Visalli, G.; Cosenza, B.; Mazzu, F.; Bertuccio, M.; Spataro, P.; Pellicanò, G.F.; di Pietro, A.; Picerno, I.; Facciolà, A. Knowledge of sexually transmitted infections and risky behaviours: A survey among high school and university students. J. Prev. Med. Hyg. 2019, 60, E84. [Google Scholar] [CrossRef]
- Xenaki, D.; Plotas, P.; Michail, G.; Poulas, K.; Jelastopulu, E. Knowledge, behaviours and attitudes for human papillomavirus (HPV) prevention among educators and health professionals in Greece. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7745–7752. [Google Scholar] [CrossRef]
- Nikolopoulos, G.K.; Chanos, S.; Tsioptsias, E.; Hodges-Mameletzis, I.; Paraskeva, D.; Dedes, N. HIV incidence among men who have sex with men at a community-based facility in Greece. Cent. Eur. J. Public Health 2019, 27, 54–57. [Google Scholar] [CrossRef] [Green Version]
- Pavlopoulou, I.D.; Dikalioti, S.K.; Gountas, I.; Sypsa, V.; Malliori, M.; Pantavou, K.; Jarlais, D.D.; Nikolopoulos, G.K.; Hatzakis, A. High-risk behaviors and their association with awareness of HIV status among participants of a large-scale prevention intervention in Athens, Greece. BMC Public Health 2020, 20, 105. [Google Scholar] [CrossRef] [PubMed]
- Loumpardia, P.; Bourmpos, K.; Loumpardias, G.A.; Kalampoki, V.; Valasoulis, G.; Valari, O.; Vythoulkasl, D.; Deligeoroglou, E.; Koliopoulos, G. Epidemiological, Clinical, and Virological Characteristics of Women with Genital Warts in Greece—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/26054116/ (accessed on 17 September 2021).
- Folasayo, A.T.; Oluwasegun, A.J.; Samsudin, S.; Saudi, S.N.S.; Osman, M.; Hamat, R.A. Assessing the Knowledge Level, Attitudes, Risky Behaviors and Preventive Practices on Sexually Transmitted Diseases among University Students as Future Healthcare Providers in the Central Zone of Malaysia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2017, 14, 159. [Google Scholar] [CrossRef] [Green Version]
- Gökengin, D.; Yamazhan, T.; Özkaya, D.; Aytuǧ, S.; Ertem, E.; Arda, B.; Serter, D. Sexual Knowledge, Attitudes, and Risk Behaviors of Students in Turkey. J. Sch. Health 2003, 73, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Ekşi, Z.; Kömürcü, N. Knowledge Level of University Students about Sexually Transmitted Diseases. Procedia Soc. Behav. Sci. 2014, 122, 465–472. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, R.X.D.; Evangelista, T.M.; Ii, A.; Xavier, R.; Carvalho, C. Knowledge, attitudes and practices of university adolescents about syphilis: A cross-sectional study in the Northeast. Rev. Saúde Pública 2020. [Google Scholar] [CrossRef]
- Caetano, M.E.; Linhares, I.M.; Pinotti, J.A.; da Fonseca, A.M.; Wojitani, M.D.; Giraldo, P.C. Sexual behavior and knowledge of sexually transmitted infections among university students in Sao Paulo, Brazil. Int. J. Gynecol. Obstet. 2010, 110, 43–46. [Google Scholar] [CrossRef]
- Samkange-Zeeb, F.N.; Spallek, L.; Zeeb, H. Awareness and knowledge of sexually transmitted diseases (STDs) among school-going adolescents in Europe: A systematic review of published literature. BMC Public Health 2011, 11, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Huppert, J.S. Trichomoniasis in teens: An update. Curr. Opin. Obstet. Gynecol. 2009, 21, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.I.; Ji, D.A.; Hung, C.H. Prevalent and Incident HIV Diagnoses among Entamoeba histolytica-Infected Adult Males: A Changing Epidemiology Associated with Sexual Transmission—Taiwan, 2006–2013. PLoS Negl. Trop. Dis. 2014, 8, e3222. [Google Scholar] [CrossRef]
- Trichomoniasis—STI Treatment Guidelines. Available online: https://www.cdc.gov/std/treatment-guidelines/trichomoniasis.htm (accessed on 17 September 2021).
- Goundry, A.L.R.; Finlay, E.R.; Llewellyn, C.D. Talking about links between sexually transmitted infections and infertility with college and university students from SE England, UK: A qualitative study. Reprod. Health 2013, 10, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Duru, O.E.; Yama, D.; Duro, A.A.; Odetola, T.; Danboyi, O.M.; Avidime, K.A. Mohammed, Correlates of socio-demographic variables and attitude to condom use in HIV/AIDS prevention among students in some selected Nigerian Universities. Niger. Med. J. 2020, 61, 316. [Google Scholar] [CrossRef]
- Almeida-Santos, M.A. Condom use and vulnerabilities to sexually transmitted infections in quilombola communities: A descriptive study Condom use in quilombola communities. Epidemiol. Serv. Saudes 2021, 30. [Google Scholar] [CrossRef]
- Zizza, A.; Guido, M.; Recchia, V.; Grima, P.; Banchelli, F.; Tinelli, A. Knowledge, Information Needs and Risk Perception about HIV and Sexually Transmitted Diseases after an Education Intervention on Italian High School and University Students. Int. J. Environ. Res. Public Health 2021, 18, 2069. [Google Scholar] [CrossRef]
- Kanda, L.; Mash, R. Reasons for inconsistent condom use by young adults in Mahalapye, Botswana. Afr. J. Prim. Health Care Fam. Med. 2018, 10, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milic, M.; Gazibara, T.; Stevanovic, J.; Parlic, M.; Nicholson, D.; Mitic, K.; Lazic, D.; Dotlic, J. Patterns of condom use in a university student population residing in a high-risk area for HIV infection. Eur. J. Contracept. Rep. Health Care 2020, 25, 269–278. [Google Scholar] [CrossRef]
- Fasciana, T.; Capra, G.; di Carlo, P.; Calà, C.; Vella, M.; Pistone, G.; Colomba, C.; Giammanco, A. Socio-Demographic Characteristics and Sexual Behavioral Factors of Patients with Sexually Transmitted Infections Attending a Hospital in Southern Italy. Int. J. Environ. Res. Public Health 2021, 18, 4722. [Google Scholar] [CrossRef]
- Samkange-Zeeb, F.; Mikolajczyk, R.T.; Zeeb, H. Awareness and Knowledge of Sexually Transmitted Diseases Among Secondary School Students in Two German Cities. J. Community Health 2012, 38, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Jahanfar, S.; Lye, M.S.; Rampal, L. A randomised controlled trial of peer-adult-led intervention on improvement of knowledge, attitudes and behaviour of university students regarding HIV/AIDS in Malaysia. Orig. Artic. Singap. Med J. 2009, 50, 173. [Google Scholar]
- Vaidakis, D.; Moustaki, I.; Zervas, I.; Barbouni, A.; Merakou, K.; Chrysi, M.S.; Creatsa, G.; Panoskaltsis, T. Knowledge of Greek adolescents on human papilloma virus (HPV) and vaccination, Medicine (United States). Medicine 2017, 96, e5287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okoboi, S.; Castelnuovo, B.; Moore, D.M.; Musaazi, J.; Kambugu, A.; Birungi, J.; Nanfuka, M.; van Rie, A. Incidence rate of sexually transmitted infections among HIV infected patients on long-term ART in an urban and a rural clinic in Uganda. BMC Public Health 2019, 19, 1–8. [Google Scholar] [CrossRef]
- Warner, C.; Carlson, S.; Crichlow, R.; Ross, M.W. Sexual Health Knowledge of U.S. Medical Students: A National Survey. J. Sex. Med. 2018, 15, 1093–1102. [Google Scholar] [CrossRef]
- Bjekic, M.D.; Sipetic-Grujicic, S.B.; Vlajinac, H.D.; Nikolic, A.M. Oral sex related knowledge and oral sex behavior among homosexual and heterosexual men in Belgrade: A cross-sectional study, Indian Journal of Dermatology. Venereol. Leprol. 2018, 84, 563–568. [Google Scholar] [CrossRef]
- Hendry, N.A.; Brown, G.; Dowsett, G.W.; Carman, M. Association between sexually transmissible infection testing, numbers of partners and talking to partners and friends about sexual health: Survey of young adults. Sex. Health 2017, 14, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Masaro, C.L.; Dahinten, V.S.; Johnson, J.; Ogilvie, G.; Patrick, D.M. Perceptions of sexual partner safety, Sexually Transmitted Diseases. Sex Transm. Dis. 2008, 35, 566–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vardavas, C.I.; Kondilis, B.K.; Patelarou, E.; Akrivos, P.D.; Falagas, M.E. Health literacy and sources of health education among adolescents in Greece. Int. J. Adolesc. Med. Health 2009, 21, 179–186. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Age: Mean ± SD (Min–Max) | 21.48 ± 2.88(18–30) |
|---|---|
| Gender: male/female/other n (%) | 449(24.5)/1377(75.10/7(0.4) |
| Education Primary/High School/University, n (%) | 16(0.9)/88(4.8)/1729(94.3) |
| Employment: Full-time/Part-time/Unemployed, n (%) | 281(15.3)/417(22.7)/1135(61.9) |
| Residence: City/Town/Village, n (%) | 1572(85.8)/157(8.6)/104(5.7) |
| Do you have a permanent partner: no/yes, n (%) | 848(46.3)/985(53.7) |
| Sexual preference: Heterosexual/Homosexual/Bisexual, n (%) | 1530(83.5)/86(4.7)/217(11.8) |
| Number of sexual partners to date: Mean ± SD (min–max) | 5.37 ± 10.32(0–250) |
| Age of 1st sexual contact(n = 1322): Mean ± SD (min–max) | 17.41 ± 1.92(10–29) |
| Diseases Classified as STDs | Diseases Causing Genital Cancer | Diseases Causing Infertility | Diseases Transmitted by Oral Contact | |
|---|---|---|---|---|
| WartsHuman papilloma virus (HPV) | 1778 (97.0) | 935 (51.0) | 467 (25.5) | 657 (35.8) |
| Trichomoniasis | 720 (39.3) | 31 (1.7) | 87 (4.8) | 66 (3.6) |
| Hepatitis C | 1089 (59.4) | 147 (8.0) | 169 (9.2) | 264 (14.4) |
| Hepatitis B | 1047 (57.1) | 124 (6.8) | 161 (8.8) | 265 (14.5) |
| Hepatitis A | 575 (31.4) | 54 (2.9) | 75 (4.1) | 135 (7.4) |
| Genital Herpes | 1647 (89.9) | 222 (12.1) | 234 (12.8) | 825 (45.0) |
| Infectious mononucleosis | 292 (15.9) | 20 (1.1) | 57 (3.1) | 235 (12.8) |
| COVID-19 | 57 (3.1) | 5 (0.3) | 7 (0.4) | 100 (5.5) |
| Malaria | 20 (1.1) | 2 (0.1) | 12 (0.7) | 18 (1.0) |
| AIDS (HIV) | 1790 (97.7) | 329 (17.9) | 386 (21.1) | 620 (33.8) |
| Mycoplasmosis | 212 (11.6) | 24 (1.3) | 94 (5.1) | 58 (3.2) |
| Syphilis | 1502 (81.9) | 145 (7.9) | 317 (17.3) | 362 (19.8) |
| Gonorrhea | 1321 (72.1) | 93 (5.1) | 323 (17.6) | 292 (15.9) |
| Amoebiasis | 136 (7.4) | 14 (0.8) | 35 (1.9) | 44 (2.4) |
| Echinococcosis | 135 (7.4) | 15 (0.8) | 40 (2.2) | 32 (1.8) |
| Molluscum contagiosum | 236 (12.9) | 16 (0.9) | 31 (1.7) | 83 (4.5) |
| Chlamydia | 1690 (92.2) | 182 (10.0) | 418 (22.8) | 312 (17.0) |
| Pubic lice | 539 (29.4) | 25 (1.4) | 61 (3.3) | 38 (2.1) |
| Do not know | 792 (43.2) | 953 (52.0) | 553 (30.2) |
| Way of Transmission | The Use of Condoms Protects Against STDs | The Use of Contraceptive Pills Protects Against STDs | |||
|---|---|---|---|---|---|
| Vaginal contact | 1782 (97.2) | No | 1198 (65.4) | Correct | 86 (4.7) |
| Anal contact | 1578 (86.1) | Yes | 545 (29.7) | No | 1544 (84.2) |
| Oral contact | 1406 (76.7) | Do not know | 90 (5.0) | Do not know | 203 (11.1) |
| Blood | 1249 (68.1) | ||||
| Clothing | 166 (9.1) | ||||
| Common utensils | 156 (8.5) | ||||
| Skin contact | 518 (28.3) | ||||
| Do not know | 19 (1.0) | ||||
| In which cases do you not use a condom? | |
| Never | 14 (0.8) |
| Only if partner prefers it | 23 (1.3) |
| In permanent sexual relationships | 512 (27.9) |
| In permanent sexual relationships following testing of a partner for STDs | 499 (27.2) |
| In case of HIV non-detectable seropositive partner | 39 (2.1) |
| In case my partner or I am receiving PrEP treatment | 5 (0.3) |
| Always | 741 (40.4) |
| How often do you test yourself for STDs? | |
| At regular intervals following physical and blood examinations | 194 (10.6) |
| At regular intervals following blood examination | 422 (23.0) |
| Following suspicious sexual activity | 105 (5.7) |
| Following suspicion of STDs due to associated symptoms | 221 (12.1) |
| Never | 891 (48.6) |
| Do you have a previous history of STDs? | |
| Yes (I always notify my partners): | 112 (6.1) |
| Yes (I notify only my permanent partner but not my occasional partners): | 56 (3.1) |
| Yes, without notifying my partners: | 16 (1.0) |
| No | 1.649 (90%) |
| STD Knowledge Score | |||
|---|---|---|---|
| Mean ± SD (%) | p Value | ||
| Gender | Male | 41.09 ± 12.16 | <0.001 |
| Female | 45.84 ± 12.36 | ||
| Education | Primary or High School | 42.33 ± 12.08 | 0.051 |
| University | 44.80 ± 12.52 | ||
| Employment | Unemployed | 44.37 a ±12.52 | <0.001 |
| Part-time | 43.50 a ±11.99 | ||
| Full-time | 47.51 ± 12.81 | ||
| Residence | Town or Village | 43.13 ± 12.92 | 0.039 |
| City | 44.91 ± 12.42 | ||
| Do you have a permanent partner | No | 43.44 ± 12.85 | <0.001 |
| Yes | 45.70 ± 12.12 | ||
| Sexual preference | Heterosexual | 44.32 ± 12.59 | 0.065 |
| Homosexual | 46.64 ± 12.66 | ||
| Bisexual | 46.21 ± 11.71 | ||
| Age | Pearson’s r | r = 0.177 | <0.001 |
| Number of sexual partners to date | r = 0.105 | <0.001 | |
| Reference Category | R2 | Beta ± SE | p-Value | |
|---|---|---|---|---|
| Age | --- | 0.031 | 0.62 ± 0.11 | <0.001 |
| Gender (female) | Male | 0.027 | 4.62 ± 0.66 | <0.001 |
| Education (university) | Primary or High School | 0.002 | 2.39 ± 1.22 | 0.050 |
| Employment (Unemployed, -Part time) | Full time | 0.000 | 0.80 ± 0.87 | 0.420 |
| Residence (town-village) | City | 0.001 | 1.01 ± 0.81 | 0.215 |
| Do you have a permanent partner | No | 0.002 | 1.23 ± 0.58 | 0.035 |
| Sexual preference(Homosexual-Bisexual) | Heterosexual | 0.003 | 1.90 ± 0.77 | 0.014 |
| Number of sexual partners to date | --- | 0.006 | 0.08 ± 0.03 | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voyiatzaki, C.; Venetikou, M.S.; Papageorgiou, E.; Anthouli-Anagnostopoulou, F.; Simitzis, P.; Chaniotis, D.I.; Adamopoulou, M. Awareness, Knowledge and Risky Behaviors of Sexually Transmitted Diseases among Young People in Greece. Int. J. Environ. Res. Public Health 2021, 18, 10022. https://doi.org/10.3390/ijerph181910022
Voyiatzaki C, Venetikou MS, Papageorgiou E, Anthouli-Anagnostopoulou F, Simitzis P, Chaniotis DI, Adamopoulou M. Awareness, Knowledge and Risky Behaviors of Sexually Transmitted Diseases among Young People in Greece. International Journal of Environmental Research and Public Health. 2021; 18(19):10022. https://doi.org/10.3390/ijerph181910022
Chicago/Turabian StyleVoyiatzaki, Chrysa, Maria S. Venetikou, Effie Papageorgiou, Fragiski Anthouli-Anagnostopoulou, Panagiotis Simitzis, Dimitrios I. Chaniotis, and Maria Adamopoulou. 2021. "Awareness, Knowledge and Risky Behaviors of Sexually Transmitted Diseases among Young People in Greece" International Journal of Environmental Research and Public Health 18, no. 19: 10022. https://doi.org/10.3390/ijerph181910022
APA StyleVoyiatzaki, C., Venetikou, M. S., Papageorgiou, E., Anthouli-Anagnostopoulou, F., Simitzis, P., Chaniotis, D. I., & Adamopoulou, M. (2021). Awareness, Knowledge and Risky Behaviors of Sexually Transmitted Diseases among Young People in Greece. International Journal of Environmental Research and Public Health, 18(19), 10022. https://doi.org/10.3390/ijerph181910022