
Marathon-Induced Cardiac Fatigue: A Review over the Last Decade for the Preservation of the Athletes’ Health

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
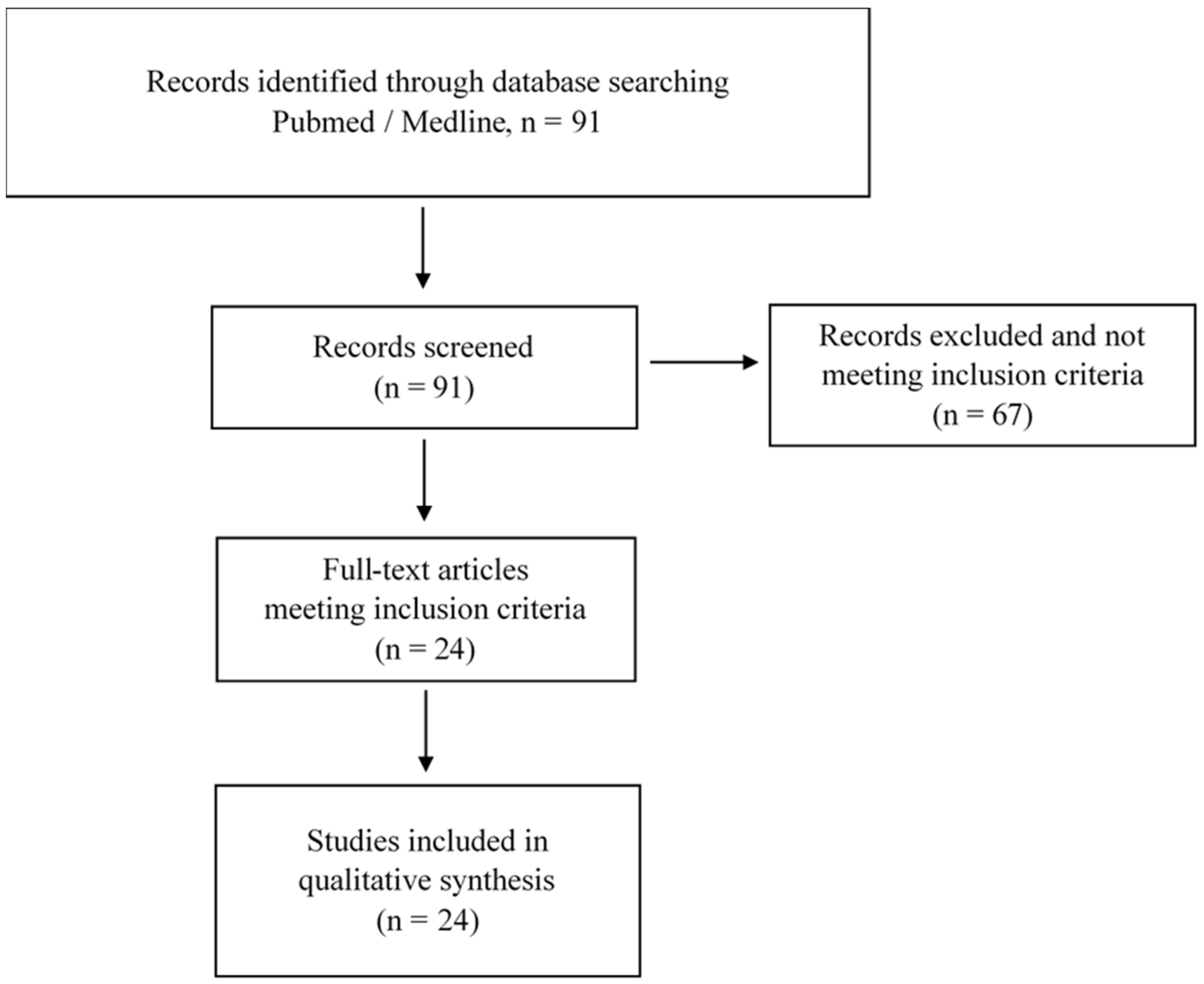
3.1. Search Results
3.2. Biomarkers of Cardiac Fatigue and Cardiac Stress after a Marathon
3.3. Cardiovascular Function after Marathon
4. Discussion
5. Conclusions
Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nystoriak, M.A.; Bhatnagar, A. Cardiovascular Effects and Benefits of Exercise. Front. Cardiovasc. Med. 2018, 5, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Saltin, B.; Stenberg, J. Circulatory Response to Prolonged Severe Exercise. J. Appl. Physiol. 1964, 19, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Douglas, P.S.; O’Toole, M.L.; Hiller, W.D.; Hackney, K.; Reichek, N. Cardiac fatigue after prolonged exercise. Circulation 1987, 76, 1206–1213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shave, R.; Baggish, A.; George, K.; Wood, M.; Scharhag, J.; Whyte, G.; Gaze, D.; Thompson, P.D. Exercise-induced cardiac troponin elevation: Evidence, mechanisms, and implications. J. Am. Coll. Cardiol. 2010, 56, 169–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eijsvogels, T.M.; Fernandez, A.B.; Thompson, P.D. Are There Deleterious Cardiac Effects of Acute and Chronic Endurance Exercise? Physiol. Rev. 2016, 96, 99–125. [Google Scholar] [CrossRef]
- Middleton, N.; Shave, R.; George, K.; Whyte, G.; Hart, E.; Atkinson, G. Left ventricular function immediately following prolonged exercise: A meta-analysis. Med. Sci. Sports Exerc. 2006, 38, 681–687. [Google Scholar] [CrossRef]
- Banks, L.; Sasson, Z.; Busato, M.; Goodman, J.M. Impaired left and right ventricular function following prolonged exercise in young athletes: Influence of exercise intensity and responses to dobutamine stress. J. Appl. Physiol. 2010, 108, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Sengupta, S.P.; Mahure, C.; Mungulmare, K.; Grewal, H.K.; Bansal, M. Myocardial fatigue in recreational marathon runners: A speckle-tracking echocardiography study. Indian Heart J. 2018, 70 (Suppl. 3), S229–S234. [Google Scholar] [CrossRef]
- Stewart, G.M.; Yamada, A.; Haseler, L.J.; Kavanagh, J.J.; Chan, J.; Koerbin, G.; Wood, C.; Sabapathy, S. Influence of exercise intensity and duration on functional and biochemical perturbations in the human heart. J. Physiol. 2016, 594, 3031–3044. [Google Scholar] [CrossRef] [Green Version]
- La Gerche, A.; Burns, A.T.; Mooney, D.J.; Inder, W.J.; Taylor, A.J.; Bogaert, J.; Macisaac, A.I.; Heidbüchel, H.; Prioret, D.L. Exercise-induced right ventricular dysfunction and structural remodelling in endurance athletes. Eur. Heart J. 2012, 33, 998–1006. [Google Scholar] [CrossRef] [Green Version]
- Vitiello, D.; Cassirame, J.; Menetrier, A.; Rupp, T.; Schuster, I.; Reboul, C.; Obert, P.; Tordi, N.; Nottin, S. Depressed systolic function after a prolonged and strenuous exercise. Med. Sci. Sports Exerc. 2013, 45, 2072–2079. [Google Scholar] [CrossRef]
- George, K.; Shave, R.; Oxborough, D.; Cable, T.; Dawson, E.; Artis, N.; Gaze, D.; Hew-Butler, T.; Sharwood, K.; Noakes, T. Left ventricular wall segment motion after ultra-endurance exercise in humans assessed by myocardial speckle tracking. Eur. J. Echocardiogr. 2009, 10, 238–243. [Google Scholar] [CrossRef]
- Elliott, A.D.; La Gerche, A. The right ventricle following prolonged endurance exercise: Are we overlooking the more important side of the heart? A meta-analysis. Br. J. Sports Med. 2015, 49, 724–729. [Google Scholar] [CrossRef]
- Kaleta-Duss, A.M.; Lewicka-Potocka, Z.; Dąbrowska-Kugacka, A.; Raczak, G.; Lewicka, E. Myocardial Injury and Overload among Amateur Marathoners as Indicated by Changes in Concentrations of Cardiovascular Biomarkers. Int. J. Environ. Res. Public Health 2020, 17, 6191. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Navarro, I.; Sánchez-Gómez, J.; Sanmiguel, D.; Collado, E.; Hernando, B.; Panizo, N.; Hernando, C. Immediate and 24-h post-marathon cardiac troponin T is associated with relative exercise intensity. Eur. J. Appl. Physiol. 2020, 120, 1723–1731. [Google Scholar] [CrossRef]
- Wegberger, C.; Tscharre, M.; Haller, P.M.; Piackova, E.; Vujasin, I.; Gomiscek, A.; Tentzeris, I.; Freynhofer, M.K.; Jäger, B.; Wojta, J.; et al. Impact of ultra-marathon and marathon on biomarkers of myocyte necrosis and cardiac congestion: A prospective observational study. Clin. Res. Cardiol. Off. J. Ger Card Soc. 2020, 109, 1366–1373. [Google Scholar] [CrossRef]
- de Gonzalo-Calvo, D.; Dávalos, A.; Fernández-Sanjurjo, M.; Amado-Rodríguez, L.; Díaz-Coto, S.; Tomás-Zapico, C.; Montero, A.; García-González, Á.; Llorente-Cortés, V.; Heras, M.E.; et al. Circulating microRNAs as emerging cardiac biomarkers responsive to acute exercise. Int. J. Cardiol. 2018, 264, 130–136. [Google Scholar] [CrossRef]
- Kosowski, M.; Młynarska, K.; Chmura, J.; Kustrzycka-Kratochwil, D.; Sukiennik-Kujawa, M.; Todd, J.A.; Jankowska, E.A.; Banasiak, W.; Reczuch, K.; Ponikowski, P. Cardiovascular stress biomarker assessment of middle-aged non-athlete marathon runners. Eur. J. Prev. Cardiol. 2019, 26, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.J.; Leckie, T.; Watkins, E.R.; Fitzpatrick, D.; Galloway, R.; Grimaldi, R.; Baker, P. Post marathon cardiac troponin T is associated with relative exercise intensity. J. Sci. Med. Sport. 2018, 21, 880–884. [Google Scholar] [CrossRef] [PubMed]
- Roca, E.; Nescolarde, L.; Lupón, J.; Barallat, J.; Januzzi, J.L.; Liu, P.; Pastor, M.C.; Bayes-Genis, A. The Dynamics of Cardiovascular Biomarkers in non-Elite Marathon Runners. J. Cardiovasc. Transl. Res. 2017, 10, 206–208. [Google Scholar] [CrossRef] [Green Version]
- Martin, T.G.; Pata, R.W.; D’Addario, J.; Yuknis, L.; Kingston, R.; Feinn, R. Impact of age on haematological markers pre- and post-marathon running. J. Sports Sci. 2015, 33, 1988–1997. [Google Scholar] [CrossRef] [PubMed]
- Scherr, J.; Braun, S.; Schuster, T.; Hartmann, C.; Moehlenkamp, S.; Wolfarth, B.; Pressler, A.; Halle, M. 72-h kinetics of high-sensitive troponin T and inflammatory markers after marathon. Med. Sci. Sports Exerc. 2011, 43, 1819–1827. [Google Scholar] [CrossRef] [PubMed]
- Clauss, S.; Scherr, J.; Hanley, A.; Schneider, J.; Klier, I.; Lackermair, K.; Hoster, E.; Vogeser, M.; Nieman, D.C.; Halle, M.; et al. Impact of polyphenols on physiological stress and cardiac burden in marathon runners—Results from a substudy of the BeMaGIC study. Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Metab. 2017, 42, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Traiperm, N.; Chaunchaiyakul, R.; Burtscher, M.; Gatterer, H. Cardiac Biomarkers Following Marathon Running: Is Running Time a Factor for Biomarker Change? Int. J. Sports Physiol. Perform. 2021, 1–8. [Google Scholar] [CrossRef]
- Sierra, A.P.; Oliveira-Junior, M.C.; Almeida, F.M.; Benetti, M.; Oliveira, R.; Felix, S.N.; Santos Genaro, I. Impairment on Cardiopulmonary Function after Marathon: Role of Exhaled Nitric Oxide. Oxid Med Cell Longev. 2019, 2019, 5134360. [Google Scholar] [CrossRef]
- Niemelä, M.; Kangastupa, P.; Niemelä, O.; Bloigu, R.; Juvonen, T. Acute Changes in Inflammatory Biomarker Levels in Recreational Runners Participating in a Marathon or Half-Marathon. Sports Med. Open. 2016, 2, 21. [Google Scholar] [CrossRef] [Green Version]
- Bekos, C.; Zimmermann, M.; Unger, L.; Janik, S.; Hacker, P.; Mitterbauer, A.; Koller, M.; Fritz, R.; Gäbler, C.; Kessler, M.; et al. Non-professional marathon running: RAGE axis and ST2 family changes in relation to open-window effect, inflammation and renal function. Sci. Rep. 2016, 6, 32315. [Google Scholar] [CrossRef]
- Baggish, A.L.; Park, J.; Min, P.-K.; Isaacs, S.; Parker, B.A.; Thompson, P.D.; Troyanos, C.; D’Hemecourt, P.; Dyer, S.; Thiel, M.; et al. Rapid upregulation and clearance of distinct circulating microRNAs after prolonged aerobic exercise. J. Appl. Physiol. Bethesda Md. 1985. 2014, 116, 522–531. [Google Scholar] [CrossRef] [Green Version]
- Lewicka-Potocka, Z.; Dąbrowska-Kugacka, A.; Lewicka, E.; Gałąska, R.; Daniłowicz-Szymanowicz, L.; Faran, A.; Nabiałek-Trojanowska, I.; Kubik, M.; Kaleta-Duss, A.M.; Raczak, G. Right Ventricular Diastolic Dysfunction after Marathon Run. Int. J. Environ. Res. Public Health 2020, 17, 5336. [Google Scholar] [CrossRef] [PubMed]
- Roeh, A.; Schuster, T.; Jung, P.; Schneider, J.; Halle, M.; Scherr, J. Two dimensional and real-time three dimensional ultrasound measurements of left ventricular diastolic function after marathon running: Results from a substudy of the BeMaGIC trial. Int. J. Cardiovasc. Imaging 2019, 35, 1861–1869. [Google Scholar] [CrossRef] [PubMed]
- Mertova, M.; Botek, M.; Krejci, J.; Mckune, A. Heart rate variability recovery after a skyrunning marathon and correlates of performance. Acta Gymnica 2017, 47, 161–170. [Google Scholar] [CrossRef] [Green Version]
- Sierra, A.P.; Silveira, A.D.; Francisco, R.C.; Barretto, R.B.; Sierra, C.A.; Meneghelo, R.S.; Kiss, M.A.; Ghorayeb, N.; Stein, R. Reduction in Post-Marathon Peak Oxygen Consumption: Sign of Cardiac Fatigue in Amateur Runners? Arq. Bras Cardiol. 2016, 106, 92–96. [Google Scholar] [CrossRef]
- Hanssen, H.; Keithahn, A.; Hertel, G.; Drexel, V.; Stern, H.; Schuster, T.; Lorang, D.; Beer, A.J.; Schmidt-Trucksäss, A.; Nickel, T.; et al. Magnetic resonance imaging of myocardial injury and ventricular torsion after marathon running. Clin. Sci. Lond Engl. 2011, 120, 143–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan-Dewar, F.; Oxborough, D.; Shave, R.; Gregson, W.; Whyte, G.; George, K. Left ventricular myocardial strain and strain rates in sub-endocardial and sub-epicardial layers before and after a marathon. Eur. J. Appl. Physiol. 2010, 109, 1191–1196. [Google Scholar] [CrossRef]
- Wilson, G.D.; Geddes, T.J.; Pruetz, B.L.; Thibodeau, B.J.; Murawka, A.; Colar, J.M.; McCullough, P.A.; Trivax, J.E. SELDI-TOF-MS Serum Profiling Reveals Predictors of Cardiac MRI Changes in Marathon Runners. Int. J. Proteom. 2012, 2012, 679301. [Google Scholar] [CrossRef]
- Ruegsegger, G.N.; Booth, F.W. Health Benefits of Exercise. Cold Spring Harb. Perspect Med. 2018, 8, a029694. [Google Scholar] [CrossRef] [Green Version]
- Burtscher, J.; Burtscher, M. Run for your life: Tweaking the weekly physical activity volume for longevity. Br. J. Sports Med. 2020, 54, 759–760. [Google Scholar] [CrossRef]
- George, K.; Oxborough, D.; Forster, J.; Whyte, G.; Shave, R.; Dawson, E.; Stephenson, C.; Dugdill, L.; Edwards, B.; Gaze, D. Mitral annular myocardial velocity assessment of segmental left ventricular diastolic function after prolonged exercise in humans. J. Physiol. 2005, 569, 305–313. [Google Scholar] [CrossRef] [Green Version]
- Oxborough, D.; Shave, R.; Middleton, N.; Whyte, G.; Forster, J.; George, K. The impact of marathon running upon ventricular function as assessed by 2D, Doppler, and tissue-Doppler echocardiography. Echocardiography 2006, 23, 635–641. [Google Scholar] [CrossRef]
- Neilan, T.G.; Januzzi, J.L.; Lee-Lewandrowski, E.; Ton-Nu, T.-T.; Yoerger, D.M.; Jassal, D.S.; Lewandrowski, K.B.; Siegel, A.J.; Marshall, J.E.; Douglas, P.S.; et al. Myocardial injury and ventricular dysfunction related to training levels among nonelite participants in the Boston marathon. Circulation 2006, 114, 2325–2333. [Google Scholar] [CrossRef] [Green Version]
- Dawson, E.A.; Whyte, G.P.; Black, M.A.; Jones, H.; Hopkins, N.; Oxborough, D.; Gaze, D.; Shave, R.E.; Wilson, M.; George, K.P.; et al. Changes in vascular and cardiac function after prolonged strenuous exercise in humans. J. Appl. Physiol. 2008, 105, 1562–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seals, D.R.; Rogers, M.A.; Hagberg, J.M.; Yamamoto, C.; Cryer, P.E.; Ehsani, A.A. Left ventricular dysfunction after prolonged strenuous exercise in healthy subjects. Am. J. Cardiol. 1988, 61, 875–879. [Google Scholar] [CrossRef]
- Dawson, E.A.; Shave, R.; Whyte, G.; Ball, D.; Selmer, C.; Jans, O.; Secher, N.H.; George, K.P. Preload maintenance and the left ventricular response to prolonged exercise in men. Exp. Physiol. 2007, 92, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Coates, A.M.; King, T.J.; Currie, K.D.; Tremblay, J.C.; Petrick, H.L.; Slysz, J.T.; Pignanelli, C.; Berard, J.A.; Millar, P.J.; Burr, J.F. Alterations in Cardiac Function Following Endurance Exercise Are Not Duration Dependent. Front. Physiol. 2020, 11, 581797. [Google Scholar] [CrossRef]
- Lee, C.T.; Eastman, S.E.; Arcinas, L.A.; Asselin, C.Y.; Cheung, D.; Mayba, A.; Zhu, A.; Strzelczyk, J.; Maycher, B.; Memauri, B.; et al. Prevalence and Functional Implication of Silent Coronary Artery Disease in Marathon Runners Over 40 Years of Age: The MATCH-40 Study. CJC Open 2021, 3, 595–602. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| References | Methods/Parameters | Pre-Marathon | Post-Marathon | p-Value |
|---|---|---|---|---|
| Biomarkers Analyses | ||||
| Traiperm [25] | ||||
| cTnT (ng/mL) | ||||
| NT-proBNP (pg/mL) | Curvilinear relationship between NT-ProBNP increment and running time (r2 = 0.359) | <0.05 | ||
| Kaleta-Duss [15] | ||||
| CK (U/l) | 148 ± 76.3 | 411 ± 170 | <0.001 | |
| hs-cTnI (ng/mL) | 0.01 ± 0.01 | 0.06 ± 0.09 | <0.001 | |
| H-FABP (ng/mL) | 2.22 ± 1.18 | 13.57 ± 9.63 | <0.001 | |
| BNP (pg/mL) | 79.86 ± 53.11 | 155.38 ± 156.23 | <0.001 | |
| NT-proANP (pg/mL) | 469.25 ± 155.44 | 753.3 ± 176.60 | <0.001 | |
| Gal-3 (ng/mL) | 8.53 ± 3.04 | 10.65 ± 2.33 | <0.001 | |
| GDF-15 (pg/mL) | 50.97 ± 27.61 | 137.34 ± 85.19 | <0.001 | |
| Martinez-Navarro [16] | ||||
| hs-cTnT (ng/L) | 5.74 ± 5.29 | 50.4 ± 57.04 | <0.001 | |
| Sierra [26] | ||||
| IL-6 (pg/mL) | 581 ± 1529 | 87 ± 53 | NS | |
| IL-8 (pg/mL) | 3099 ± 6511 | 1450 ± 6233 | NS | |
| IL-12p40 (pg/mL) | 3775 ± 12406 | 285 ± 131 | <0.05 | |
| IL-23 (pg/mL) | 3722 ± 12115 | 1004 ± 254 | <0.05 | |
| IL-33 (pg/mL) | 412 ± 1546 | 267 ± 145 | <0.05 | |
| TSLP (pg/mL) | 387 ± 1974 | 20 ± 16 | <0.05 | |
| eNO (ppb) | 20 ± 11 | 35 ± 19 | ↑ | |
| Wegberger [17] | ||||
| Troponin I (µg/L) | btw 0–0.01 | 0.03 (0.02–0.05) | 0.016 | |
| CK (U/L) | btw 0–250 | 425 (327–681) | 0.001 | |
| Copeptin (pmol/L) | btw 0–20 | 26.25 (16.29–39.02) | 0.078 | |
| NT-proBNP (ng/L) | btw 0–100 | 132 (64–198) | 0.001 | |
| MR-proADM (nmol/L) | btw 0.25–0.60 | 0.88 (0.55–0.99) | 0.023 | |
| de Gonzalo-Calvo [18] | ||||
| hs-cTnT (pg/mL) | btw 0–5 | btw 0–35 | <0.01 | |
| NT-proBNP (pg/mL) | btw 0–25 | btw 0–110 | <0.05 | |
| CK (U/L) | btw 0–150 | btw 0–300 | <0.001 | |
| hFABP (ng/mL) | btw 0–3 | btw 0–24 | <0.01 | |
| Gal-3 (ng/mL) | btw 0–7 | btw 0–22 | <0.001 | |
| Kosowski [19] | ||||
| hs-cTnI (pg/mL) | 3.67 (1.88–5.38) | 22 (9.58–34.56) | <0.001 | |
| NT-proBNP (pg/mL) | 50 (33–73) | 169 (112–365) | <0.001 | |
| ET-1 (pg/mL) | 3.03 (2.5–3.4) | 5.22 (4.4–5.89) | <0.001 | |
| Creatinine (mg/dL) | 0.85 (0.79–0.98) | 1.39 (1.22–1.56) | <0.001 | |
| Richardson [20] | ||||
| cTnT (ng/L) | 5.60 ± 3.27 | 74.52 ± 30.39 | <0.001 | |
| Sengupta [9] | ||||
| NT-proBNP (pg/mL) | 86.0 ± 9.5 | 106.5 ± 24.2 | 0.001 | |
| Clauss [24] | ||||
| Chromogranin A (pg/mL) | btw 0–60 | btw 0–90 | <0.001 | |
| NT-proBNP (ng/mL) | btw 0–30 | btw 0–110 | <0.001 | |
| Roca [21] | ||||
| NT-proBNP (ng/L) | 70 (70–70) | 92 (70–147) | <0.001 | |
| ST2 (ng/mL) | 34.2 (24.7–40.9) | 54.2 (38.2–72.4) | <0.001 | |
| hs-TnT (ng/L) | 2.9 (1.7–7) | 46.9 (24.1–91.1) | <0.001 | |
| Bekos [28] | ||||
| sRAGE (pg/mL) | btw 250–600 | btw 400–750 | <0.001 | |
| ST2 (pg/mL) | btw 0–250 | btw 125–400 | <0.001 | |
| Niemelä [27] | ||||
| suPAR (ng/mL) | btw 0.5–2 | btw 1.2–3.5 | <0.01 | |
| CD163 (ng/mL) | btw 300–800 | btw 500–1100 | <0.05 | |
| CRP (mg/L) | btw 0–12 | btw 0–22 | <0.05 | |
| IL-6 (pg/mL) | btw 0–8 | btw 17–25 | <0.01 | |
| IL-8 (pg/mL) | btw 5–12 | btw 25–42 | <0.05 | |
| IL-10 (pg/mL) | btw 0–1 | btw 1–3.5 | <0.05 | |
| TNF-α (pg/mL) | btw 0–1 | btw 1–2.5 | NS | |
| TGF-β (pg/mL) | btw 500–1000 | btw 0–1000 | NS | |
| Martin [22] | ||||
| Creatinine (mg/dL) | 0.94 ± 0.12 | 1.42 ± 0.24 | <0.001 | |
| CK (U/L) | 133 ± 60 | 367 ± 167 | <0.001 | |
| White blood cells (thousand/μL) | 5.75 ± 1.19 | 15.77 ± 3.29 | <0.001 | |
| Neutrophils (cells/μL) | 3420 ± 1049 | 13580 ± 3019 | <0.001 | |
| Scherr [23] | ||||
| hs-cTnT (ng/L) | 3 (3–5) | 31 (19–47) | <0.001 | |
| NT-proBNP (ng/L) | 27 (14–40) | 93 (57–150) | <0.001 | |
| h-FABP (Kg/L) | 7 (5–10) | 45 (32–64) | <0.001 | |
| hs-CRP (mg/L) | 0.52 (0.30–0.93) | 0.40 (0.24–0.85) | <0.001 | |
| IL-6 (ng/L) | 2.1 (1.9–2.2) | 32 (21–41) | <0.001 | |
| IL-10 (ng/L) | 5.1 (4.9–5.4) | 20 (11–50) | <0.001 | |
| TNF-α (ng/L) | 9 (7–10) | 10 (9–12) | <0.001 | |
| Cystatin C (mg/L) | 0.8 (0.7–0.9) | 0.9 (0.9–1.0) | <0.001 | |
| Baggish [29] | ||||
| c-miR-1 (fold change) | 21.8 | 0.04 | ||
| c-miR-126 (fold change) | 1.9 | <0.001 | ||
| c-miR-133 (fold change) | 18.5 | 0.02 | ||
| c-miR-134 (fold change) | 1.9 | <0.001 | ||
| c-miR-146a (fold change) | 3.3 | <0.001 | ||
| hsCRP (fold change) | 1.0 | 1.000 | ||
| Echography, HRV & STE analyses | ||||
| Lewicka-Potocka [30] | ||||
| LV EF (%) | 61.8 ± 4.9 | 60.5 ± 4.4 | 0.38 | |
| LV GLS (%) | −19.9 ± 2.3 | −19.4 ± 2.1 | 0.41 | |
| RV 4CSL (%) | −22.0 ± 2.8 | −20.80 ± 2.6 | <0.05 | |
| TAPSE (mm) | 25.0 ± 3.6 | 24.0 ± 3.7 | 0.56 | |
| RVd MID (cm) | 3.4 ± 0.6 | 3.7 ± 0.5 | <0.01 | |
| RVd BAS (cm) | 3.8 ± 0.4 | 3.8 ± 0.5 | 0.44 | |
| LVd BAS (cm) | 4.8 ± 0.4 | 4.6 ± 0.3 | <0.001 | |
| RVd/LVd BAS | 0.77 ± 0.1 | 0.82 ± 0.1 | <0.05 | |
| Roeh [31] | ||||
| E/A | 1.6 ± 0.5 | 1.1 ± 0.3 | <0.001 | |
| E/e’ mean | 6.4 ± 1.5 | 6.5 ± 1.8 | 0.6 | |
| DT (s) | 0.18 ± 0.05 | 0.20 ± 0.05 | <0.001 | |
| Vmin (mL/m2) | 11.4 ± 3.7 | 9.9 ± 3.5 | <0.01 | |
| Vmax (mL/m2) | 28.0 ± 6.2 | 25.0 ± 7.0 | <0.01 | |
| Total-SV (mL/m2) | 59.6 ± 7.8 | 60.7 ± 6.0 | 0.3 | |
| Total-EF (%) | 34.9 ± 8.6 | 31.33 ± 10.2 | <0.01 | |
| ASV (mL/m2) | 16.6 ± 3.8 | 15.1 ± 4.1 | <0.01 | |
| True-EF (%) | 6.1 ± 2.4 | 4.8 ± 2.8 | <0.001 | |
| Sengupta [9] | ||||
| Heart rate (beats/minute) | 74.1 ± 6.4 | 64.5 ± 7.6 | <0.001 | |
| Systolic BP (mmHg) | 123 ± 11 | 120 ± 9 | 0.214 | |
| Diastolic BP (mmHg) | 79 ± 5 | 79 ± 5 | 0.675 | |
| IVSd (cm) | 0.94 ± 0.16 | 1.03 ± 0.20 | 0.005 | |
| LV mass (gm) | 0.94 ± 0.16 | 1.03 ± 0.20 | 0.005 | |
| LV mass (gm) | 120.2 ± 30.0 | 160.3 ± 43.0 | <0.001 | |
| LVEDV (mL) | 61.8 ± 16.5 | 72.8 ± 5.1 | <0.001 | |
| LVESV (mL) | 21.9 ± 7.5 | 20.3 ± 3.7 | 0.191 | |
| LVEF (%) | 64.9 ± 5.6 | 72.0 ± 5.7 | <0.001 | |
| Mitral E (cm/s) | 89.8 ± 17.1 | 80.1 ± 17.0 | 0.001 | |
| Mitral annular e0 (cm/s) | 10.4 ± 2.1 | 10.1 ± 2.2 | 0.638 | |
| Mitral E/e0 | 9.1 ± 2.4 | 8.3 ± 2.7 | 0.227 | |
| Left atrial volume index (mL/m2) | 23.2 ± 6.1 | 19.0 ± 6.5 | 0.01 | |
| LV global longitudinal strain (%) | −19.3 ± 2.71 | −16.5 ± 4.6 | 0.003 | |
| LV global circumferential strain (%) | −17.2 ± 2.41 | −15.2 ± 2.6 | 0.001 | |
| LV global radial strain (%) | 31.9 ± 7.4 | 30.9 ± 1.3 | 0.422 | |
| Mertová [32] | ||||
| Sympathovagal balance | - | Ln LF/HF | ↑ | |
| Heart rate (bpm) | - | +30 | ||
| Sierra [33] | ||||
| Peak VO2 (mL/kg/min) | 51 (46–52) | 46 (43–49) | <0.05 | |
| Peak VE (L/min) | 134 (99–148) | 120 (111–147) | NS | |
| VE/VCO2 slope | 34 (30–41) | 31 (27–39) | <0.05 | |
| HR | 62 (60–67) | 104 (101–111) | <0.05 | |
| Systolic volume | 80 (79–100) | 61 (51–68) | <0.05 | |
| Cardiac output | 5354(4747–6458) | 6234(5238–7433) | NS | |
| LVEDD | 51(49–52) | 51 (45–58) | NS | |
| LVESD | 32 (29–32) | 32 (28–34) | NS | |
| EF | 67 (66–70) | 62 (61–67) | NS | |
| E wave | 0.9 (0.7–1.0) | 0.6 (0.5–0.7) | <0.05 | |
| A wave | 0.7 (0.5–0.9) | 0.9 (0.8–0.9) | NS | |
| E/A ratio | 1.3 (1.1–1.5) | 0.7 (0.6–0.8) | <0.05 | |
| s’ wave | 8.8 (8.2–9.7) | 6.7 (5.9–8.0) | <0.05 | |
| e’ wave | 9.2 (8.4–10.6) | 8.5 (6.4–10.4) | NS | |
| a’ wave | 8.1 (7.6–9.1) | 7.6 (6.6–9.6) | NS | |
| E/e’ ratio | 0.09 (0.08–0.10) | 0.08 (0.06–0.09) | NS | |
| Hanssen [34] | ||||
| Heart rate (beats/min) | 57 ± 7 | 86 ± 13 | <0.001 | |
| Systolic blood pressure (mmHg) | 132 ±13 | 121 ± 12 | <0.001 | |
| Diastolic blood pressure (mmHg) | 86 ± 8 | 74 ± 7 | <0.001 | |
| LVEF (%) | 65 ± 4 | 67 ± 5 | 0.280 | |
| LV end-diastolic volume (cm3) | 120 ± 25 | 113 ± 27 | 0.142 | |
| E (cm/s) | 74 ± 14 | 66 ± 14 | 0.054 | |
| A (cm/s) | 56 ± 13 | 72 ± 12 | <0.001 | |
| E /A ratio | 1.4 ± 0.3 | 0.9 ± 0.2 | <0.001 | |
| Septal E’ (cm/s) | 10 ± 1 | 8 ± 2 | 0.001 | |
| Septal A’ (cm/s) | 10 ± 2 | 12 ± 3 | 0.001 | |
| E /E’ ratio | 8.3 ± 1.6 | 8.4 ± 3.4 | 0.871 | |
| Chan-Dewar [35] | ||||
| Sub-epicardial radial strain (%) | 32.6 ± 12.5 | 20.3 ± 9.6% | <0.01 | |
| Sub-endocardial circumferential strain (%) | −26.9 ± 3.6 | −23.7 ± 4.1 | <0.01 | |
| EF | 63 ± 5 | 62 ± 7 | NS | |
| E/A | 1.8 ± 0.7 | 1.1 ± 0.2 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitiello, D.; Palacin, F.; Poinsard, L.; Kirsch, M.; Jouini, S.; Billat, V. Marathon-Induced Cardiac Fatigue: A Review over the Last Decade for the Preservation of the Athletes’ Health. Int. J. Environ. Res. Public Health 2021, 18, 8676. https://doi.org/10.3390/ijerph18168676
Vitiello D, Palacin F, Poinsard L, Kirsch M, Jouini S, Billat V. Marathon-Induced Cardiac Fatigue: A Review over the Last Decade for the Preservation of the Athletes’ Health. International Journal of Environmental Research and Public Health. 2021; 18(16):8676. https://doi.org/10.3390/ijerph18168676
Chicago/Turabian StyleVitiello, Damien, Florent Palacin, Luc Poinsard, Marine Kirsch, Steeve Jouini, and Véronique Billat. 2021. "Marathon-Induced Cardiac Fatigue: A Review over the Last Decade for the Preservation of the Athletes’ Health" International Journal of Environmental Research and Public Health 18, no. 16: 8676. https://doi.org/10.3390/ijerph18168676
APA StyleVitiello, D., Palacin, F., Poinsard, L., Kirsch, M., Jouini, S., & Billat, V. (2021). Marathon-Induced Cardiac Fatigue: A Review over the Last Decade for the Preservation of the Athletes’ Health. International Journal of Environmental Research and Public Health, 18(16), 8676. https://doi.org/10.3390/ijerph18168676