
Selecting Risk of Bias Tools for Observational Studies for a Systematic Review of Anthropometric Measurements and Dental Caries among Children

Abstract
:
1. Introduction
2. Materials and Methods
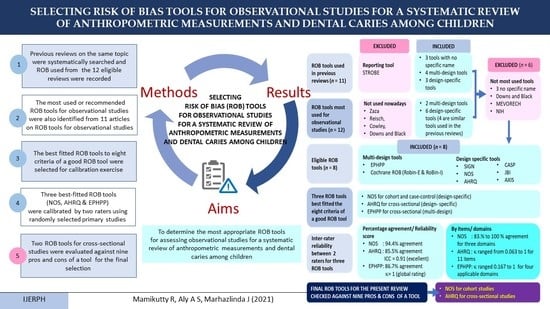
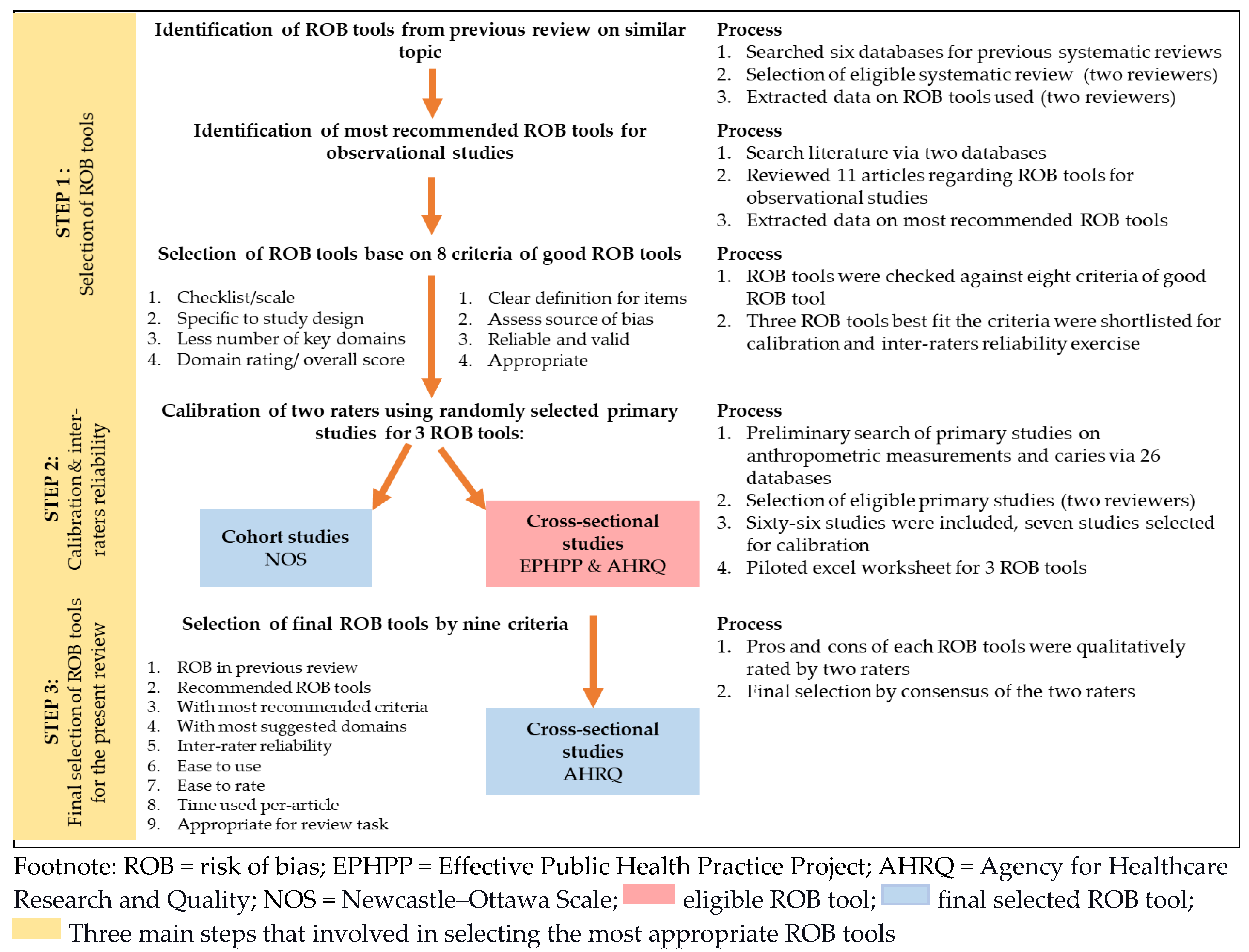
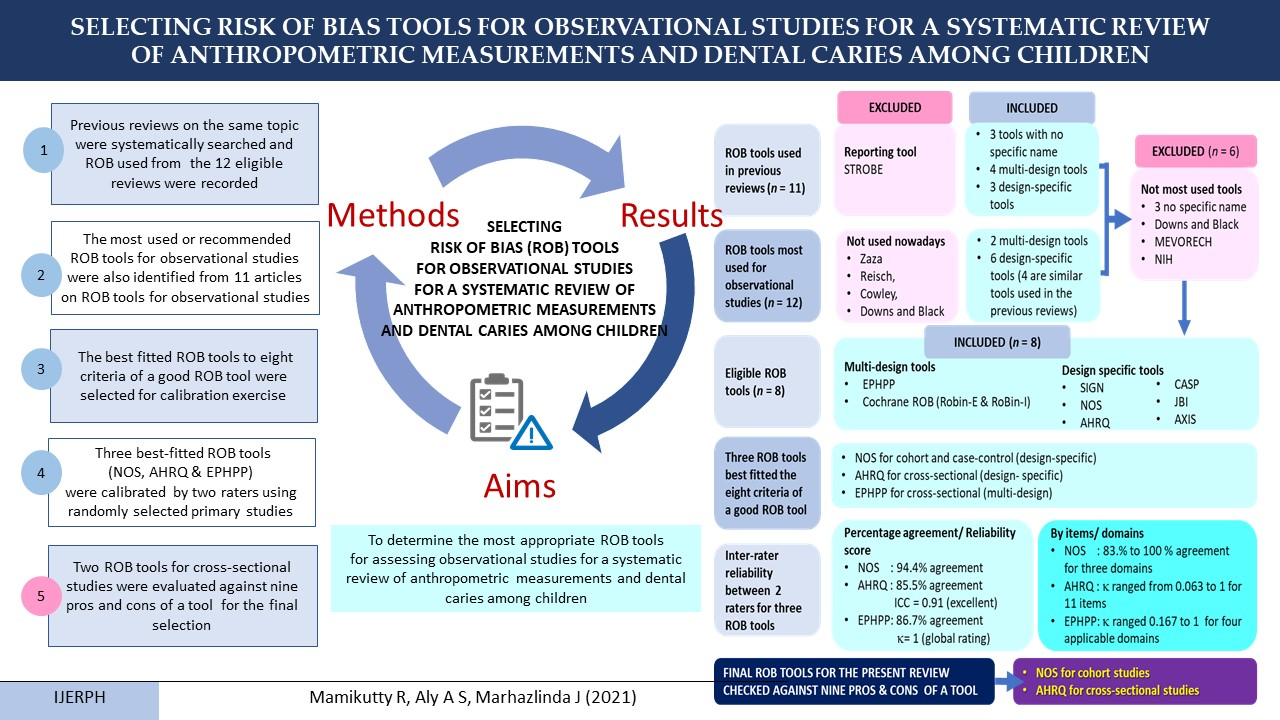
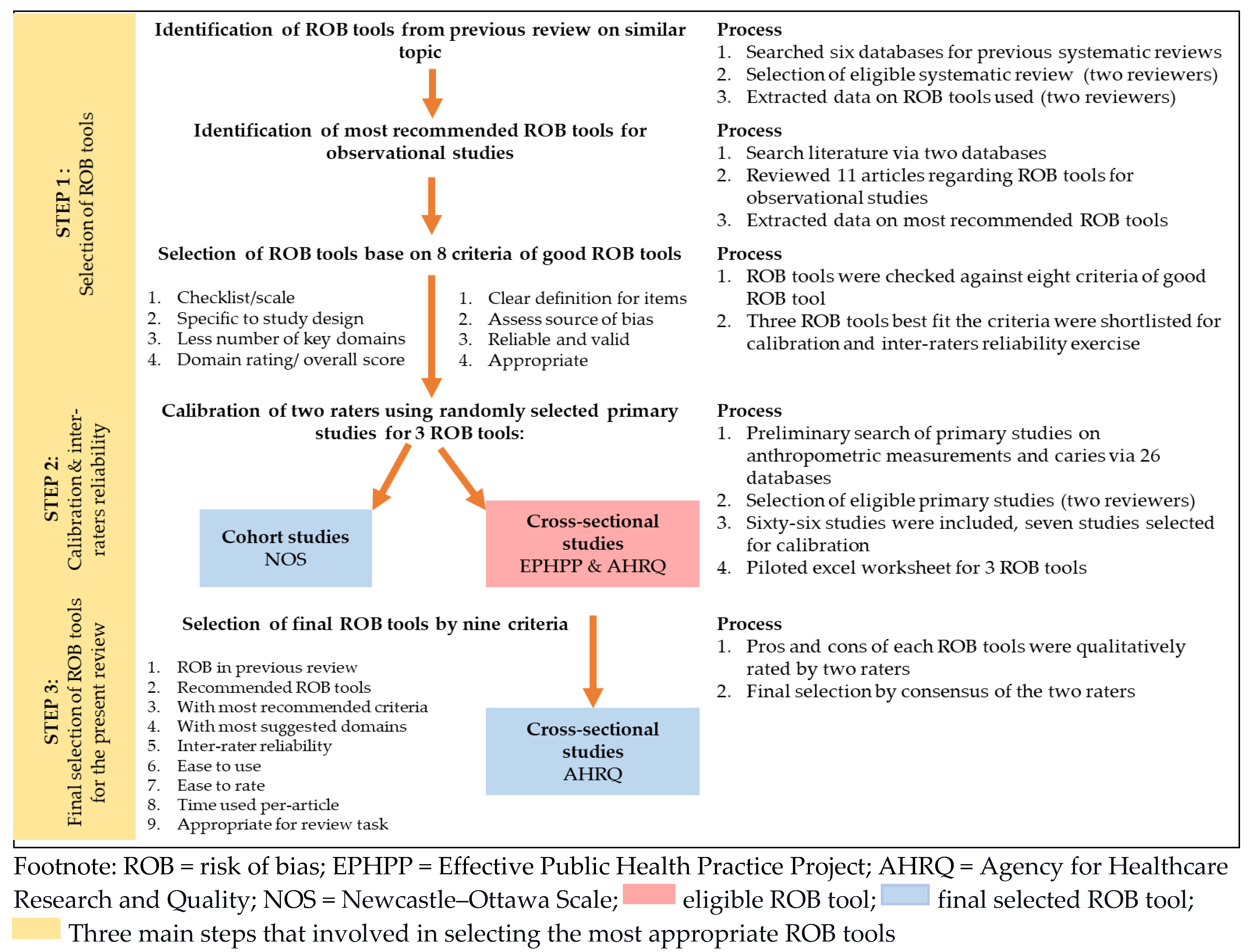
2.1. Selecting the Most Appropriate ROB Tools for Observational Studies in a Review of Anthropometric Measurements and Dental Caries among Children (Selecting the ROB Instruments)
2.1.1. Identifying the ROB Tools Used in the Previous Reviews of a Similar Topic
2.1.2. Identifying the Most Recommended ROB Tools for Observational Studies
2.1.3. Selecting the Most Appropriate ROB Tools for the Review
2.2. Calibration and Inter-Rater Reliability Test of the Selected ROB Tools
2.2.1. Selected ROB Tools (Instruments)
2.2.2. Rating Procedures
2.2.3. Data Analysis
2.3. Qualitative Evaluation of Pros and Cons of the Selected ROB Tools
3. Results
3.1. Selection of ROB Instruments
3.1.1. ROB Tools Used in Previous Reviews
3.1.2. Recommended ROB Tools for Observational Studies
3.1.3. Most Appropriate ROB Tools for the Included Observational Studies in the Present Review
3.2. Calibration and Inter-Rater Reliability of the Selected ROB Tools
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J. (Eds.) WVA: Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Taylor, K.; Allman-Farinelli, M.A.B.; Askie, L.; Ghersi, D.; McKenzie, J.; Norris, S.; Page, M.; Rooney, A.; Woodruff, T.; et al. A systematic review: Tools for assessing methodological quality of human observational studies. NHMRC 2019. Available online: https://osf.io/preprints/metaarxiv/pnqmy/ (accessed on 25 June 2021). [CrossRef] [Green Version]
- Hootman, J.M.; Driban, J.B.; Sitler, M.R.; Harris, K.P.; Cattano, N.M. Reliability and validity of three quality rating instruments for systematic reviews of observational studies. Res. Synth. Methods 2011, 2, 110–118. [Google Scholar] [CrossRef]
- West, S.; King, V.; Carey, T.; Lohr, K.; McKoy, N.; Sutton, S.; Lux, L. Systems to Rate the Strength of Scientific Evidence: Summary. In AHRQ Evidence Report Summaries; 2002 March edn.; Rockville (MD), Agency for Healthcare Research and Quality: Rockville, MD, USA, 2002; pp. 1–11. [Google Scholar]
- Bero, L.; Chartres, N.; Diong, J.; Fabbri, A.; Ghersi, D.; Lam, J.; Lau, A.; McDonald, S.; Mintzes, B.; Sutton, P. The risk of bias in observational studies of exposures (ROBINS-E) tool: Concerns arising from application to observational studies of exposures. Syst. Rev. 2018, 7, 242. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Dinnes, J.; D’Amico, R.; Sowden, A.J.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D.G. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7, 1–173. [Google Scholar] [CrossRef] [Green Version]
- Sanderson, S.; Tatt, I.D.; Higgins, J.P. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: A systematic review and annotated bibliography. Int. J. Epidemiol. 2007, 36, 666–676. [Google Scholar] [CrossRef] [Green Version]
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med Res. 2020, 7, 7. [Google Scholar] [CrossRef] [Green Version]
- Eick, S.M.; Goin, D.E.; Chartres, N.; Lam, J.; Woodruff, T.J. Assessing risk of bias in human environmental epidemiology studies using three tools: Different conclusions from different tools. Syst. Rev. 2020, 9, 249. [Google Scholar] [CrossRef]
- Mamikutty, R.; Aly, A.S.; Marhazlinda, J. Databases Selection in a Systematic Review of the Association between Anthropometric Measurements and Dental Caries among Children in Asia. Children 2021, 8, 565. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, L.; Santesso, N.; Tugwell, P.S.; Wells, G.A.; Judd, M.; Buchbinder, R. Method guidelines for Cochrane Musculoskeletal Group systematic reviews. J. Rheumatol. 2006, 33, 2304–2311. [Google Scholar]
- Viswanathan, M.; Ansari, M.; Berkman, N.; Chang, S.; Hartling, L.; McPheeters, L.; Santaguida, P.; Shamliyan, T.; Singh, K.; Tsertsvadze, A. Assessing the risk of bias of individual studies in systematic reviews of health care interventions. In Methods Guide for Effectiveness and Comparative Effectiveness Reviews; Rockville (MD), Agency for Healthcare Research and Quality: Rockville, MD, USA, 2012. [Google Scholar]
- Zeng, X.; Zhang, Y.; Kwong, J.S.; Zhang, C.; Li, S.; Sun, F.; Niu, Y.; Du, L. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. J. Evid. Based Med. 2015, 8, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Farrah, K.; Young, K.; Tunis, M.C.; Zhao, L. Risk of bias tools in systematic reviews of health interventions: An analysis of PROSPERO-registered protocols. Syst. Rev. 2019, 8, 280. [Google Scholar] [CrossRef]
- Zawacki-Richter, O.; Kerres, M.; Bedenlier, S.; Bond, M.; Buntins, K. Systematic Reviews in Educational Research: Methodology, Perspectives and Application; Springer Nature: Basingstoke, UK, 2020; p. 99. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D.a.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Oxford, UK. 2000. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 25 June 2021).
- Gupta, P.; Lanca, C.; Gan, A.T.L.; Soh, P.; Thakur, S.; Tao, Y.; Kumari, N.; Man, R.E.K.; Fenwick, E.K.; Lamoureux, E.L. The Association between Body Composition using Dual energy X-ray Absorptiometry and Type-2 Diabetes: A Systematic Review and Meta-Analysis of Observational studies. Sci. Rep. 2019, 9, 12634. [Google Scholar] [CrossRef] [Green Version]
- Rostom, A.; Dubé, C.; Cranney, A.; Saloojee, N.; Sy, R.; Garritty, C.; Sampson, M.; Zhang, L.; Yazdi, F.; Mamaladze, V. Appendix D. In Quality Assessment Forms; 2004 Sep. (Evidence Reports/Technology assessments, No. 104.); Rockville (MD), Agency for Healthcare Research and Quality: Rockville, MD, USA, 2014. [Google Scholar]
- Chen, D.; Zhi, Q.; Zhou, Y.; Tao, Y.; Wu, L.; Lin, H. Association between Dental Caries and BMI in Children: A Systematic Review and Meta-Analysis. Caries Res. 2018, 52, 230–245. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H.; Ciliska, D.; Dobbins, M. Quality assessment tool for quantitative studies. In Toronto: Effective Public Health Practice Project; McMaster University: Hamilton, ON, Canada, 2003. [Google Scholar]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef] [Green Version]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009; Volume 892. [Google Scholar]
- Fleiss, J.L.; Levin, B.; Paik, M.C. Statistical Methods for Rates and Proportions; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Jeyaraman, M.M.; Rabbani, R.; Al-Yousif, N.; Robson, R.C.; Copstein, L.; Xia, J.; Pollock, M.; Mansour, S.; Ansari, M.T.; Tricco, A.C.; et al. Inter-rater reliability and concurrent validity of ROBINS-I: Protocol for a cross-sectional study. Syst. Rev. 2020, 9, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantovitz, K.R.; Pascon, F.M.; Rontani, R.M.; Gavião, M.B. Obesity and dental caries—A systematic review. Oral Health Prev. Dent. 2006, 4, 137–144. [Google Scholar]
- Hooley, M.; Skouteris, H.; Boganin, C.; Satur, J.; Kilpatrick, N. Body mass index and dental caries in children and adolescents: A systematic review of literature published 2004 to 2011. Syst. Rev. 2012, 1, 57. [Google Scholar] [CrossRef] [Green Version]
- Hayden, C.; Bowler, J.O.; Chambers, S.; Freeman, R.; Humphris, G.; Richards, D.; Cecil, J.E. Obesity and dental caries in children: A systematic review and meta-analysis. Community Dent. Oral Epidemiol. 2013, 41, 289–308. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.E.; Menezes, A.M.; Demarco, F.F.; Vargas-Ferreira, F.; Peres, M.A. Obesity and dental caries: Systematic review. Rev. Saúde Pública 2013, 47, 799–812. [Google Scholar] [CrossRef]
- Li, L.-W.; Wong, H.M.; Peng, S.-M.; McGrath, C.P. Anthropometric measurements and dental caries in children: A systematic review of longitudinal studies. Adv. Nutr. 2015, 6, 52–63. [Google Scholar] [CrossRef] [Green Version]
- Shivakumar, S.; Srivastava, A.; Shivakumar, G.C. Body Mass Index and Dental Caries: A Systematic Review. Int. J. Clin. Pediatr. Dent. 2018, 11, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Paisi, M.; Kay, E.; Bennett, C.; Kaimi, I.; Witton, R.; Nelder, R.; Lapthorne, D. Body mass index and dental caries in young people: A systematic review. BMC Pediatr. 2019, 19, 122. [Google Scholar] [CrossRef] [PubMed]
- Angelopoulou, M.V.; Beinlich, M.; Crain, A. Early Childhood Caries and Weight Status: A Systematic Review and Meta-Analysis. Pediatr. Dent. 2019, 41, 261–272. [Google Scholar]
- Alshihri, A.A.; Rogers, H.J.; Alqahtani, M.A.; Aldossary, M.S. Association between Dental Caries and Obesity in Children and Young People: A Narrative Review. Int. J. Dent. 2019, 2019, 9105759. [Google Scholar] [CrossRef]
- Alshehri, Y.F.A.; Park, J.S.; Kruger, E.; Tennant, M. Association between body mass index and dental caries in the Kingdom of Saudi Arabia: Systematic review. Saudi Dent. J. 2020, 32, 171–180. [Google Scholar] [CrossRef]
- Manohar, N.; Hayen, A.; Fahey, P.; Arora, A. Obesity and dental caries in early childhood: A systematic review and meta-analyses. Obes. Rev. 2020, 21, e12960. [Google Scholar] [CrossRef]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [Green Version]
- Morgan, R.L.; Thayer, K.A.; Santesso, N.; Holloway, A.C.; Blain, R.; Eftim, S.E.; Goldstone, A.E.; Ross, P.; Ansari, M.; Akl, E.A.; et al. A risk of bias instrument for non-randomized studies of exposures: A users’ guide to its application in the context of GRADE. Environ. Int. 2019, 122, 168–184. [Google Scholar] [CrossRef]
- Yang, J.C.; Yang, Z.R.; Yu, S.Q.; Zhan, S.Y.; Sun, F. Introduction on ’assessing the risk of bias of individual studies’ in systematic review of health-care intervention programs revised by the Agency for Healthcare Research and Quality. Zhonghua Liu Xing Bing Xue Za Zhi 2019, 40, 106–111. [Google Scholar] [CrossRef]
- Moskalewicz, A.; Oremus, M. No clear choice between Newcastle–Ottawa Scale and Appraisal Tool for Cross-Sectional Studies to assess methodological quality in cross-sectional studies of health-related quality of life and breast cancer. J. Clin. Epidemiol. 2020, 120, 94–103. [Google Scholar] [CrossRef]
- Basha, S.; Mohamed, R.N.; Swamy, H.S.; Ramamurthy, P.H.; Sexena, V. Caries Incidence Among Obese Adolescents: A 3-year Prospective Study. Oral Health Prev. Dent 2017, 15, 65–71. [Google Scholar]
- Li, L.W.; Wong, H.M.; McGrath, C.P. Longitudinal Association between Obesity and Dental Caries in Adolescents. J. Pediatr. 2017, 189, 149–154e145. [Google Scholar] [CrossRef]
- Begum, M.Z.; Nagamalleshwari, M.; Sriniva, P.; Gadagi, J.; Gadde, P.; Jyothirmai, K. Is body mass index truly related to dental caries? Survey on predisposing factors for overweight among Indian school children. Dent. Hypotheses 2014, 5, 150–154. [Google Scholar] [CrossRef]
- Dikshit, P.; Limbu, S.; Bhattarai, R. Relationship of Body Mass Index with Dental Caries among Children attending Pediatric Dental Department in an Institute. JNMA J. Nepal Med. Assoc. 2018, 56, 582–586. [Google Scholar] [CrossRef]
- Elangovan, A.; Mungara, J.; Joseph, E. Exploring the relation between body mass index, diet, and dental caries among 6-12-year-old children. J. Indian Soc. Pedod. Prev. Dent. 2012, 30, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Farsi, D.J.; Elkhodary, H.M.; Merdad, L.A.; Farsi, N.M.; Alaki, S.M.; Alamoudi, N.M.; Bakhaidar, H.A.; Alolayyan, M.A. Prevalence of obesity in elementary school children and its association with dental caries. Saudi Med. J. 2016, 37, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Goodson, J.M.; Tavares, M.; Wang, X.; Niederman, R.; Cugini, M.; Hasturk, H.; Barake, R.; Alsmadi, O.; Al-Mutawa, S.; Ariga, J.; et al. Obesity and dental decay: Inference on the role of dietary sugar. PLoS ONE 2013, 8, e74461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B.; et al. Meta-analysis of Observational Studies in EpidemiologyA Proposal for Reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Quigley, J.M.; Thompson, J.C.; Halfpenny, N.J.; Scott, D.A. Critical appraisal of nonrandomized studies-A review of recommended and commonly used tools. J. Eval. Clin. Pract. 2019, 25, 44–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J. Meta-Anal. 2017, 5, 80–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Authors | Titles | Tools | Study Designs | Comments |
|---|---|---|---|---|
| Kantovitz et al. [26] | Obesity and dental caries: systematic review | Swedish Council on Technology Assessment in Health Care | Cohort Case-control Cross-sectional | ROB tool name not mentioned |
| Hooley et al. [27] | Body mass index and dental caries in children and adolescents: a systematic review of the literature published 2004 to 2011 | Evaluated based on several criteria to assess the quality of methodology, i.e., representative of the sample, control confounder, BMI measure, dental caries measure | Cohort Case-control Cross-sectional | ROB tool name not mentioned. |
| Hayden et al. [28] | Obesity and dental caries in children: a systematic review and meta-analysis | Appraisal checklists developed by the University of Wales (HEB Wales critical appraisal checklist) | Cohort Case-control Cross-sectional | Multi design tools |
| Silva et al. [29] | Obesity and dental caries: systematic review | Downs and Black Of 27 items, 18 items selected. | Cohort Case-control Cross-sectional | Multi design tools |
| Li et al. [30] | Anthropometric Measurements and Dental Caries in Children: A Systematic Review of Longitudinal Studies | STROBE | Case-control Cohort Cross-sectional nested in a birth cohort study | Not ROB tool |
| Chen et al. [20] | Association between Dental Caries and BMI in Children: A Systematic Review and Meta-Analysis | AHRQ (Modified version) | Cross-sectional | Design specific |
| Shivakumar et al. [31] | Body Mass Index and Dental Caries: A Systematic Review | Downs and Black Out of 27, 10 items excluded as it applied for intervention studies. | Case-control Cross-sectional Cohort | Multi design tools |
| Paisi et al. [32] | Body mass index and dental caries in young people: a systematic review | MEVORECH | Case-control Cross-sectional | Multi design tools |
| Angelopoulou et al. [33] | Early Childhood Caries and Weight Status: A Systematic Review and Meta-Analysis | NIH | Cross-sectional | Multi design tool |
| Alshiri et al. [34] | Association between Dental Caries and Obesity in Children and Young People: A Narrative Review | Not applicable (Narrative review) | Case-control Cross-sectional Cohort | Not applicable |
| Alshehri et al. [35] | Association between body mass index and dental caries in the Kingdom of Saudi Arabia: Systematic review | AXIS | Cross-sectional | Design specific |
| Manohar et al. [36] | Obesity and dental caries in early childhood: A systematic review and meta-analyses | JBI and ROBINS-I | Cross-sectional nested in a cohort Case-Control Cohort | Design specific |
| Authors | Most Used/Recommended ROB Tools (Multi-Design) | Most Used/Recommended ROB Tools (Design-Specific) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Downs & Black | Zaza | Reisch | Cowley | Cochrane ROB | EPHPP | SIGN | NOS | AHRQ | CASP | JBI | AXIS | |
| West et al. [5] | C CC | C CC | C CC | |||||||||
| Deeks et al. [7] | C CC | C CC | C CC | C CC | C CC CS | C CC | ||||||
| Maxwell et al. [12] | C CC | C CC | C CC | |||||||||
| Sanderson et al. [8] | Lack of single obvious tool for observational studies | |||||||||||
| Higgins et al. [2] | C CC | ** | ** | ** | C CC | |||||||
| Viswanathan et al. [13] | # | C CC | ||||||||||
| Zeng et al. [14] | C CC | C CC | CS | C CC | ||||||||
| NICE | C CC CS | NRS | C CC CS | C CC | C CC | |||||||
| Wang et al. [3] | ## | ## | ||||||||||
| All the above tools except Reisch and Cowley were listed, but no recommendation was given. | ||||||||||||
| Farah et al. [15] | C CC CS | NRS | C CC CS | C CC | C CC | C CC | C CC CS | |||||
| Ma et al. [9] | * | * | * | * | NRS | C CC | CS | CS | ||||
| Conclusion | X | X | X | X | √ | √ | √ | √ | √ | √ | √ | √ |
 multi-design ROB tools,
multi-design ROB tools,  design-specific ROB tools.
design-specific ROB tools.| No | Criteria | Recommended/Most Used ROB Tools for Observational Studies | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ROBINS-E | ROBINS-I | EPHPP | SIGN | NOS | AHRQ | CASP | JBI | AXIS | ||
| 1 | Applicability (checklist/ scale) | Risk of bias in non-randomized studies - of exposures (ROBINS-E) (checklist) | Risk of bias in non-randomised studies - of interventions (ROBINS-I) (checklist) | Effective Public Health Practice Project (EPHPP) for quality assessment (checklist) | Scottish Intercollegiate Guidelines Network (SIGN) (Methodology checklist) | Newcastle–Ottawa Scale (NOS) for quality assessment (checklist) | Agency for Healthcare Research and Quality (AHRQ) (Methodology checklist) | Critical Appraisal Skills Programme (CASP) critical appraisal tool (checklist) | Joanna Briggs Institute tools (JBI) for a critical appraisal (checklist) | The critical appraisal tool for Cross-Sectional Studies (AXIS) (checklist) |
| 2 | Design specific / multi-design and type of study | Multi-design. Non-randomised studies. | Multi-design. Non-randomised studies of intervention (cohort-like design). | Multi-design. Quantitative studies. | Design-specific. Cohort. Case-control. | Design-specific. Non-randomised studies. Cohort. Case-control. | Design-specific. Cohort. Case-control. Cross-sectional. Case series. | Design-specific. Cohort. Case-control. | Design-specific. Cohort. Case-control. Cross-sectional. | Design-specific. Cross-sectional studies. |
| 3 | Number of items and domains | 35 Items 7 Domains | 34 Items 7 Domains | 21 Items 8 Domains | C:18 Items C/C: 15 items 4 Domains | 8 Items 3 Domains | C/S: 11 items | C: 12 items C/C: 11 items | 8 items | 20 items 5 domains |
| 4 | Domain rating | Yes | Yes | Yes | No | Yes | No | No | No | No |
| 5 | Clear definition of items/ manual | NA | Manual provided | Manual provided | Manual provided | Manual Provided [17] | Hints are Provided | Hints are provided | Manual provided | Manual provided |
| 6 | Concentrate on the source of bias (nine domains by Wang et al., [3]) | NA | 6/9 domains Selection. Exposure. Outcome. Selective reporting. Analysis. Confounders. | 6/9 domains Selection. Outcome. Confounding. Loss to follow-up. Analysis. | 5/9 domains Selection. Exposure. Confounder. Outcome. Analysis. | 4/9 domains Selection. Exposure. Confounder. Outcome. | 5/9 domains. Selection. Exposure. Outcome. Confounding. Loss of follow-up. | 4/9 domains Selection. Exposure. Outcome. Analys is. | 5/9 domains. Selection. Exposure. Outcome. Confounding. Analysis. | 5/9 domains Selection. Outcome. Confounding. Analysis. Conflict of interest. |
| 7 | Validity and Reliability | N/A | Unclear A Protocol was published to assess the reliability and validity of this tool [25]. | Content and construct validity and inter-rater reliability tested [21,37]. | Unclear | Established content validity, inter-rater reliability and criterion validity being examined [17]. | Unclear Expert consultation. | Unclear Experts piloted checklist [3]. | Unclear Peer reviewed. | Unclear Three rounds of the Delphi expert consultation [38]. |
| 8 | Appropriate for task a. Usability | The tool is under development | For intervention, not exposure. Used in a previous review [36]. Guide to incorporate GRADE [39]. | Comprise of global Rating. Easy to use. Good for systematic review [21,37]. | Less recommended compared with NOS (Cohort and C/C). | Frequently used Easy to use. May incorporate in RevMan. The best tool for cohort and case-control [14]. | Frequently used for CS [14]. Suitable for descriptive cross- sectional studies [9]. Used in a previous review [20]. Can be incorporated in RevMan [40]. | Less recommended compared with NOS for cohort and C/C studies. | Preferred for analytic cross- sectional studies and descriptive cross- sectional studies [9]. Used in a previous review [36]. | Can be changed and improved where Required. Used in a previous review [35]. |
| b. Issues/ limitation | This tool is under development. Time-consuming & confusing [6]. | For intervention, not exposure. Required substantial epidemiological expertise. Not suitable for present review topic (exposure). | Manual provided. It may be interpreted differently by a different user. Items need to be customised to the review question. | Lack of comprehensive manual which means instruction may interpreted differently by a different user. | No rating/ scale. New tool [9] not much used. | New tools. Critical appraisal tool [9]. Poor inter-rater reliability compared with NOS [41]. No clear psychometrics properties [41]. | ||||
| Shortlisted tools | X | X | √ Multi-design | X | √ Cohort/ Case-control | √ Cross-sectional | X | X | X | |
 multi-design ROB tools,
multi-design ROB tools,  design-specific ROB tools.
design-specific ROB tools.| Article | Rater | Selection | Comparability | Outcome | Total Score | Rating | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | T | Q1a | Q1b | T | Q1 | Q2 | Q3 | T | ||||
| Basha et al. [42] | R1 | * | * | * | * | 4 | * | * | 2 | * | * | * | 3 | 9 | Low risk |
| R2 | * | * | * | * | 4 | * | * | 2 | * | * | * | 3 | 9 | Low risk | |
| C | * | * | * | * | 4 | * | * | 2 | * | * | * | 3 | 9 | Low risk | |
| Li et al. [43] | R1 | * | * | * | * | 4 | * | * | 2 | * | * | * | 3 | 9 | Low risk |
| R2 | * | * | * | * | 4 | * | * | 2 | * | * | 2 | 8 | Low risk | ||
| C | * | * | * | * | 4 | * | * | 2 | * | * | * | 3 | 9 | Low risk | |
 low risk bias.
low risk bias. | AHRQ | EPHPP | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Items | Total | Rating | Domains | ||||||||||||||||||
| Article | Rater | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Selection bias | Study design | Confounder | Blinding | Data Collection method | Withdrawal/ dropout | Global rating | ||
| Begum et al. [44] | R1 | + | + | + | - | ? | + | + | + | NA | - | + | 7 | M | S | W | M | NA | M | NA | M |
| R2 | + | + | + | - | ? | ? | + | + | NA | ? | + | 6 | M | S | W | M | NA | S | NA | M | |
| C | + | + | + | - | ? | + | + | + | NA | - | + | 7 | M | S | W | M | NA | M | NA | M | |
| Diksit et al. [45] | R1 | + | + | - | + | ? | ? | ? | + | NA | + | + | 6 | M | M | W | W | NA | W | NA | W |
| R2 | + | + | - | + | ? | ? | ? | + | NA | - | + | 5 | M | M | W | W | NA | W | NA | W | |
| C | + | + | - | + | ? | ? | ? | + | NA | + | + | 6 | M | M | W | W | NA | W | NA | W | |
| Elangovan et al. [46] | R1 | + | + | + | + | ? | + | + | NA | + | ? | 7 | M | S | W | W | NA | W | NA | W | |
| R2 | + | + | + | + | ? | + | + | + | NA | + | ? | 8 | M | S | W | W | NA | S | NA | W | |
| C | + | + | + | + | ? | + | ? | + | NA | + | ? | 7 | M | S | W | W | NA | W | NA | W | |
| Farsi et al. [47] | R1 | + | + | + | + | + | + | + | + | NA | + | + | 10 | L | S | W | W | NA | S | NA | W |
| R2 | + | + | + | + | + | + | + | + | NA | ? | + | 9 | L | S | W | W | NA | W | NA | W | |
| C | + | + | + | + | + | + | + | + | NA | + | + | 10 | L | S | W | W | NA | S | NA | W | |
| Goodman et al. [48] | R1 | + | + | - | + | ? | ? | ? | ? | NA | + | + | 5 | M | S | W | M | NA | W | NA | W |
| R2 | + | + | - | + | ? | + | - | - | NA | + | + | 6 | M | S | W | W | NA | W | NA | W | |
| C | + | + | - | + | ? | ? | ? | ? | NA | + | + | 5 | M | S | W | M | NA | W | NA | W | |
| Qualitative Characteristic | Descriptions | EPHPP | AHRQ | Consensus | |
|---|---|---|---|---|---|
| 1 | Used in previous SR | Tested with a similar review topic | X | √ | AHRQ |
| 2 | Most used/recommended by literature | Frequently cited by literature | √ (Multi-design) | √ (Design-specific) | Both |
| 3 | Contains recommended criteria | 1. Methodological checklist | √ | √ | EPHPP |
| 2. Reliability and validity | √ | Unclear | |||
| 3. Design specific | X | √ | |||
| 4. Domain rating | √ | X | |||
| 5. Clear definition of items/manual | √ | X | |||
| 4 | Contains most domains as suggested by Wang et al. [3] | a. Selection | EPHPP | ||
| Sample representative of the target population | √ | √ | |||
| Comparability of exposure and comparison groups | √ | X | |||
| Appropriateness of eligibility criteria | √ | √ | |||
| Recruitment time frame | √ | √ | |||
| Non-response rate | √ | √ | |||
| b. Exposure | |||||
| Validity and reliability of exposure measurement | √ | √ | |||
| c. Outcome assessment | |||||
| Accuracy of outcome measurement | √ | √ | |||
| Blinding of the research staff | NA | NA | |||
| d. Confounding | |||||
| Description of confounding variables | √ | √ | |||
| Accounting for confounding | √ | √ | |||
| e. Loss of follow-up | |||||
| Adequacy of the length of follow-up | √ | √ | |||
| Amount of loss of follow-up | √ | √ | |||
| Handling of loss of follow-up | √ | √ | |||
| f. Analysis | |||||
| Appropriate statistical method | √ | X | |||
| g. Selective reporting | |||||
| Selective reporting of outcome | X | X | |||
| h. COI e.g., funding | X | X | |||
| i. Other bias | X | X | |||
| Total Domain | 6/9 | 5/9 | |||
| 5 | Inter-rater reliability (calibration) | a. Overall | κ = 1 | ICC = 0.91 | Both excellent |
| b. By item/domain (range) | Κ = 0.167 to 1 | Κ = 0.063 to 1 | Both need improvement | ||
| 6 | Ease of use | Easy | Difficult | EPHPP | |
| 7 | Ease of rating values for each item | Easy | Difficult | EPHPP | |
| 8 | Time per article | 30 min | 30 min | Both | |
| 9 | Appropriate for the task | a. Of 66 included studies in the systematic review, 64 were cross-sectional studies, and two were cohort studies; thus, design-specific ROB is more useful. | AHRQ better to rate cross-sectional studies | ||
| b. EPHPP includes study design as one of the domains; thus, it lowered the rating due to study design, making it less suitable. | |||||
| c. AHRQ does not have a clear manual; hence, a manual that is topic-specific should be developed before the actual assessment | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamikutty, R.; Aly, A.S.; Marhazlinda, J. Selecting Risk of Bias Tools for Observational Studies for a Systematic Review of Anthropometric Measurements and Dental Caries among Children. Int. J. Environ. Res. Public Health 2021, 18, 8623. https://doi.org/10.3390/ijerph18168623
Mamikutty R, Aly AS, Marhazlinda J. Selecting Risk of Bias Tools for Observational Studies for a Systematic Review of Anthropometric Measurements and Dental Caries among Children. International Journal of Environmental Research and Public Health. 2021; 18(16):8623. https://doi.org/10.3390/ijerph18168623
Chicago/Turabian StyleMamikutty, Rokiah, Ameera Syafiqah Aly, and Jamaludin Marhazlinda. 2021. "Selecting Risk of Bias Tools for Observational Studies for a Systematic Review of Anthropometric Measurements and Dental Caries among Children" International Journal of Environmental Research and Public Health 18, no. 16: 8623. https://doi.org/10.3390/ijerph18168623
APA StyleMamikutty, R., Aly, A. S., & Marhazlinda, J. (2021). Selecting Risk of Bias Tools for Observational Studies for a Systematic Review of Anthropometric Measurements and Dental Caries among Children. International Journal of Environmental Research and Public Health, 18(16), 8623. https://doi.org/10.3390/ijerph18168623