
Phenotypic Clustering in Non-Cystic Fibrosis Bronchiectasis Patients: The Role of Eosinophils in Disease Severity

 , , , ,
, , , ,  , , and
, , and 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
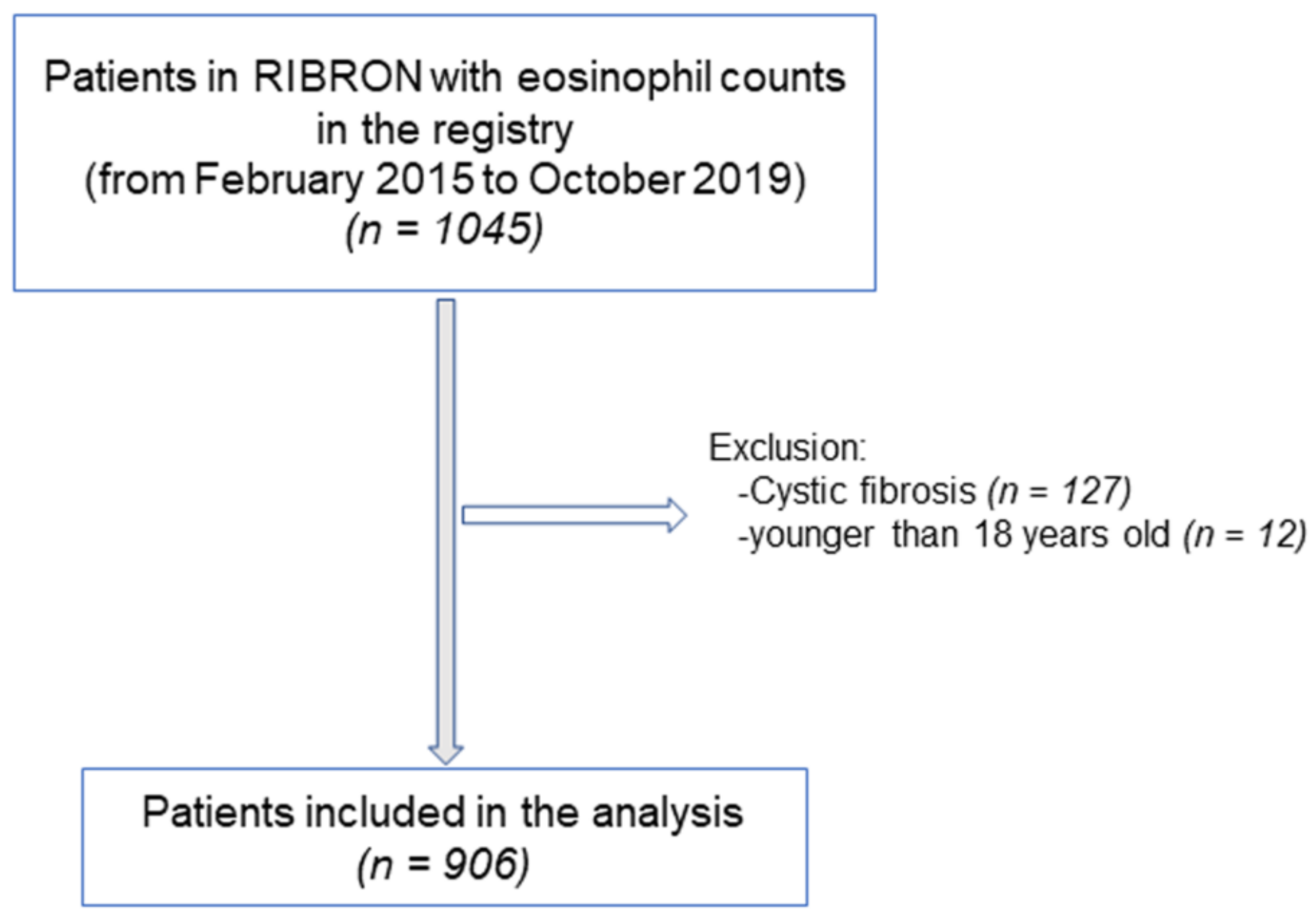
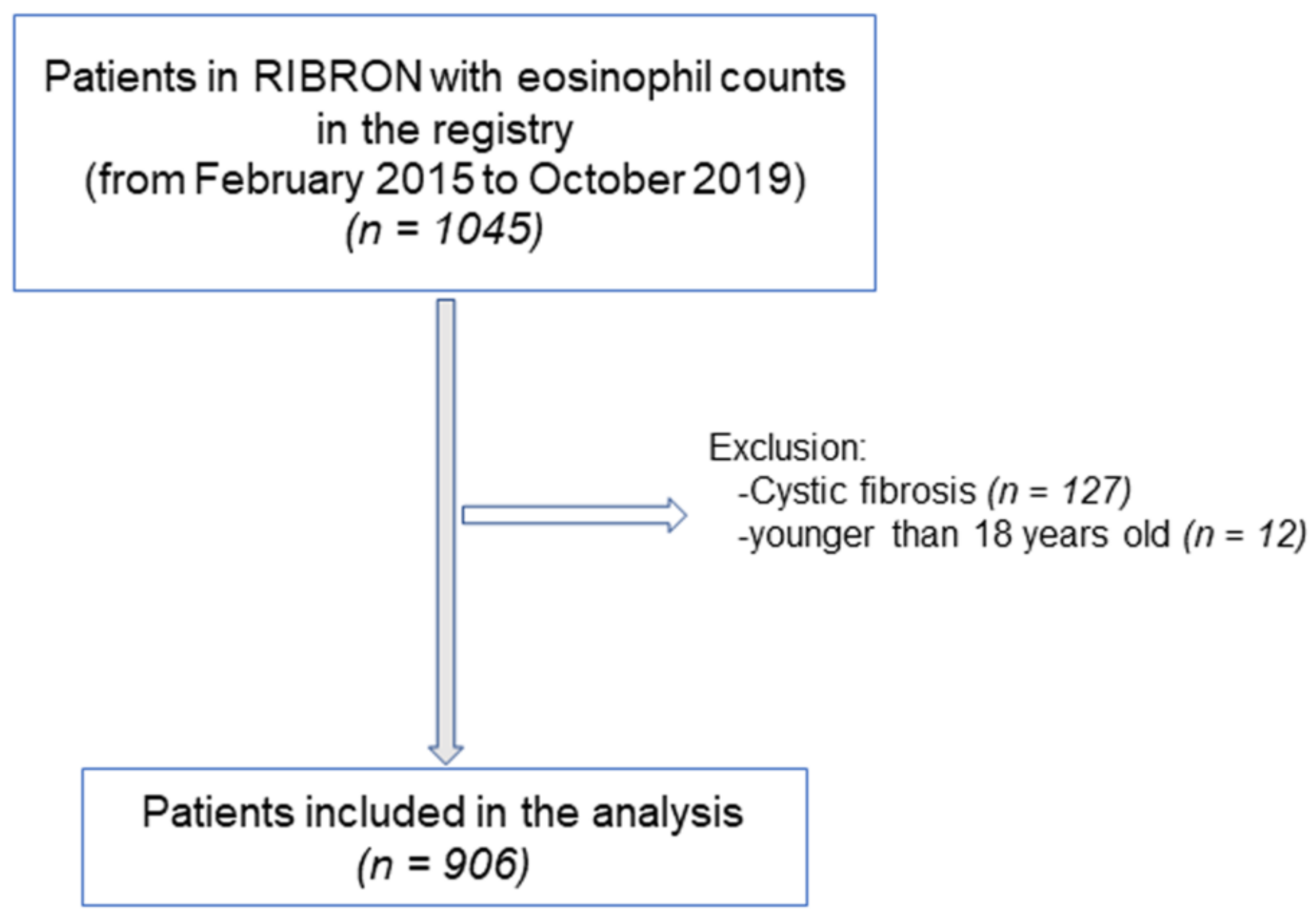
2.2. Study Population
2.3. Study Variables and Scores
2.4. Severity Scores
2.5. Patient Clustering
2.6. Statistical Analysis
3. Results
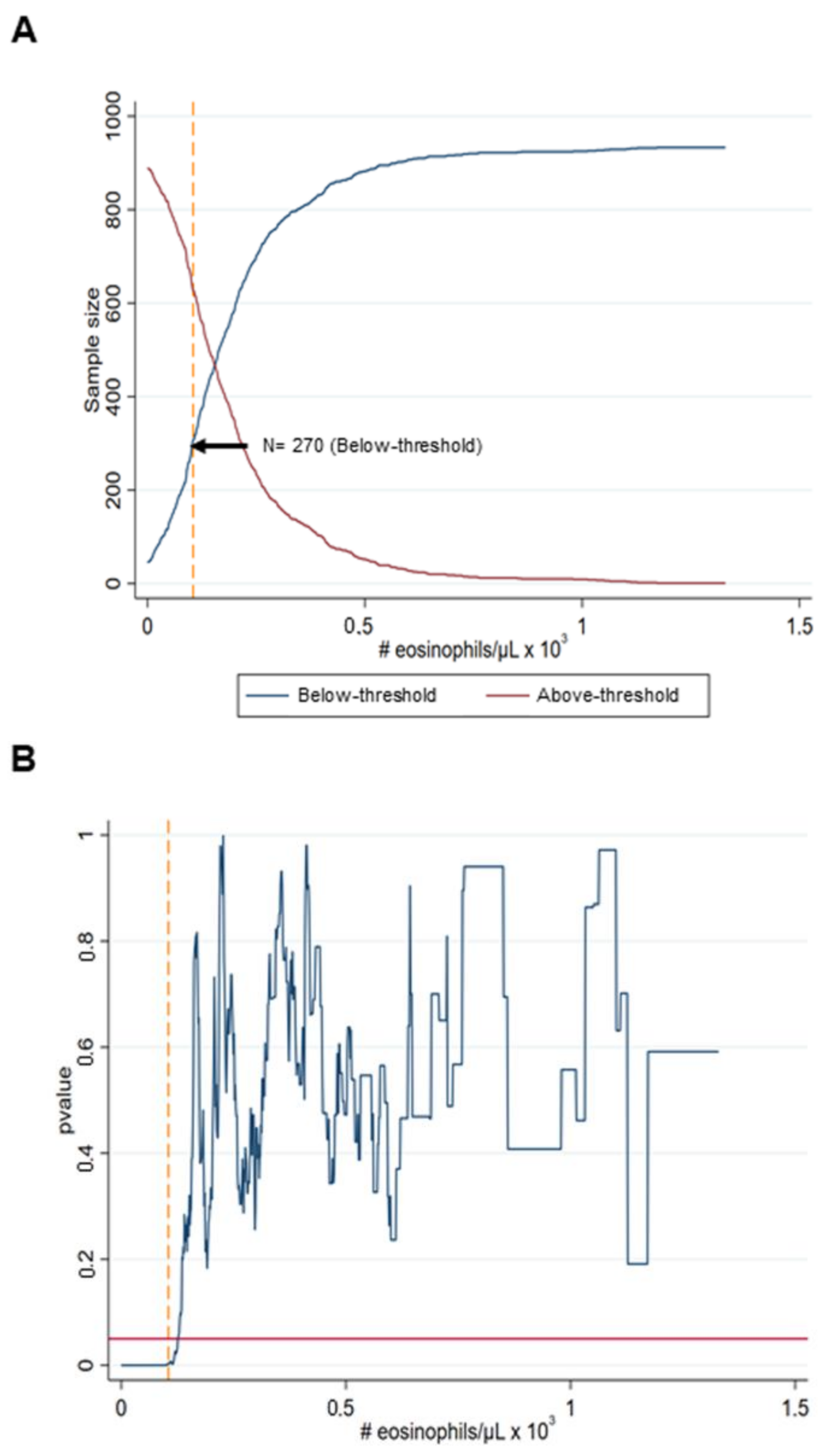
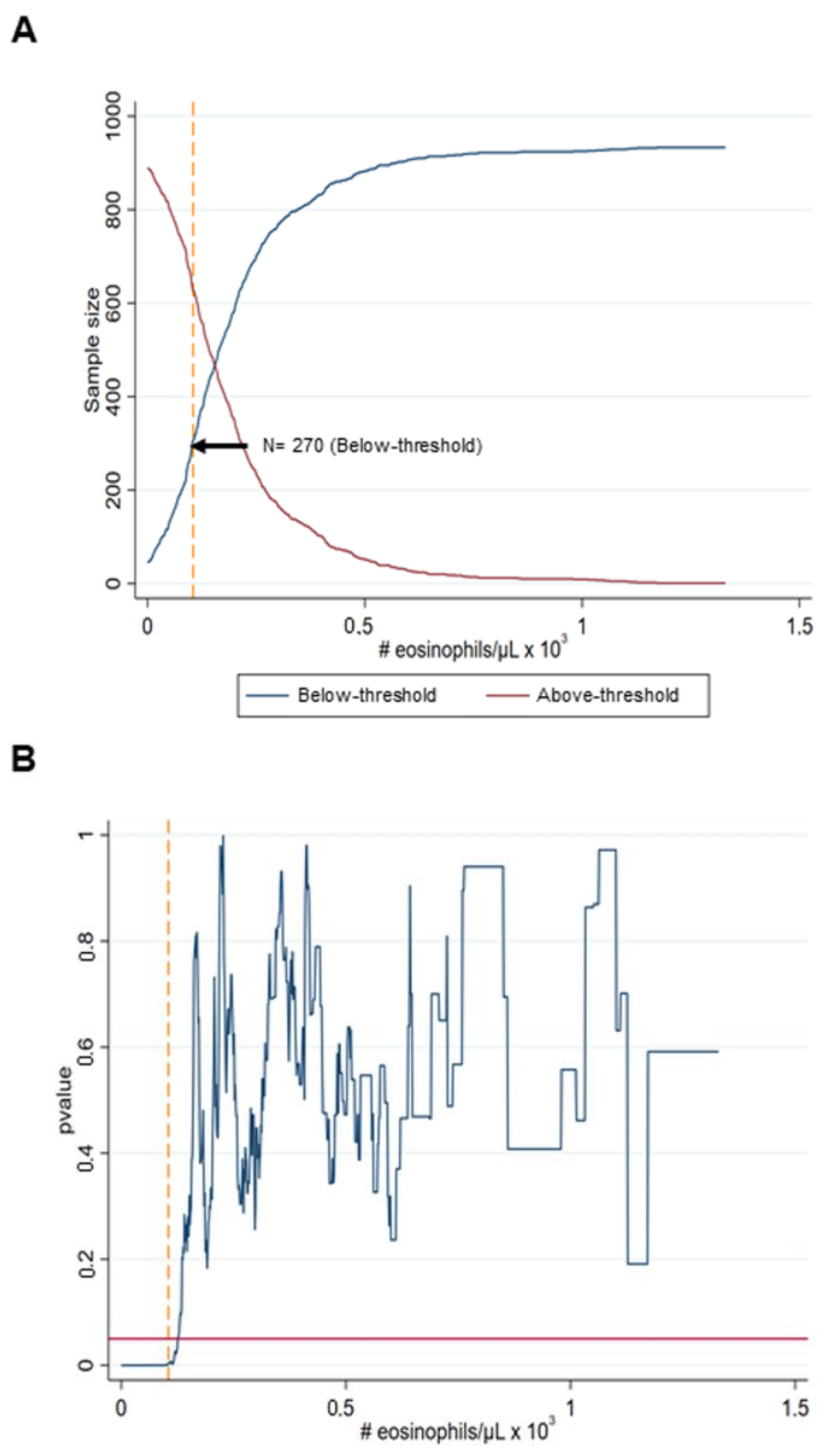
3.1. Cut-off Analysis
3.2. Anthropometry
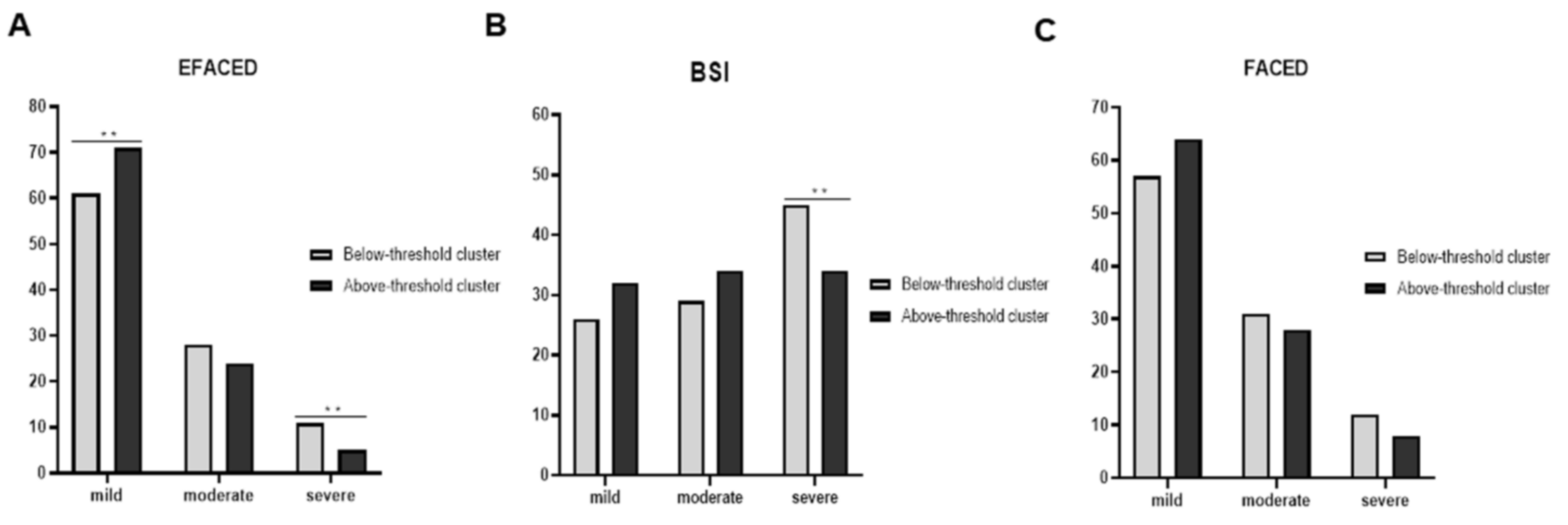
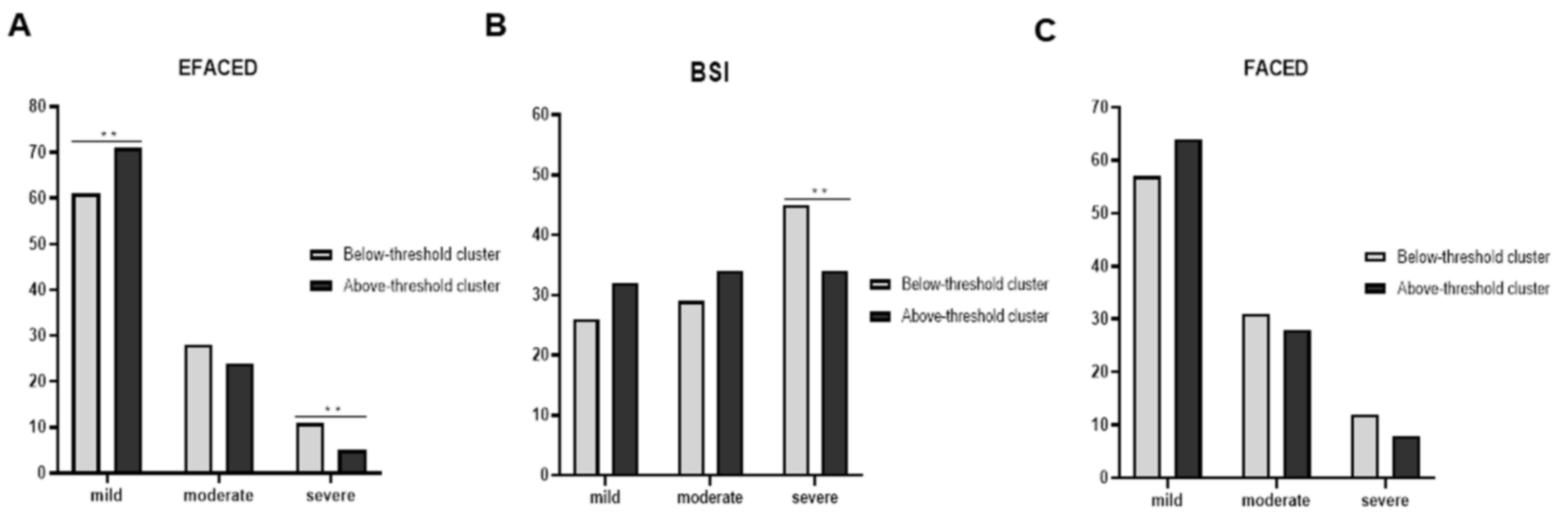
3.3. Disease Severity
3.4. Lung Function
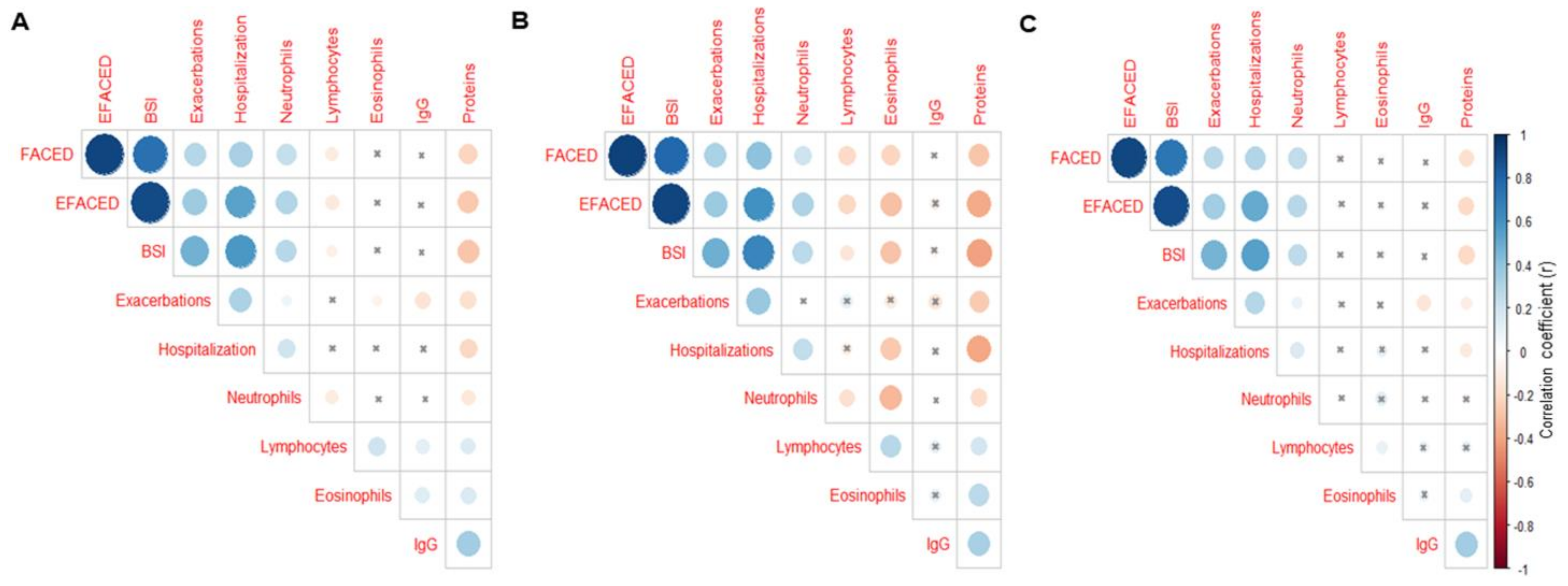
3.5. Blood Inflammatory Markers
3.6. Etiology of Non-CF Bronchiectasis
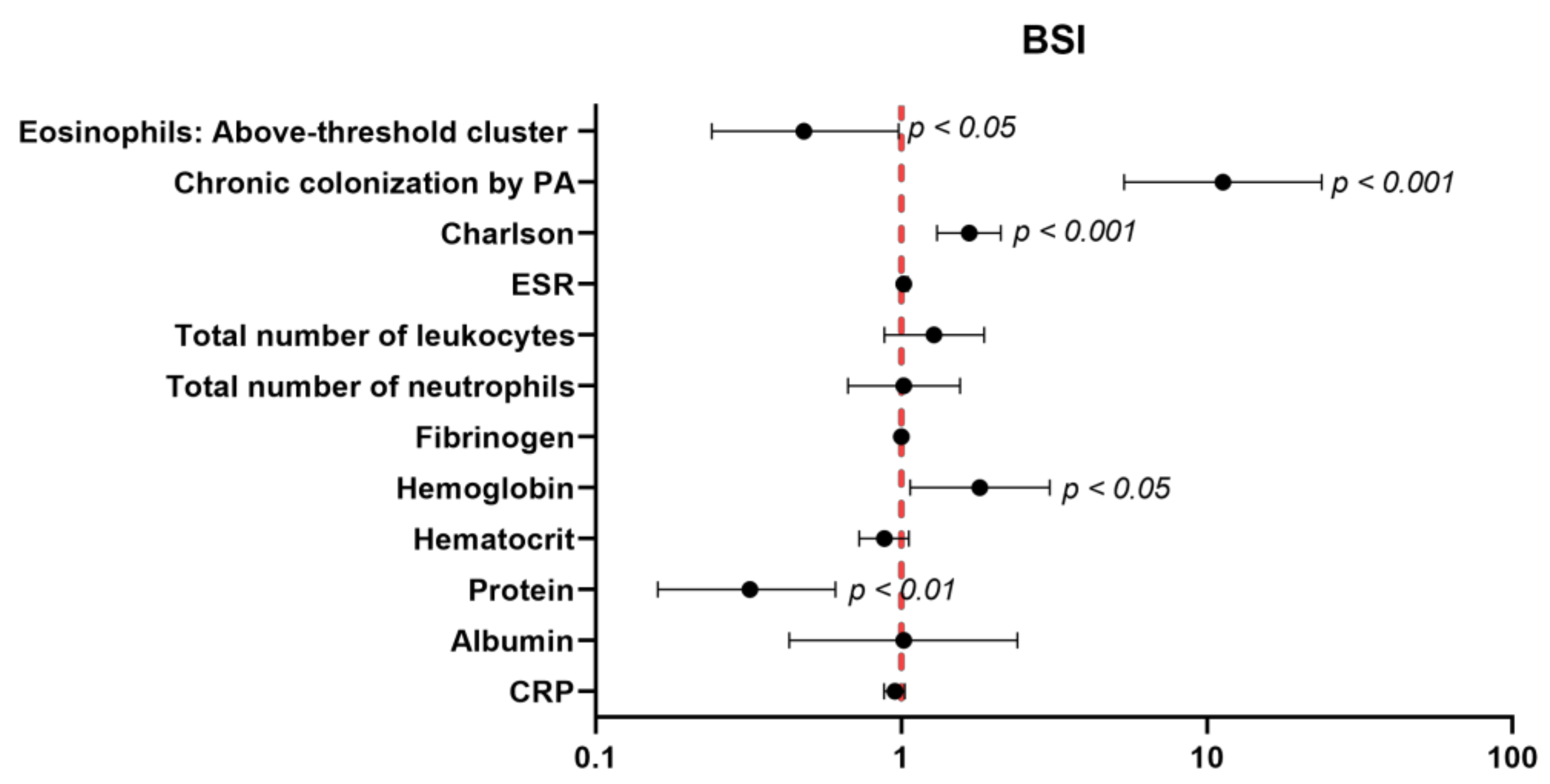
3.7. Multivariate Analyses
4. Discussion
Study Critique
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martinez-Garcia, M.A.; Agustí, A. Heterogeneidad y complejidad del síndrome bronquiectasias: Un reto pendiente. Arch. Bronconeumol. 2019, 55, 187–188. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Garcia, M.A.; de la Rosa, D.; Cantón, R.; Olveira, C.; Máiz-Carro, L.; Girón, R.; Prados, C.; Blanco, M. Bronquiectasias: Cuando la evidencia científica publicada no resulta suficiente. Arch. Bronconeumol. 2019, 55, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Martínez-García, M.A.; Olveira, C.; Máiz, L.; Girón, R.M.; Prados, C.; de la Rosa, D.; Blanco, M.; Agustí, A. Bronchiectasis: A Complex, Heterogeneous Disease. Arch. Bronconeumol. 2019, 55, 427–433. [Google Scholar] [CrossRef]
- Menéndez, R.; Méndez, R.; Amara-Elori, I.; Reyes, S.; Montull, B.; Feced, L.; Alonso, R.; Amaro, R.; Alcaraz, V.; Fernandez-Barat, L.; et al. Systemic Inflammation during and after Bronchiectasis Exacerbations: Impact of Pseudomonas aeruginosa. J. Clin. Med. 2020, 9, 2631. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.T.; Haworth, C.S.; Aliberti, S.; Barker, A.; Blasi, F.; Boersma, W.; Chalmers, J.D.; De Soyza, A.; Dimakou, K.; Elborn, J.S.; et al. Pulmonary exacerbation in adults with bronchiectasis: A consensus definition for clinical research. Eur. Respir. J. 2017, 49, 1700051. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.T.; Sullivan, A.L.; Chalmers, J.D.; De Soyza, A.; Elborn, J.S.; Floto, R.A.; Grillo, L.; Gruffydd-Jones, K.; Harvey, A.; Haworth, C.S.; et al. British Thoracic Society guideline for bronchiectasis in adults. BMJ Open Respir. Res. 2018, 5, e000348. [Google Scholar] [CrossRef] [Green Version]
- Martínez-García, M.Á.; Máiz, L.; Olveira, C.; Girón, R.M.; de la Rosa, D.; Blanco, M.; Cantón, R.; Vendrell, M.; Polverino, E.; de Gracia, J.; et al. Spanish Guidelines on the Evaluation and Diagnosis of Bronchiectasis in Adults. Arch. Bronconeumol. 2018, 54, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Martínez-García, M.Á.; Máiz, L.; Olveira, C.; Girón, R.M.; de la Rosa, D.; Blanco, M.; Cantón, R.; Vendrell, M.; Polverino, E.; de Gracia, J.; et al. Spanish Guidelines on Treatment of Bronchiectasis in Adults. Arch. Bronconeumol. 2018, 54, 88–98. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Aliberti, S.; Filonenko, A.; Shteinberg, M.; Goeminne, P.C.; Hill, A.T.; Fardon, T.C.; Obradovic, D.; Gerlinger, C.; Sotgiu, G.; et al. Characterization of the “frequent exacerbator phenotype” in bronchiectasis. Am. J. Respir. Crit. Care Med. 2018, 197, 1410–1420. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Chang, A.B.; Chotirmall, S.H.; Dhar, R.; McShane, P.J. Bronchiectasis. Nat. Rev. Dis. Prim. 2018, 4, 45. [Google Scholar] [CrossRef]
- Lee, S.J.; Kim, H.J.; Kim, J.Y.; Ju, S.; Lim, S.; Yoo, J.W.; Nam, S.J.; Lee, G.D.; Cho, H.S.; Kim, R.B.; et al. Serum albumin and disease severity of non-cystic fibrosis bronchiectasis. Respir. Care 2018, 62, 1075–1084. [Google Scholar] [CrossRef] [Green Version]
- Wilson, C.B.; Jones, P.W.; O’Leary, C.J.; Hansell, D.M.; Dowling, R.B.; Cole, P.J.; Wilson, R. Systemic markers of inflammation in stable bronchiectasis. Eur. Respir J. 1998, 12, 820–824. [Google Scholar] [CrossRef] [Green Version]
- King, P.T.; Hutchinson, P.; Holmes, P.W.; Freezer, N.J.; Bennett-Wood, V.; Robins-Browne, R.; Holdsworth, S.R. Assessing immune function in adult bronchiectasis. Clin. Exp. Immunol. 2006, 144, 440–446. [Google Scholar] [CrossRef]
- Stead, A.; Douglas, J.G.; Broadfoot, C.J.; Kaminski, E.R.; Herriot, R. Humoral immunity and bronchiectasis. Clin. Exp. Immunol. 2002, 130, 325–330. [Google Scholar] [CrossRef]
- Kanthakumar, K.; Taylor, G.; Tsang, K.W.; Cundell, D.R.; Rutman, A.; Smith, S.; Jeffery, P.K.; Cole, P.J.; Wilson, R. Mechanisms of action of Pseudomonas aeruginosa pyocyanin on human ciliary beat in vitro. Infect. Immun. 1993, 61, 2848–2853. [Google Scholar] [CrossRef] [Green Version]
- Fuschillo, S.; De Felice, A.; Balzano, G. Mucosal inflammation in idiopathic bronchiectasis: Cellular and molecular mechanisms. Eur. Respir. J. 2008, 31, 396–406. [Google Scholar] [CrossRef] [Green Version]
- Aliberti, S.; Sotgiu, G.; Blasi, F.; Saderi, L.; Posadas, T.; Martinez Garcia, M.A. Blood eosinophils predict inhaled fluticasone response in bronchiectasis. Eur. Respir. J. 2020, 56, 2000453. [Google Scholar] [CrossRef]
- Lipworth, B.; Chan, R.; Kuo, C.R. Blood eosinophils do not predict inhaled budesonide response in bronchiectasis. Eur. Respir. J. 2020, 56, 2002005. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Garcia, M.A.; Posadas, T.; Sotgiu, G.; Blasi, F.; Saderi, L.; Aliberti, S. Repeteability of Circulating Eosinophil Measures and Inhaled Corticosteroids Effect in Bronchiectasis. A Post Hoc Analysis of a Randomized Clinical Trial. Arch. Bronconeumol. 2020, 56, 681–683. [Google Scholar] [CrossRef] [PubMed]
- Rademacher, J.; Konwert, S.; Fuge, J.; Dettmer, S.; Welte, T.; Ringshausen, F.C. Anti-IL5 and anti-IL5Rα therapy for clinically significant bronchiectasis with eosinophilic endotype: A case series. Eur. Respir. J. 2020, 55, 1901333. [Google Scholar] [CrossRef] [PubMed]
- Carpagnano, G.E.; Scioscia, G.; Lacedonia, D.; Curradi, G.; Barbaro, M.P.F. Severe uncontrolled asthma with bronchiectasis: A pilot study of an emerging phenotype that responds to mepolizumab. J. Asthma Allergy 2019, 12, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Garcia, M.A.; Posadas, T.; Sotgiu, G.; Blasi, F.; Saderi, L.; Aliberti, S. Role of inhaled corticosteroids in reducing exacerbations in bronchiectasis patients with blood eosinophilia pooled post-hoc analysis of 2 randomized clinical trials. Respir. Med. 2020, 172, 106127. [Google Scholar] [CrossRef] [PubMed]
- Pavord, I.D.; Lettis, S.; Anzueto, A.; Barnes, N. Blood eosinophil count and pneumonia risk in patients with chronic obstructive pulmonary disease: A patient-level meta-analysis. Lancet Respir. Med. 2016, 4, 731–741. [Google Scholar] [CrossRef]
- Casanova, C.; Celli, B.R.; de-Torres, J.P.; Martínez-Gonzalez, C.; Cosio, B.G.; Pinto-Plata, V.; de Lucas-Ramos, P.; Divo, M.; Fuster, A.; Peces-Barba, G.; et al. Prevalence of persistent blood eosinophilia: Relation to outcomes in patients with COPD. Eur. Respir. J. 2017, 50, 1701162. [Google Scholar] [CrossRef] [PubMed]
- Martinez-García, M.A.; Oscullo, G.; Posadas, T.; Zaldivar, E.; Villa, C.; Dobarganes, Y.; Girón, R.; Olveira, C.; Maíz, L.; García-Clemente, M.; et al. Pseudomonas aeruginosa and lung function decline in patients with bronchiectasis. Clin. Microbiol. Infect. 2021, 27, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.-H.; Fang, Y.-F.; Chung, F.-T.; Lee, C.-S.; Chang, Y.-C.; Liu, Y.-Z.; Wu, C.-H. Distance-saturation product of the 6-min walk test predicts mortality of patients with non-cystic fibrosis bronchiectasis. J. Thorac. Dis. 2017, 9, 3168–3176. [Google Scholar] [CrossRef] [Green Version]
- Perea, L.; Cantó, E.; Suarez-Cuartin, G.; Aliberti, S.; Chalmers, J.D.; Sibila, O.; Vidal, S. A Cluster Analysis of Bronchiectasis Patients Based on the Airway Immune Profile. Chest 2021, 159, 1758–1767. [Google Scholar] [CrossRef]
- Menéndez, R.; Méndez, R.; Polverino, E.; Rosales-Mayor, E.; Amara-Elori, I.; Reyes, S.; Posadas, T.; Fernández-Barat, L.; Torres, A. Factors associated with hospitalization in bronchiectasis exacerbations: A one-year follow-up study. Respir. Res. 2017, 18, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, M.; Zhu, M.; Wang, C.; Wu, Z.; Xiong, X.; Wu, H.; Cheng, D.; Ji, Y. Prognostic performance of the FACED score and bronchiectasis severity index in bronchiectasis: A systematic review and meta-analysis. Biosci. Rep. 2020, 40, BSR20194514. [Google Scholar] [CrossRef]
- Martinez-García, M.A.; Villa, C.; Dobarganes, Y.; Girón, R.; Maíz, L.; García-Clemente, M.; Sibila, O.; Golpe, R.; Rodríguez, J.; Barreiro, E.; et al. RIBRON: The spanish Online Bronchiectasis Registry. Characterization of the First 1912 Patients. Arch. Bronconeumol. 2021, 57, 28–35. [Google Scholar] [CrossRef]
- Posadas, T.; Oscullo, G.; Zaldivar, E.; Villa, C.; Dobarganes, Y.; Girón, R.; Olveira, C.; Maíz, L.; García-Clemente, M.; Sibila, O.; et al. C-Reactive Protein Concentration in Steady-State Bronchiectasis: Prognostic Value of Future Severe Exacerbations. Data From the Spanish Registry of Bronchiectasis (RIBRON). Arch. Bronconeumol. 2021, 57, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Polverino, E.; Goeminne, P.C.; McDonnell, M.J.; Aliberti, S.; Marshall, S.E.; Loebinger, M.R.; Murris, M.; Cantón, R.; Torres, A.; Dimakou, K.; et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur. Respir. J. 2017, 50, 1700629. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, S.; Masefield, S.; Polverino, E.; De Soyza, A.; Loebinger, M.R.; Menendez, R.; Ringshausen, F.C.; Vendrell, M.; Powell, P.; Chalmers, J.D. Research priorities in bronchiectasis: A consensus statement from the EMBARC Clinical Research Collaboration. Eur. Respir. J. 2016, 48, 632–647. [Google Scholar] [CrossRef] [Green Version]
- Shrestha, B.; Dunn, L. The Declaration of Helsinki on Medical Research involving Human Subjects: A Review of Seventh Revision. J. Nepal Health Res. Counc. 2020, 17, 548–552. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Garcia, M.A.; de Gracia, J.; Vendrell Relat, M.; Giron, R.-M.; Maiz Carro, L.; de la Rosa Carrillo, D.; Olveira, C. Multidimensional approach to non-cystic fibrosis bronchiectasis: The FACED score. Eur. Respir. J. 2014, 43, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Garcia, M.A.; Athanazio, R.A.; Girón, R.M.; Máiz-Carro, L.; de la Rosa, D.; Olveira, C.; de Gracia, J.; Vendrell, M.; Prados-Sánchez, C.; Gramblicka, G.; et al. Predicting high risk of exacerbations in bronchiectasis: The E-FACED score. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 275–284. [Google Scholar] [CrossRef] [Green Version]
- Chalmers, J.D.; Goeminne, P.; Aliberti, S.; McDonnell, M.J.; Lonni, S.; Davidson, J.; Poppelwell, L.; Salih, W.; Pesci, A.; Dupont, L.J.; et al. The bronchiectasis severity index an international derivation and validation study. Am. J. Respir. Crit. Care Med. 2014, 189, 576–585. [Google Scholar] [CrossRef]
- Lehrer, R.I.; Szklarek, D.; Barton, A.; Ganz, T.; Hamann, K.J.; Gleich, G.J. Antibacterial properties of eosinophil major basic protein and eosinophil cationic protein. J. Immunol. 1989, 142, 4428–4434. [Google Scholar]
- Martinez-Garcia, M.A.; Faner, R.; Oscullo, G.; de la Rosa, D.; Soler-Cataluña, J.J.; Ballester, M.; Agusti, A. Inhaled Steroids, Circulating Eosinophils, Chronic Airway Infection, and Pneumonia Risk in Chronic Obstructive Pulmonary Disease. A Network Analysis. Am. J. Respir. Crit. Care Med. 2020, 201, 1078–1085. [Google Scholar] [CrossRef]
- Nerpin, E.; Jacinto, T.; Fonseca, J.A.; Alving, K.; Janson, C.; Malinovschi, A. Systemic inflammatory markers in relation to lung function in NHANES. 2007–2010. Respir. Med. 2018, 142, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Bedi, P.; Davidson, D.J.; McHugh, B.J.; Rossi, A.G.; Hill, A.T. Blood Neutrophils Are Reprogrammed in Bronchiectasis. Am. J. Respir. Crit. Care Med. 2018, 198, 880–890. [Google Scholar] [CrossRef]
- Wilm, J.; Costa, J.H.C.; Neave, H.W.; Weary, D.M.; von Keyserlingk, M.A.G. Technical note: Serum total protein and immunoglobulin G concentrations in neonatal dairy calves over the first 10 days of age. J. Dairy Sci. 2018, 101, 6430–6436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaya, M.; Usami, O.; Nakayama, S.; Tode, N.; Yamada, A.; Ito, S.; Omata, F.; Momma, H.; Funakubo, M.; Ichinose, M. Malnutrition, airflow limitation and severe emphysema are risks for exacerbation of chronic obstructive pulmonary disease in Japanese subjects: A retrospective single-center study. Int. J. COPD 2020, 15, 857–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK Biobank: An Open Access Resource for Identifying the Causes of a Wide Range of Complex Diseases of Middle and Old Age. PLOS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; McQueenie, R.; Lee, D.; Gallacher, K.I.; Mair, F.S. Examining patterns of multimorbidity, polypharmacy and risk of adverse drug reactions in chronic obstructive pulmonary disease: A cross-sectional UK Biobank study. BMJ Open 2018, 8, e018404. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (A) | ||
| Below-Threshold Cluster | Above-Threshold Cluster | |
| (N = 270) | (N = 636) | |
| Anthropometric variables, (SD) | ||
| Age, years | 68.8 (13.8) | 67 (15.1) |
| Body weight, kg | 65.3 (15.1) | 68.7 (14.4) ** |
| BMI, kg/m2 | 25.2 (5.2) | 26.4 (5) ** |
| Disease severity, (SD) | ||
| FACED score | 2.21 (1.82) | 2.07 (1.64) |
| EFACED score | 3.11 (2.40) | 2.65 (2.09) ** |
| BSI | 8.60 (4.96) | 7.29 (4.51) *** |
| Exacerbations | 1.82 (1.97) | 1.39 (1.45) ** |
| Hospitalizations | 0.84 (1.30) | 0.56 (1.38) ** |
| Charlson Index | 2.0 (1.71) | 1.83 (1.53), p = 0.1 |
| Chronic colonization by PA, N (%) | 62 (23) | 166 (26) |
| Smoking history | ||
| Never smokers, N (%) | 152 (56) | 375 (59) |
| Current smokers, N (%) | 28 (11) | 58 (9) |
| Ex-smokers, N (%) | 90 (33) | 203 (32) |
| Packs-year, (SD) | 14.5 (23.9) | 11.9 (21.1) |
| Lung function, (SD) | ||
| FEV1, % predicted | 71 (27) | 75 (24) * |
| FVC, % predicted | 83 (24) | 86 (21), p = 0.065 |
| FEV1/FVC, % | 67 (13) | 69 (13) ** |
| DLCO, % predicted | 76 (23) | 85 (24) ** |
| KCO, % predicted | 77 (34) | 77 (39) |
| RV, % predicted | 137 (40) | 138 (53) |
| TLC, % predicted | 99 (20) | 103 (20) |
| RV/TLC, % | 52 (10) | 49 (12), p = 0.061 |
| (B) | ||
| Below-Threshold Cluster | Above-Threshold Cluster | |
| (N = 236) | (N = 567) | |
| Anthropometric variables,(SD) | ||
| Age, years | 67.8 (14.0) | 66.0 (15.3) |
| Body weight, kg | 64.4 (14.6) | 68.1 (14.2) ** |
| BMI, kg/m2 | 25.0 (5.2) | 26.3 (5.0) ** |
| Disease severity,(SD) | ||
| FACED score | 2.03 (1.76) | 1.92 (1.52) |
| EFACED score | 2.85 (2.31) | 2.45 (1.93) * |
| BSI | 8.08 (4.79) | 6.86 (4.22) ** |
| Exacerbations | 1.75 (1.98) | 1.35 (1.44) ** |
| Hospitalizations | 0.76 (1.3) | 0.51 (1.36) * |
| Charlson Index | 1.92 (1.69) | 1.75 (1.47) |
| Chronic colonization by PA, N (%) | 30 (25) | 171 (25) |
| Smoking history | ||
| Never smokers, N (%) | 151 (64) | 368 (65) |
| Current smokers, N (%) | 20 (8) | 45 (8) |
| Ex-smokers, N (%) | 65 (28) | 154 (27) |
| Packs-year, (SD) | 10.1 (19.4) | 7.8 (15.6) |
| Lung function,(SD) | ||
| FEV1, % predicted | 74 (27) | 78 (23), p = 0.07 |
| FVC, % predicted | 85 (24) | 87 (21) |
| FEV1/FVC, % | 68 (13) | 71 (11) ** |
| DLCO, % predicted | 79 (22) | 87 (23) * |
| KCO, % predicted | 78 (33) | 78 (39) |
| RV, % predicted | 134 (38) | 134 (49) |
| TLC, % predicted | 98 (20) | 101 (18) |
| RV/TLC, % | 52 (10) | 49 (12), p = 0.084 |
| (A) | ||
| Below-Threshold Cluster | Above-Threshold Cluster | |
| (N = 270) | (N = 636) | |
| Blood parameters,(SD) | ||
| Total leukocytes, cells/µL | 7.68 (3.29) × 103 | 7.5 (2.53) × 103 |
| Total neutrophils, cells/µL | 5.28 (3.09) × 103 | 4.49 (2.21) × 103 *** |
| Neutrophils, % | 65.41 (13.1) | 58.11 (10.36) *** |
| Total lymphocytes, cells/µL | 1.72 (0.8) × 103 | 2.12 (0.74) × 103 *** |
| Lymphocytes, % | 25.29 (12.11) | 29.7 (9.61) *** |
| Total eosinophils, cells/µL | 0.06 (0.05) × 103 | 0.26 (0.17) × 103 *** |
| Eosinophils, % | 0.79 (0.65) | 3.6 (2.23) *** |
| Platelets, cells/µL | 246 (81) × 103 | 256 (73) × 103 |
| IgE, U/mL | 94.41 (422.47) | 152.42 (404.19) |
| IgE aspergillus, KU/L | 6.37 (17.65) | 3.77 (12.33) |
| IgM, mg/dL | 86.1 (103.56) | 100.6 (101.17) |
| IgA, mg/dL | 191.08 (153.45) | 216.63 (147.07) |
| IgG, mg/dL | 777.44 (545.66) | 945.15 (516.38) ** |
| Alpha-1 antitrypsin, mg/dL | 132.48 (34.76) | 133.77 (34.3) |
| CRP, mg/dL | 2.81 (5.69) | 2.8 (5.64) |
| ESR, mm/h | 17.4 (16.42) | 16.94 (15.4) |
| Fibrinogen, mg/dL | 435 (139) | 419 (134) |
| Hemoglobin, g/dL | 13.36 (1.66) | 13.77 (1.45) *** |
| Hematocrit, % | 40.54 (4.78) | 41.94 (4.09) *** |
| Creatinine, mg/dL | 0.83 (0.53) | 0.83 (0.42) |
| Total proteins, g/dL | 6.9 (0.69) | 7.04 (0.58) * |
| Albumin, g/dL | 4.11 (0.46) | 4.24 (0.41) ** |
| (B) | ||
| Below-Threshold Cluster | Above-Threshold Cluster | |
| (N = 236) | (N = 567) | |
| Blood Parameters,(SD) | ||
| Total leukocytes, cells/µL | 7.44 (3.19) × 103 | 7.39 (2.4) × 103 |
| Total neutrophils, cells/µL | 5.04 (2.98) × 103 | 4.4 (2.09) × 103 ** |
| Neutrophils, % | 64.45 (12.94) | 57.85 (10.31) *** |
| Total lymphocytes, cells/µL | 1.73 (0.78) × 103 | 2.12 (0.74) × 103*** |
| Lymphocytes, % | 26.13 (11.99) | 30.01 (9.55) *** |
| Total eosinophils, cells/µL | 0.05 (0.03) × 103 | 0.26 (0.18) × 103 *** |
| Eosinophils, % | 0.84 (0.65) | 3.63 (2.26) *** |
| Platelets, cells/µL | 247.68 (82.7) × 103 | 257.31 (72.26) × 103 |
| IgE, U/mL | 86.8 (442.43) | 146.66 (400.49) |
| IgE aspergillus, KU/L | 6.45 (17.99) | 3.89 (12.64) |
| IgM, mg/dL | 87.25 (108) | 95.48 (81.91) |
| IgA, mg/dL | 185.04 (147.07) | 211.7 (146.35) |
| IgG, mg/dL | 789.22 (546.8) | 936.31 (511.64) ** |
| Alpha-1 antitrypsin, mg/dL | 132.84 (36.23) | 132.75 (34.28) |
| CRP, mg/dL | 2.8 (5.85) | 2.65 (5.31) |
| ESR, mm/h | 17.66 (17.12) | 17.07 (15.18) |
| Fibrinogen, mg/dL | 430 (140) | 415 (133) |
| Hemoglobin, g/dL | 13.3 (1.63) | 13.69 (1.39) ** |
| Hematocrit, % | 40.37 (4.67) | 41.72 (3.84) *** |
| Creatinine, mg/dL | 0.83 (0.56) | 0.82 (0.43) |
| Total proteins, g/dL | 6.95 (0.67) | 7.07 (0.55) * |
| Albumin, g/dL | 4.16 (0.44) | 4.26 (0.4) * |
| Etiology, N, % | Total | Below-Threshold Cluster | Above-Threshold Cluster |
|---|---|---|---|
| Post-infectious | 343, 37.9% | 113, 42% | 230, 36.2% |
| Tuberculosis | 122, 13.5% | 42, 15.6% | 80, 12.6% |
| Childhood infections | 83, 9.2% | 26, 9.6% | 57, 9% |
| Necrotizing pneumonia | 29, 3.2% | 6, 2.2% | 23, 3.6% |
| Non-tuberculous mycobacteria | 10, 1.1% | 3, 1.1% | 7, 1.1% |
| Fungal infections | 4, 0.4% | 2, 0.7% | 2, 0.3% |
| Others | 658, 72.6% | 191, 70.7% | 467, 73.4% |
| COPD | 103, 11.4% | 34, 12.6% | 69, 10.8% |
| Asthma | 90, 9.9% | 24, 8.9% | 66, 10.4% |
| Hyperimmune response | 3, 0.3% | 1, 0.4% | 2, 0.3% |
| Vasculitis | 2, 0.2% | 0 | 2, 0.3% |
| Systemic disorders | 78, 8.6% | 17, 6.3% | 61, 9.6% |
| Immunodeficiencies | 42, 4.6% | 13, 4.8% | 29, 4.6% |
| Inflammatory pneumonitis | 21, 2.3% | 7, 2.6% | 14, 2.2% |
| Congenital malformations | 9, 1% | 1, 0.4% | 8, 1.3% |
| Inflammatory bowel diseases | 9, 1% | 2, 0.7% | 7, 1.1% |
| Obliterative bronchiolitis | 6, 0.7% | 3, 1.1% | 3, 0.5% |
| Unknown etiology | 166, 18.3% | 45, 16.7% | 121, 19.0% |
| Other etiologies | 34, 3.8% | 10, 3.7% | 24, 3.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Villa, C.; Dobarganes, Y.; Olveira, C.; Girón, R.; García-Clemente, M.; Máiz, L.; Sibila, O.; Golpe, R.; Menéndez, R.; et al. Phenotypic Clustering in Non-Cystic Fibrosis Bronchiectasis Patients: The Role of Eosinophils in Disease Severity. Int. J. Environ. Res. Public Health 2021, 18, 8431. https://doi.org/10.3390/ijerph18168431
Wang X, Villa C, Dobarganes Y, Olveira C, Girón R, García-Clemente M, Máiz L, Sibila O, Golpe R, Menéndez R, et al. Phenotypic Clustering in Non-Cystic Fibrosis Bronchiectasis Patients: The Role of Eosinophils in Disease Severity. International Journal of Environmental Research and Public Health. 2021; 18(16):8431. https://doi.org/10.3390/ijerph18168431
Chicago/Turabian StyleWang, Xuejie, Carmen Villa, Yadira Dobarganes, Casilda Olveira, Rosa Girón, Marta García-Clemente, Luis Máiz, Oriol Sibila, Rafael Golpe, Rosario Menéndez, and et al. 2021. "Phenotypic Clustering in Non-Cystic Fibrosis Bronchiectasis Patients: The Role of Eosinophils in Disease Severity" International Journal of Environmental Research and Public Health 18, no. 16: 8431. https://doi.org/10.3390/ijerph18168431
APA StyleWang, X., Villa, C., Dobarganes, Y., Olveira, C., Girón, R., García-Clemente, M., Máiz, L., Sibila, O., Golpe, R., Menéndez, R., Rodríguez-López, J., Prados, C., Martinez-García, M. A., Rodriguez, J. L., de la Rosa, D., Duran, X., Garcia-Ojalvo, J., & Barreiro, E. (2021). Phenotypic Clustering in Non-Cystic Fibrosis Bronchiectasis Patients: The Role of Eosinophils in Disease Severity. International Journal of Environmental Research and Public Health, 18(16), 8431. https://doi.org/10.3390/ijerph18168431