
An Integrative Review of Recovery Services to Improve the Lives of Adults Living with Severe Mental Illness


Abstract
1. Introduction
2. Methods
2.1. Methodology
2.2. Inclusion Criteria
2.3. Exclusion Criteria
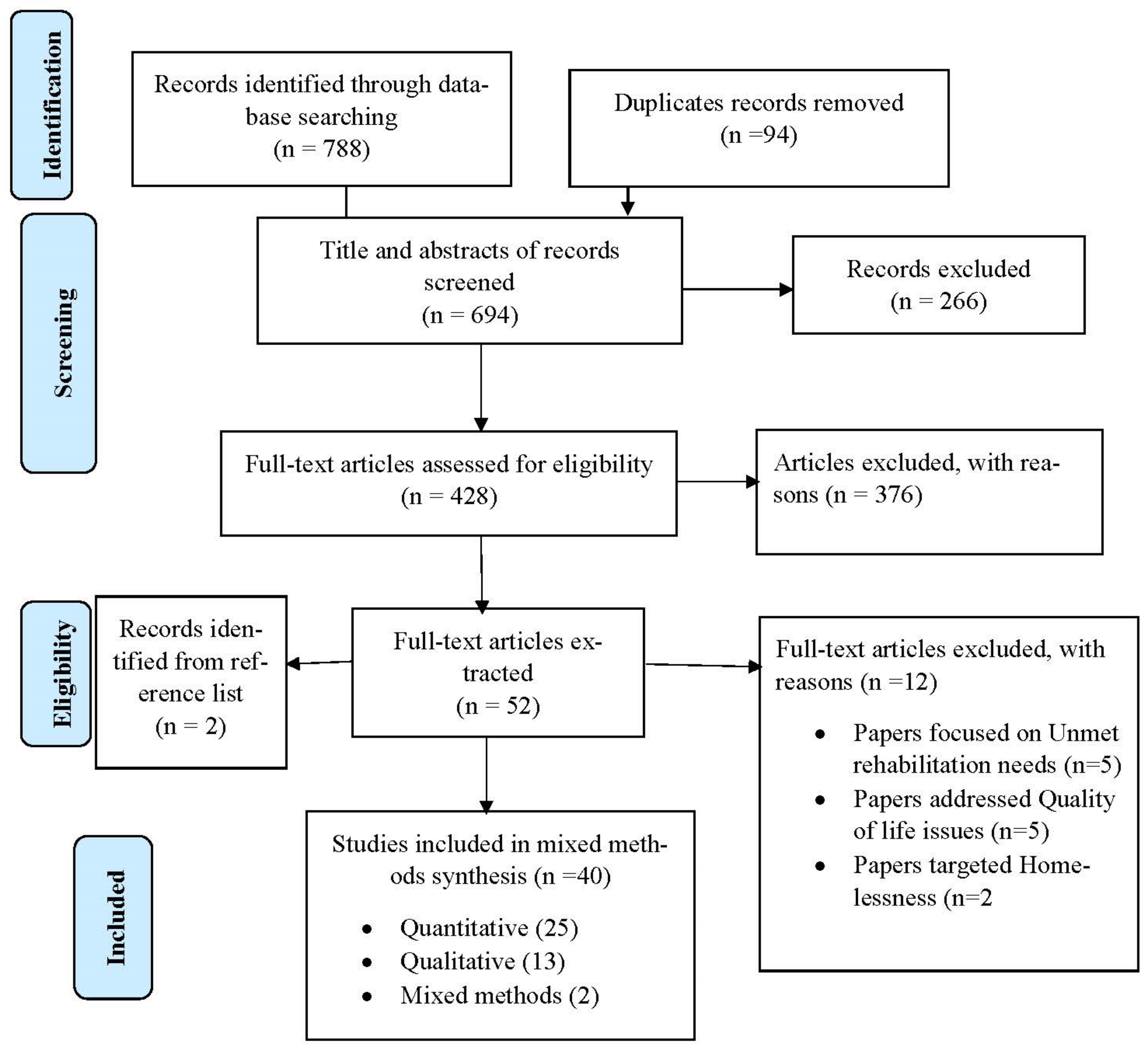
2.4. Search Strategy and Selection Procedure
2.5. Data Management and Extraction
2.6. Assessment of Methodological Quality
3. Data Synthesis
4. Results
Description of Retrieved Papers
5. Characteristics of Included Articles
6. Context for Implementing Recovery Services
7. Mechanisms for Implementing Recovery Services
7.1. An Integrated Recovery Service
7.2. Vocational Rehabilitation (Individual Placement Services)
7.3. Recovery Narrative Photovoice, Art Making and Exhibition
8. Outcome of Recovery Services
8.1. Psychiatric Medication and Treatment
8.2. Improve Functionality
8.3. Reduce Symptoms
8.4. Improvement in Physical Health and Social Behaviour
8.5. Self-Efficacy
8.6. Economic Empowerment
8.7. Social Inclusion (Community Integration)
8.8. Household Integration
8.9. Social Support
9. Discussion
9.1. Mechanisms for Implementing Recovery Services
9.2. Outcome of Recovery Services
10. Limitations
11. Conclusions
12. Implications for Mental Health Policy and Practice
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Individual Placement Services | (IPS); |
| Joanna Briggs Institute | (JBI); |
| Mixed-Methods Appraisal Tool | (MMAT); |
| Preferred Reporting Items for Systematic Reviews and Meta-Analyses | (PRISMA); |
| Severe Mental Illness | (SMI); |
| World Health Organization Disability Assessment Scale | (WHODAS). |
References
- Yildiz, M. Recovery as a process in severe mental illnesses. Nöro Psikiyatr. Arş. 2015, 52, 1. [Google Scholar] [CrossRef]
- Frost, B.G.; Tirupati, S.; Johnston, S.; Turrell, M.; Lewin, T.J.; Sly, K.A.; Conrad, A.M. An Integrated Recovery-oriented Model (IRM) for mental health services: Evolution and challenges. BMC Psychiatry 2017, 17, 22. [Google Scholar] [CrossRef] [PubMed]
- Gopal, S.; Henderson, A.R. Trans-cultural study of recovery from severe enduring mental illness in Chennai, India and Perth, Western Australia. J. Psychosoc. Rehabil. Ment. Health 2015, 2, 51–57. [Google Scholar] [CrossRef]
- Slade, M.; Longden, E. Empirical evidence about recovery and mental health. BMC Psychiatry 2015, 15, 285. [Google Scholar] [CrossRef]
- Drake, R.E.; Whitley, R. Recovery and Severe Mental Illness: Description and Analysis. Can. J. Psychiatry Rev. Can. Psychiatr. 2014, 59, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Noordsy, D.; Torrey, W.; Mueser, K.; Mead, S.; O’Keefe, C.; Fox, L. Recovery from severe mental illness: An intrapersonal and functional outcome definition. Int. Rev. Psychiatry 2002, 14, 318–326. [Google Scholar] [CrossRef]
- Davidson, L.; Roe, D. Recovery from versus recovery in serious mental illness: One strategy for lessening confusion plaguing recovery. J. Ment. Health 2007, 16, 459–470. [Google Scholar] [CrossRef]
- Psych, B.; Remington, G.; Lee, J. Personal recovery in serious mental illness: Making sense of the concept. Ann. Acad. Med. Singap. 2017, 46, 29–31. [Google Scholar]
- Badu, E.; O’Brien, A.P.; Mitchell, R. The Conceptualization of Mental Health Service Quality Assessment: Consumer Perspective. Adm. Policy Ment. Health Ment. Health Serv. Res. 2019, 26, 790–806. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.W.; D’Amico, M.; Jaffe, L.; Arbesman, M. Occupational Therapy Interventions for Recovery in the Areas of Community Integration and Normative Life Roles for Adults with Serious Mental Illness: A Systematic Review. Am. J. Occup. Ther. 2011, 65, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Gyamfi, N.; Badu, E.; Mprah, W.K.; Mensah, I. Recovery services and expectation of consumers and mental health professionals in community-based residential facilities of Ghana. BMC Psychiatry 2020, 20, 355. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, J.D.; E Drake, R.; Bond, G.R. Economic, Labor, and Regulatory Moderators of the Effect of Individual Placement and Support Among People with Severe Mental Illness: A Systematic Review and Meta-analysis. Schizophr. Bull. 2018, 44, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Gmitroski, T.; Bradley, C.; Heinemann, L.; Liu, G.; Blanchard, P.; Beck, C.; Mathias, S.; Leon, A.; Barbic, S.P. Barriers and facilitators to employment for young adults with mental illness: A scoping review. BMJ Open 2018, 8, e024487. [Google Scholar] [CrossRef]
- Whittemore, R.; Knafl, K. The integrative review: Updated methodology. J. Adv. Nurs. 2005, 52, 546–553. [Google Scholar] [CrossRef]
- Hopia, H.; Latvala, E.; Liimatainen, L. Reviewing the methodology of an integrative review. Scand. J. Caring Sci. 2016, 30, 662–669. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Mental Health. Mental Illness. 2018. Available online: https://www.nimh.nih.gov/health/statistics/mental-illness.shtml (accessed on 15 December 2020).
- Pratt, L.A. Characteristics of Adults with Serious Mental Illness in the United States Household Population in 2007. Psychiatr. Serv. 2012, 63, 1042–1046. [Google Scholar] [CrossRef] [PubMed]
- Pearson, A.; White, H.; Bath-Hextall, F.; Apostolo, J.; Salmond, S.; Kirkpatrick, P. Methodology for JBI mixed methods systematic reviews. Joanna Briggs Inst. Rev. Man. 2014, 1, 5–34. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. On behalf of the PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- The Joanna Briggs Institute (JBI). Critical Appraisal Tools. 2017 [cited 2017 June 19]. Available online: http://joannabriggs.org/research/critical-appraisal-tools.html (accessed on 19 June 2021).
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Fossey, E.; Harvey, C.; McDermott, F.; Davidson, L. Understanding and Evaluating Qualitative Research. Aust. N. Z. J. Psychiatry 2002, 36, 717–732. [Google Scholar] [CrossRef]
- Asher, L.; Hanlon, C.; Birhane, R.; Habtamu, A.; Eaton, J.; Weiss, H.A.; Patel, V.; Fekadu, A.; De Silva, M. Community-based rehabilitation intervention for people with schizophrenia in Ethiopia (RISE): A 12 month mixed methods pilot study. BMC Psychiatry 2018, 18, 250. [Google Scholar] [CrossRef] [PubMed]
- Brooke-Sumner, C.; Lund, C.; Selohilwe, O.; Petersen, I. Community-based psychosocial rehabilitation for schizophrenia service users in the north west province of South Africa: A formative study. Soc. Work. Ment. Health 2016, 15, 249–283. [Google Scholar] [CrossRef]
- Brooke-Sumner, C.; Selohilwe, O.; Mazibuko, M.S.; Petersen, I. Process Evaluation of a Pilot Intervention for Psychosocial Rehabilitation for Service Users with Schizophrenia in North West Province, South Africa. Community Ment. Health J. 2018, 54, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Browne, D.J.; Waghorn, G. Employment services as an early intervention for young people with mental illness. Early Interv. Psychiatry 2010, 4, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Burns, T.; White, S.J.; Catty, J. Individual placement and support in Europe: The EQOLISE trial. Int. Rev. Psychiatry 2018, 20, 498–502. [Google Scholar] [CrossRef]
- Catty, J.; Lissouba, P.; White, S.; Becker, T.; Drake, R.E.; Fioritti, A.; Knapp, M.; Lauber, C.; Rössler, W.; Tomov, T.; et al. Predictors of employment for people with severe mental illness: Results of an international six-centre randomised controlled trial. Br. J. Psychiatry 2008, 192, 224–231. [Google Scholar] [CrossRef]
- Chang, B.-H.; Chen, B.-W.; Beckstead, J.W.; Yang, C.-Y. Effects of a music-creation programme on the anxiety, self-esteem, and quality of life of people with severe mental illness: A quasi-experimental design. Int. J. Ment. Health Nurs. 2018, 27, 1066–1076. [Google Scholar] [CrossRef]
- Chiu, M.Y.L.; Ho, W.W.N.; Lo, W.T.L.; Yiu, M.G.C. Operationalization of the SAMHSA model of recovery: A quality of life perspective. Qual. Life Res. 2009, 19, 1–13. [Google Scholar] [CrossRef]
- Clements, K. Participatory action research and photovoice in a psychiatric nursing/clubhouse collaboration exploring recovery narrative. J. Psychiatr. Ment. Health Nurs. 2012, 19, 785–791. [Google Scholar] [CrossRef]
- Crain, M.; Penhale, C.; Newstead, C.; Thomson, L.; Heah, T.; Barclay, K. The contribution of IPS to recovery from serious mental illness: A case study. Work 2009, 33, 459–464. [Google Scholar] [CrossRef]
- De Heer-Wunderink, C.; Visser, E.; Sytema, S.; Wiersma, D. Social Inclusion of People With Severe Mental Illness Living in Community Housing Programs. Psychiatr. Serv. 2012, 63, 1102–1107. [Google Scholar] [CrossRef]
- Fenner, P.; Ryan, B.; Latai, L.; Percival, S. Art making and the promotion of wellbeing in Samoa—Participants’ lived experience of a recovery oriented intervention. Arts Health 2018, 10, 124–137. [Google Scholar] [CrossRef]
- Harpaz-Rotem, I.; Rosenheck, R.A.; Desai, R. Residential treatment for homeless female veterans with psychiatric and substance use disorders: Effect on 1-year clinical outcomes. J. Rehabil. Res. Dev. 2011, 48, 891–900. [Google Scholar] [CrossRef]
- Hultqvist, J.; Markström, U.; Tjörnstrand, C.; Eklund, M. Quality of life among people with psychiatric disabilities attending community-based day centres or Clubhouses. Scand. J. Caring Sci. 2018, 32, 1418–1427. [Google Scholar] [CrossRef] [PubMed]
- Hultqvist, J.; Markström, U.; Tjörnstrand, C.; Eklund, M. Programme characteristics and everyday occupations in day centres and clubhouses in Sweden. Scand. J. Occup. Ther. 2016, 24, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Iancu, S.C.; Zweekhorst, M.B.M.; Veltman, D.J.; Van Balkom, A.J.L.M.; Bunders, J.F.G. Mental health recovery on care farms and day centres: A qualitative comparative study of users’ perspectives. Disabil. Rehabil. 2013, 36, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, Y.; Coyle, C.; Shank, J.; Messina, E.; Porter, H. Leisure-Generated Meanings and Active Living for Persons with Mental Illness. Rehabil. Couns. Bull. 2013, 57, 46–56. [Google Scholar] [CrossRef]
- Ketch, R.A.; Rubin, R.T.; Baker, M.R.; Sones, A.C.; Ames, D. Art appreciation for veterans with severe mental illness in a VA Psychosocial Rehabilitation and Recovery Center. Arts Health 2015, 7, 172–181. [Google Scholar] [CrossRef][Green Version]
- Kilian, R.; Lauber, C.; Kalkan, R.; Dorn, W.; Rössler, W.; Wiersma, D.; Van Buschbach, J.T.; Fioritti, A.; Tomov, T.; Catty, J.; et al. The relationships between employment, clinical status, and psychiatric hospitalisation in patients with schizophrenia receiving either IPS or a conventional vocational rehabilitation programme. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 47, 1381–1389. [Google Scholar] [CrossRef] [PubMed]
- Koletsi, M.; Niersman, A.; Van Busschbach, J.T.; Catty, J.; Becker, T.; Burns, T.; Fioritti, A.; Kalkan, R.; Lauber, C.; Rössler, W.; et al. Working with mental health problems: Clients’ experiences of IPS, vocational rehabilitation and employment. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 961–970. [Google Scholar] [CrossRef]
- Lee, C.C.; Liem, S.K.; Leung, J.; Young, V.; Wu, K.; Kenny, K.K.W.; Yuen, S.K.; Lee, W.F.; Leung, T.; Shum, M.; et al. From deinstitutionalization to recovery-oriented assertive community treatment in Hong Kong: What we have achieved. Psychiatry Res. 2015, 228, 243–250. [Google Scholar] [CrossRef]
- Lindström, M.; Hariz, G.-M.; Bernspång, B. Dealing with Real-Life Challenges: Outcome of a Home-Based Occupational Therapy Intervention for People with Severe Psychiatric Disability. OTJR Occup. Particip. Health 2011, 32, 5–14. [Google Scholar] [CrossRef]
- López-Navarro, E.; Del Canto, C.; Belber, M.; Mayol, A.; Fernández-Alonso, O.; Lluis, J.; Munar, E.; Chadwick, P. Mindfulness improves psychological quality of life in community-based patients with severe mental health problems: A pilot randomized clinical trial. Schizophr. Res. 2015, 168, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Luk, A.L. Investigating the long-term effects of a psychiatric rehabilitation programme for persons with serious mental illness in the community: A follow-up study. J. Clin. Nurs. 2011, 20, 2712–2720. [Google Scholar] [CrossRef]
- Malinovsky, I.; Lehrer, P.; Silverstein, S.M.; Shankman, S.A.; O’Brien, W.; Samuelson, T.; van Nostrand, G. An empirical evaluation of recovery transformation at a large community psychiatric rehabilitation organization. Psychol. Serv. 2013, 10, 428–441. [Google Scholar] [CrossRef] [PubMed]
- Mizock, L.; Russinova, Z.; DeCastro, S. Recovery Narrative Photovoice: Feasibility of a Writing and Photography Intervention for Serious Mental Illnesses. Psychiatr. Rehabil. J. 2015, 38, 279–282. [Google Scholar] [CrossRef]
- Mizock, L.; Russinova, Z.; Shani, R. New roads paved on losses: Photovoice perspectives about recovery from mental illness. Qual. Health Res. 2014, 24, 1481–1491. [Google Scholar] [CrossRef] [PubMed]
- Panczak, A.; Pietkiewicz, I. Work activity in the process of recovery—An interpretive phenomenological analysis of the experiences of people with a schizophrenia spectrum diagnosis. Psychiatr. Pol. 2016, 50, 805–826. [Google Scholar] [CrossRef] [PubMed]
- Raeburn, T.; Schmied, V.; Hungerford, C.; Cleary, M. The use of social environment in a psychosocial clubhouse to facilitate recovery-oriented practice. BJPsych Open 2016, 2, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Salyers, M.P.; McGuire, A.B.; Kukla, M.; Fukui, S.; Lysaker, P.; Mueser, K.T. A Randomized Controlled Trial of Illness Management and Recovery with an Active Control Group. Psychiatr. Serv. 2014, 65, 1005–1011. [Google Scholar] [CrossRef]
- Svanberg, J.; Gumley, A.; Wilson, A. How do social firms contribute to recovery from mental illness? A qualitative study. Clin. Psychol. Psychother. 2010, 17, 482–496. [Google Scholar] [CrossRef]
- Swildens, W.; van Busschbach, J.T.; Michon, H.; Kroon, H.; Koeter, M.W.J.; Wiersma, D.; van Os, J. Effectively Working on Rehabilitation Goals: 24-Month Outcome of a Randomized Controlled Trial of the Boston Psychiatric Rehabilitation Approach. Can. J. Psychiatry 2011, 56, 751–760. [Google Scholar] [CrossRef]
- Tjörnstrand, C.; Bejerholm, U.; Eklund, M. Participation in day centres for people with psychiatric disabilities: Characteristics of occupations. Scand. J. Occup. Ther. 2011, 18, 243–253. [Google Scholar] [CrossRef]
- Tsang, A.W.K.; Ng, R.M.K.; Yip, K.C. A six-month prospective case-controlled study of the effects of the clubhouse rehabilitation model on Chinese patients with chronic schizophrenia. East Asian Arch. Psychiatry 2010, 20, 23. [Google Scholar]
- Tondora, J.; O’Connell, M.; Miller, R.; Dinzeo, T.; Bellamy, C.; Andres-Hyman, R.; Davidson, L. A clinical trial of peer-based culturally responsive person-centered care for psychosis for African Americans and Latinos. Clin. Trials 2010, 7, 368–379. [Google Scholar] [CrossRef] [PubMed]
- Twamley, E.W.; Vella, L.; Burton, C.Z.; Becker, D.R.; Bell, M.D.; Jeste, D.V. The efficacy of supported employment for middle-aged and older people with schizophrenia. Schizophr. Res. 2012, 135, 100–104. [Google Scholar] [CrossRef]
- Waghorn, G.; Dias, S.; Gladman, B.; Harris, M. Measuring what matters: Effectiveness of implementing evidence-based supported employment for adults with severe mental illness. Int. J. Ther. Rehabil. 2015, 22, 411–420. [Google Scholar] [CrossRef]
- Whitley, R.; Harris, M.; Fallot, R.D.; Berley, R.W. The active ingredients of intentional recovery communities: Focus group evaluation. J. Ment. Health 2008, 17, 173–182. [Google Scholar] [CrossRef]
- Zemore, S.E.; Kaskutas, L.A. Services received and treatment outcomes in day-hospital and residential programs. J. Subst. Abus. Treat. 2008, 35, 232–244. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhou, Y.; Zhou, R.; Li, W.; Lin, Y.; Yao, J.; Chen, J.; Shen, T. Controlled trial of the effectiveness of community rehabilitation for patients with schizophrenia in Shanghai, China. Shanghai Arch. Psychiatry 2015, 27, 167–174. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Stages | Search Terms and Keywords |
|---|---|
| Stage 1 (initial search in MEDLINE and EMBASE) | (Disabilit* or “psychosocial disability” or Adult or “mental disorders” or “mental illness” or “mental condition”).mp. AND (“Social Support” or “Individual Support” or “disability support” or “social inclusion” or integration or “community acceptance” or participation).mp. AND (“nursing homes” or “residential facilities” or “residential care” or “rehabilitation centers” or “community rehabilitation” or “residential program” or “residential care” or institutions or residential treatment).mp. AND (“service model” or “service typology” or rehabilitation or rehabilitat * or “disabled persons” or vocational or “psychosocial support” or or “psychosocial deprivation”).mp. AND (recovery or effectiv * or “patient reported” or “outcome measures” or “treatment outcome” or “patient outcome” or assessment or functioning or “quality of life” or coping or “patient-centered care”).mp |
| Stage 2 (search across CINAHL, Web of Science, Scopus, and PsycINFO) | (Disabilit * or “psychosocial disability” or Adult or “ental disorders” or “mental illness” or “mental condition”).mp. AND (“social support” or “individual support” or “disability support” or “social inclusion” or integration or “community acceptance” or participation).mp. AND (“nursing homes” or “residential facilities” or “residential care” or “rehabilitation centers” or “community rehabilitation” or “residential program” or “residential care” or institutions or residential treatment).mp. AND (“service model” or “service typology” or rehabilitation or rehabilitat * or “disabled persons” or vocational or “psychosocial support” or or “psychosocial deprivation”).mp. AND (recovery or effectiv * or “patient reported” or “outcome measures” or “treatment outcome” or “patient outcome” or assessment or functioning or “quality of life” or coping or “patient-centered care”).mp |
| Stage 3 | Hand searching the reference list |
| Papers | Objectives | Setting | Age/Gender | Participants | Study Design/Methods | Data Collection Instrument | Analysis | Q+ | Summary of Article |
|---|---|---|---|---|---|---|---|---|---|
| Asher, Hanlon [24] | The acceptability and feasibility of CBR in practice as well as how CBR may improve functioning among people with schizophrenia | Ethiopia | Mean age = 39.5; males and females | Schizophrenia | Quasi-experimental design/Mixed methods |
| Thematic analysis and descriptive statistics | H | CBR program has the capacity to improve functioning of people with schizophrenia |
| Brooke-Sumner, Lund [25] | To develop a community-based psychosocial rehabilitation program for service users with schizophrenia | South Africa | Maximum age = 45; females | Schizophrenia | Quasi-experimental design/Qualitative | • In-depth interviews (IDIs) | Thematic analysis | H | The program improved the lives of service users with schizophrenia—self-esteem, social support, illness knowledge, self-care, and contribution to their households |
| Brooke-Sumner, Selohilwe [26] | Investigated a non-specialist-delivered program for psychosocial rehabilitation for service users with schizophrenia in a low-resource South African setting | South Africa | Age range = 21–44; males and females | Schizophrenia | Quasi-experimental design/Mixed methods |
| Thematic analysis and inferential statistics | H | The program achieved reduction in ISMI assessment as well as improved psychosocial well-being of service users with schizophrenia |
| Browne and Waghorn [27] | to retrospectively assess the implementation of IPS practices and youth employment outcomes | New Zealand | Age range = 16–25; males and females | Affective (including comorbid anxiety), bipolar affective disorder, generalized anxiety disorder | Observational design (retrospective case study)/Quantitative | • Case review | Descriptive statistics | M | The IPS program was effective in terms of the proportion of young clients commencing competitive employment, and duration of longest job held |
| Burns, White [28] | The acceptability and effectiveness of IPS in Europe | Five European countries | Mean age = 38 | schizophrenia or schizoaffective disorder bipolar disorder | Randomized controlled trial/Quantitative | • Questionnaire | Inferential statistics | High | Individual Placement and Support (IPS) was approximately two-fold more effective than vocational services in returning to open employment |
| Catty, Lissouba [29] | Determine which patients with severe mental illness do well in vocational services and which process and service factors are associated with better outcomes | Six European centres | Age range = 18–local retirement age; males and females | Schizophrenia | Randomized controlled trial/Quantitative |
| Inferential statistics | H | The IPS services were more effective than the vocational services for every vocational outcome |
| Chang, Chen [30] | Investigated the effect of a music-creation group program on the anxiety, self-esteem, and quality of life of patients with SMI | Taiwan | Age range 20–65; males and females | Schizophrenia or affective disorders | Quasi-experimental design/Quantitative |
| Inferential statistics | H | Participating in a structured music-creation intervention improved the psychological well-being, self-esteem, quality of life and social relationship of consumers with SMI |
| Chiu, Ho [31] | To test empirically the Substance Abuse and Mental Health Services Administration (SAMHSA) recovery model | Hong Kong | Mean age = 41.6; males and females | Schizophrenia spectrum disorder | Cross-sectional/Quantitative |
| Inferential statistics | H | Psychosocial symptoms, respect, resilience, and empowerment were significant contributors of recovery |
| Clements [32] | To pilot a PAR and photovoice project to facilitate discussions about recovery based on personal and local experience | Canada | Participatory action research/Qualitative (e.g., photovoice) | Photo/text pieces, other ‘readers’ or audiences | Recovery photo gallery | H | Photovoice proved as a useful research method for the construction of local knowledge about recovery and as a vehicle for sharing that knowledge | ||
| Crain, Penhale [33] | Application of IPS in a Canadian community mental health team through the study of a competitively employed individual and support network | Canada | Mean age = 42; males | Schizophrenia | Instrumental case study/Qualitative | • In-depth interviews (IDIs) | Thematic analysis | H | The IPS program had positive outcomes through securing and maintaining job, changing perceptions, self-confidence, social skills and recovery |
| De Heer-Wunderink, Visser [34] | Investigated levels of social inclusion among service users of two types of psychiatric community housing programs in the Netherlands | Netherlands | Mean age = 44; males and females | Schizophrenia, anxiety or depression, personality disorder | Cross-sectional design/Quantitative |
| Descriptive and inferential statistics | H | Supported independent living programs seemed to positively influence the level of social inclusion among service users compared with residential programs |
| Fenner, Ryan [35] | Analysed what consumers and staff reported at the end of the project | Samoa | Interpretive phenomenological design/Qualitative | • Focus group discussion | IPA | H | Art making positively impacts on consumers senses of identity and independence and demonstrates their talents and capacities | ||
| Harpaz-Rotem, Rosenheck [36] | Observational data comparing 1 year clinical outcomes among women who received RT services and those who did not | USA | Psychiatric/substance abuse problems | Quasi-experimental design/Quantitative |
| Descriptive and inferential statistics | H | Placement in residential treatment was associated with significantly improved clinical outcomes in a variety of domains | |
| Hultqvist, Markstrom [37] | Comparing users of two approaches to psychosocial rehabilitation in Sweden, community-based mental health day centres (DCs) and clubhouses | Sweden | Mean age = 48.7; males and females | Psychoses, mood and anxiety disorders, autism/neuropsychiatric disorders | Quasi-experimental design/Quantitative |
| Descriptive and inferential statistics | The study showed that visiting clubhouses appears to be more beneficial for improved QOL in a longer-term perspective | |
| Hultqvist, Markström [38] | Compared DC and clubhouses, concerning the users’ perceptions of unit and program characteristics, and aspects of everyday occupations in terms of engagement and satisfaction | Sweden | Mean age = 48.7; males and females | Psychoses, mood and anxiety disorders, autism/neuropsychiatric disorders | Combined cross-sectional and longitudinal comparative study/Quantitative |
| Descriptive and inferential statistics | The users of clubhouse performed better than day centre users various on social network sub-scales (feeling valued by others, feelings of inclusion and belonging to a group) | |
| Iancu, Zweekhorst [39] | Analysed and compared experiences of recovery on prevocational services, in order to assess if users make progress towards recovery, relative to a staged recovery model | Netherlands | Mean age = 42.5; males and females | Schizophrenia and personality disorders, depressive and anxiety disorders | Interpretive phenomenological design/Qualitative | • Semi-structured interviews | Thematic analysis | H | The prevocational services provide the needed services for people with mental disorders who desire to engage in recovery (create strong internal motivation for change) |
| Iwasaki, Coyle [40] | The role of leisure-generated meanings (LGMs) experienced by culturally diverse individuals with mental illness in potentially helping them to better cope with stress, adjust and recover | USA | Mean age = 48; males and females | Bipolar disorder, major depression, schizophrenia, bipolar/schizophrenic, schizoaffective disorder, substance abuse, panic disorder, borderline personality | Cross-sectional/Quantitative |
| Descriptive and inferential statistics | H | Leisure can contribute to stress-coping, recovery, adjustment, and active living for individuals with mental illness |
| Ketch, Rubin [41] | Art appreciation for veterans with severe mental illness in a VA Psychosocial Rehabilitation and Recovery Centre | USA | Quasi-experimental design/Qualitative | • Photos and interviews | Thematic analysis | H | The program had positive effects on mood, self-esteem, socialization community participation and recovery process of veterans with SMI | ||
| Kilian, Lauber [42] | Analyses the relationships between employment hours, psychopathological symptoms and the days of inpatient treatment detected | Six European centres | Mean age = 37.8; males and females | Schizophrenia/schizoaffective disorders, bipolar disorder | Randomized controlled trial/Quantitative |
| Descriptive and inferential statistics | M | IPS intervention through its effect on the time spent in competitive employment leads to reduced need for psychiatric inpatient care |
| Koletsi, Niersman [43] | Explore clients’ experiences of the support received from their IPS or vocational service workers and the perceived impact of work on clients’ lives | Six European centres | Age range = 18–57; males and females | Schizophrenia/schizoaffective disorders, bipolar disorder | Randomized controlled trial/Qualitative | • Semi-structured interviews | Thematic analysis | H | The IPS program improved financial stability, illness, social life, increased self-esteem, integration into society, self-improvement, coping strategy and reduced loneliness |
| Lee, Liem [44] | Explored the effectiveness of Assertive Community Treatment (ACT) for severely ill mental patients during a period of rapid deinstitutionalization in Hong Kong | Hong Kong | Age range = 18–65; males and females | Psychotic disorders | Flanking historical control design/Quantitative |
| Descriptive and inferential Statistics | H | The ACT had positive effect over and above the conventional treatment models—outcome parameters (bed days, readmission episodes, missed psychiatric appointments, BPRS and quality of life) improved |
| Lindstrom, Hariz [45] | To evaluate clients’ activities of daily living (ADL) ability and health factors outcomes following their participation in occupation-centred interventions in home and community settings | Sweden | Mean age = 48; males and females | Schizophrenia, schizoaffective disorder, bipolar disorder, Asperger syndrome, obsessive compulsive disorder | Quasi-experimental design/Quantitative |
| Descriptive and inferential Statistics | H | The occupational therapy services integrated in to sheltered or supported housing achieved positive lifestyle, meaningful occupations and participation in society |
| Lopez-Navarro, Del Canto [46] | The effectiveness of group mindfulness-based intervention (MBI) in patients diagnosed with severe mental illness | Balearic Islands | Mean age = 38.44 | Schizophrenia, bipolar disorder, delusional disorder | Randomized controlled trial/Quantitative |
| Descriptive and inferential statistics | H | Mindfulness intervention in rehabilitation has potential to enhance quality of life and reduce negative symptoms |
| Luk [47] | Investigate the long-term effects of a holistic care program for the rehabilitation of persons with serious mental illness | Hong Kong | Mean age = 35; males and females | Schizophrenia, manic depressive, depression | Cross-sectional/Quantitative |
| Descriptive and inferential statistics | H | The program is effective to provide positive changes—support, encouragement, self-confidence, spiritual assistance and reflection of values |
| Malinovsky, Lehrer [48] | Evaluate the effectiveness of a recovery-oriented transformation carried out by a large, private, not-for-profit psychiatric rehabilitation organization serving individuals with SM | USA | Mean age = 46.42; males and females | Schizophrenia, mood disorder (unipolar/bipolar), other psychotic disorder | Longitudinal study/Quantitative |
| Descriptive and inferential statistics | H | Recovery-oriented services are effective to reduce hospitalizations and improve quality of life |
| Mizock, Russinova [49] | Describe the development and feasibility of the recovery narrative photovoice intervention | USA | Serious mental illnesses | Community-based participatory research/Quantitative |
| Descriptive statistics | The program has the potential to facilitate recovery-related outcomes, including empowerment, positive identity, and community integration | ||
| Mizock, Russinova [50] | Explore the meaning of recovery for individuals with serious mental illness | USA | Serious mental illness | Community-based participatory research/Qualitative | • Photos and archival data | Thematic analysis | H | The study identify several internal and external recovery strategies and outcomes | |
| Panczak and Pietkiewicz [51] | Explore personal experiences of people employed in Vocational Development Centres | Poland | Age range = 28–58; males and females | Schizophrenia spectrum disorders | Interpretative phenomenological design/Qualitative | • Semi-structured interviews | Consecutive analytical | H | The program improved the economic and social well-being of people with schizophrenia—economic empowerment, empowerment, functioning and social inclusion |
| Raeburn, Schmied [52] | Explore how recovery practices are implemented in a psychosocial clubhouse | Australia | Mean age = 47; males and females | Schizophrenia, bipolar disorder or schizoaffective disorder | Case study/Qualitative |
| Theoretical thematic analysis | H | The psychosocial clubhouse is a community that provide opportunity to participate in a personal recovery journey |
| Salyers, McGuire [53] | To rigorously test Illness Management and Recovery (IMR) against an active control group in a sample that included veterans | USA | Mean age = 47.7; males and females | Schizophrenia, schizoaffective disorder | Randomized controlled trial/Quantitative |
| Descriptive and inferential statistics | H | Improved significantly in a number of domains related to illness management—symptoms, psychosocial functioning, self-rated illness management, and emergency department use |
| Svanberg, Gumley [54] | Explore the experience of recovery from mental illness in the context of two emerging social firms | Scotland | Age range = 19–64; males and females | Bipolar disorder, depression, psychosis, anxiety, addictions | Social constructionist (grounded theory)/Qualitative | • Open-ended interview questions | Thematic analysis | H | The social firms are effective to enhance self-confidence, acceptance and inclusion of people with mental illness |
| Swildens, van Busschbach [55] | Investigate the effect of the Boston Psychiatric Rehabilitation (PR) approach on attainment of personal rehabilitation goals, social functioning, empowerment, needs for care, and quality of life in people with severe mental illness (SMI) in the Netherlands | Netherlands | Age = 41 and over; males and females | Schizophrenia or schizoaffective disorder, bipolar disorder, depressive or anxiety disorder, personality, addiction, cognitive disorder | Randomized controlled trial/Quantitative |
| Descriptive and inferential statistics | H | Psychiatric rehabilitation has a significant impact on goal attainment, societal participation and social contacts |
| Tjornstrand, Bejerholm [56] | Gaining knowledge regarding the occupations performed in day centres, in terms of the participants’ descriptions of what they were doing | Sweden | Mean age = 45.3; males and females | Schizophrenia, other psychoses | Interpretative phenomenological design/Qualitative |
| Content analysis | H | The study showed that social interaction and occupations formed the two foundations of the day centres |
| Tsang, Ng [57] | Effects of the ‘clubhouse’ model of rehabilitation on various psychosocial issues for Chinese patients with schizophrenia living in the community | Hong Kong | Mean age = 40.5; males and females | Chronic schizophrenia | longitudinal, case–control and naturalistic design/Quantitative |
| Descriptive and inferential statistics | The program improved the psychological, social relationship and environmental quality of life of participants | |
| Tondora, O’Connell [58] | Rationale, design, and lessons learned during the implementation of a randomized clinical trial testing the effect of using peer facilitative advocates to promote culturally responsive person-centred care planning on QOL variables, community connections, and coping for people of colour with psychotic disorders | USA | Mean age = 43.5; males and females | Schizophrenia, schizoaffective disorder, or affective disorder | Randomized clinical trial/Quantitative |
| Descriptive and inferential statistics | H | The project suggests the need to make cultural modifications, longer engagement period with participants |
| Twamley, Vella [59] | To evaluate the efficacy of supported employment for middle-aged or older people with schizophrenia | USA | Mean age = 51; males and females | Schizophrenia or schizoaffective disorder aged | Randomized controlled trial/Quantitative |
| Descriptive and inferential statistics | H | Individual Placement and Support (IPS) was effective for people with schizophrenia compared with conventional vocational rehabilitation (CVR) |
| Waghorn, Dias [60] | This investigation compared the utility of two approaches to measuring the effectiveness of a supported employment program | Australia | Mean age = 34.1; males and females | Schizophrenia, schizoaffective disorder, schizophreniform disorders, bipolar affective disorder, major depression and anxiety disorders | Non-randomized trial/Quantitative |
| Descriptive and inferential statistics | H | The non-RCT IPS cohort were more effective in gaining competitive employment compared with RCT IPS |
| Whitley, Harris [61] | Explore and elucidate whether components of these communities appeared to assist recovery from the point of view of consumers, and if so which were the most important factors | USA | Grounded theory approach/Qualitative |
| Grounded theory approach | H | The community is perceived as a place of safety, surrogate family, socialization and individual growth | ||
| Zemore and Kaskutas [62] | explores whether services received differed by program modality (i.e., day hospital vs. residential) | USA | Age = ≥18; males and females | Alcohol-dependent only, drug-dependent only, alcohol and drug dependent | Randomized controlled trial/Quantitative |
| Descriptive and inferential statistics | H | Residential participants showed greater participation in sober recreational events and informal socialization with peers. Higher participation in optional or extracurricular 12-step meetings was associated with better treatment outcomes |
| Zhou, Zhou [63] | Effectiveness of the rehabilitation services provided at the ‘Sunshine Soul Park’ on the psychotic symptoms and social functioning of individuals with schizophrenia | China | Mean age = 39.2; males and females | Schizophrenia | Non-randomized controlled trial/Quantitative |
| Descriptive and inferential statistics | H | The intervention is effective in improving the social functioning of patients with schizophrenia and in helping them understand and manage their illness |
| Global Themes | Organizing Themes | N | Papers |
|---|---|---|---|
| Context or environment for implementing recovery services | Community based | 22 | [24,27,29,32,37,38,40,45,46,47,48,50,51,53,54,55,57,58,59,60,61,63] |
| Residential facilities | 7 | [27,28,29,35,36,41,62] | |
| Home-based care or services | 4 | [33,34,36,45] | |
| Day centre-structured program | 3 | [28,37,56] | |
| Psychiatric day hospital/primary services | 6 | [25,26,30,31,44,57] | |
| Mechanisms for implementing recovery services | Integrated recovery services | 17 | [24,25,26,30,34,40,44,45,46,47,48,53,56,58,61,62,63] |
| Vocational rehabilitation | 18 | [27,28,29,33,34,37,38,39,42,43,51,54,55,56,57,59,60] | |
| Recovery narrative photovoice and art making | 5 | [32,35,41,49,50] | |
| Outcome of recovery services | Psychiatric medication | 10 | [24,25,33,36,42,44,48,53,62,63] |
| Improving functionality | 14 | [24,26,36,37,39,41,43,44,45,48,51,53,55,63] | |
| Reduce symptoms | 11 | [25,30,31,36,42,44,45,46,53,57,63] | |
| Improving physical health and social behaviour | 7 | [24,26,36,45,46,48] | |
| Economic empowerment | 19 | [24,25,26,27,28,29,31,33,34,36,38,42,43,47,51,56,57,59,60] | |
| Household integration | 3 | [24,26,36] | |
| Social inclusion (community integration) | 27 | [24,25,26,30,31,32,33,34,35,37,38,39,41,43,44,45,49,51,52,54,55,56,57,58,61,62,63] | |
| Social support | 7 | [31,33,34,36,39,50,61] | |
| Self-efficacy | 21 | [24,25,26,30,32,33,34,35,38,39,40,43,47,49,50,51,52,54,55,57,61] |
| Recovery Services | Intervention | How to Deliver the Intervention | Process or Outcome |
|---|---|---|---|
| Integrated recovery services | Illness management |
| Antipsychotic medication adherence, improve knowledge, decrease relapse, reducing inpatient and crisis services |
| Mindfulness-based interventions |
| Improving functioning, symptoms and quality of life | |
| Task-sharing or task-shifting approaches |
| Increase access to psychiatric medication, improve physical health and social behaviour, self-efficacy | |
| Home visits concept |
| Household integration, improving self-care or practical skills | |
| Music-creation therapy | • A 90 min music-creation group activity organized weekly for 32 consecutive weeks | Community acceptance, inclusion, empowerment | |
| Active leisure or recreational activities | • Playing sports, opportunity to play games, eat, and socialize, embarking on excursions and relaxation | Social inclusion (community integration, social contacts or social interactions and socialization) | |
| Everyday life rehabilitation |
| Self-efficacy (self-esteem or self-confidence) | |
| Vocational rehabilitation | Individual Placement and Support (IPS) |
| Returning to open employment, gaining competitive employment, economic empowerment, gaining financial literacy skills, financial independence and stability |
| Conventional vocational rehabilitation (e.g., sheltered employment, supported employment enterprises and social firms) | Economic empowerment | ||
| Narrative photovoice and art making | Photovoice |
| Empowerment, community integration, hope, progress in recovery |
| Art making and exhibition |
| Development of new skills, community integration |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badu, E.; O’Brien, A.P.; Mitchell, R. An Integrative Review of Recovery Services to Improve the Lives of Adults Living with Severe Mental Illness. Int. J. Environ. Res. Public Health 2021, 18, 8873. https://doi.org/10.3390/ijerph18168873
Badu E, O’Brien AP, Mitchell R. An Integrative Review of Recovery Services to Improve the Lives of Adults Living with Severe Mental Illness. International Journal of Environmental Research and Public Health. 2021; 18(16):8873. https://doi.org/10.3390/ijerph18168873
Chicago/Turabian StyleBadu, Eric, Anthony Paul O’Brien, and Rebecca Mitchell. 2021. "An Integrative Review of Recovery Services to Improve the Lives of Adults Living with Severe Mental Illness" International Journal of Environmental Research and Public Health 18, no. 16: 8873. https://doi.org/10.3390/ijerph18168873
APA StyleBadu, E., O’Brien, A. P., & Mitchell, R. (2021). An Integrative Review of Recovery Services to Improve the Lives of Adults Living with Severe Mental Illness. International Journal of Environmental Research and Public Health, 18(16), 8873. https://doi.org/10.3390/ijerph18168873