

Healthcare Professionals’ Perspectives of Patients’ Experiences of the Self-Management of Type 2 Diabetes in the Rural Areas of Pakistan: A Qualitative Analysis



Abstract
:1. Introduction
2. Methods
2.1. Qualitative Design
- What are the differences between physician and patient understandings of self-management of type 2 diabetes in the rural area of Pakistan?
- What factors affect diabetes self-management practices?
2.2. Sample and Recruitment
2.3. Consent to Participate
2.4. Data Collection
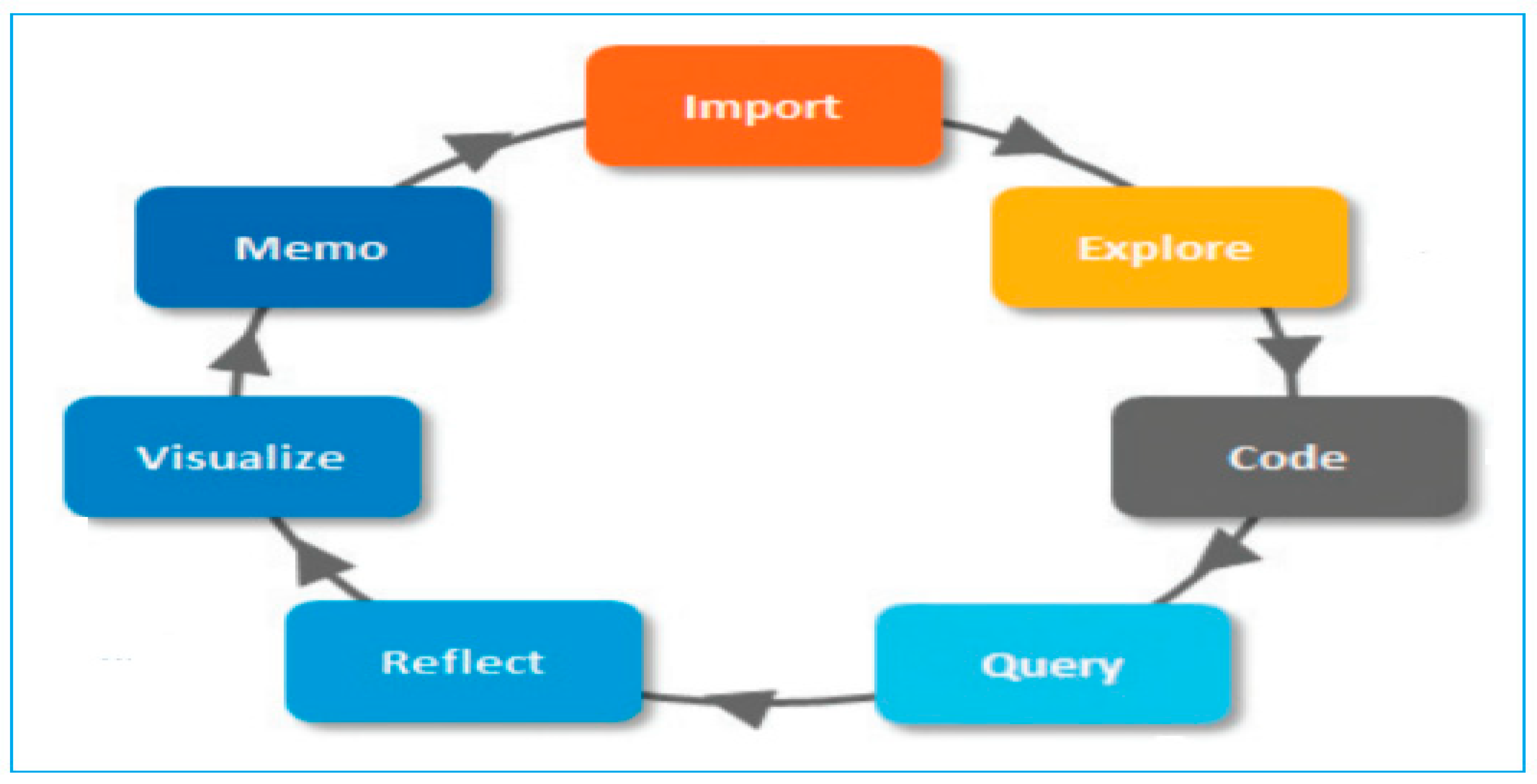
2.5. Qualitative Data Analysis
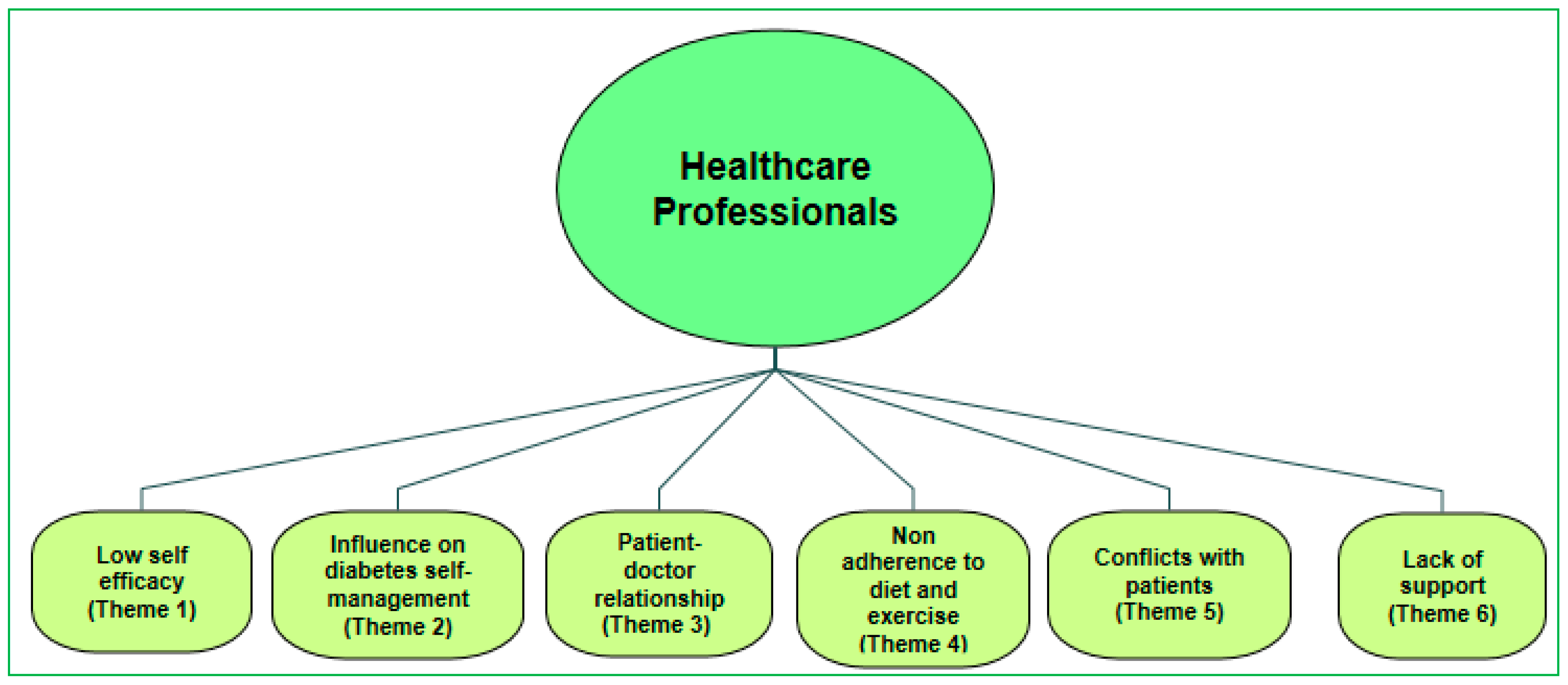
3. Results
3.1. Low Self-Efficacy
“I consider the non-compliance of patients to the advice given to them as a rude behaviour on their part”. “I came to this part of the country with great enthusiasm to help this under-served population and then feel frustrated when realize that I am talking to the walls and then the enthusiasm for putting the patient on the right track diminishes with the time.”(GP-1)
“I always asked them to follow the GP’s advice but patients lack of follow-up of GP’s advice all the time frustrated me”(Nurse-2)
“I have told patients, in case they have any problems in managing their diabetes or they face any problem or need any clarifications, just call me and I will help them out even after working hours.”(GP-5)
“I have received a call from the patient that he has a problem controlling his sugar level in the morning (fasting glucose level > 140 mg/dl). I advised him to have light meals in the night, take prescribed medicines, walk for 30 minutes and have at least 3 hours gap between the food and sleep and that worked very well for the patient.”(GP-8)
“After couple of days, the patient sent me a message on my mobile thanking me for the help and advice. I think that kind of communication may bridge the gap of misunderstanding between the patient and doctor.”(GP-8)
“I always discussed a lot with the patients about their self-management activities and encouraged them to continue or make more efforts – that way patients are encouraged and felt that they are taken care of the clinical staff.”(Nurse-3)
3.2. Influence on Diabetes Self-Management Activities
“Women in this rural area of Pakistan had a difficult time in managing their diabetes as compared to men. In this society, women cook the food according to the choices of the family–women don’t have much to say on the choice of the food, so they have no idea how to manage their diabetes in the environment they live and in relation to the healthy food choices.”(GP-6)
“In Pakistani culture, if unhealthy food is served in parties on a special occasion, it is considered rude not to eat that and bringing diabetes–appropriate food to such events would not be accepted.”(Nurse-4)
“Religious belief plays an important role in this population. Some patients considered that this disease came from “Allah” (God), so Allah will cure that as well so no need to make efforts on self-management activities.”(GP-10)
“One of the nurses mentioned that patients are reluctant to follow the strict diet and want to enjoy the food of their choices.”(Nurse-5)
“There is a need to promote self-monitoring behaviour and health education for the patients as these patients do not understand the complications of the disease and how to care for themselves.”(GP-9)
“I think that diabetes self-care education can play an important role for this population as there is a complete lack of knowledge about this disease among these patients.”(Nurse-6)
3.3. Patient-Doctor Relationship
“I have provided clear direction how to use the medicines and follow up the healthy diet and exercise to my patients but it was of no use as the patients did not follow my advice. In fact, patients complained that there was no control on blood sugar and indicated that their health further deteriorated.”(GP-10)
“The patients do not follow my suggestions, and hence, they decided not to adhere to dietary and behavioural recommendations.”(GP-10)
“…. Many patients in Pakistan are using traditional medicines and sometime their side effects make them more sick blaming the general practitioners for not looking after their health well.”(GP-7)
3.4. Non-Adherence to Diet and Exercise
“There is no diet and exercise consideration—patients with diabetes eat whatever is cooked at home for the family. Physical activity is non-existent as they don’t have proper facilities in this area where they can safely do the physical activities.”(GP-1)
3.5. Conflicts with Patients
“In Pakistani society, food is considered a very important factor which unites people and keeps them together. Many patients with type 2 diabetes in Pakistan eat whatever is presented to them in parties, so the doctor’s advice is not followed.”(GP-2)
“This type of behaviour always results in a conflict with the patients.”(GP-3)
3.6. Lack of Support
“Patients don’t get any support from the family members to manage their diabetes. It was hard for them to cook diabetes “health-food” which may be separate from the rest of the extended family members living together.”(Nurse-7)
“I feel like giving up my efforts as there is no way I can convince these patients about the complications of diabetes and make them understand the benefits of self-management of diabetes.”(GP-2)
4. Discussion
5. Conclusions
6. Practice Implication
- This study is the first of its kind to explore the healthcare professionals’ perspectives of type 2 diabetes mellitus patients in the middle-aged population of Pakistan.
- The article highlighted the ways type 2 diabetes is managed in Pakistan.
- This article will help to minimize the gap between patient–doctor relationships and to achieve optimal glycaemic control and medication adherence.
- Healthcare professionals to set achievable management and self-management goals.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
Appendix A
- Please tell me about the barriers to self-management in patients? Are there any issues related to?
- Human resources and the availability of trained staff
- Funding for clinical consultations, medicines and other public health services
- Cultural/religious barriers which might prevent people from seeking care
- To what extent do diabetic patients use existing services?
- What is your experience of under-usage?
- What is your experience of over-usage?
- What is the effect of the service usage patterns you have mentioned?[Prompt: relevant to self-management]
- To what extent does culture influence patients’ access to health care?
- What in particular influences the Pakistani communities?
- Can you give me an example specific to the Pakistani communities?
- Many people in Pakistan with chronic illness like diabetes often report seeking traditional medicines. What do you think about that? Are there any issues related to?
- Reported effect of these treatments
- Self-medication
- Side-effects reported from the treatment
- How do patients respond to the treatments you might prescribe? Are there any issues related to?
- Reported effect of the treatment
- Self-medication
- Non-compliance
- Side-effects reported from the treatment
- Thinking about the issues raised in the earlier discussions, what could be done to address or overcome these issues?
- What do you think would improve diabetes care of patients with type 2 diabetes?[Prompt: what impacts would more self-management have?]
- What could be done in your profession to improve things?
- What sort of things need to be done more broadly to improve service for people with diabetes?
- Are there any other issues that you want to raise that we have not discussed about management of diabetes?
References
- Bukhsh, A.; Khan, T.M.; Nawaz, M.S.; Sajjad, H.; Chan, K.G.; Lee, L.-H.; Goh, B.-H. Association of diabetes-related self-care activities with glycemic control of patients with type 2 diabetes in Pakistan. Patient Prefer. Adherence 2018, 12, 2377–2385. [Google Scholar] [CrossRef] [Green Version]
- Almutairi, N.; Hosseinzadeh, H.; Gopaldasani, V. The effectiveness of patient activationintervention on type 2 diabetes mellitus glycemic controland slef-management behaviors: A systematic review of RCTs. Prim. Care Diabetes 2020, 14, 12–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, M.H.; Auerbach, S.B.; Harrison, J.F.; Koppert, J.; Jin, L.; Thiel, F.; Karrison, T.G.; Harrand, A.G.; Schaefer, C.T.; Takashima, H.T.; et al. Quality of diabetes care in community health centres. Am. J. Public Health 2000, 90, 431–434. [Google Scholar] [PubMed] [Green Version]
- Mensing, C.; Boucher, J.; Cypress, M.; Weinger, K.; Mulcahy, K.; Barta, P.; Hosey, G.; Kopher, W.; Lasichak, A.; Lamb, B.; et al. National standards for diabetes self-management education. Diabetes Care 2007, 29, S96–S103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norris, S.L.; Lau, J.; Smith, S.J.; Schmid, C.; Engelgau, M.M. Self-management education for adults with type 2 diabetes: A meta-analysis of the effect on glycemic control. Diabetes Care 2002, 25, 1159–1171. [Google Scholar] [CrossRef] [Green Version]
- Hosseinzadeh, H.; Verma, I.; Gopaldasani, V. Patient activation and type 2 diabetes mellitus self-management: A systematic review and meta-analysis. Aust. J. Prim. Health 2020, 26, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Fisher, E.B.; Brownson, C.A.; O’Toole, M.L.; Shetty, G.; Anwuri, V.V.; Glasgow, R.E. Ecological approaches to self-management: The case of diabetes. Am. J. Public Health 2005, 95, 1523–1535. [Google Scholar] [CrossRef]
- Ansari, R.M. Effect of physical activity and obesity on type 2 diabetes in the middle-aged population. J. Environ. Public Health 2009, 2009, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Freeman, J.; Loewe, R. Barriers to communication about diabetes mellitus. Patients’ and practitioners’ different views of the disease. J. Fam. Pract. 2000, 49, 507–512. [Google Scholar]
- Nicknami, M.; Mirbalouchzehi, A.; Zareban, I.; Kalkalinia, E.; Rikhtgarha, G.; Hosseinzadeh, H. Association of health literacy with type 2 diabetes self-management and clinical outcomes within the primary care settings of Iran. Aust. J. Prim. Health 2020, 26, 431–442. [Google Scholar] [CrossRef]
- Wollny, A.; Pentzek, M.; Herber, O.R.; Abholz, H.-H.; Der Schmitten, J.I.; Icks, A.; Wilm, S.; Gummersbach, E. General Practitioners’ attitudes towards patients with poorly controlled type 2 diabetes: A qualitative study. BMC Fam. Pract. 2018, 19, 49. [Google Scholar] [CrossRef] [Green Version]
- Street, R.L., Jr.; Gordon, H.; Haidet, P. Practitioners’ communication and perceptions of patients: Is it how they look, how they talk, or is it just the doctor? Soc. Sci. Med. 2007, 65, 586–598. [Google Scholar] [CrossRef] [Green Version]
- Ghafranipour, F.; Ghaffarifar, S.; Ahmadi, F.; Hosseinzadeh, H.; Akbarzadeh, A. Improving interns’ patient-physician communication skills: Application of self-efficacy theory, a pilot study. Cogent Psychol. 2018, 5, 1524083. [Google Scholar] [CrossRef]
- Wagner, E.H.; Austin, B.T.; Von Korff, M. Organizing care for patients with chronic illness. Milbank Q. 1996, 74, 511–544. [Google Scholar] [CrossRef]
- Macfarlane, A.; Kelleher, D. Concepts of illness causation and attitudes to health care among older people in the Republic of Ireland. Soc. Sci. Med. 2002, 54, 1389–1400. [Google Scholar] [CrossRef] [Green Version]
- Beverly, E.A.; Wray, L.A.; LaCoe, C.L.; Gabbay, R.A. Listening to older adults’ values and preferences for type 2 diabetes care: A qualitative study. Diabetes Spectr. 2014, 27, 44–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Clinical practice recommendations. Diabetes Care 2000, 23 (Suppl. 1), S1–S116. [Google Scholar]
- Khalid, G.H.A.; Pirkani, G.S. Level of health education in patients with type 2 diabetes mellitus in Quetta. J. Pak. Med. Assoc. 1998, 48, 334–336. [Google Scholar]
- Jabbar, A.; Contractor, Z.; Ebrahim, M.A.; Mahmood, K. Standard of knowledge about their disease among patients with diabetes in Karachi, Pakistan. J. Pak. Med. Assoc. 2001, 51, 216. [Google Scholar] [PubMed]
- Shera, A.S.; Jawad, F.; Basit, A. Diabetes related knowledge, attitude and practices of family physicians in Pakistan. J. Pak. Med. Assoc. 2002, 52, 465–470. [Google Scholar]
- Hasan, Z.U.; Zia, S.; Maracy, M. Baseline disease knowledge assessment in patients with type 2 diabetes in a rural area of northwest of Pakistan. J. Pak. Med. Assoc. 2000, 54, 67–73. [Google Scholar]
- Adil, M.M.; Alam, A.Y.; Jeffery, T. Knowledge of type 2 diabetes patients about their illness: A pilot project. J. Med. Assoc. 2005, 55, 221–224. [Google Scholar]
- Sabri, A.A.; Qayyum, M.A.; Saigol, N.U.; Zafar, K.; Aslam, F. Comparing knowledge of diabetes mellitus among rural and urban diabetics. McGill J. Med. 2007, 10, 87–89. [Google Scholar]
- Ulvi, O.S.; Chaudhary, R.Y.; Ali, T.; Alvi, R.A.; Khan, M.F.A.; Khan, M.; Malik, F.A.; Mushtaq, M.; Sarwar, A.; Shahid, T.; et al. Investigating the awareness level about diabetes mellitus and associated factors in rural Islamabad. J. Pak. Med. Assoc. 2009, 59, 798–801. [Google Scholar] [PubMed]
- Afridi, M.A.; Khan, M.N. Role of health education in the management of diabetes mellitus. J. Coll. Physicians Surg. Pak. 2003, 13, 558–561. [Google Scholar] [PubMed]
- Edwards, J.; Hosseinzadeh, H. The impact of structured physical activity on glycemic control in diabetes prevention programmes: A systematic review. Process. Singap. Healthc. 2018, 27, 193–204. [Google Scholar] [CrossRef]
- Brewer-Lowry, A.N.; Arcury, T.A.; Bell, R.A.; Quandt, S.A. Differentiating approaches to diabetes self-management of multi-ethnic rural older adults at the extremes of glycemic control. Gerontologist 2010, 50, 657–667. [Google Scholar] [CrossRef] [Green Version]
- Ansari, R.M.; Hosseinzadeh, H.; Zwar, N. Exploring the qualitative research on diabetes self-management in middle-aged population of rural area of Pakistan. Int. J. Public Health Epidemiol. 2016, 5, 285–291. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Ansari, R.M.; Hosseinzadeh, H.; Harris, M.; Zwar, N. Conceptual Model of Diabetes Self-Management for Middle-Aged Population of Rural Area of Pakistan. Int. J. Diabetes Res. 2017, 6, 68–72. [Google Scholar]
- Rafique, G.; Shaikh, F. Identifying needs and barriers to diabetes education in patients with diabetes. J. Pak. Med. Assoc. 2000, 56, 347–352. [Google Scholar]
- Creswell, J. Qualitative Inquiry and Research Design: Choosing among Five Traditions; Sage: Thousand Oak, CA, USA, 2007. [Google Scholar]
- Robinson, O.C.; Wright, G.R.T.; Smith, J.A. The holistic phase model of early adult crisis. J. Adult Dev. 2013, 20, 27–37. [Google Scholar] [CrossRef]
- QSR International NVivo 11 Pro. Qualitative Data Analysis Software, 2018 [Software]. Available online: https://qsrinternational.com/nvivo/nvivo-products/ (accessed on 11 August 2020).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Howitt, D.; Cramer, D. Thematic Analysis: Introduction to Qualitative Methods in Psychology; Pearson: London, UK, 2010; pp. 163–186. [Google Scholar]
- Meyrick, J. A first step towards a comprehensive approach to judging rigor/quality. J. Health Psychol. 2006, 11, 799–808. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.; Parker, N. Unsatisfactory saturation: A critical exploration of the notion of saturated sample sizes in qualitative research. Qual. Res. J. 2012, 13, 190–197. [Google Scholar] [CrossRef]
- Khawaja, K.; Waheed, H. Self-glucose monitoring and glycemic control at a tertiary care University Hospital Karachi, Pakistan. J. Pak. Med. Assoc. 2010, 60, 1035–1038. [Google Scholar]
- Pakistan Medical Research Council. National Health Survey of Pakistan. Health Profile of the People of Pakistan, 1990–1994; Pakistan Medical Research Council: Islamabad, Pakistan, 1998. [Google Scholar]
- Wens, J.; Vermeire, E.; Van Royen, P.; Sabbe, B.; Denekens, J. GP’s perspectives of type 2 diabetes patients’ adherence to treatment: A qualitative analysis of barriers and solutions. BMC Fam. Pract. 2005, 6, 20. [Google Scholar] [CrossRef] [Green Version]
- Heisler, M.; Vijan, S.; Anderson, R.M.; Ubel, P.A.; Bernstein, S.J.; Hofer, T.P. When do patients and their practitioners agree on diabetes treatment goals and strategies, and what difference does it make? J. Gen. Intern. Med. 2003, 18, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Jeavons, D.; Hungin, A.P.S.; Cornford, C.S. Patients with poorly controlled diabetes in primary care: Healthcare clinicians’ beliefs and attitudes. Postgrad. Med. J. 2006, 82, 347–350. [Google Scholar] [CrossRef] [Green Version]
- Beverly, E.; Hultgren, B.; Brooks, K.M.; Ritholz, M.D.; Abrahamson, M.J.; Weinger, K. Understanding physicians’ challenges when treating type 2 diabetic patients’ social and emotional difficulties. Diabetes Care 2011, 34, 1086–1088. [Google Scholar] [CrossRef] [Green Version]
- Ansari, R.M.; Hosseinzadeh, H.; Harris, M.; Zwar, N. Self-management experiences among middle-aged population of rural area of Pakistan with type 2 diabetes: A qualitative analysis. Clin. Epidemiol. Glob. Health 2019, 7, 177–183. [Google Scholar] [CrossRef] [Green Version]
- Rehan, S.; Naz, H. Diabetes Self-care and Diabetes stress in patients with type 2 diabetes. Pak. J. Prof. Psychol. 2015, 6, 61–73. [Google Scholar]
- Whittemore, R.; Chase, S.; Mandle, C.L.; Roy, S.C. The content, integrity, and efficacy of a nurse coaching intervention in type 2 diabetes. Diabetes Educ. 2001, 27, 887–898. [Google Scholar] [CrossRef]
- Lawton, J.; Ahmad, N.; Hanna, L.; Douglas, M.; Hallowell, N. “I Can’t Do Any Serious Exercise”: Barriers to Physical Activity Amongst People of Pakistani and Indian Origin with Type 2 Diabetes. Health Educ. Res. 2006, 21, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Broom, D.; Whittaker, A. Controlling diabetes: Moral language in the management of diabetes type 2. Soc. Sci. Med. 2004, 58, 2371–2382. [Google Scholar] [CrossRef] [PubMed]
- Feudtner, C. Bittersweet: Diabetes, Insulin and Transformation of Illness; University of North Caroline Press: Chapel Hill, NC, USA, 2003. [Google Scholar]
- Glasgow, R.E.; Toobert, D.J.; Gillette, C.D. Psychosocial barriers to diabetes self-management and quality of life. Diabetes Spectrum 2001, 14, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Brown, S.A.; Hedges, L.V. Predicting Metabolic Control in Diabetes: A Pilot Study Using Meta-Analysis to Estimate a Linear Model. Nurs. Res. 1994, 43, 362–368. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic | GPs (n = 10) | Nurses (n = 10) | Total (n = 20) |
|---|---|---|---|
| Age (average, in years) | 48 | 50 | 49 |
| Marital Status | |||
| Single/never married | 0 | 1 | 1 |
| Married | 10 | 9 | 19 |
| Separated/divorced | 0 | 0 | 0 |
| Education | |||
| Completed college or university | 10 | 10 | 20 |
| Professional degree (MBBS/MD) | 10 | 0 | 10 |
| Specialization (MRCGP/MRCP) | 4 | 0 | 4 |
| Employment | |||
| Full/part-time | 10 | 10 | 20 |
| Unemployed | 0 | 0 | 0 |
| Years in Practice (mean) | 16 | 18 | 17 |
| Family Background | |||
| Languages spoken at home | Urdu/Punjabi Pushto | Urdu/Punjabi Pushto | - |
| Cultural Background | Mohajir/Punjabi and Pathan | Mohajir/Punjabi and Pathan | - |
| Themes | GP’s (Feelings) | Nurses (Feelings) |
|---|---|---|
| Low self-efficacy | Personally affected by conflicts with the patients | Lack of follow-up by patients frustrating |
| Influence on diabetes self-management activities | Social and cultural barriers | Barriers from: joint family, religious |
| Patient–doctor relationship | Conflict with the patients | More expectations from patients |
| Non-adherence to diet and exercise | Patients do not follow instructions | Difficulties to follow-up instructions |
| Conflicts with patients | Patients do not listen to advice | Patients poor attitude |
| Lack of support | No support from the Healthcare providers No Social support | Less support from family |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ansari, R.M.; Harris, M.; Hosseinzadeh, H.; Zwar, N. Healthcare Professionals’ Perspectives of Patients’ Experiences of the Self-Management of Type 2 Diabetes in the Rural Areas of Pakistan: A Qualitative Analysis. Int. J. Environ. Res. Public Health 2021, 18, 9869. https://doi.org/10.3390/ijerph18189869
Ansari RM, Harris M, Hosseinzadeh H, Zwar N. Healthcare Professionals’ Perspectives of Patients’ Experiences of the Self-Management of Type 2 Diabetes in the Rural Areas of Pakistan: A Qualitative Analysis. International Journal of Environmental Research and Public Health. 2021; 18(18):9869. https://doi.org/10.3390/ijerph18189869
Chicago/Turabian StyleAnsari, Rashid M., Mark Harris, Hassan Hosseinzadeh, and Nicholas Zwar. 2021. "Healthcare Professionals’ Perspectives of Patients’ Experiences of the Self-Management of Type 2 Diabetes in the Rural Areas of Pakistan: A Qualitative Analysis" International Journal of Environmental Research and Public Health 18, no. 18: 9869. https://doi.org/10.3390/ijerph18189869
APA StyleAnsari, R. M., Harris, M., Hosseinzadeh, H., & Zwar, N. (2021). Healthcare Professionals’ Perspectives of Patients’ Experiences of the Self-Management of Type 2 Diabetes in the Rural Areas of Pakistan: A Qualitative Analysis. International Journal of Environmental Research and Public Health, 18(18), 9869. https://doi.org/10.3390/ijerph18189869