
Effect of Mobile-Based Lifestyle Intervention on Weight Loss among the Overweight and Obese Elderly Population in China: A Randomized Controlled Trial

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Methods
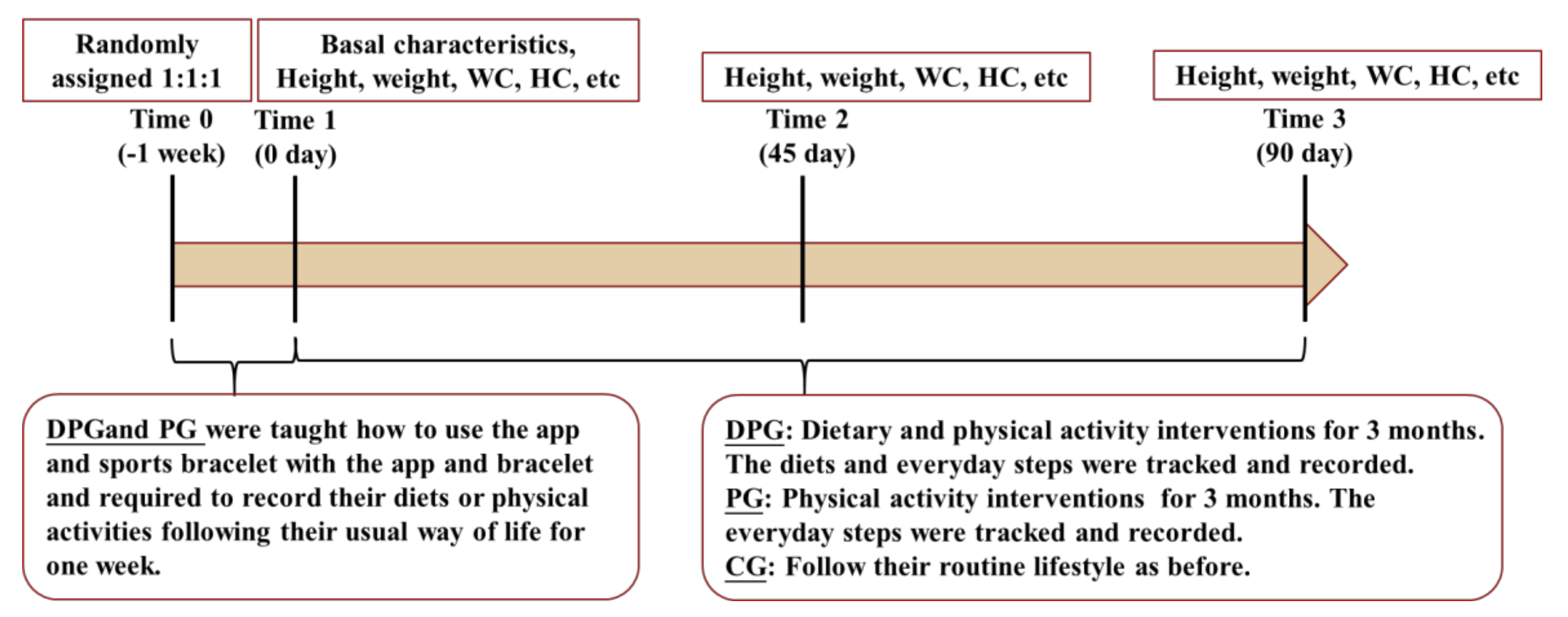
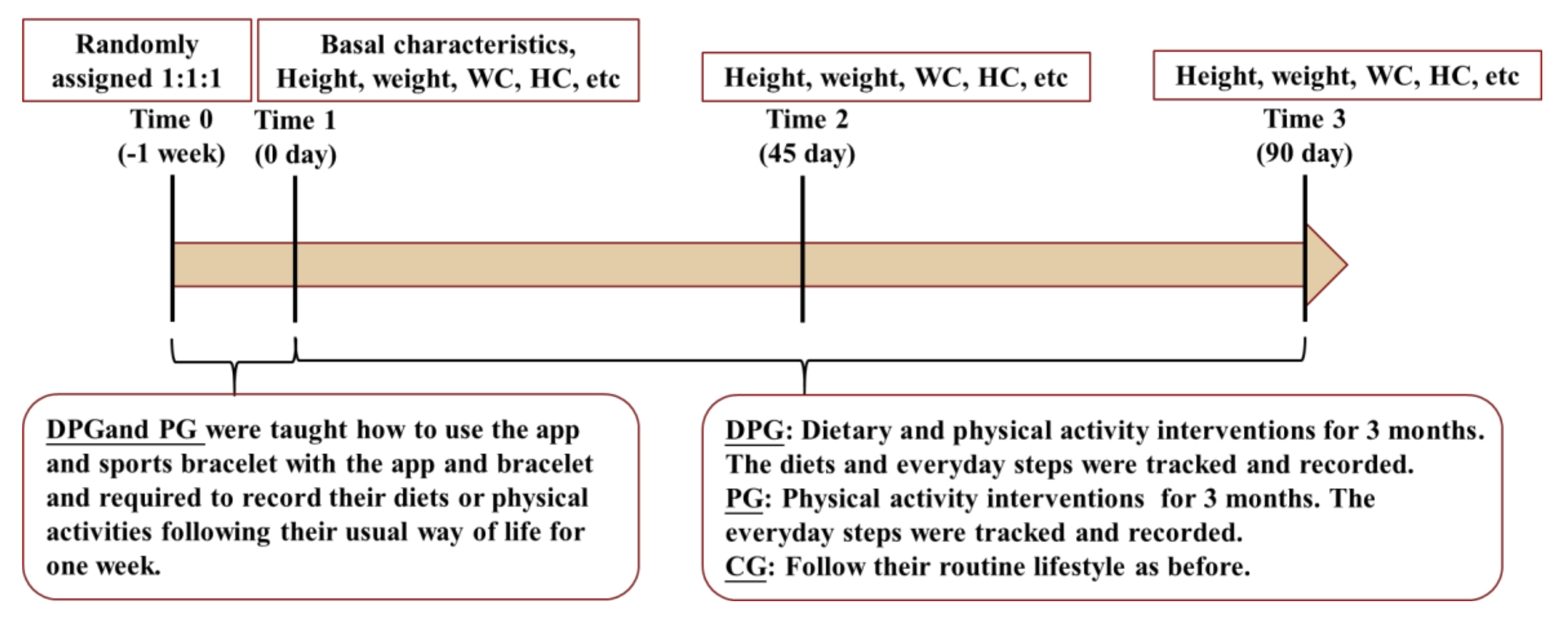
2.1. Study Design
2.2. Participants and Randomization
2.3. Blinding
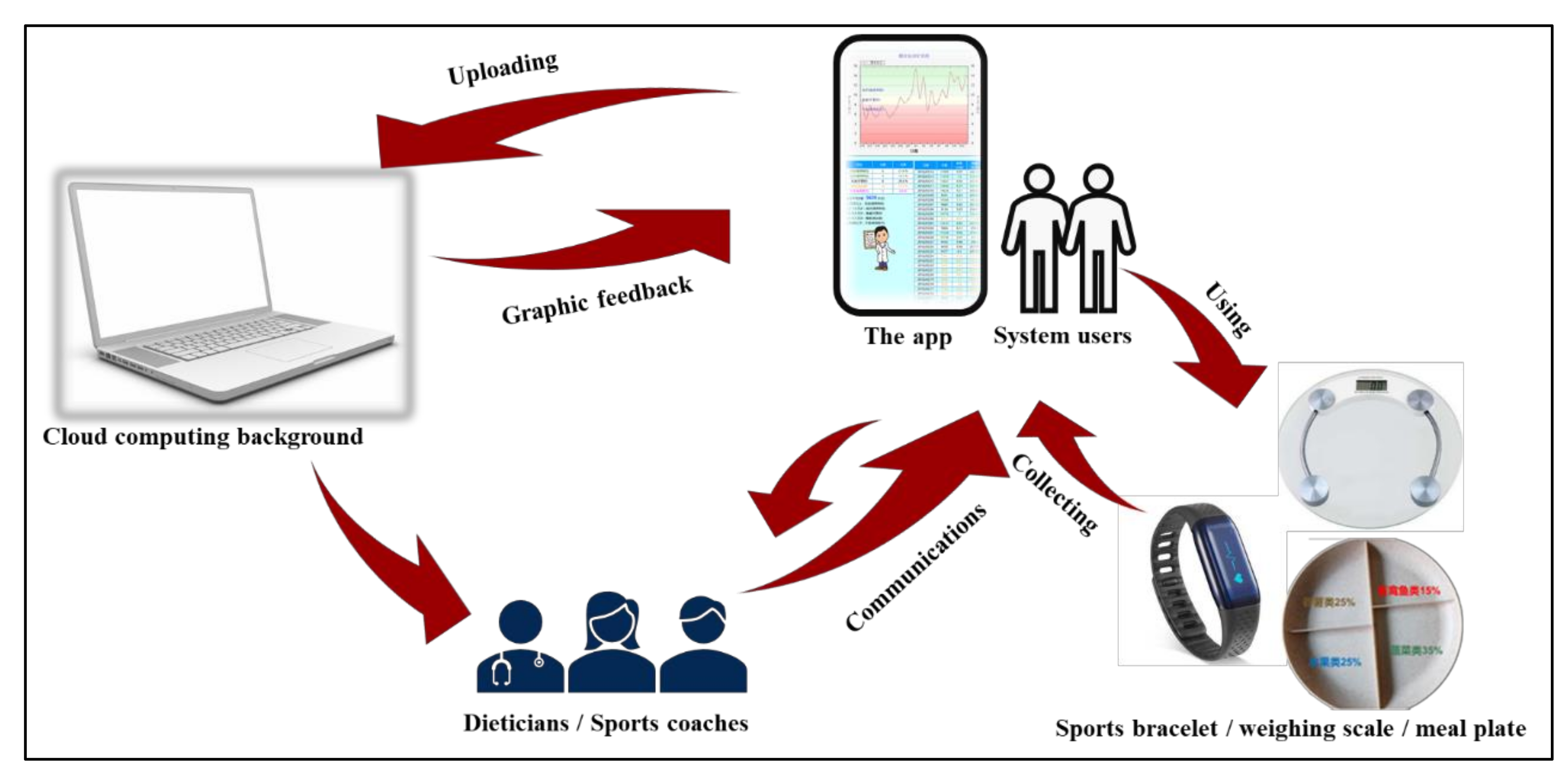
2.4. Mobile-Based Support System
2.5. Intervention
2.6. Study Procedure
2.7. Outcome Measurements
2.8. Statistical Analysis
3. Results
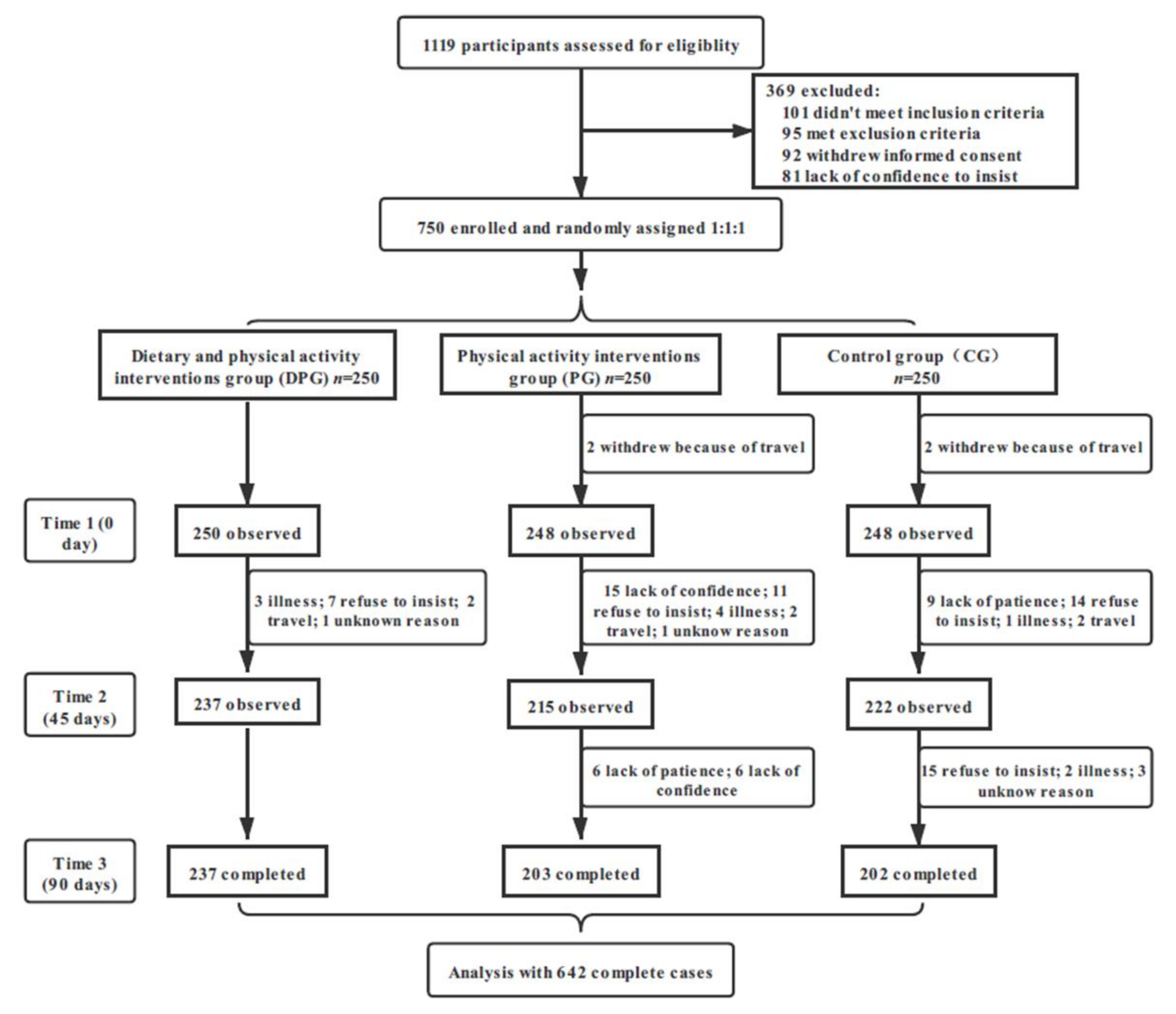
3.1. Participants
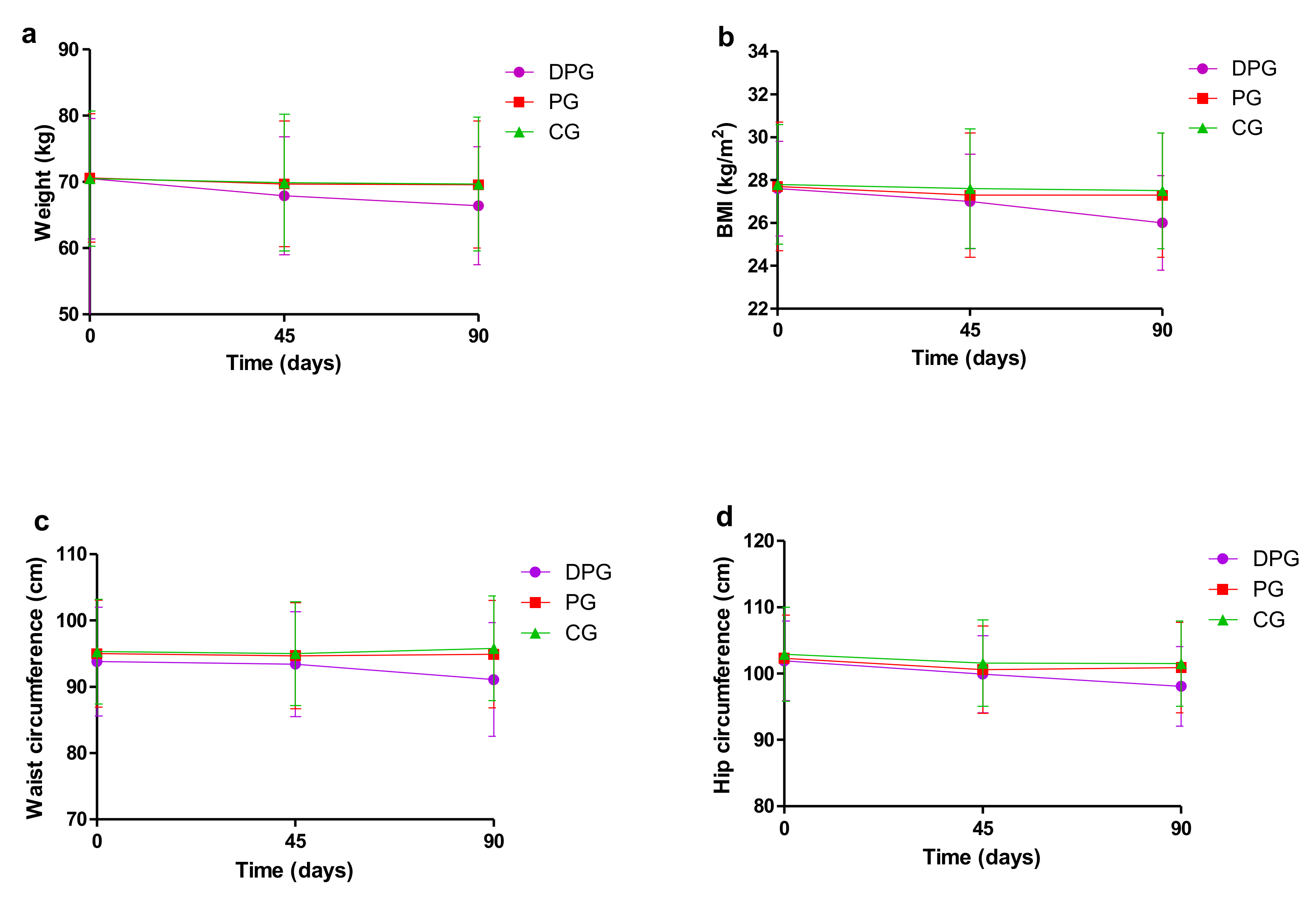
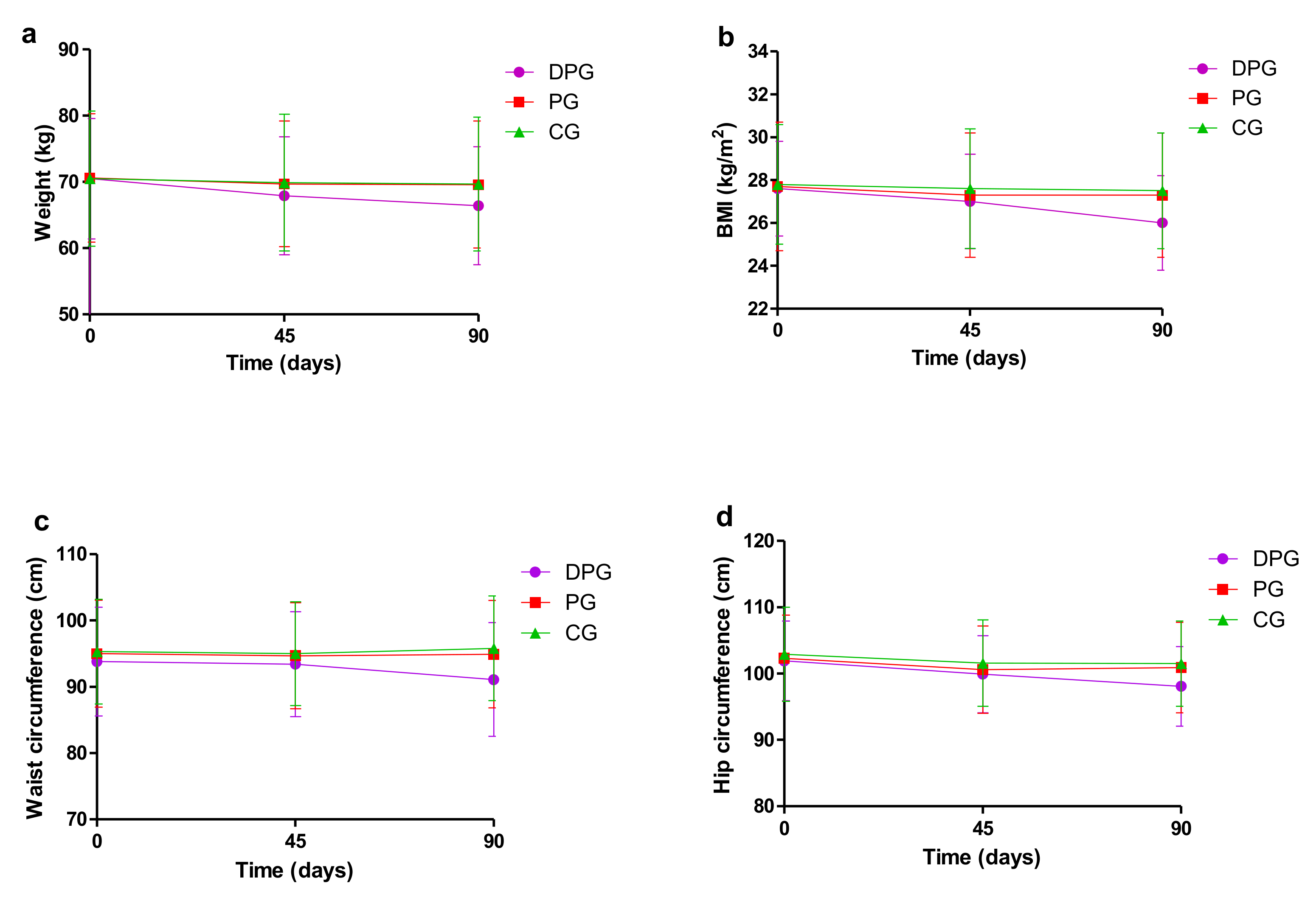
3.2. Weight Outcomes at Three Different Time in Each Group
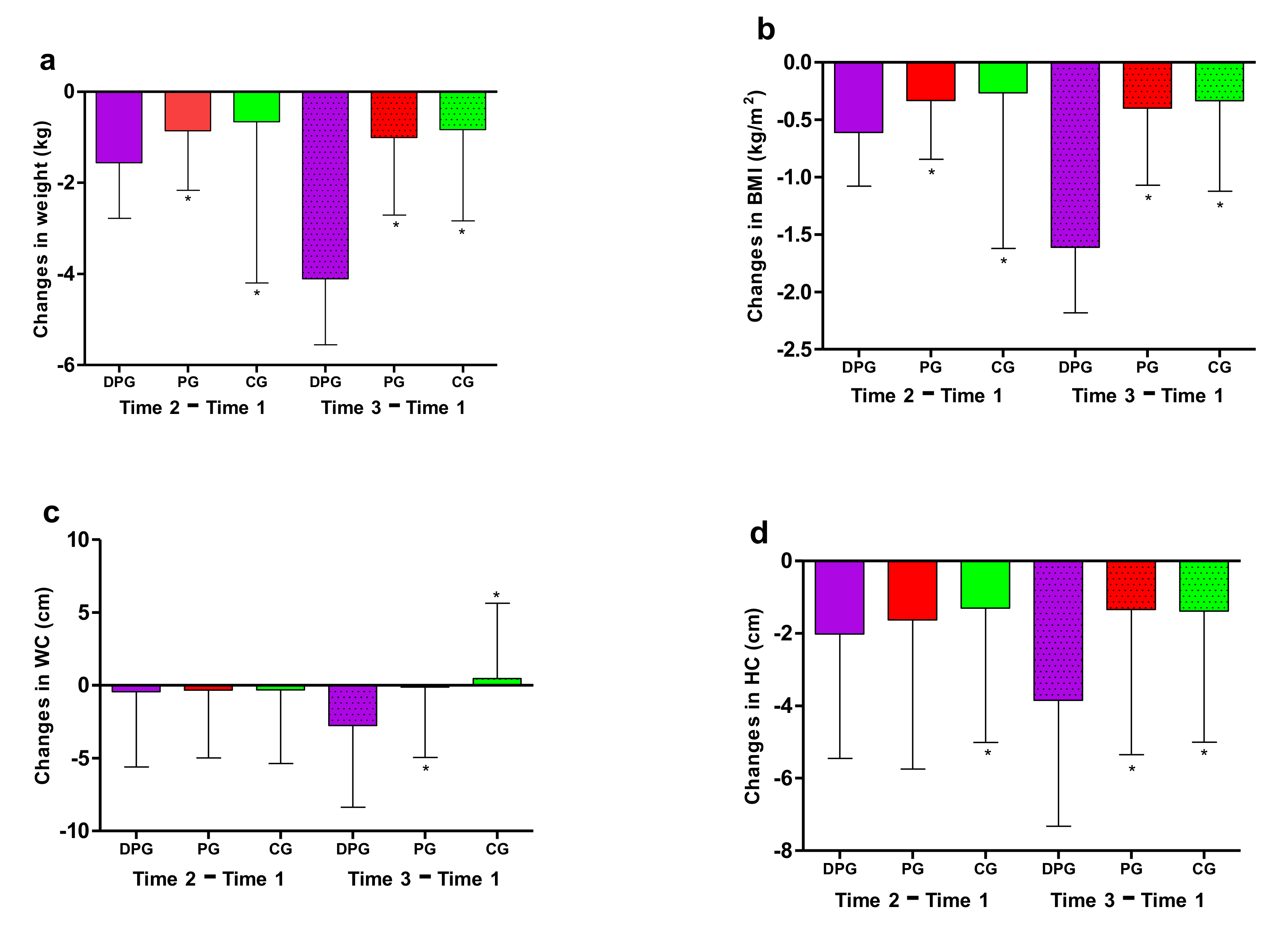
3.3. Outcome Changes between Groups
3.4. Analysis by Subgroups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Global Strategy and Action Plan on Ageing and Health (2016–2020); World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Kontis, V.; Bennett, J.E.; Mathers, C.D.; Li, G.; Foreman, K.; Ezzati, M. Future life expectancy in 35 industrialised countries: Projections with a Bayesian model ensemble. Lancet 2017, 389, 1323–1335. [Google Scholar] [CrossRef] [Green Version]
- Mathus-Vliegen, E.M. Obesity and the Elderly. J. Clin. Gastroenterol. 2012, 46, 533–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haas, K.; Hayoz, S.; Maurer-Wiesner, S. Effectiveness and Feasibility of a Remote Lifestyle Intervention by Dietitians for Overweight and Obese Adults: Pilot Study. JMIR mHealth uHealth 2019, 7, e12289. [Google Scholar] [CrossRef] [Green Version]
- Kopelman, P.G. Obesity as a medical problem. Nat. Cell Biol. 2000, 404, 635–643. [Google Scholar] [CrossRef]
- Kalish, V.B. Obesity in Older Adults. Prim. Care 2016, 43, 137–144. [Google Scholar] [CrossRef]
- Jacobs, E.J.; Newton, C.C.; Wang, Y.; Patel, A.V.; McCullough, M.L.; Campbell, P.T.; Thun, M.J.; Gapstur, S.M. Waist Circumference and All-Cause Mortality in a Large US Cohort. Arch. Intern. Med. 2010, 170, 1293–1301. [Google Scholar] [CrossRef]
- Kahn, S.E.; Hull, R.L.; Utzschneider, K.M. Mechanisms linking obesity to insulin resistance and type 2 diabetes. Nature 2006, 444, 840–846. [Google Scholar] [CrossRef]
- Seravalle, G.; Grassi, G. Obesity and hypertension. Pharmacol. Res. 2017, 122, 1–7. [Google Scholar] [CrossRef]
- Ortega, F.B.; Lavie, C.J.; Blair, S.N. Obesity and Cardiovascular Disease. Circ. Res. 2016, 118, 1752–1770. [Google Scholar] [CrossRef] [Green Version]
- McTigue, K.M.; Hess, R.; Ziouras, J. Obesity in Older Adults: A Systematic Review of the Evidence for Diagnosis and Treatment*. Obesity 2006, 14, 1485–1497. [Google Scholar] [CrossRef]
- Yang, Y.; Shields, G.; Guo, C.; Liu, Y. Executive function performance in obesity and overweight individuals: A meta-analysis and review. Neurosci. Biobehav. Rev. 2018, 84, 225–244. [Google Scholar] [CrossRef] [PubMed]
- Starr, K.N.P.; McDonald, S.R.; Bales, C.W. Obesity and Physical Frailty in Older Adults: A Scoping Review of Lifestyle Intervention Trials. J. Am. Med Dir. Assoc. 2014, 15, 240–250. [Google Scholar] [CrossRef] [Green Version]
- Waters, D.L.; Ward, A.L.; Villareal, D.T. Weight loss in obese adults 65years and older: A review of the controversy. Exp. Gerontol. 2013, 48, 1054–1061. [Google Scholar] [CrossRef] [Green Version]
- Lemamsha, H.; Randhawa, G.; Papadopoulos, C. Prevalence of Overweight and Obesity among Libyan Men and Women. BioMed Res. Int. 2019, 2019, 8531360. [Google Scholar] [CrossRef]
- Han, T.; Tajar, A.; Lean, M.E.J. Obesity and weight management in the elderly. Br. Med. Bull. 2011, 97, 169–196. [Google Scholar] [CrossRef]
- Allegrante, J.P.; Wells, M.T.; Peterson, J.C. Interventions to Support Behavioral Self-Management of Chronic Diseases. Annu. Rev. Public Health 2019, 40, 127–146. [Google Scholar] [CrossRef] [Green Version]
- Jiang, W.; Huang, S.; Ma, S.; Gong, Y.; Fu, Z.; Zhou, L.; Hu, W.; Mao, G.; Ma, Z.; Yang, L.; et al. Effectiveness of companion-intensive multi-aspect weight management in Chinese adults with obesity: A 6-month multicenter randomized clinical trial. Nutr. Metab. 2021, 18, 17. [Google Scholar] [CrossRef]
- Gomez-Marcos, M.A.; Patino-Alonso, C.; Recio-Rodriguez, J.I.; Agudo-Conde, C.; Romaguera-Bosch, M.; Magdalena-Gonzalez, O.; Gomez-Arranz, A.; Mendizabal-Gallastegui, N.; Fernandez-Diez, J.A.; Gomez-Sanchez, L.; et al. Short- and long-term effectiveness of a smartphone application for improving measures of adiposity: A randomised clinical trial—EVIDENT II study. Eur. J. Cardiovasc. Nurs. 2018, 17, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Guo, X.; Zhang, N.; Yan, X.; Li, M.; Zhou, M.; He, H.; Li, Y.; Guo, W.; Zhang, M.; et al. Effect of Mobile-Based Lifestyle Intervention on Body Weight, Glucose and Lipid Metabolism among the Overweight and Obese Elderly Population in China: A Randomized Controlled Trial Protocol. Int. J. Environ. Res. Public Health 2021, 18, 4854. [Google Scholar] [CrossRef]
- Xu, W.; Zhang, H.; Paillard-Borg, S.; Zhu, H.; Qi, X.; Rizzuto, D. Prevalence of Overweight and Obesity among Chinese Adults: Role of Adiposity Indicators and Age. Obes. Facts 2016, 9, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Shi, J.; Wu, Z.; Xie, H.; Yu, Y.; Li, P.; Liu, R.; Jing, L. Changes in chronic disease management among community health centers (CHCs) in China: Has health reform improved CHC ability? Int. J. Health Plan. Manag. 2017, 32, 317–328. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.S.; French, D.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef] [PubMed]
- Cavero-Redondo, I.; Martinez-Vizcaino, V.; Fernandez-Rodriguez, R.; Saz-Lara, A.; Pascual-Morena, C.; Álvarez-Bueno, C. Effect of Behavioral Weight Management Interventions Using Lifestyle mHealth Self-Monitoring on Weight Loss: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 1977. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Sasai, H.; Wakaba, K.; Murakami, S.; Ueda, M.; Yamagata, F.; Sawada, M.; Takekoshi, K. Professional dietary coaching within a group chat using a smartphone application for weight loss: A randomized controlled trial. J. Multidiscip. Health 2018, ume 11, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Oh, B.; Shin, H.-Y. Effect of mHealth With Offline Antiobesity Treatment in a Community-Based Weight Management Program: Cross-Sectional Study. JMIR mHealth uHealth 2020, 8, e13273. [Google Scholar] [CrossRef]
- Lisón, J.F.; Palomar, G.; Mensorio, M.S.; Baños, R.M.; Cebolla-Martí, A.; Botella, C.; Benavent-Caballer, V.; Rodilla, E. Impact of a Web-Based Exercise and Nutritional Education Intervention in Patients Who Are Obese With Hypertension: Randomized Wait-List Controlled Trial. J. Med. Internet Res. 2020, 22, e14196. [Google Scholar] [CrossRef]
- Ahn, J.S.; Lee, H.; Kim, J.; Park, H.; Kim, D.W.; Lee, J.E. Use of a Smartphone App for Weight Loss Versus a Paper-Based Dietary Diary in Overweight Adults: Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e14013. [Google Scholar] [CrossRef]
- Carter, M.C.; Burley, V.; Nykjaer, C.; Cade, J. Adherence to a Smartphone Application for Weight Loss Compared to Website and Paper Diary: Pilot Randomized Controlled Trial. J. Med. Internet Res. 2013, 15, e32. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Stull, K.R.; Fantigrassi, M.; Motel, I. The efficacy of wearable activity tracking technology as part of a weight loss program: A systematic review. J. Sports Med. Phys. Fit. 2018, 58, 534–548. [Google Scholar] [CrossRef]
- Hernandez-Reyes, A.; Cámara-Martos, F.; Molina-Recio, G.; Molina-Luque, R.; Romero-Saldana, M.; Moreno-Rojas, R.; Pérez, C.T.; Pitti, J.A.; Carrion, C.; Ciptaningtyas, R.; et al. Push Notifications From a Mobile App to Improve the Body Composition of Overweight or Obese Women: Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e13747. [Google Scholar] [CrossRef] [Green Version]
- DiFrancisco-Donoghue, J.; Jung, M.-K.; Stangle, A.; Werner, W.G.; Zwibel, H.; Happel, P.; Balentine, J. Utilizing wearable technology to increase physical activity in future physicians: A randomized trial. Prev. Med. Rep. 2018, 12, 122–127. [Google Scholar] [CrossRef]
- Lugones-Sanchez, C.; Sanchez-Calavera, M.A.; Repiso-Gento, I.; Adalia, E.G.; Ramirez-Manent, J.I.; Agudo-Conde, C.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; Recio-Rodriguez, J.I.; Garcia-Ortiz, L.; et al. Effectiveness of an mHealth Intervention Combining a Smartphone App and Smart Band on Body Composition in an Overweight and Obese Population: Randomized Controlled Trial (EVIDENT 3 Study). JMIR mHealth uHealth 2020, 8, e21771. [Google Scholar] [CrossRef] [PubMed]
- Samdal, G.B.; Eide, G.E.; Barth, T.; Williams, G.; Meland, E. Effective behaviour change techniques for physical activity and healthy eating in overweight and obese adults; systematic review and meta-regression analyses. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moustgaard, H.; Clayton, G.; Jones, H.; Boutron, I.; Jørgensen, L.; Laursen, D.R.T.; Olsen, M.F.; Paludan-Müller, A.; Ravaud, P.; Savović, J.; et al. Impact of blinding on estimated treatment effects in randomised clinical trials: Meta-epidemiological study. BMJ 2020, 368, l6802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakata, Y.; Sasai, H.; Tsujimoto, T.; Hashimoto, K.; Kobayashi, H. Web-based intervention to promote weight-loss maintenance using an activity monitor: A randomized controlled trial. Prev. Med. Rep. 2019, 14, 100839. [Google Scholar] [CrossRef]
- Aneni, E.C.; Roberson, L.L.; Maziak, W.; Agatston, A.S.; Feldman, T.; Rouseff, M.; Tran, T.H.; Blumenthal, R.S.; Blaha, M.J.; Blankstein, R.; et al. A Systematic Review of Internet-Based Worksite Wellness Approaches for Cardiovascular Disease Risk Management: Outcomes, Challenges & Opportunities. PLoS ONE 2014, 9, e83594. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 746) | DPG (n = 250) | PG (n = 248) | CG (n = 248) | p Value |
|---|---|---|---|---|---|
| Sex, n (%) | |||||
| Males | 344 (46.1%) | 114 (45.6%) | 115 (46.4%) | 115 (46.4%) | 0.980 # |
| Females | 402 (53.9%) | 136 (54.4%) | 133 (53.6%) | 133 (53.6%) | |
| Age (year) | 70.1 ± 5.3 | 70.3 ± 5.5 | 69.7 ± 5.3 | 70.2 ± 5.3 | 0.425 * |
| Marital status, n (%) | |||||
| Single | 10 (1.3%) | 2 (0.8%) | 3 (1.2%) | 5 (2.0%) | 0.407 # |
| Married | 623 (83.5%) | 216 (86.4%) | 201 (83.1%) | 206 (83.1%) | |
| Divorced | 14 (1.9%) | 4 (1.6%) | 8 (3.2%) | 2 (0.8%) | |
| Widowed | 97 (13.0%) | 27 (10.8%) | 35 (14.1%) | 35 (14.1%) | |
| Separated | 2 (0.3%) | 1 (0.4%) | 1 (0.4%) | 0 (0.0%) | |
| Education, n (%) | |||||
| Elementary school or below | 140 (18.8%) | 46 (18.4%) | 46 (18.5%) | 48 (19.4%) | 0.985 # |
| Middle or high school | 456 (61.1%) | 153 (61.2%) | 150 (60.5%) | 153 (61.7%) | |
| University studies | 150 (20.1%) | 51 (20.4%) | 52 (21.0%) | 47 (19.0%) | |
| Smoking, n (%) | |||||
| Smoker | 111 (14.9%) | 28 (11.2%) | 40 (16.1%) | 43 (17.3%) | 0.114 # |
| Former smoker | 105 (14.1%) | 35 (14.0%) | 42 (16.9%) | 28 (11.3%) | |
| Non-smoker | 530 (71.0%) | 187 (74.8%) | 166 (66.9%) | 177 (71.4%) | |
| City, n (%) | |||||
| Jinan | 113 (15.1%) | 38 (15.2%) | 35 (14.1%) | 40 (16.1%) | 0.988 # |
| Taiyuan | 159 (21.3%) | 51 (20.4%) | 55 (22.2%) | 53 (21.4%) | |
| Nanchang | 181 (24.3%) | 61 (24.4%) | 56 (22.6%) | 64 (25.8%) | |
| Hefei | 159 (21.3%) | 55 (22.0%) | 55 (22.2%) | 49 (19.8%) | |
| Guangzhou | 134 (18.0%) | 45 (18.0%) | 47 (19.0%) | 42 (16.9%) | |
| Height (cm) | 159.6 ± 8.0 | 159.7 ± 8.0 | 159.7 ± 8.1 | 159.5 ± 7.8 | 0.935 * |
| Weight (kg) | 70.6 ± 9.6 | 70.6 ± 9.1 | 70.5 ± 9.7 | 70.9 ± 10.0 | 0.895 * |
| BMI (kg/m2) | 27.5 ± 2.6 | 27.6 ± 2.3 | 27.6 ± 2.9 | 27.8 ± 2.7 | 0.634 * |
| <28 | 468 (62.7%) | 153 (61.2%) | 165 (66.5%) | 150 (60.5%) | 0.314 # |
| ≥28 | 278 (37.3%) | 97 (38.8%) | 83 (33.5%) | 98 (39.5%) | |
| WC (cm) | 94.8 ± 8.0 | 93.9 ± 8.1 | 95.2 ± 7.9 | 95.2 ± 7.9 | 0.124 * |
| HC (cm) | 102.3 ± 6.4 | 101.9 ± 6.0 | 102.1 ± 6.3 | 103.0 ± 6.8 | 0.149 * |
| Time 1 (0 Day) | Time 2 (45 Days) | Time 3 (90 Days) | |
|---|---|---|---|
| Weight (kg) | |||
| DPG | 70.5 ± 9.1 | 68.9 ± 8.9 | 66.4 ± 8.9 ab |
| PG | 70.6 ± 9.7 | 69.7 ± 9.5 | 69.6 ± 9.6 |
| CG | 70.5 ± 10.2 | 69.9 ± 10.3 | 69.7 ± 10.1 |
| BMI (kg/m2) | |||
| DPG | 27.6 ± 2.2 | 27.0 ± 2.2 c | 26.0 ± 2.2 ab |
| PG | 27.7 ± 3.0 | 27.3 ± 2.9 | 27.3 ± 2.9 |
| CG | 27.8 ± 2.8 | 27.6 ± 2.8 | 27.5 ± 2.7 |
| WC (cm) | |||
| DPG | 93.8 ± 8.2 | 93.4 ± 7.9 | 91.1 ± 8.6 ab |
| PG | 95.0 ± 8.1 | 94.7 ± 8.0 | 94.9 ± 8.1 |
| CG | 95.3 ± 7.9 | 95.0 ± 7.8 | 95.8 ± 7.9 |
| HC (cm) | |||
| DPG | 101.9 ± 6.0 | 99.9 ± 5.8 c | 98.1 ± 6.0 ab |
| PG | 102.3 ± 6.5 | 100.6 ± 6.6 c | 100.9 ± 6.8 a |
| CG | 102.9 ± 7.1 | 101.6 ± 6.5 | 101.5 ± 6.4 a |
| MD (Time 2–Time 1) | MD (Time 3–Time 1) | |||||
|---|---|---|---|---|---|---|
| DPG | PG | CG | DPG | PG | CG | |
| Weight (kg) | −1.6 ± 1.2 ab | −0.9 ± 1.3 | −0.7 ± 3.5 | −4.1 ± 1.5 ab | −1.0 ± 1.7 | −0.8 ± 2.0 |
| BMI (kg/m2) | −0.6 ± 0.5 ab | −0.3 ± 0.5 | −0.3 ± 1.4 | −1.6 ± 0.6 ab | −0.4 ± 0.7 | −0.3 ± 0.8 |
| WC (cm) | −0.4 ± 5.2 | −0.3 ± 4.7 | −0.3 ± 5.1 | −2.8 ± 5.6 ab | −0.1 ± 4.8 | 0.5 ± 5.2 |
| HC (cm) | −2.0 ± 3.4 a | −1.6 ± 4.1 | −1.3 ± 3.7 | −3.8 ± 3.5 ab | −1.3 ± 4.0 | −1.3 ± 3.6 |
| MD (Time 2−Time 1) | MD (Time 3−Time 1) | |||||
|---|---|---|---|---|---|---|
| DPG | PG | CG | DPG | PG | CG | |
| Sex | ||||||
| Males | ||||||
| Weight (kg) | −1.8 ± 1.3 ab | −0.8 ± 1.4 | −0.4 ± 3.5 | −4.4 ± 1.4 ab | −0.8 ± 1.8 | −0.7 ± 2.2 |
| BMI (kg/m2) | −0.7 ± 0.5 ab | −0.3 ± 0.5 | −0.1 ± 1.2 | −1.6 ± 0.5 ab | −0.3 ± 0.6 | −0.2 ± 0.8 |
| WC (cm) | −1.6 ± 4.0 | −1.9 ± 3.0 | −1.4 ± 4.5 | −3.6 ± 4.0 ab | −1.0 ± 3.6 | −0.2 ± 4.5 |
| HC (cm) | −2.1 ± 3.3 a | −1.7 ± 3.2 | −1.1 ± 3.2 | −3.8 ± 3.6 ab | −1.1 ± 3.0 | −1.3 ± 3.3 |
| Females | ||||||
| Weight (kg) | −1.4 ± 1.1 | −0.9 ± 1.2 | −0.9 ± 3.6 | −3.8 ± 1.4 ab | −1.2 ± 1.6 | −1.0 ± 1.9 |
| BMI (kg/m2) | −0.6 ± 0.4 | −0.4 ± 0.5 | −0.4 ± 1.4 | −1.6 ± 0.6 ab | −0.5 ± 0.7 | −0.4 ± 0.8 |
| WC (cm) | 0.5 ± 5.8 | 1.0 ± 5.3 | 0.6 ± 5.3 | −2.1 ± 6.6 ab | 0.6 ± 5.5 | 1.0 ± 5.6 |
| HC (cm) | −1.9 ± 3.5 | −1.6 ± 4.7 | −1.4 ± 4.1 | −3.9 ± 3.4 ab | −1.5 ± 4.7 | −1.4 ± 3.9 |
| BMI | ||||||
| BMI<28 kg/m2 | ||||||
| Weight (kg) | −1.4 ± 1.1 ab | −0.7 ± 1.3 c | −0.2 ± 3.1 | −4.0 ± 1.5 ab | −0.8 ± 1.5 | −0.5 ± 1.4 |
| BMI (kg/m2) | −0.6 ± 0.4 ab | −0.3 ± 0.5 | −0.1 ± 1.2 | −1.6 ± 0.6 ab | −0.3 ± 0.6 | −0.2 ± 0.5 |
| WC (cm) | −0.2 ± 5.3 | −0.4 ± 4.6 | 0.1 ± 5.2 | −2.8 ± 5.4 ab | −0.5 ± 4.4 c | 0.8 ± 4.9 |
| HC (cm) | −1.9 ± 3.2 a | −1.5 ± 3.3 | −0.9 ± 3.4 | −3.8 ± 3.5 ab | −1.2 ± 3.4 | −0.9 ± 3.4 |
| BMI ≥ 28 kg/m2 | ||||||
| Weight (kg) | −1.8 ± 1.3 | −1.1 ± 1.3 | −1.4 ± 4.0 | −4.3 ± 1.4 ab | −1.4 ± 1.9 | −1.3 ± 2.6 |
| BMI (kg/m2) | −0.7 ± 0.5 | −0.4 ± 0.5 | −0.5 ± 1.6 | −1.7 ± 0.6 ab | −0.6 ± 0.8 | −0.5 ± 1.0 |
| WC (cm) | −0.9 ± 5.0 | −0.2 ± 4.8 | −1.0 ± 4.7 | −2.7 ± 6.0 ab | 0.5 ± 5.5 | −0.1 ± 5.5 |
| HC (cm) | −2.2 ± 3.8 | −1.9 ± 5.3 | −2.0 ± 4.1 | −3.8 ± 3.4 ab | −1.6 ± 5.0 | −2.6 ± 4.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, M.; Zhang, N.; Zhang, Y.; Yan, X.; Li, M.; Guo, W.; Guo, X.; He, H.; Guo, K.; Ma, G. Effect of Mobile-Based Lifestyle Intervention on Weight Loss among the Overweight and Obese Elderly Population in China: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 8825. https://doi.org/10.3390/ijerph18168825
Zhou M, Zhang N, Zhang Y, Yan X, Li M, Guo W, Guo X, He H, Guo K, Ma G. Effect of Mobile-Based Lifestyle Intervention on Weight Loss among the Overweight and Obese Elderly Population in China: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(16):8825. https://doi.org/10.3390/ijerph18168825
Chicago/Turabian StyleZhou, Mingzhu, Na Zhang, Yu Zhang, Xinyu Yan, Muxia Li, Wen Guo, Xiaohui Guo, Hairong He, Kaiwei Guo, and Guansheng Ma. 2021. "Effect of Mobile-Based Lifestyle Intervention on Weight Loss among the Overweight and Obese Elderly Population in China: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 16: 8825. https://doi.org/10.3390/ijerph18168825
APA StyleZhou, M., Zhang, N., Zhang, Y., Yan, X., Li, M., Guo, W., Guo, X., He, H., Guo, K., & Ma, G. (2021). Effect of Mobile-Based Lifestyle Intervention on Weight Loss among the Overweight and Obese Elderly Population in China: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 18(16), 8825. https://doi.org/10.3390/ijerph18168825