
Ergonomic Risk Assessment during an Informal Hand-Made Cookware Operation: Extending an Existing Model

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
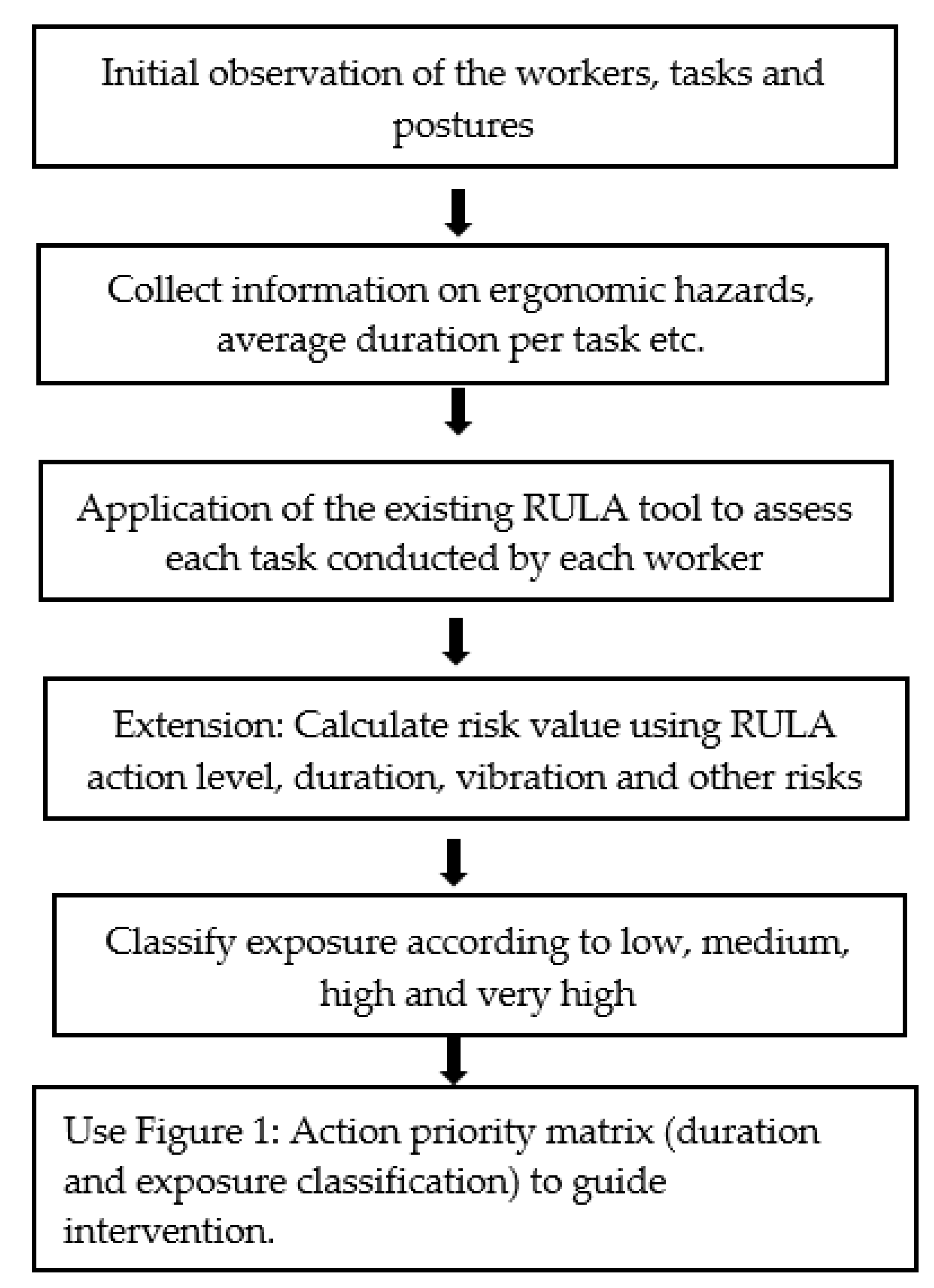
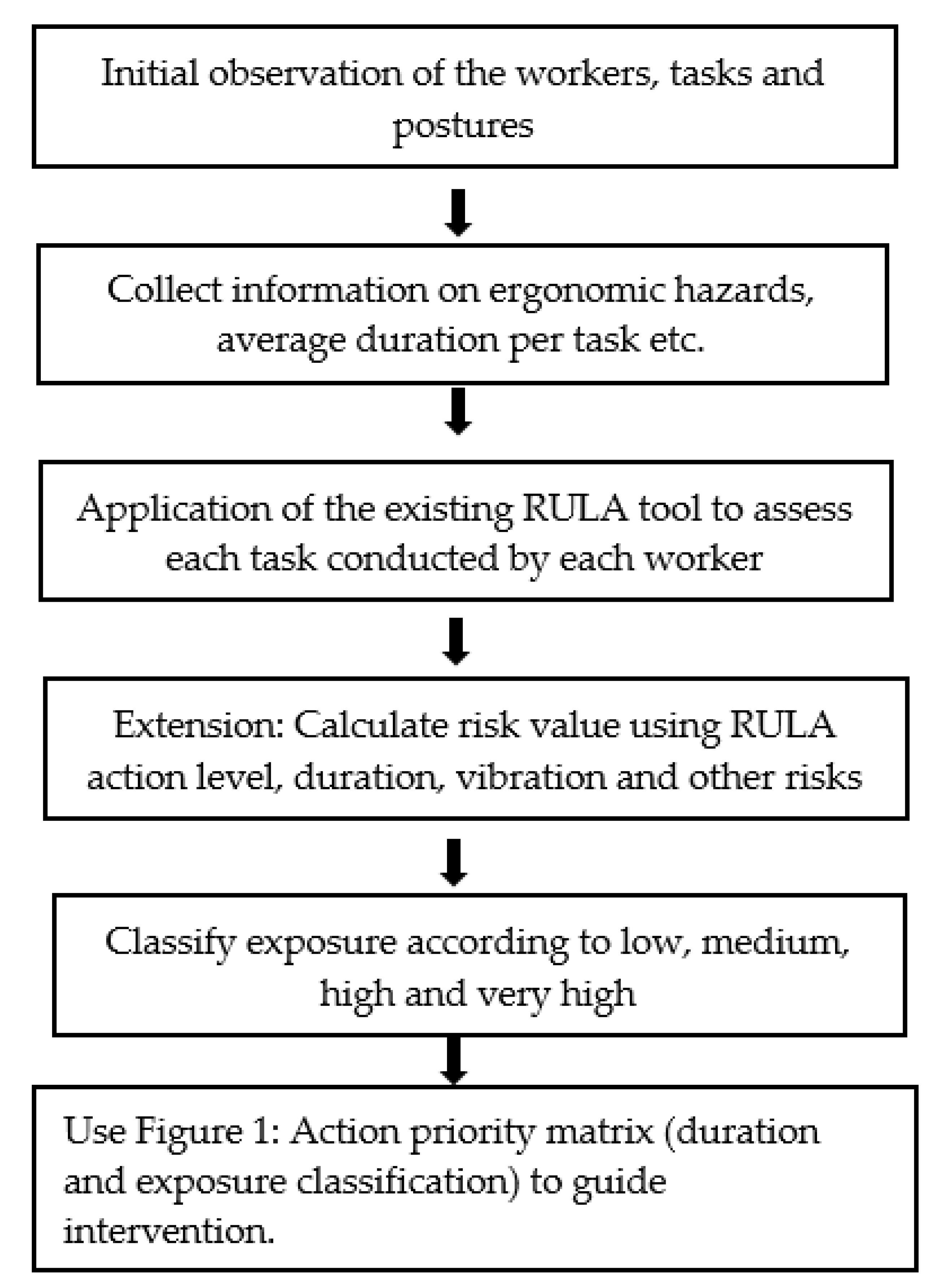
2.2. Data Analysis
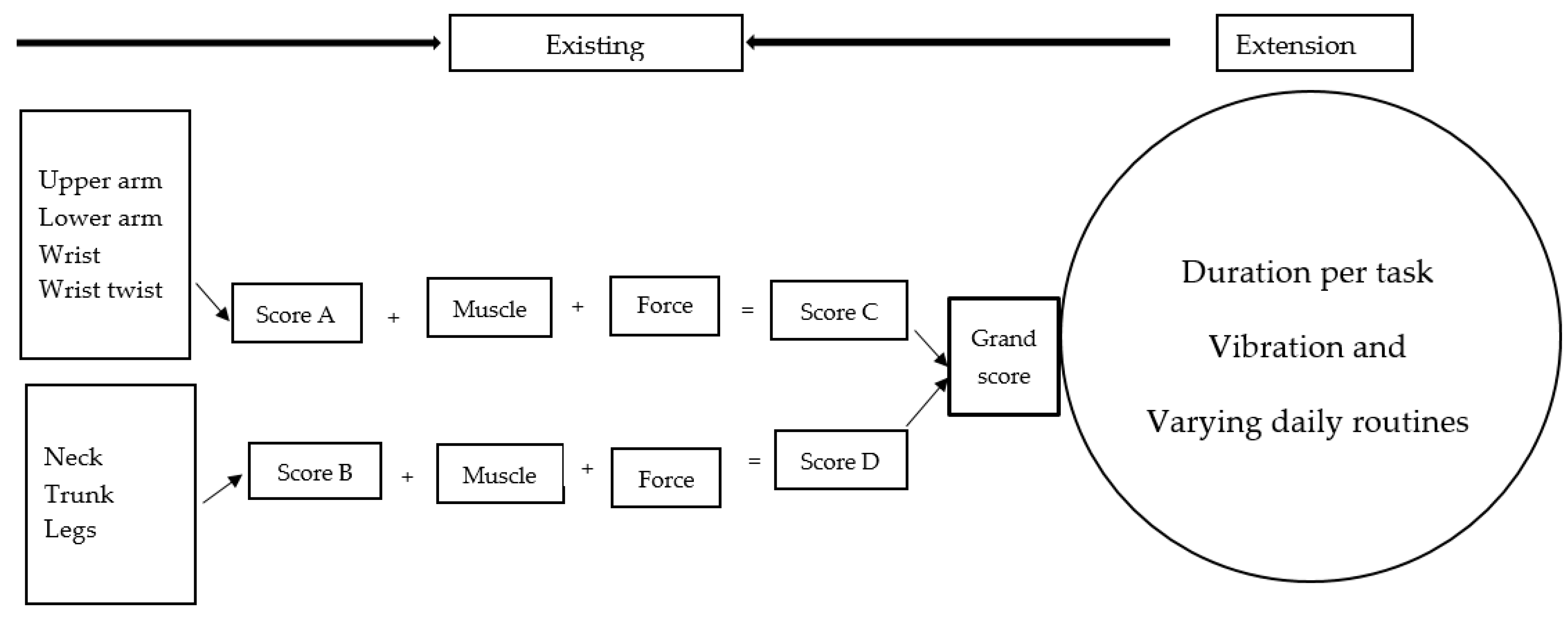
Rapid Upper Limb Assessment (RULA) Tool
- (i)
- RULA—An Existing Ergonomic Risk Assessment Tool
- (ii)
- An extended RULA method
3. Results
3.1. Demographic and Work Characteristics
3.2. Hand-Made Cookware Operation Process
3.3. Risk Assessment
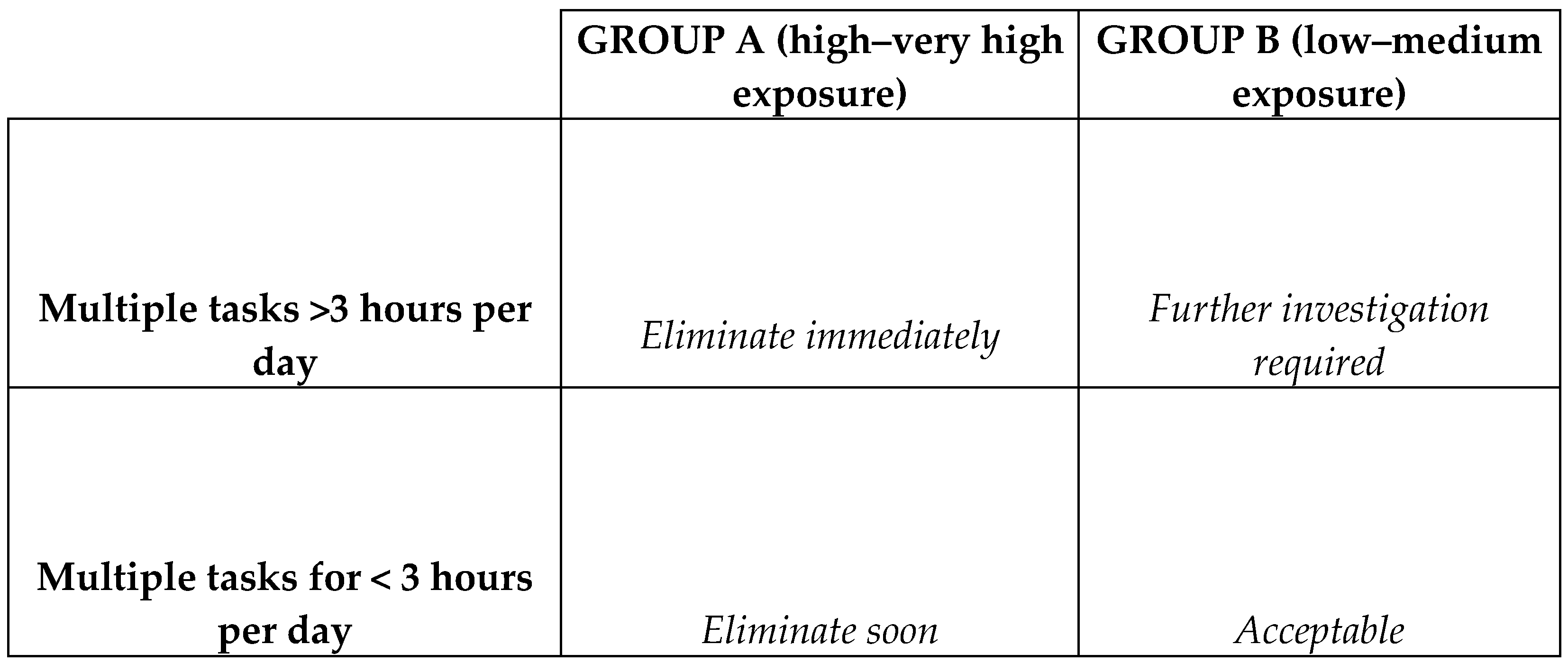
3.4. Action Priority Matrix
3.5. Application of the Extended Tool in Other Informal Work Settings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Choobineh, A.; Tabatabaei, S.H.; Mokhtarzadeh, A.; Salehi, M. Musculoskeletal problems among workers of an Iranian rubber factory. J. Occup. Health 2007, 49, 418–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punnett, L.; Wegman, D.H. Work-related musculoskeletal disorders: The epidemiologic evidence and the debate. J. Electromyogr. Kinesiol. 2004, 14, 13–23. [Google Scholar] [CrossRef]
- Sim, J.; Lacey, R.J.; Lewis, M. The impact of workplace risk factors on the occurrence of neck and upper limb pain: A general population study. BMC Public Health 2006, 6, 234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernard, B. A Critical Review of Epidemiologic Evidence for Work-Related Musculoskeletal Disorders of the Neck, Upper Extremity, and Low Back. Available online: https://www.cdc.gov/niosh/docs/97-141/ (accessed on 25 June 2020).
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Hoy, D.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Bain, C.; Williams, G.; Smith, E.; Vos, T.; Barendregt, J. The global burden of low back pain: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 968–974. [Google Scholar] [CrossRef] [Green Version]
- David, G.; Woods, V.; Li, G.; Buckle, P. The development of the Quick Exposure Check (QEC) for assessing exposure to risk factors for work-related musculoskeletal disorders. Appl. Ergon. 2008, 39, 57–69. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, L.; Karasek, R.; Punnett, L.; Scharf, T. Covariation between workplace physical and psychosocial stressors: Evidence and implications for occupational health research and prevention. Ergonomics 2001, 44, 696–718. [Google Scholar] [CrossRef]
- McAtamney, L.; Hignett, S. REBA: A rapid entire body assessment method for investigating work related musculoskeletal disorders. In Proceedings of the 31st Annual Conference of the Ergonomics Society of Australia, Adelaide, Australia, 13–15 December 1995. [Google Scholar]
- McAtamney, L.; Corlett, E.N. RULA: A survey method for the investigation of work-related upper limb disorders. Appl. Ergon. 1993, 24, 91–99. [Google Scholar] [CrossRef]
- Steven Moore, J.; Garg, A. The strain index: A proposed method to analyze jobs for risk of distal upper extremity disorders. Am. Ind. Hyg. Assoc. J. 1995, 56, 443–458. [Google Scholar] [CrossRef]
- Waters, T.R.; Putz-Anderson, V.; Garg, A.; Fine, L.J. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics 1993, 36, 749–776. [Google Scholar] [CrossRef]
- Karhu, O.; Kansi, P.; Kuorinka, I. Correcting working postures in industry: A practical method for analysis. Appl. Ergon. 1977, 8, 199–201. [Google Scholar] [CrossRef]
- Sesek, R.; Gilkey, D.; Rosecrance, J.; Guzy, A. The Utility of OWAS in Auto Manufacturing Assembly Job Evaluations. Available online: https://www.academia.edu/5314247/the_utility_of_owas_in_auto_manufacturing_assembly (accessed on 15 February 2020).
- Roman-Liu, D.; Groborz, A.; Tokarski, T. Comparison of risk assessment procedures used in OCRA and ULRA methods. Ergonomics 2013, 56, 1584–1598. [Google Scholar] [CrossRef] [Green Version]
- Roman-Liu, D. Upper limb load as a function of repetitive task parameters: Part 1—A model of upper limb load. Int. J. Occup. Saf. Ergon. 2005, 11, 93–102. [Google Scholar] [CrossRef]
- Roman-Liu, D.; Tokarski, T. Upper limb load as a function of repetitive task parameters: Part 2—An experimental study. Int. J. Occup. Saf. Ergon. 2005, 11, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Chander, D.S.; Cavatorta, M.P. An observational method for postural ergonomic risk assessment (PERA). Int. J. Ind. Ergon. 2017, 57, 32–41. [Google Scholar] [CrossRef]
- Tangkittipaporn, J.; Jiangsathaporn, W. Musculoskeletal pain and mental agony reacting to ergonomic risks in the Thai informal working environment. Psychology 2017, 7, 73–88. [Google Scholar] [CrossRef] [Green Version]
- De Sousa, M.N.A.; de Oliveira Santos, B.M.; Zaia, J.E.; Bertoncello, D.; Feitosa, A.D.N.A.; de Assis, E.V.; Batista, H.M.T.; de Mello Monteiro, C.B.; Maia, P.C.G.G.S.; Bezerra, I.M.P. Musculoskeletal disorders in informal mining workers. Int. Arch. Med. 2015, 8. [Google Scholar] [CrossRef] [Green Version]
- Acquah, A.; Arko-Mensah, J.; D’Souza, C.; Martin, B.; Quakyi, I.; Robins, T.; Fobil, J. Prevalence of work-related musculoskeletal disorders among e-waste workers at Agbogbloshie in Accra, Ghana. Environ. Epidemiol. 2019, 3, 2–3. [Google Scholar] [CrossRef]
- ILO. Safety and Health at Work: A Vision for Sustainable Prevention. In Proceedings of the XX World Congress on Safety and Health at Work 2014, Frankfurt, Germany, 24–27 August 2014. Available online: https://www.ilo.org/global/topics/safety-and-health-at-work/resources-library/publications/WCMS_301214/lang--en/index.htm (accessed on 30 May 2020).
- Forastieri, V. Improvement of Working Conditions and Environment in the Informal Sector through Safety and Health Measures. Available online: https://www.ilo.org/safework/info/publications/WCMS_110306/lang--en/index.htm (accessed on 25 June 2020).
- WHO. Global Strategy on Occupational Health for All: The Way to Health at Work, Recommendation of the Second Meeting of the WHO Collaborating Centres in Occupational Health, Beijing, China, 11–14 October 1994; WHO: Geneva, Switzerland, 1994. [Google Scholar]
- Takala, E.-P.; Pehkonen, I.; Forsman, M.; Hansson, G.-Å.; Mathiassen, S.E.; Neumann, W.P.; Sjøgaard, G.; Veiersted, K.B.; Westgaard, R.H.; Winkel, J. Systematic evaluation of observational methods assessing biomechanical exposures at work. Scand. J. Work. Environ. Health 2010, 3–24. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.-X.; Sun, S.-Q.; Tang, Z.-C. Comparison of contact interface factors for surface electromyography control wearable device. Adv. Mech. Eng. 2018, 10. [Google Scholar] [CrossRef] [Green Version]
- Shezi, B.; Naidoo, R.N.; Muttoo, S.; Mathee, A.; Alfers, L.; Dobson, R.; Ndlovu, P.; Street, R.A. Informal-sector occupational hazards: An observational workplace assessment of the traditional medicine trade in South Africa. Int. J. Occup. Saf. Ergon. 2019. [Google Scholar] [CrossRef]
- Guma, T.N.; Uche, L.O. Sand Mould Design for Casting an Aluminium Pot-A Basic Procedure of Supplementing Artisanal Practices. Eur. J. Eng. Res. Sci. 2019, 4, 24–30. [Google Scholar] [CrossRef]
- Guma, T.; Uche, O.L. A typification of foundry practices for correct artisanal sand casting of aluminum pots. Engineering 2019. [Google Scholar] [CrossRef]
- Street, R.A.; Mathee, A.; Tanda, S.; Hauzenberger, C.; Naidoo, S.; Goessler, W. Recycling of scrap metal into artisanal cookware in the informal sector: A public health threat from multi metal exposure in South Africa. Sci. Total Environ. 2020, 699, 134324. [Google Scholar] [CrossRef] [PubMed]
- Shezi, B.; Mathee, A.; Cele, N.; Ndabandaba, S.; Street, R.A. Occupational Exposure to Fine Particulate Matter (PM4 and PM2. 5) during Hand-Made Cookware Operation: Personal, Indoor and Outdoor Levels. Int. J. Environ. Res. Public Health 2020, 17, 7522. [Google Scholar] [CrossRef]
- Park, S.; Vega, R.; Choto, Z.; Grewe, M. Risk-based asset prioritization of water transmission/distribution pipes for the City of Tampa. Fla. Water Resour. J. 2010, 22–28. Available online: https://www.fwrj.com/techarticles/1210%20tech%203.pdf (accessed on 27 August 2021).
- Ramani, V.K. Prioritization matrix for the diabetes prevention and control program: A concept paper. J. Diabetol. 2021, 12, 191. [Google Scholar] [CrossRef]
- Wahlström, J. Ergonomics, musculoskeletal disorders and computer work. Occup. Med. 2005, 55, 168–176. [Google Scholar] [CrossRef] [Green Version]
- Thiehoff, R. Economic significance of work disability caused by musculoskeletal disorders. Der Orthop. 2002, 31, 949–956. [Google Scholar] [CrossRef]
- Gentzler, M.; Stader, S. Posture stress on firefighters and emergency medical technicians (EMTs) associated with repetitive reaching, bending, lifting, and pulling tasks. Work 2010, 37, 227–239. [Google Scholar] [CrossRef]
- Acquah, A.A.; D’Souza, C.; Martin, B.; Arko-Mensah, J.; Asabea Nti, A.; Kwarteng, L.; Takyi, S.; Botwe, P.K.; Tettey, P.; Dwomoh, D. Development of an Observation-Based Tool for Ergonomic Exposure Assessment in Informal Electronic Waste Recycling and Other Unregulated Non-Repetitive Work. Available online: https://www.researchgate.net/publication/349144912_ (accessed on 19 March 2021).
- Middlesworth, M. Rapid Entire Body Assessment (REBA). Available online: https://ergo-plus.com/reba-assessment-tool-guide/ (accessed on 11 April 2020).
- Comper, M.L.C.; Padula, R.S. Ergonomic risk assessment among textile industry workers using two instruments: Quick Exposure Check and Job Factors Questionnaire. Educação Pesquisa 2013, 20, 215–221. [Google Scholar] [CrossRef]
- Lind, C. Assessment and Design of Industrial Manual Handling to Reduce Physical Ergonomics Hazards: Use and Development of Assessment Tools. Available online: https://www.diva-portal.org/smash/get/diva2:1094542/FULLTEXT02 (accessed on 30 June 2020).
- Bovenzi, M.; Hulshof, C. An updated review of epidemiologic studies on the relationship between exposure to whole-body vibration and low back pain (1986–1997). Int. Arch. Occup. Environ. Health 1999, 72, 351–365. [Google Scholar] [CrossRef] [PubMed]
- Lowe, B.D. Accuracy and validity of observational estimates of wrist and forearm posture. Ergonomics 2004, 47, 527–554. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) |
|---|---|
| Age: mean (SD) | 36 (14) |
| Gender: Male | 18 (100) |
| Education: never completed high school | 14 (78) |
| Personal protective equipment | 2 (11) |
| Working period: ≥5 years | 7 (40) |
| Description of the Activity | Description of the Hazard | ||||||
|---|---|---|---|---|---|---|---|
| Back | Arm | Legs | Wrist | Instrumentation/Load | |||
| Preparing sand |  | Loosening sand and breaking up lumps in the soils | The movement of the back is very frequent (around 12 times per minute or more) | Repetitive movements of the arms and lifting weights above shoulder height (12 times per minute or more) | Body weight is evenly distributed over both feet, with room for changes or position | Repetitive movements of the wrist (12 times per minute or more with 15° or more in either flexion or extension | Spade or shovel, maximum force exerted was ±2 kg |
| Preparing flat sand surface |  | Preparing a flat sand surface to make a bed for the mould cavity | The range in movement of the trunk is 60° or more flexion (12 times per minute or more) | Repetitive movements of the arms (12 times per minute or more) | Body weight is evenly distributed over both feet, with room for changes or position | Repetitive movements of the wrist. The task involves 0–15° in either flexion or extension (12 times per minute or more) | The maximum force exerted was ±2 kg |
| Loading sand |  | Loading sand onto the replica of the cookware and the casting box to create mould cavity | The range in movement of the trunk is at or between 20–60° flexion. In some instances, the back is excessively flexed or twisted or the side is bent. The movement of the back is very frequent (around 12 times per minute or more) | Repetitive movements of the arms (12 times per minute or more) | Body weight is evenly distributed over both feet, with room for changes or position | Repetitive movements of the wrist. The task involves 0–15° in either flexion or extension (12 times per minute or more) | Spade, maximum weight of between 3 and 5 kg |
| Creating mould cavity |  | Packing sand onto the replica of the cookware to make a mould cavity and ramming sand onto the excess space of the casting box | The range in movement of the trunk is at or between 20–60° flexion. In some instances, the back is excessively flexed or twisted or side bent. The movement of the back is very frequent (around 12 times per minute or more) | Lifting weights above shoulder height and repeating similar motion patterns more than 12 times per minute | Kneeling on one or both knees | Repetitive movements of the wrist. The task involves 0–15° in either flexion or extension (12 times per minute or more) | Shovel and a 7-kg rod is used for ramming the sand |
| Dismantle the casting box and sprinkling ash |  | Dismantling the casting box and sprinkling ash onto the mould cavity and flat sand surface | Moderately/excessively flexed or twisted or side bent | Lower arm working across the midline of the body or out to the side; in most cases, the hands are at or below waist height | Standing or squatting with one knee bent or kneeling on one or more knees | The task involves a deviated or bent wrist | The maximum weight handled manually ranges from light (5 kg or less), moderate (6 to 10 kg), heavy (11 to 20 kg) and very heavy (more than 20 kg) |
| Liquefying scrap metal |  | Liquifying scrap metal (i.e., used car and motor bike engine parts, waste aluminium and computer components) | Moderately flexed | Repetitive movements of the arms (12 times per minute or more) | Body weight is evenly distributed over both feet, with room for changes or position. | Repetitive movements of the wrist. The task involves 0–15° in either flexion or extension (12 times per minute or more) | Handling maximum weight of ±10 kg |
| Transporting and pouring molten metal into the mould |  | Transporting molten metal from the furnace to the workstation and pouring molten metal into the mould cavity | The back remains in a static position during the pouring of molten metal | Static posture of the arms | Body weight is evenly distributed over both feet, with room for changes or position | Static posture of the wrist | Long hand handled cup shaped bowl maximum weight of between 11 to 20 kg. The load of more than 10 kg is static for more than 1 min |
| Breaking the mould |  | Breaking the mould | The range in movement of the trunk is at or between 20–60° flexion. In some instances, the back is excessively flexed or twisted or side bent. The movement of the back is very frequent (around 12 times per minute or more) | Repetitive movements of the arms (more than 12 times per minute) | Body weight is evenly distributed over both feet, with room for changes or positions | Repetitive movements of the wrist (around 12 times per minute or more) | Spade or 7 kg rod, maximum weight of between 3 and 5 kg |
| Removing defects |  | Inspection of the final product to remove any defects by removing sand, excess metal from the casting | Moderately/excessively flexed or twisted or side bent, vibration | Repetitive movements of the arms, (around 12 times per minute or more) and vibration | Body weight is evenly distributed over both feet, with room for changes or position, vibration | Repetitive movements of the wrist (around 12 times per minute or more) and vibration | Sanding machine, maximum weight of more than 20 kg. |
| Task | Mean (SD) | Median | Minimum | Maximum |
|---|---|---|---|---|
| Preparing sand | 4 (0.0) | 4 | - | 4 |
| Preparing flat sand surface | 4 (0.6) | 4 | 2 | 4 |
| Loading sand | 4 (0.3) | 4 | 3 | 4 |
| Creating mould cavity | 4 (0.3) | 4 | 3 | 4 |
| Dismantling the mould cavity and sprinkling ash | 3 (0.3) | 3 | 2 | 3 |
| Liquifying metal | 3 (0.5) | 3 | 2 | 3 |
| Transporting and pouring molten metal into the mould | 3 (0.9) | 3 | 2 | 4 |
| Breaking the mould | 3 (0.8) | 3 | 2 | 4 |
| Removing defects | 4 (0.0) | 4 | - | 4 |
| Task | * Average RULA Action Level | ** Duration Per Task | *** Vibration | # Exposure Value | ## Exposure Classification |
|---|---|---|---|---|---|
| 4 | 1 | 0 | 4 | Medium |
| 4 | 2 | 0 | 8 | High |
| 4 | 1 | 0 | 4 | Medium |
| 4 | 3 | 0 | 12 | High |
| 3 | 1 | 0 | 3 | Medium |
| 3 | 2 | 0 | 3 | Medium |
| 3 | 1 | 0 | 3 | Medium |
| 3 | 1 | 0 | 3 | Medium |
| 4 | 4 | 1 | 17 | Very high |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shezi, B.; Street, R.A.; Mathee, A.; Cele, N.; Ndabandaba, S.; Naidoo, R.N. Ergonomic Risk Assessment during an Informal Hand-Made Cookware Operation: Extending an Existing Model. Int. J. Environ. Res. Public Health 2021, 18, 9459. https://doi.org/10.3390/ijerph18189459
Shezi B, Street RA, Mathee A, Cele N, Ndabandaba S, Naidoo RN. Ergonomic Risk Assessment during an Informal Hand-Made Cookware Operation: Extending an Existing Model. International Journal of Environmental Research and Public Health. 2021; 18(18):9459. https://doi.org/10.3390/ijerph18189459
Chicago/Turabian StyleShezi, Busisiwe, Renee A. Street, Angela Mathee, Nokulunga Cele, Sipho Ndabandaba, and Rajen N. Naidoo. 2021. "Ergonomic Risk Assessment during an Informal Hand-Made Cookware Operation: Extending an Existing Model" International Journal of Environmental Research and Public Health 18, no. 18: 9459. https://doi.org/10.3390/ijerph18189459
APA StyleShezi, B., Street, R. A., Mathee, A., Cele, N., Ndabandaba, S., & Naidoo, R. N. (2021). Ergonomic Risk Assessment during an Informal Hand-Made Cookware Operation: Extending an Existing Model. International Journal of Environmental Research and Public Health, 18(18), 9459. https://doi.org/10.3390/ijerph18189459