
Characteristics of Home-Visit Nursing Agencies That Closed after the 2012 Fee Revision for Home-Visit Nursing Services: A Nationwide Panel Data Analysis in Japan


Abstract
1. Introduction
2. Materials and Methods
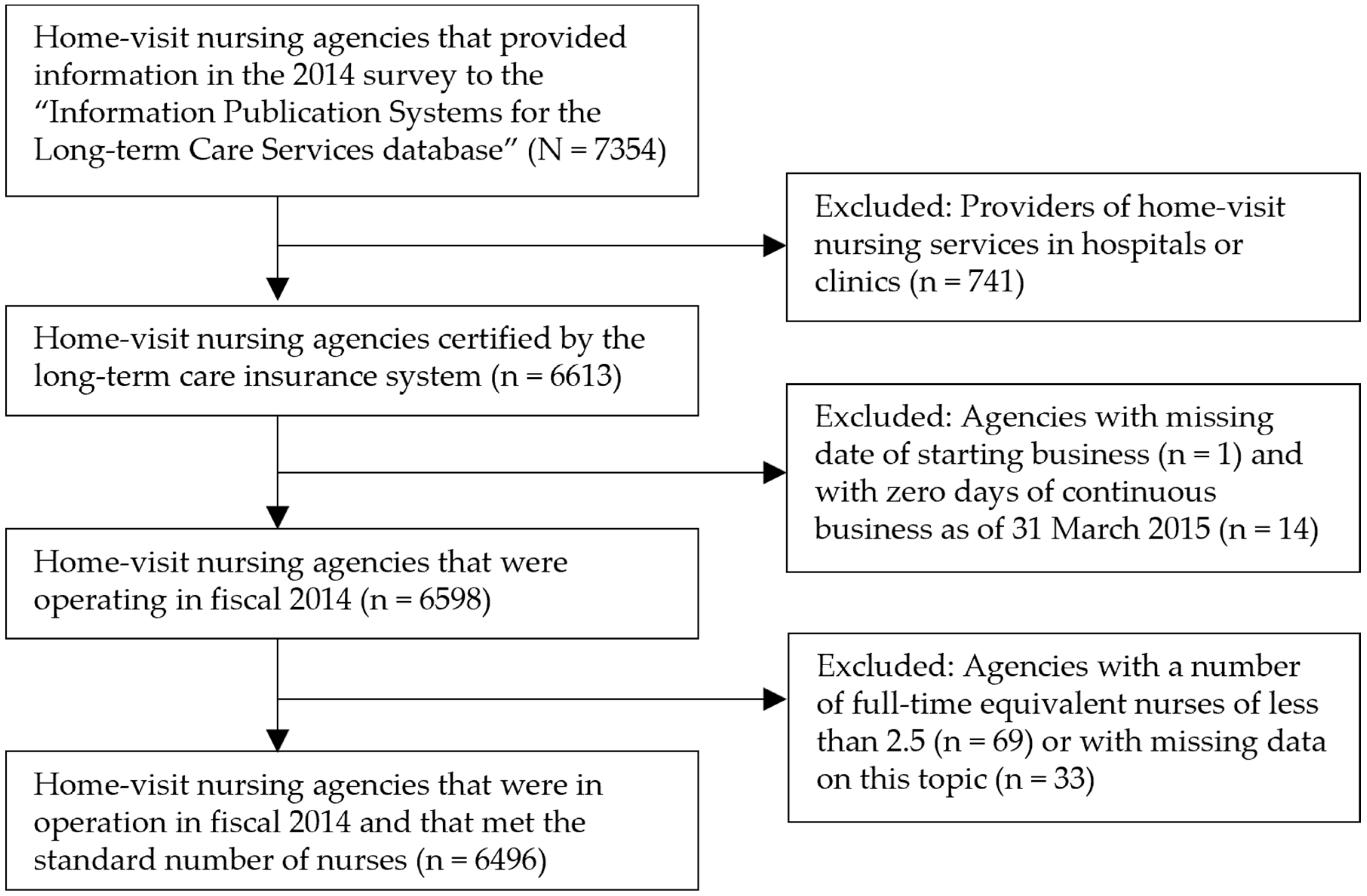
2.1. Design and Data Collection
2.2. Measurements
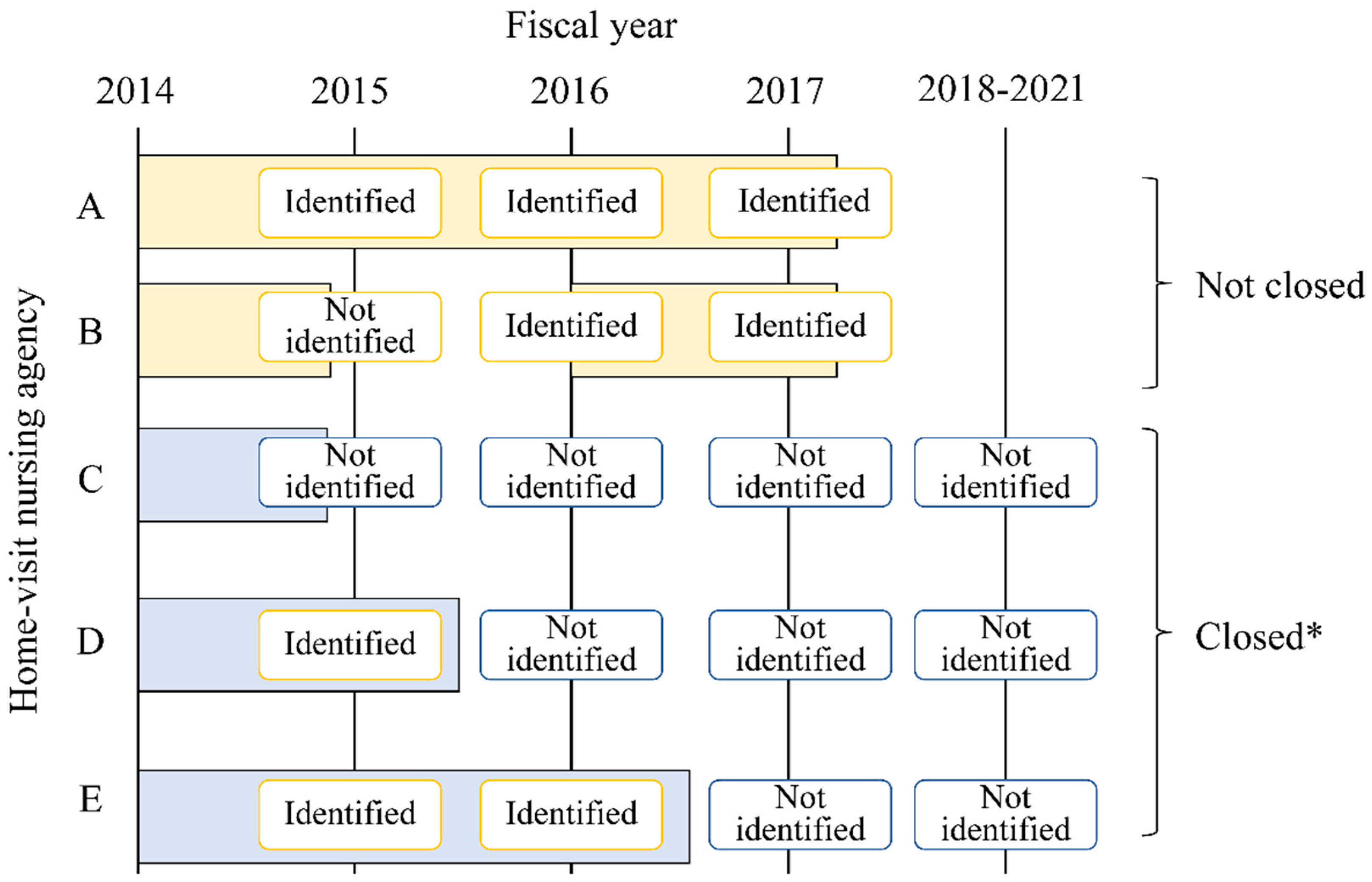
2.2.1. Dependent Variables
2.2.2. Independent Variables
A. Regional Factors
B. Organizational Factors
2.3. Statistical Analysis
3. Results
3.1. Basic Characteristics of the Study’s Population and Closed Agencies
3.2. Factors Related to Home-Visit Nursing Agency Closure by Years of Operation
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Independent Variables | <3 Years of Operation | 3–14 Years of Operation | ≥15 Years of Operation | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Not Closed | Closed | p | Not Closed | Closed | p | Not Closed | Closed | p | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||||
| A. Regional factors | |||||||||
| Percentage of older adults 65 years old or over † | 25.7 (22.9–30.3) | 25.0 (22.3–29.3) | 0.007 b | 26.6 (23.4–30.6) | 26.3 (23.6–30.6) | 0.714 b | 27.5 (24.3–32.2) | 27.1(24.4–32.3) | 0.788 b |
| Inhabitable area (square km) † | 2827.7 (1097.3–7898.3) | 3269.3 (1083.7–8172.1) | 0.330 b | 2488.1 (883.6–7875.3) | 3669.3 (983.5–8792.5) | 0.034 b | 1507.4 (647.1–5694.3) | 1792.9 (614.4–7975.2) | 0.377 b |
| Number of VNAs per 100,000 population † | 7.0 (5.3–9.5) | 6.5 (4.9–9.2) | 0.038 b | 7.3 (5.3–9.4) | 7.4 (5.5–10.1) | 0.253 b | 6.8 (4.9–9.6) | 7.4 (5.8–11.6) | 0.004 b |
| Number of clinics per 100,000 population † | 77.3 (63.5–91.5) | 75.9 (63.4–92.5) | 0.789 b | 78.6 (65.8–94.1) | 81.2 (68.0–99.3) | 0.012 b | 77.3 (64.9–91.5) | 80.8 (68.0–95.6) | 0.062 b |
| B. Organizational factors | |||||||||
| Ownership 1 | |||||||||
| For-profit | 798 (75.7) | 256 (24.3) | 0.099 a | 1287 (87.3) | 188 (12.8) | 0.446 a | 60 (92.3) | 5 (7.7) | 0.774 a |
| Non-profit | 338 (79.7) | 86 (20.3) | 896 (88.3) | 119 (11.7) | 2295 (93.2) | 167 (6.8) | |||
| Ownership 2 | |||||||||
| Medical | 205 (82.7) | 43 (17.3) | 0.018 a | 464 (87.7) | 65 (12.3) | 0.974 a | 1208 (92.7) | 95 (7.3) | 0.318 a |
| Non-medical | 931 (75.7) | 299 (24.3) | 1719 (87.7) | 242 (12.3) | 1147 (93.7) | 77 (6.2) | |||
| Years of operation as of 2014 † | 1.5 (0.8–2.2) | 0.9 (0.6–1.9) | <0.001 b | 7.9 (4.9–10.9) | 6.9 (4.3–10.2) | 0.002 b | 17.0 (15.1–19.1) | 16.2 (15.2–18.1) | 0.013 b |
| Provision of care management services | |||||||||
| No | 599 (74.5) | 205 (25.5) | 0.018 a | 739 (85.9) | 121 (14.1) | 0.055 a | 236 (90.1) | 26 (9.9) | 0.034 a |
| Yes | 538 (79.7) | 137 (20.3) | 1444 (88.6) | 186 (11.4) | 2119 (93.6) | 146 (6.5) | |||
| Number of medical institutions issuing home-visit nursing orders † | 10.0 (3.0–22.0) | 4.5 (1.0–13.0) | <0.001 b | 22.0 (12.0–37.0) | 16.0 (7.0–31.0) | <0.001 b | 22.0 (13.0–33.0) | 16.0 (7.0–27.5) | <0.001 b |
| Number of FTE nurses s † | 3.1(2.6–4.0) | 3.0 (2.6–3.8) | 0.003 b | 4.0 (3.0–5.5) | 3.3 (2.8–4.9) | <0.001 b | 4.9 (3.6–6.8) | 3.9 (3.0–5.0) | <0.001 b |
| Percentage of nurses with less than 3 years of experience in the VNA † | 66.7 (75.0) | 77.5 (83.4) | 0.371 b | 33.0 (45.7) | 40.0 (54.2) | 0.241 b | 25.0 (11.1–40.0) | 25.0 (0.0–40.0) | 0.232 b |
| Percentage of full-time nurses † | 66.7 (42.9–100.0) | 66.7 (40.0–100.0) | 0.802 b | 60.0 (40.0–80.0) | 60.0 (40.0–80.0) | 0.993 b | 66.7 (50.0–85.7) | 75.0 (50.0–100.0) | 0.012 b |
| Number of users per FTE nurses † | 7.2 (2.6–4.0) | 3.7 (0.8–9.3) | <0.001 b | 12.9 (9.1–18.5) | 10.3 (6.1–15.8) | <0.001 b | 13.1 (10.0–16.8) | 11.7 (7.3–15.8) | <0.001 b |
| Change in number of nurses in fiscal 2013 | |||||||||
| Decrease | 55 (83.3) | 11 (16.7) | 0.037 a | 342 (89.3) | 41 (10.7) | 0.169 a | 441 (92.9) | 34 (7.2) | 0.039 a |
| No change | 707 (74.8) | 238 (25.2) | 1106 (86.5) | 173 (13.5) | 1345 (92.4) | 111 (7.6) | |||
| Increase | 375 (80.1) | 93 (19.9) | 735 (88.8) | 93 (11.2) | 569 (95.5) | 27 (4.5) | |||
| Percentage of rehabilitation professionals among home-visit staff † | 0.0 (0.0–28.6) | 0.0 (0.0–8.0) | <0.001 b | 4.7 (0.0–44.4) | 0.0 (0.0–27.1) | <0.001 b | 5.0 (0.0–25.0) | 0.0 (0.0–15.2) | <0.001 b |
| Provision system of services | |||||||||
| Emergency home-visits | |||||||||
| No | 249 (65.5) | 131 (34.5) | <0.001 a | 309 (82.4) | 66 (17.6) | <0.001 a | 234 (90.4) | 25 (9.7) | 0.055 a |
| Yes | 888 (80.8) | 211 (19.2) | 1874 (88.6) | 241 (11.4) | 2121 (93.5) | 147 (6.5) | |||
| Home-based palliative care | |||||||||
| No | 338 (67.6) | 162 (32.4) | <0.001 a | 361 (80.6) | 87 (19.4) | <0.001 a | 259 (87.5) | 37 (12.5) | <0.001 a |
| Yes | 799 (81.6) | 180 (18.4) | 1822 (89.2) | 220 (10.8) | 2096 (94.0) | 135 (6.1) | |||
| Specialized medical care 1 | |||||||||
| No | 286 (66.8) | 142 (33.2) | <0.001 a | 237 (79.8) | 60 (20.2) | <0.001 a | 112 (84.2) | 21 (15.8) | <0.001 a |
| Yes | 851 (81.0) | 200 (19.0) | 1946 (88.7) | 247 (11.3) | 2243 (93.7) | 151 (6.3) | |||
| Specialized medical care 2 | |||||||||
| No | 292 (66.1) | 150 (33.9) | <0.001 a | 257 (79.8) | 65 (20.2) | <0.001 a | 110 (82.7) | 23 (17.3) | <0.001 a |
| Yes | 845 (81.5) | 192 (18.5) | 1926 (88.8) | 242 (11.2) | 2245 (93.8) | 149 (6.2) | |||
| Enhanced service delivery system | |||||||||
| No | 999 (76.1) | 313 (23.9) | 0.061 a | 1275 (85.2) | 222 (14.8) | <0.001 a | 457 (88.7) | 58 (11.3) | <0.001 a |
| Yes | 138 (82.6) | 29 (17.4) | 908 (91.4) | 85 (8.6) | 1898 (94.3) | 114 (5.7) | |||
| Cooperative discharge guidance with hospitals | |||||||||
| No | 411 (70.0) | 176 (30.0) | <0.001 a | 507 (82.3) | 109 (17.7) | <0.001 a | 404 (89.0) | 50 (11.0) | <0.001 a |
| Yes | 726 (81.4) | 166 (18.6) | 1676 (89.4) | 198 (10.6) | 1951 (94.1) | 122 (5.9) | |||
| Number of types of medical care that can be provided † | 11 (6–13) | 9 (1–13) | <0.001 b | 12 (10–13) | 11 (8–13) | <0.001 a | 12 (11–13) | 11 (9–13) | <0.001 b |
| Percentage of users under the age of 40 † | 0.0 (0.0–2.8) | 0.0 (0.0–4.2) | 0.977 b | 1.2 (0.0–4.6) | 0.0 (0.0–4.5) | 0.052 b | 2.0 (0.0–5.0) | 0.0 (0.0–3.4) | <0.001 b |
| Percentage of users with care need level of 4 or higher † | 31.8 (20.0–44.4) | 30.8 (18.2–50.0) | 0.712 b | 33.3 (25.0–43.6) | 34.3 (24.0–48.6) | 0.596 b | 36.1 (27.1–46.5) | 34.1 (25.4–46.2) | 0.235 b |
References
- OECD. OECD Health Project: Long-Term Care for Older People; OECD Publishing: Paris, France, 2005. [Google Scholar] [CrossRef]
- Statistics Bureau of Japan. Statistical Handbook of Japan 2020. Available online: https://www.stat.go.jp/english/data/handbook/c0117.html (accessed on 22 March 2021).
- Tamiya, N.; Noguchi, H.; Nishi, A.; Reich, M.R.; Ikegami, N.; Hashimoto, H.; Shibuya, K.; Kawachi, I.; Cambell, J.C. Population ageing and wellbeing: Lessons from Japan’s long-term care insurance policy. Lancet 2011, 378, 1183–1192. [Google Scholar] [CrossRef]
- Campbell, J.C.; Ikegami, N. Long-term care insurance comes to Japan. Health Aff. 2000, 19, 26–39. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour, and Welfare. Survey of Institutions and Establishments for Long-Term Care. 2000–2019. Available online: https://www.e-stat.go.jp/stat-search/files?page=1&toukei=00450042&tstat=000001029805 (accessed on 22 March 2021). (In Japanese).
- Ministry of Health, Labour, and Welfare. Fact-Finding Survey on Economic Conditions in Long-Term Care. 2020. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/kaigo/jittai20/dl/r02_kekka.pdf (accessed on 22 March 2021). (In Japanese).
- Fukui, S.; Yoshiuchi, K.; Fujita, J.; Ikezaki, S. Determinants of financial performance of home-visit nursing agencies in Japan. BMC Health Serv. Res. 2014, 14, 11. [Google Scholar] [CrossRef] [PubMed]
- The National Association for Visiting Nurse Service. Survey on the Number of Home-Visit Nursing Agencies. Available online: https://www.zenhokan.or.jp/new/topic/basic/ (accessed on 22 March 2021). (In Japanese).
- Choi, S.; Davitt, J.K. Change in the Medicare home health care market. The impact of reimbursement policy. Med. Care 2009, 47, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Porell, F.W.; Liu, K.; Brungo, D.P. Agency and market area factors affecting home health agency supply changes. Health Sev. Res. 2006, 41, 1847–1875. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, S. How has the Japanese health system implemented the care management system? Asian Pac. J. Dis. Manag. 2009, 3, 33–38. [Google Scholar] [CrossRef][Green Version]
- Yamada, M. Long-term care system in Japan. Ann. Geriatr. Med. Res. 2020, 24, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.; Igarashi, A.; Noguchi-Watanabe, M.; Yoshie, S.; Iijima, K.; Yamamoto-Mitani, N. Characteristics of care management agencies affect expenditure on home help and day care services: A population-based cross-sectional study in Japan. Geriatr. Gerontol. Int. 2017, 17, 2224–2231. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, S.; Nakamura, J. Gatekeeper incentive and demand inducement: An empirical analysis of care managers in the Japan long-term care insurance program. J. Jpn. Int. Economics. 2016, 40, 1–16. [Google Scholar] [CrossRef]
- Japan Visiting Nursing Foundation. Structure of the Visiting Nursing System in Japan. Available online: https://www.jvnf.or.jp/global/Structure_of_the_Visiting_Nursing_system_in_Japan_EN.pdf (accessed on 22 March 2021).
- Castle, N.G. Nursing home closures, changes in ownership, and competition. Inquiry 2005, 42, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Castle, N.G.; Engberg, J.; Lave, J.; Fisher, A. Factors associated with increasing nursing home closures. Health Serv. Res. 2009, 44, 1088–1109. [Google Scholar] [CrossRef] [PubMed]
- Allan, S.; Forder, J. The determinants of care home closure. Health Econ. 2015, 24, 132–145. [Google Scholar] [CrossRef] [PubMed]
- Kitchener, M.; Bostrom, A.; Harrington, C. Smoke without fire: Nursing facility closure in California, 1997–2001. J. Health Care Organ. Provis. Financ. 2004, 41, 189–202. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Information Publication System for Long-Term Care Insurance Services Database. Available online: https://www.kaigokensaku.mhlw.go.jp/ (accessed on 22 March 2021). (In Japanese).
- Statistics Bateau of Japan. Statistical Observations of Municipalities. Available online: https://www.e-stat.go.jp/regional-statistics/ssdsview (accessed on 5 September 2021). (In Japanese).
- McCall, N.; Komisar, H.L.; Peterson, A.; Moore, S. Medicare home health before and after the BBA. Health Aff. 2001, 20, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Long, S.K.; Brungo, D.P. Medicare interim payment system’s impact on Medicare home health utilization. Health Care Financ. Rev. 2003, 25, 81–97. [Google Scholar] [PubMed]
- Jung, K.; Polsky, D. Competition and quality in home health care markets. Health Econ. 2013, 23, 298–313. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfre. Survey of Long-Term Care Benefit Expenditures. Available online: https://www.mhlw.go.jp/toukei/list/45-1b.html (accessed on 22 March 2021). (In Japanese).
- Japanese Nursing Association; Japan Visiting Nursing Foundation; The National Association for Visiting Nurse Service. Action Plan of Home-Visit Nursing 2025. Available online: https://www.jvnf.or.jp/2017/actionplan2025.pdf (accessed on 5 September 2021). (In Japanese).


| Total | Closed | |||
|---|---|---|---|---|
| (n = 6496) | (n = 821) | |||
| Median ± 25–75 percentile or number of subjects (%) | ||||
| A. Regional factor | ||||
| Percentage of older adults 65 years old or over | 26.7 | 23.5–31.2 | 26.0 | 23.0–30.3 |
| Inhabitable area (square km) | 2229.7 | 823.9–7417.9 | 3031.3 | 930.3–8329.9 |
| Number of VNAs per 100,000 population | 7.0 | 5.2–9.6 | 7.0 | 5.3–10.1 |
| Number of clinics per 100,000 population | 77.8 | 64.9–93.5 | 79.3 | 65.9–94.9 |
| B. Organizational factor | ||||
| For-profit organization | ||||
| Yes | 2594 | (39.9) | 449 | (54.7) |
| No | 3901 | (60.1) | 372 | (45.3) |
| Medical organization | ||||
| Yes | 2080 | (30.2) | 203 | (24.7) |
| No | 4415 | (68.0) | 618 | (75.3) |
| Years of operation as of March 31, 2015 | 10.3 | 3.2–15.9 | 4.0 | 1.0–12.7 |
| Provision of care management services | ||||
| Yes | 4570 | (29.6) | 469 | (57.1) |
| No | 1926 | (70.4) | 352 | (42.9) |
| Number of medical institutions issuing home-visit nursing orders | 19 | 9–32 | 11 | 3–23 |
| Number of FTE nurses | 4.0 | 3.0–5.6 | 3.2 | 2.7–4.5 |
| Percentage of nurses with less than three years of experience in the VNAs | 33.3 | 12.5–62.5 | 40.0 | 0.0–85.7 |
| Percentage of full-time nurses | 66.7 | 42.9–85.7 | 66.7 | 42.9–100.0 |
| Number of users per FTE nurses | 11.8 | 7.7–16.5 | 8.0 | 3.4–14.0 |
| Change in the number of nurses in 2013 | ||||
| Decrease | 924 | (14.2) | 86 | (10.5) |
| No change | 3680 | (56.7) | 522 | (63.6) |
| Increase | 1892 | (29.1) | 213 | (25.9) |
| Percentage of rehabilitation professionals among home-visit staff | 1.3 | 0.0–30.0 | 0.0 | 0.20.0 |
| Provision system of services | ||||
| Emergency home-visits | ||||
| Yes | 5482 | (84.4) | 222 | (27.0) |
| No | 1014 | (15.6) | 599 | (73.0) |
| Home-based palliative care | ||||
| Yes | 5252 | (80.8) | 535 | (65.2) |
| No | 1244 | (19.2) | 286 | (34.8) |
| Specialized medical care 1 | ||||
| Yes | 5638 | (86.8) | 598 | (72.8) |
| No | 858 | (13.2) | 223 | (27.1) |
| Specialized medical care 2 | ||||
| Yes | 5599 | (86.2) | 583 | (71.0) |
| No | 897 | (13.8) | 238 | (29.0) |
| Enhanced service delivery | ||||
| Yes | 3172 | (48.8) | 228 | (27.8) |
| No | 3324 | (51.2) | 593 | (72.2) |
| Cooperative discharge guidance with hospitals | ||||
| Yes | 4839 | (74.5) | 486 | (59.2) |
| No | 1657 | (25.5) | 335 | (40.8) |
| Number of types of medical care that can be provided | 12 | 10–13 | 11 | 6–13 |
| Percentage of users under the age of 40 years | 1.1 | 0.0–4.5 | 0.0 | 0.0–4.2 |
| Percentage of users with care need level of four or higher | 34.2 | 25.0–45.5 | 33.3 | 22.6–48.6 |
| Years of Operation | Total (n = 6496) | Closed (n = 821) | Not Closed (n = 5673) | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| <3 years | 1479 | 342 | 23.1 | 1137 | 76.9 |
| 3–14 years | 2490 | 307 | 12.3 | 2183 | 87.7 |
| ≥15 years | 2527 | 172 | 6.8 | 2355 | 93.2 |
| Variables | <3 Years of Operation (n = 1195) | 3–14 Years of Operation (n = 2356) | ≥15 Years of Operation (n = 2450) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| AOR | (95%CI) | p | AOR | (95%CI) | p | AOR | (95%CI) | p | |
| A. Regional factor | |||||||||
| Percentage of older adults 65 years old or over | 0.963 | (0.935–0.991) | 0.010 | 0.999 | (0.976–1.023) | 0.957 | 1.006 | (0.978–1.034) | 0.672 |
| Inhabitable area (square km) | 1.000 | (1.000–1.000) | 0.448 | 1.000 | (1.000–1.000) | 0.001 | 1.000 | (1.000–1.000) | 0.002 |
| Number of VNAs per 100,000 population | 0.991 | (0.978–0.999) | 0.113 | 0.997 | (0.991–1.000) | 0.114 | 1.000 | (0.993–1.005) | 0.962 |
| Number of clinics per 100,000 population | 1.004 | (1.001–1.007) | 0.012 | 1.003 | (1.001–1.006) | 0.008 | 1.000 | (0.994–1.005) | 0.962 |
| B. Organizational factor | |||||||||
| For-profit organization (ref = non-profit) | 1.132 | (0.689–1.914) | 0.634 | 0.845 | (0.582–1.242) | 0.384 | 0.777 | (0.251–1.969) | 0.625 |
| Medical organization (ref = non-medical) | 0.612 | (0.330–1.137) | 0.118 | 1.050 | (0.691–1.598) | 0.821 | 0.869 | (0.610–1.240) | 0.437 |
| Years of operation as of FY2014 | 0.938 | (0.761–1.157) | 0.552 | 0.983 | (0.942–1.025) | 0.427 | 0.938 | (0.866–1.009) | 0.101 |
| Provision of care management services (ref = no) | 1.117 | (0.814–1.533) | 0.493 | 0.955 | (0.721–1.270) | 0.748 | 0.724 | (0.461–1.179) | 0.177 |
| Number of medical institutions issuing home-visit nursing orders | 0.986 | (0.945–1.029) | 0.005 | 0.992 | (0.980–1.004) | 0.223 | 0.994 | (0.976–1.012) | 0.534 |
| Number of FTE nurses | 1.003 | (0.970–1.035) | 0.110 | 0.952 | (0.927–0.976) | 0.006 | 0.848 | (0.755–0.942) | 0.004 |
| Percentage of nurses with less than three years of experience | 1.001 | (0.998–1.005) | 0.493 | 1.002 | (0.997–1.006) | 0.423 | 0.996 | (0.989–1.003) | 0.297 |
| Percentage of full-time nurses | 0.996 | (0.990–1.002) | 0.162 | 1.000 | (0.995–1.005) | 0.934 | 1.005 | (0.998–1.012) | 0.161 |
| Number of users per FTE nurses | 1.003 | (0.970–1.035) | 0.878 | 0.952 | (0.927–0.976) | <0.001 | 0.978 | (0.944–1.011) | 0.204 |
| Change in number of nurses in 2013 | |||||||||
| Decrease (ref = no change) | 0.808 | (0.361–1.656) | 0.613 | 0.806 | (0.540–1.178) | 0.536 | 1.308 | (0.845–1.985) | 0.132 |
| Increase (ref = no change) | 0.955 | (0.676–1.342) | 0.793 | 0.825 | (0.601–1.125) | 0.603 | 0.887 | (0.545–1.404) | 0.280 |
| Percentage of rehabilitation professionals among home-visit staff | 1.002 | (0.997–1.006) | 0.463 | 1.003 | (0.999–1.007) | 0.101 | 0.997 | (0.988–1.005) | 0.423 |
| Provision system of services | |||||||||
| Emergency home-visits (ref = no) | 0.801 | (0.493–1.303) | 0.370 | 1.061 | (0.669–1.706) | 0.804 | 1.869 | (1.023–3.571) | 0.049 |
| Home-based palliative care (ref = no) | 0.898 | (0.569–1.429) | 0.645 | 0.814 | (0.526–1.274) | 0.360 | 0.847 | (0.489–1.511) | 0.564 |
| Specialized medical care 1 (ref = no) | 1.213 | (0.661–2.251) | 0.535 | 1.033 | (0.552–1.949) | 0.920 | 1.053 | (0.437–2.630) | 0.911 |
| Specialized medical care 2 (ref = no) | 0.802 | (0.457–1.417) | 0.444 | 0.923 | (0.520–1.670) | 0.787 | 0.531 | (0.236–1.234) | 0.132 |
| Enhanced service delivery (ref = no) | 1.457 | (0.860–2.413) | 0.151 | 0.728 | (0.522–1.010) | 0.059 | 0.703 | (0.481–1.036) | 0.071 |
| Cooperative discharge guidance with hospitals (ref = no) | 0.760 | (0.531–1.091) | 0.134 | 0.824 | (0.599–1.142) | 0.241 | 0.925 | (0.608–1.431) | 0.720 |
| Number of types of medical care that can be provided | 0.986 | (0.945–1.029) | 0.521 | 0.940 | (0.894–0.988) | 0.015 | 0.937 | (0.873–1.006) | 0.071 |
| Percentage of users under the age of 40 years | 1.019 | (1.005–1.034) | 0.007 | 1.011 | (0.995–1.026) | 0.174 | 0.968 | (0.927–1.004) | 0.110 |
| Percentage of users with care need level of four or higher | 1.004 | (0.998–1.011) | 0.202 | 1.003 | (0.996–1.011) | 0.363 | 0.995 | (0.984–1.006) | 0.397 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashiwagi, M.; Morioka, N. Characteristics of Home-Visit Nursing Agencies That Closed after the 2012 Fee Revision for Home-Visit Nursing Services: A Nationwide Panel Data Analysis in Japan. Int. J. Environ. Res. Public Health 2021, 18, 9820. https://doi.org/10.3390/ijerph18189820
Kashiwagi M, Morioka N. Characteristics of Home-Visit Nursing Agencies That Closed after the 2012 Fee Revision for Home-Visit Nursing Services: A Nationwide Panel Data Analysis in Japan. International Journal of Environmental Research and Public Health. 2021; 18(18):9820. https://doi.org/10.3390/ijerph18189820
Chicago/Turabian StyleKashiwagi, Masayo, and Noriko Morioka. 2021. "Characteristics of Home-Visit Nursing Agencies That Closed after the 2012 Fee Revision for Home-Visit Nursing Services: A Nationwide Panel Data Analysis in Japan" International Journal of Environmental Research and Public Health 18, no. 18: 9820. https://doi.org/10.3390/ijerph18189820
APA StyleKashiwagi, M., & Morioka, N. (2021). Characteristics of Home-Visit Nursing Agencies That Closed after the 2012 Fee Revision for Home-Visit Nursing Services: A Nationwide Panel Data Analysis in Japan. International Journal of Environmental Research and Public Health, 18(18), 9820. https://doi.org/10.3390/ijerph18189820