
National Trends and Policy Impacts on Provision of Home Medicines Reviews and Residential Medication Management Reviews in Older Australians, 2009–2019

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Sources
2.2. Statistical Analysis
3. Results
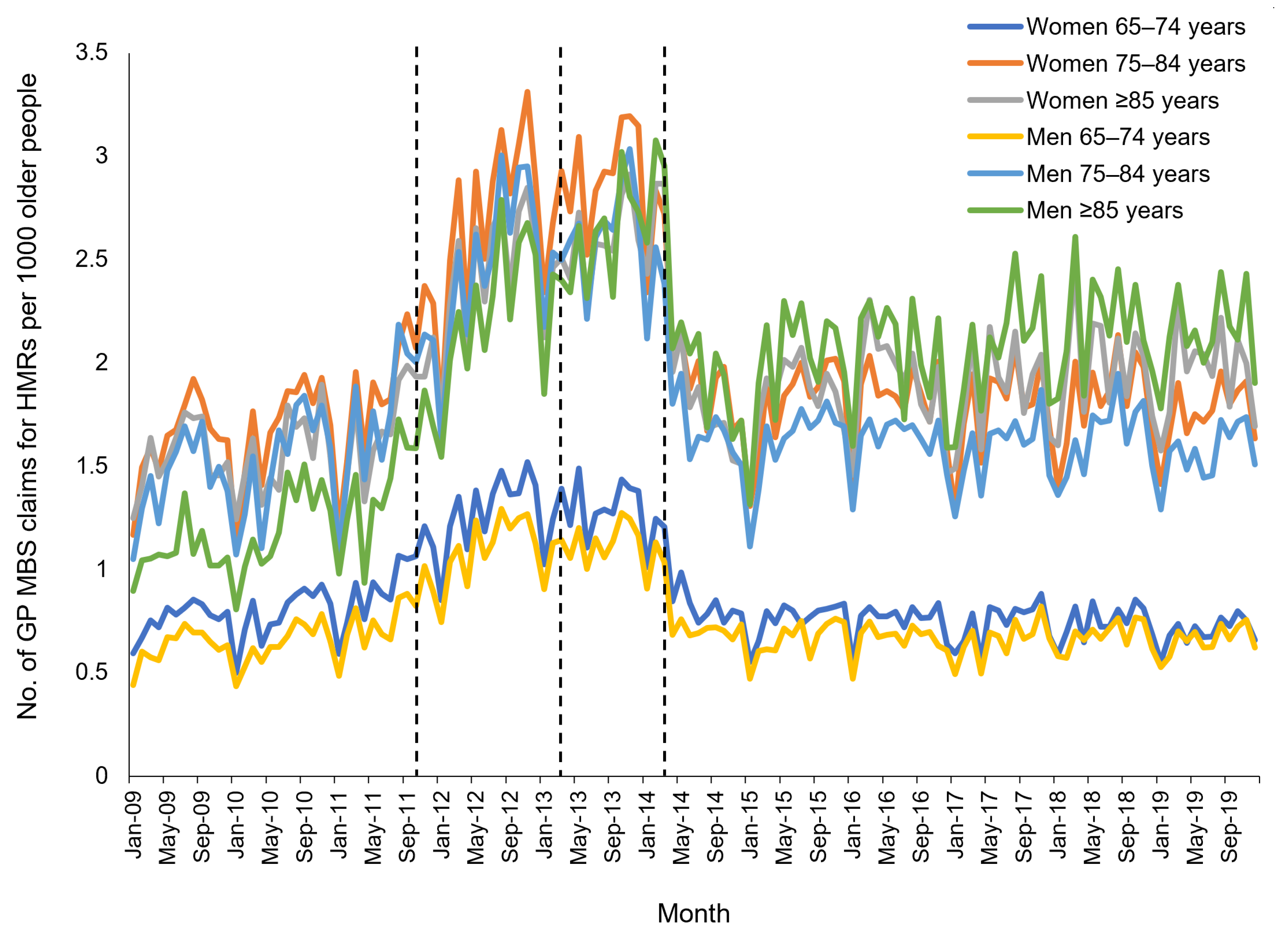
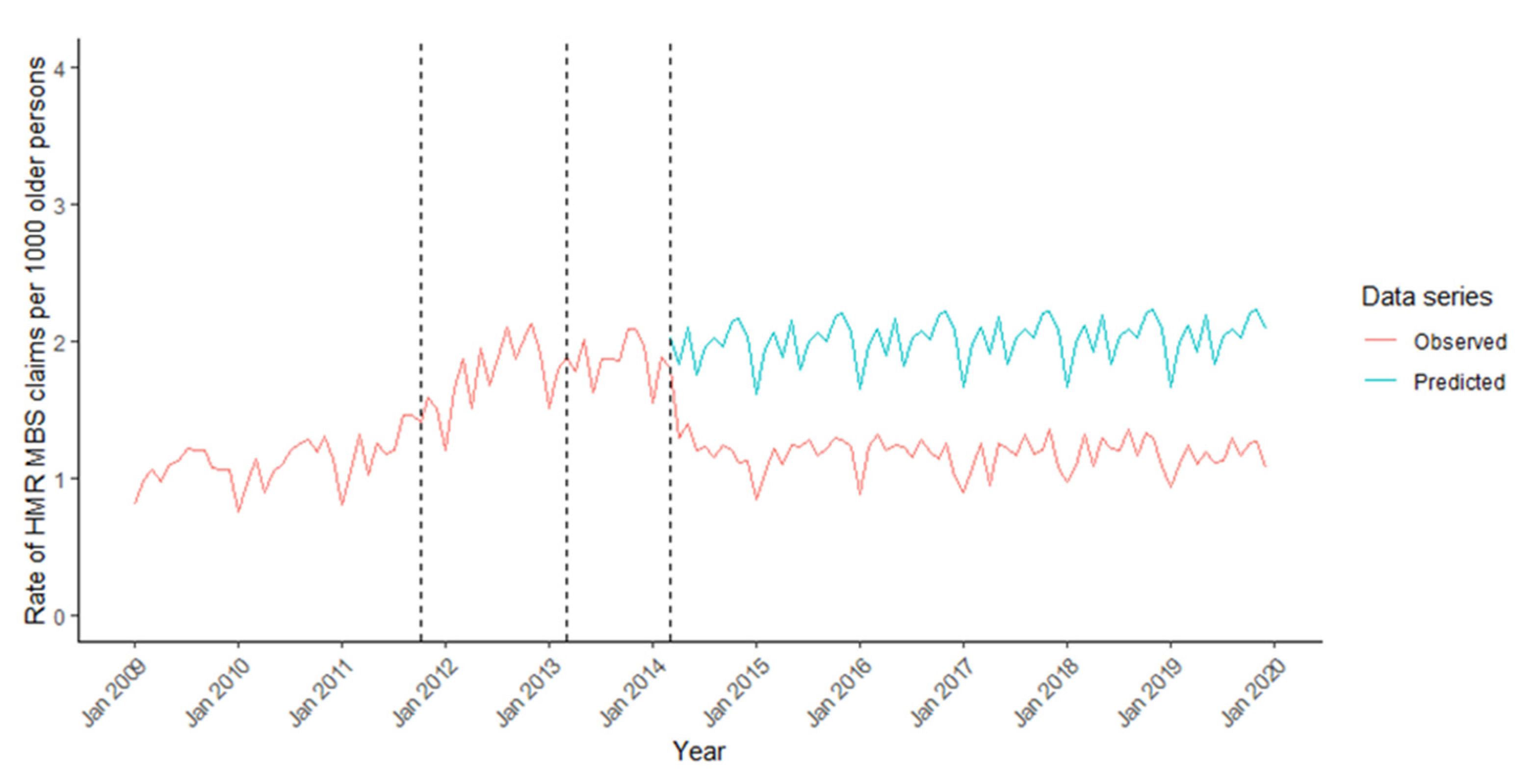
3.1. Impact of Program Changes on HMR Provision
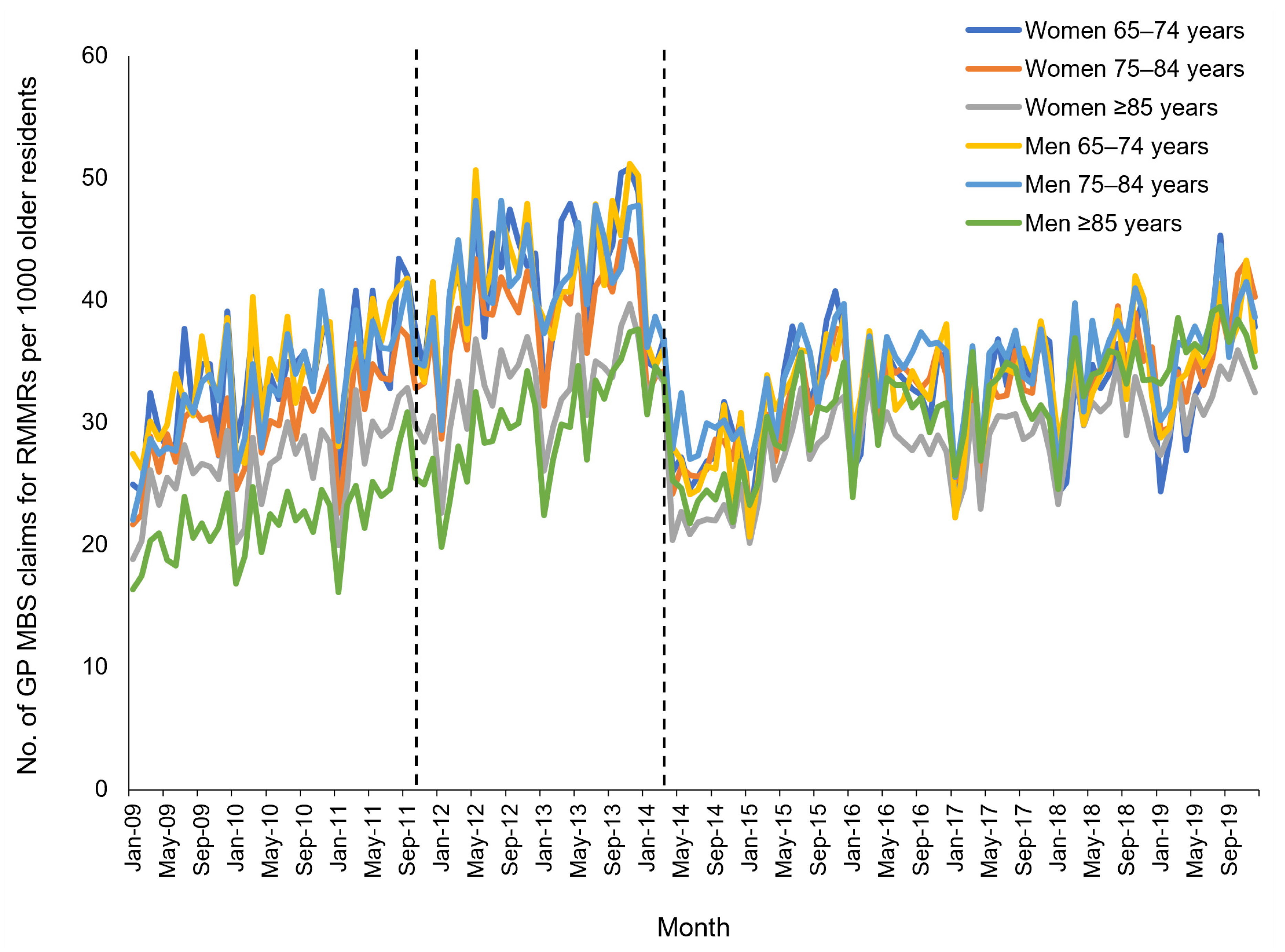
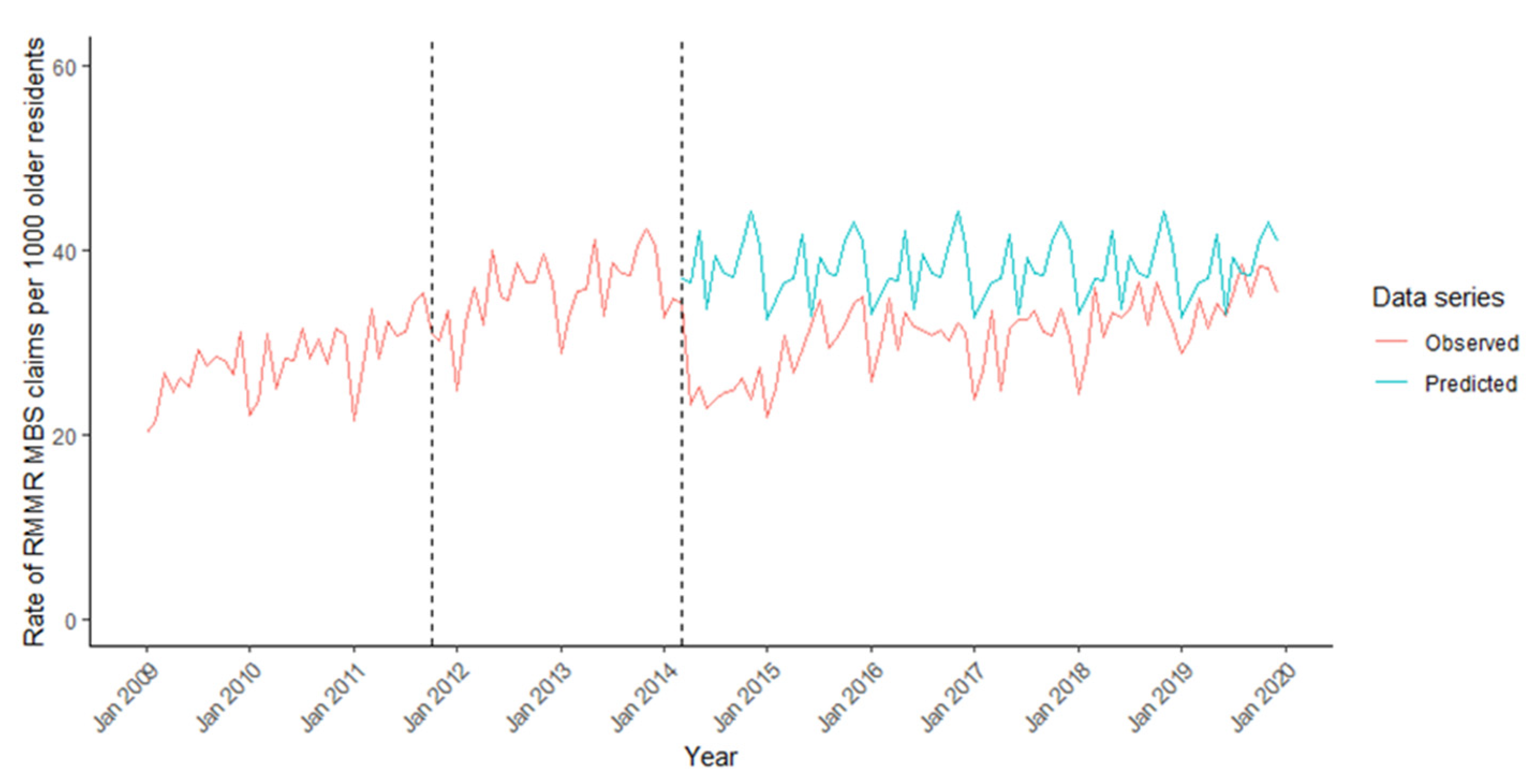
3.2. Impact of Program Changes on RMMR Provision
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pharmaceutical Society of Australia. Medicine Safety: Take Care; PSA: Canberra, Australia, 2019. [Google Scholar]
- Chen, T.F. Pharmacist-Led Home Medicines Review and Residential Medication Management Review: The Australian Model. Drugs Aging 2016, 33, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.Y.H.; Wang, K.N.; Sluggett, J.K.; Ilomäki, J.; Hilmer, S.N.; Corlis, M.; Bell, J.S. Process, impact and outcomes of medication review in Australian residential aged care facilities: A systematic review. Aust. J. Ageing 2019, 38, 9–25. [Google Scholar] [CrossRef]
- Jokanovic, N.; Tan, E.C.K.; van den Bosch, D.; Kirkpatrick, C.M.; Dooley, M.J.; Bell, J.S. Clinical medication review in Australia: A systematic review. Res. Soc. Adm. Pharm. 2016, 12, 384–418. [Google Scholar] [CrossRef]
- Australian Commission on Safety and Quality in Health Care. Medication without Harm-WHO Global Patient Safety Challenge. Australia’s Response; ACSQHC: Sydney, Australia, 2020. [Google Scholar]
- Spinks, J.; Birch, S.; Wheeler, A.J.; Nissen, L.; Freeman, C.; Thai, T.; Byrnes, J. Provision of home medicines reviews in Australia: Linking population need with service provision and available pharmacist workforce. Aust. Health Rev. 2020, 44, 973–982. [Google Scholar] [CrossRef]
- PricewaterhouseCoopers. Combined Review of Fifth Community Pharmacy Agreement Medication Management Programmes: Final Report; PwC Australia: Sydney, Australia, 2015. [Google Scholar]
- HealthConsult Pty Ltd. Initial Evaluation of Sixth Community Pharmacy Agreement Medication Management Programs: Home Medication Review; Final Evaluation Report; HealthConsult Pty Ltd.: Sydney, Australia, 2017. [Google Scholar]
- Royal Commission into Aged Care Quality and Safety. Interim Report: Neglect; Commonwealth of Australia: Canberra, Australia, 2019; Volume 1. [Google Scholar]
- Australian Government Services Australia. Medicare Item Reports; Commonwealth of Australia: Canberra, Australia, 2020. Available online: http://medicarestatistics.humanservices.gov.au/statistics/mbs_item.jsp (accessed on 14 January 2021).
- Australian Bureau of Statistics. National, State and Territory Population; ABS: Canberra, Australia, 2020. Available online: https://www.abs.gov.au/statistics/people/population/national-state-and-territory-population/latest-release (accessed on 14 January 2021).
- Australian Institute of Health and Welfare and Australian Government Department of Health. Aged Care Data Snapshot; AIHW: Canberra, Australia, 2020. Available online: https://www.gen-agedcaredata.gov.au/Resources/Access-data/2020/September/Aged-care-data-snapshot (accessed on 12 August 2021).
- Schaffer, A.L.; Dobbins, T.A.; Pearson, S.-A. Interrupted time series analysis using autoregressive integrated moving average (ARIMA) models: A guide for evaluating large-scale health interventions. BMC Med. Res. Methodol. 2021, 21, 58. [Google Scholar] [CrossRef] [PubMed]
- Sluggett, J.K.; Bell, J.S.; Lang, C.; Corlis, M.; Whitehead, C.; Wesselingh, S.L.; Inacio, M.C. Variation in Provision of Collaborative Medication Reviews on Entry to Long-Term Care Facilities. J. Am. Med. Dir. Assoc. 2021, 22, 148–155.e1. [Google Scholar] [CrossRef]
- Australian Commission on Safety and Quality in Health Care and Australian Institute of Health and Welfare. The Fourth Australian Atlas of Healthcare Variation; ACSQHC: Sydney, Australia, 2021. [Google Scholar]
- Sluggett, J.K.; Bell, J.S.; Lang, C.; Corlis, M.; Whitehead, C.; Wesselingh, S.L.; Inacio, M.C. Residential medication management reviews in Australian residential aged care facilities. Med. J. Aust. 2021, 214, 432–433. [Google Scholar] [CrossRef]
- Du, W.; Gnjidic, D.; Pearson, S.-A.; Hilmer, S.; McLachlan, A.J.; Blyth, F.; Viney, R.; Joshy, G.; Day, C.; Banks, E. Patterns of high-risk prescribing and other factors in relation to receipt of a home medicines review: A prospective cohort investigation among adults aged 45 years and over in Australia. BMJ Open 2019, 9, e027305. [Google Scholar] [CrossRef] [Green Version]
- Kalisch Ellett, L.M.; Pratt, N.L.; Sluggett, J.K.; Ramsay, E.N.; Kerr, M.; LeBlanc, V.T.; Barratt, J.D.; Gilbert, A.L.; Roughead, E.E. Sustaining practice change in health care: The impact of a national quality improvement program on the uptake of collaborative medicines reviews. J. Pharm. Pr. Res. 2018, 48, 222–230. [Google Scholar] [CrossRef]
- Inacio, M.C.; Lang, C.; Bray, S.C.; Visvanathan, R.; Whitehead, C.; Griffith, E.C.; Evans, K.; Corlis, M.; Wesselingh, S. Health Status and Health Care Trends of Individuals Accessing Australian Aged Care Programs Over a Decade: The Registry of Senior Australians (ROSA) Historical Cohort. Intern. Med. J. 2021, 51, 712–724. [Google Scholar] [CrossRef]
- Australian Government Department of Health. Pharmacy Programs Data; Commonwealth of Australia: Canberra, Australia, 2021. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/pharmacy-programs-data (accessed on 12 August 2021).
- Weir, K.R.; Naganathan, V.; Rigby, D.; McCaffery, K.; Bonner, C.; Trevena, L.; McLachlan, A.J.; Jansen, J. Home medicines reviews: A qualitative study of GPs’ experiences. Aust. J. Prim. Health 2020, 26, 24. [Google Scholar] [CrossRef]
- Dhillon, A.K.; Hattingh, H.L.; Stafford, A.; Hoti, K. General practitioners’ perceptions on home medicines reviews: A qualitative analysis. BMC Fam. Pract. 2015, 16, 16. [Google Scholar] [CrossRef] [Green Version]
- Picton, L.; Lalic, S.; Ryan-Atwood, T.E.; Stewart, K.; Kirkpatrick, C.M.; Dooley, M.J.; Turner, J.P.; Bell, J.S. The role of medication advisory committees in residential aged care services. Res. Soc. Adm. Pharm. 2020, 16, 1401–1408. [Google Scholar] [CrossRef]
- Medicare Benefits Schedule Review Taskforce. Taskforce Findings–General Practice and Primary Care Clinical Committee Report; MBS Review–Final taskforce reports, findings and recommendations; Commonwealth of Australia: Canberra, Australia, 2020. [Google Scholar]
- Sawan, M.J.; Jeon, Y.-H.; Fois, R.J.; Chen, T.F. A qualitative study exploring visible components of organizational culture: What influences the use of psychotropic medicines in nursing homes? Int. Psychogeriatr. 2016, 28, 1725–1735. [Google Scholar] [CrossRef]
- McDerby, N.; Bail, K.; Kosari, S.; Shield, A.; Peterson, G.; Dawda, P.; Naunton, M. Canaries in the coalmine: Stakeholder perspectives of medication management reviews for residents with dementia. Res. Soc. Adm. Pharm. 2020, 16, 1220–1227. [Google Scholar] [CrossRef]
- Freeman, C.R.; Scott, I.A.; Hemming, K.; Connelly, L.B.; Kirkpatrick, C.M.; Coombes, I.; Whitty, J.; Martin, J.; Cottrell, N.; Sturman, N.; et al. Reducing Medical Admissions and Presentations Into Hospital through Optimising Medicines (REMAIN HOME): A stepped wedge, cluster randomised controlled trial. Med. J. Aust. 2021, 214, 212–217. [Google Scholar] [CrossRef]
- Elliott, R.A.; Martinac, G.; Campbell, S.; Thorn, J.; Woodward, M.C. Pharmacist-led medication review to identify medication-related problems in older people referred to an Aged Care Assessment Team. Drugs Aging 2012, 29, 593–605. [Google Scholar] [CrossRef]
- McDerby, N.; Kosari, S.; Bail, K.; Shield, A.; Peterson, G.; Naunton, M. The effect of a residential care pharmacist on medication administration practices in aged care: A controlled trial. J. Clin. Pharm. Ther. 2019, 44, 595–602. [Google Scholar] [CrossRef]
- Czarniak, P.; Hattingh, L.; Sim, T.F.; Parsons, R.; Wright, B.; Sunderland, B. Home medicines reviews and residential medication management reviews in Western Australia. Int. J. Clin. Pharm. 2020, 42, 567–578. [Google Scholar] [CrossRef]
- Australian Government Department of Health. 2018–2019 Report on the Operation of the Aged Care Act 1997; Commonwealth of Australia: Canberra, Australia, 2019.
- Cations, M.; Lang, C.; Crotty, M.; Wesselingh, S.; Whitehead, C.; Inacio, M.C. Factors associated with success in transition care services among older people in Australia. BMC Geriatr. 2020, 20, 496. [Google Scholar] [CrossRef]
- Hillen, J.B.; Soulsby, N.; Clarke, M. Too many pills, too many sick older Australians: Working together is key. Aust. J. Gen. Pract. 2021, 50, 171–174. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Home Medicines Review (HMR) | Residential Medication Management Review (RMMR) |
|---|---|
| Prior to October 2011 | |
|
|
| October 20111 | |
|
|
| 15 March 2013 | |
| |
| 1 March 2014 | |
|
|
| 1 July 20182 | |
|
|
| Month of Program Change. | Type of Change 1,2 | Estimate (95% CI) | p-Value |
|---|---|---|---|
| Home Medicines Reviews | |||
| October 2011 | Step | −0.01 (−0.20, 0.18) | 0.90 |
| Ramp | 0.03 (0.01, 0.06) | 0.04 | |
| March 2013 | Step | 0.04 (−0.16, 0.23) | 0.72 |
| Ramp | −0.03 (−0.09, 0.04) | 0.42 | |
| March 2014 | Step | −0.32 (−0.52, −0.11) | <0.01 |
| Ramp | −0.01 (−0.06, 0.04) | 0.70 | |
| Residential Medication Management Reviews | |||
| October 2011 | Step | −0.54 (−3.30, 2.23) | 0.70 |
| Ramp | 0.05 (−0.12, 0.21) | 0.58 | |
| March 2014 | Step | −12.80 (−15.22, −10.37) | <0.01 |
| Ramp | −0.15 (−0.27, −0.02) | 0.02 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sluggett, J.K.; Collier, L.R.; Bartholomaeus, J.D.; Inacio, M.C.; Wesselingh, S.L.; Caughey, G.E. National Trends and Policy Impacts on Provision of Home Medicines Reviews and Residential Medication Management Reviews in Older Australians, 2009–2019. Int. J. Environ. Res. Public Health 2021, 18, 9898. https://doi.org/10.3390/ijerph18189898
Sluggett JK, Collier LR, Bartholomaeus JD, Inacio MC, Wesselingh SL, Caughey GE. National Trends and Policy Impacts on Provision of Home Medicines Reviews and Residential Medication Management Reviews in Older Australians, 2009–2019. International Journal of Environmental Research and Public Health. 2021; 18(18):9898. https://doi.org/10.3390/ijerph18189898
Chicago/Turabian StyleSluggett, Janet K., Luke R. Collier, Jonathan D. Bartholomaeus, Maria C. Inacio, Steve L. Wesselingh, and Gillian E. Caughey. 2021. "National Trends and Policy Impacts on Provision of Home Medicines Reviews and Residential Medication Management Reviews in Older Australians, 2009–2019" International Journal of Environmental Research and Public Health 18, no. 18: 9898. https://doi.org/10.3390/ijerph18189898
APA StyleSluggett, J. K., Collier, L. R., Bartholomaeus, J. D., Inacio, M. C., Wesselingh, S. L., & Caughey, G. E. (2021). National Trends and Policy Impacts on Provision of Home Medicines Reviews and Residential Medication Management Reviews in Older Australians, 2009–2019. International Journal of Environmental Research and Public Health, 18(18), 9898. https://doi.org/10.3390/ijerph18189898