
Comparison of Patient Satisfaction in Inpatient Care Provided by Hospitalists and Nonhospitalists in South Korea




Abstract
1. Introduction
2. Methods
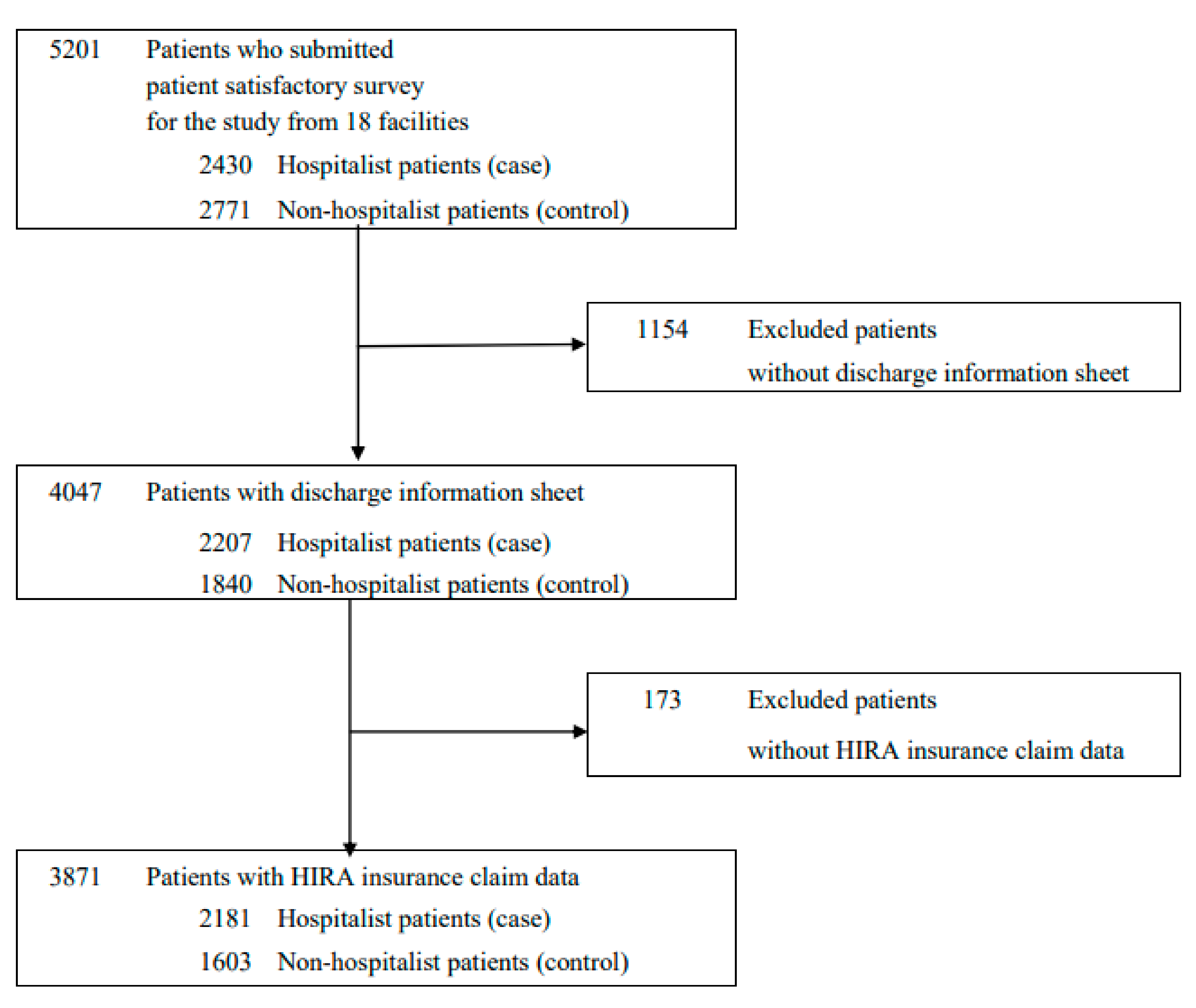
2.1. Data, Study Design, and Study Population
2.2. Patient Satisfaction Survey and Discharge Summary Sheet
2.3. Measure of Patient Satisfaction
2.4. Confounding Variables
2.5. Statistical Analysis
2.6. Ethical Statement
3. Results
3.1. General Characteristics and Health Condition of the Study Population
3.2. Patient Satisfaction in Hospitalist Care Compared to Non-Hospitalist Care
3.3. Patient Satisfaction in Hospitalist Ward Stratified by the Medical Division
3.4. Patient Satisfaction in Hospitalist Ward Stratified by Region
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cleary, P.D.; McNeil, B.J. Patient satisfaction as an indicator of quality care. Inquiry 1988, 25, 25–36. [Google Scholar]
- Renzi, C.; Abeni, D.; Picardi, A.; Agostini, E.; Melchi, C.; Pasquini, P.; Puddu, P.; Braga, M. Factors associated with patient satisfaction with care among dermatological outpatients. Br. J. Dermatol. 2001, 145, 617–623. [Google Scholar] [CrossRef]
- Kane, R.L.; Maciejewski, M.; Finch, M. The relationship of patient satisfaction with care and clinical outcomes. Med. Care 1997, 35, 714–730. [Google Scholar] [CrossRef]
- Bain, J.; Kelly, H.; Snadden, D.; Staines, H. Day surgery in scotland: Patient satisfaction and outcomes. Qual. Health Care 1999, 8, 86–91. [Google Scholar] [CrossRef]
- Figueroa, J.F.; Feyman, Y.; Zhou, X.; Joynt Maddox, K. Hospital-level care coordination strategies associated with better patient experience. BMJ Qual. Saf. 2018, 27, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, D.; Manning, W.G.; Morrison, J.; Shah, M.N.; Jin, L.; Guth, T.; Levinson, W. Effects of physician experience on costs and outcomes on an academic general medicine service: Results of a trial of hospitalists. Ann. Intern. Med. 2002, 137, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.M.; Koch, K.E.; Harvey, J.K.; Wilson, R.; Englert, J.; Gerard, P.D. Effects of hospitalists on cost, outcomes, and patient satisfaction in a rural health system. Am. J. Med. 2000, 108, 621–626. [Google Scholar] [CrossRef]
- Turner, J.; Hansen, L.; Hinami, K.; Christensen, N.; Peng, J.; Lee, J.; Williams, M.V.; O’Leary, K.J. The impact of hospitalist discontinuity on hospital cost, readmissions, and patient satisfaction. J. Gen. Intern. Med. 2014, 29, 1004–1008. [Google Scholar] [CrossRef]
- McKinley, R.K.; Roberts, C. Patient satisfaction with out of hours primary medical care. Qual. Health Care 2001, 10, 23–28. [Google Scholar] [CrossRef]
- Rozenblum, R.; Lisby, M.; Hockey, P.M.; Levtizion-Korach, O.; Salzberg, C.A.; Lipsitz, S.; Bates, D.W. Uncovering the blind spot of patient satisfaction: An international survey. BMJ Qual. Saf. 2011, 20, 959–965. [Google Scholar] [CrossRef]
- Halasyamani, L.K.; Valenstein, P.N.; Friedlander, M.P.; Cowen, M.E. A comparison of two hospitalist models with traditional care in a community teaching hospital. Am. J. Med. 2005, 118, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Seiler, A.; Visintainer, P.; Brzostek, R.; Ehresman, M.; Benjamin, E.; Whitcomb, W.; Rothberg, M.B. Patient satisfaction with hospital care provided by hospitalists and primary care physicians. J. Hosp. Med. 2012, 7, 131–136. [Google Scholar] [CrossRef]
- Kripalani, S.; LeFevre, F.; Phillips, C.O.; Williams, M.V.; Basaviah, P.; Baker, D.W. Deficits in communication and information transfer between hospital-based and primary care physiciansimplications for patient safety and continuity of care. JAMA 2007, 297, 831–841. [Google Scholar] [CrossRef]
- Chen, L.M.; Birkmeyer, J.D.; Saint, S.; Jha, A.K. Hospitalist staffing and patient satisfaction in the national medicare population. J. Hosp. Med. 2013, 8, 126–131. [Google Scholar] [CrossRef]
- Lindenauer, P.K.; Rothberg, M.B.; Pekow, P.S.; Kenwood, C.; Benjamin, E.M.; Auerbach, A.D. Outcomes of care by hospitalists, general internists, and family physicians. N. Engl. J. Med. 2007, 357, 2589–2600. [Google Scholar] [CrossRef] [PubMed]
- Fiscella, K.; Meldrum, S.; Franks, P.; Shields, C.G.; Duberstein, P.; McDaniel, S.H.; Epstein, R.M. Patient trust: Is it related to patient-centered behavior of primary care physicians? Med. Care 2004, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Mainous, A.G.; Baker, R.; Love, M.M.; Gray, D.P.; Gill, J.M. Continuity of care and trust in one’s physician: Evidence from primary care in the united states and the united kingdom. Fam. Med. 2001, 33, 22–27. [Google Scholar]
- Wachter, R.M.; Goldman, L. The emerging role of “hospitalists” in the american health care system. N. Engl. J. Med. 1996, 335, 514–517. [Google Scholar] [CrossRef] [PubMed]
- White, H.L.; Glazier, R.H. Do hospitalist physicians improve the quality of inpatient care delivery? A systematic review of process, efficiency and outcome measures. BMC Med. 2011, 9, 58. [Google Scholar] [CrossRef]
- Southern, W.N.; Berger, M.A.; Bellin, E.Y.; Hailpern, S.M.; Arnsten, J.H. Hospitalist care and length of stay in patients requiring complex discharge planning and close clinical monitoring. Arch. Intern. Med. 2007, 167, 1869–1874. [Google Scholar] [CrossRef]
- Hock Lee, K.; Yang, Y.; Soong Yang, K.; Chi Ong, B.; Seong Ng, H. Bringing generalists into the hospital: Outcomes of a family medicine hospitalist model in singapore. J. Hosp. Med. 2011, 6, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Kisuule, F.; Howell, E.E. Hospitalists and their impact on quality, patient safety, and satisfaction. Obstet. Gynecol. Clin. N. Am. 2015, 42, 433–446. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Patient Experience in Adult nhs Services: Improving the Experience of Care for People Using Adult Nhs Services. Available online: https://www.nice.org.uk/guidance/qs152021 (accessed on 30 June 2021).
- Wong, E.; Mavondo, F.; Fisher, J. Patient feedback to improve quality of patient-centred care in public hospitals: A systematic review of the evidence. BMC Health Serv. Res. 2020, 20, 530. [Google Scholar] [CrossRef]
- Kleefstra, S.M.; Zandbelt, L.C.; Borghans, I.; de Haes, H.J.; Kool, R.B. Investigating the potential contribution of patient rating sites to hospital supervision: Exploratory results from an interview study in the netherlands. J. Med. Internet Res. 2016, 18, e201. [Google Scholar] [CrossRef]
- Aboumatar, H.J.; Chang, B.H.; Al Danaf, J.; Shaear, M.; Namuyinga, R.; Elumalai, S.; Marsteller, J.A.; Pronovost, P.J. Promising practices for achieving patient-centered hospital care: A national study of high-performing us hospitals. Med. Care 2015, 53, 758–767. [Google Scholar] [CrossRef] [PubMed]
- Richard, M.L.; Parmar, M.P.; Calestagne, P.P.; McVey, L. Seeking patient feedback: An important dimension of quality in cancer care. J. Nurs. Care Qual. 2010, 25, 344–351. [Google Scholar] [CrossRef]
- Buurman, B.M.; Verhaegh, K.J.; Smeulers, M.; Vermeulen, H.; Geerlings, S.E.; Smorenburg, S.; de Rooij, S.E. Improving handoff communication from hospital to home: The development, implementation and evaluation of a personalized patient discharge letter. Int. J. Qual. Health Care J. Int. Soc. Qual. Health Care 2016, 28, 384–390. [Google Scholar] [CrossRef]
- Harnett, M.J.; Correll, D.J.; Hurwitz, S.; Bader, A.M.; Hepner, D.L. Improving efficiency and patient satisfaction in a tertiary teaching hospital preoperative clinic. Anesthesiology 2010, 112, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Madden, P.B.; Davies, E.A. Reporting cancer patients’ experiences of care for quality improvement: Analysis of 2000 and 2004 survey results for south east england. J. Eval. Clin. Pract. 2010, 16, 776–783. [Google Scholar] [CrossRef]
- Piper, D.; Iedema, R.; Gray, J.; Verma, R.; Holmes, L.; Manning, N. Utilizing experience-based co-design to improve the experience of patients accessing emergency departments in new south wales public hospitals: An evaluation study. Health Serv. Manag. Res. 2012, 25, 162–172. [Google Scholar] [CrossRef]
- Jang, S.-I.; Jang, S.-y.; Park, E.-C. Trends of us hospitalist and suggestions for introduction of korean hospitalist. Korean J. Med. 2015, 89, 1–5. [Google Scholar] [CrossRef]
- Chae, W.; Park, E.C.; Lee, K.Y.; Kang, H.J.; Lee, W.Y.; Kim, Y.M.; Jang, S.I. Development and evolution of hospital medicine in korea. J. Hosp Med. 2021, 16, 247–250. [Google Scholar]
- Jang, S.-I.; Park, E.-C.; Nam, J.M.; Chae, W.; Lee, N.-K.; Kim, J.Y.; Lee, J.E.; Cho, Y.D. A Study on the Implementation and the Evaluation of Korean Hospitalist System to Improve the Quality of Hospitalization (Phase 2); Institute of Health Services Research, Yonsei University: Seoul, Korea, 2018. [Google Scholar]
- Park, E.-C.; Lee, S.G.; Kim, T.-H.; Jang, S.-I.; Kim, J.Y.; Lee, N.-K.; Lee, S.A.; Lee, J.E.; Jang, J.E.; Choi, J.W. A Study on the Implementation and the Evaluation of Korean Hospitalist System to Improve the Quality of Hospitalization (Phase 1); Institute of Health Services Research, Yonsei University: Seoul, Korea, 2016. [Google Scholar]
- Wachter, R.M.; Goldman, L. Zero to 50,000—The 20th anniversary of the hospitalist. N. Engl. J. Med. 2016, 375, 1009–1011. [Google Scholar] [CrossRef]
- Rifkin, W.D.; Burger, A.; Holmboe, E.S.; Sturdevant, B. Comparison of hospitalists and nonhospitalists regarding core measures of pneumonia care. Am. J. Manag. Care 2007, 13, 129. [Google Scholar]
- Richards, S.; Thompson, R.; Paulmeyer, S.; Garg, A.; Malik, S.; Carlson, K.; Lyden, E.; Shiffermiller, J. Can specific feedback improve patients’ satisfaction with hospitalist physicians? A feasibility study using a validated tool to assess inpatient satisfaction. Patient Exp. J. 2018, 5, 34–40. [Google Scholar] [CrossRef]
- Beresford, L. Hospital medicine flourishing around the world. Hospitalist 2015. Available online: https://cdn.mdedge.com/files/s3fs-public/hosp_apr2021_lorez_digital.pdf. (accessed on 30 June 2021).
- Shu, C.C.; Lin, J.W.; Lin, Y.F.; Hsu, N.C.; Ko, W.J. Evaluating the performance of a hospitalist system in taiwan: A pioneer study for nationwide health insurance in asia. J. Hosp. Med. 2011, 6, 378–382. [Google Scholar] [CrossRef]
- Torok, H.; Ghazarian, S.R.; Kotwal, S.; Landis, R.; Wright, S.; Howell, E. Development and validation of the tool to assess inpatient satisfaction with care from hospitalists. J. Hosp. Med. 2014, 9, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Chesluk, B.J.; Bernabeo, E.; Hess, B.; Lynn, L.A.; Reddy, S.; Holmboe, E.S. A new tool to give hospitalists feedback to improve interprofessional teamwork and advance patient care. Health Aff. 2012, 31, 2485–2492. [Google Scholar] [CrossRef] [PubMed]
- Skelly, A.C.; Dettori, J.R.; Brodt, E.D. Assessing bias: The importance of considering confounding. Evid. Based Spine Care J. 2012, 3, 9–12. [Google Scholar] [CrossRef]
- Marcoulides, K.M.; Raykov, T. Evaluation of variance inflation factors in regression models using latent variable modeling methods. Educ. Psychol. Meas. 2019, 79, 874–882. [Google Scholar] [CrossRef]
- Lappé, K.L.; Raaum, S.E.; Ciarkowski, C.E.; Reddy, S.P.; Johnson, S.A. Impact of hospitalist team structure on patient-reported satisfaction with physician performance. J. Gen. Intern. Med. 2020, 35, 2668–2674. [Google Scholar] [CrossRef] [PubMed]
- Lindenauer, P.K.; Chehabeddine, R.; Pekow, P.; Fitzgerald, J.; Benjamin, E.M. Quality of care for patients hospitalized with heart failure: Assessing the impact of hospitalists. Arch. Intern. Med. 2002, 162, 1251–1256. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.C.; Westfall, J.M.; Nicholas, R.A. Primary care family physicians and 2 hospitalist models: Comparison of outcomes, processes, and costs. J. Fam. Pract. 2002, 51, 1021–1027. [Google Scholar] [PubMed]
- Rachoin, J.S.; Skaf, J.; Cerceo, E.; Fitzpatrick, E.; Milcarek, B.; Kupersmith, E.; Scheurer, D.B. The impact of hospitalists on length of stay and costs: Systematic review and meta-analysis. Am. J. Manag. Care 2012, 18, e23–e30. [Google Scholar] [PubMed]
- Auerbach, A.D.; Wachter, R.M.; Cheng, H.Q.; Maselli, J.; McDermott, M.; Vittinghoff, E.; Berger, M.S. Comanagement of surgical patients between neurosurgeons and hospitalists. Arch. Intern. Med. 2010, 170, 2004–2010. [Google Scholar] [CrossRef] [PubMed]
- Tsianakas, V.; Robert, G.; Maben, J.; Richardson, A.; Dale, C.; Griffin, M.; Wiseman, T. Implementing patient-centred cancer care: Using experience-based co-design to improve patient experience in breast and lung cancer services. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2012, 20, 2639–2647. [Google Scholar]
- Davies, E.A.; Meterko, M.M.; Charns, M.P.; Seibert, M.E.; Cleary, P.D. Factors affecting the use of patient survey data for quality improvement in the veterans health administration. BMC Health Serv. Res. 2011, 11, 334. [Google Scholar] [CrossRef] [PubMed]
- Blackwell, R.W.; Lowton, K.; Robert, G.; Grudzen, C.; Grocott, P. Using experience-based co-design with older patients, their families and staff to improve palliative care experiences in the emergency department: A reflective critique on the process and outcomes. Int. J. Nurs. Stud. 2017, 68, 83–94. [Google Scholar] [CrossRef]
- Chae, W.; Choi, D.-W.; Park, E.-C.; Jang, S.-I. Improved inpatient care through greater patient–doctor contact under the hospitalist management approach: A real-time assessment. Int. J. Environ. Res. Public Health 2021, 18, 5718. [Google Scholar] [CrossRef]
- Jang, S.-I. Korean hospitalist system implementation and development strategies based on pilot studies. J. Korean Med. Assoc. 2019, 62, 558–563. [Google Scholar] [CrossRef]
- Kim, S.-S. Working conditions of interns/residents and patient safety: Painful training might not be authentic. J. Korean Med. Assoc. 2016, 59, 82–84. [Google Scholar] [CrossRef]
- Wang, X.; Cheng, Z. Cross-sectional studies: Strengths, weaknesses, and recommendations. Chest 2020, 158, S65–S71. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | Hospitalist Patients | Non-Hospitalist Patients | χ2 † | |||||
|---|---|---|---|---|---|---|---|---|
| 3784 | % | 2181 | % | 1603 | % | <0.0001 | ||
| Sex | 0.8302 | |||||||
| Male | 1843 | 48.7 | 1059 | 57.5 | 784 | 42.5 | ||
| Female | 1941 | 51.3 | 1122 | 57.8 | 819 | 42.2 | ||
| Age | 0.1363 | |||||||
| ≥19 | 37 | 1 | 21 | 56.8 | 16 | 43.2 | ||
| 20–29 | 128 | 3.4 | 62 | 48.4 | 66 | 51.6 | ||
| 30–39 | 262 | 6.9 | 151 | 57.6 | 111 | 42.4 | ||
| 40–49 | 528 | 14 | 286 | 54.2 | 242 | 45.8 | ||
| 50–59 | 861 | 22.8 | 487 | 56.6 | 374 | 43.4 | ||
| 60–69 | 868 | 22.9 | 495 | 57 | 373 | 43 | ||
| 70–79 | 791 | 20.9 | 484 | 61.2 | 307 | 38.8 | ||
| ≥80 | 309 | 8.2 | 195 | 63.1 | 114 | 36.9 | ||
| Admitted department | <0.0001 | |||||||
| Internal Medicine | 2706 | 71.5 | 1644 | 60.8 | 1062 | 39.2 | ||
| Surgery | 1078 | 28.5 | 537 | 49.8 | 541 | 50.2 | ||
| Admission type | 0.0057 | |||||||
| General admission | 3330 | 88 | 1892 | 56.8 | 1438 | 43.2 | ||
| ER admission ‡ | 454 | 12 | 289 | 63.7 | 165 | 36.3 | ||
| Admission experience | 0.1886 | |||||||
| Yes | 3019 | 79.8 | 1714 | 56.8 | 1305 | 43.2 | ||
| No | 719 | 19 | 430 | 59.8 | 289 | 40.2 | ||
| Region | <0.0001 | |||||||
| Capital | 2667 | 70.5 | 1379 | 51.7 | 1288 | 48.3 | ||
| Rural | 1117 | 29.5 | 802 | 71.8 | 315 | 28.2 | ||
| Length of Stay (Mean, SD †) | 6.16 (5.79) | 6.50 (6.12) | 5.69 (5.34) | 0.0116 | ||||
| Surgery | 3722 | 2138 | 1584 | 0.0152 | ||||
| Yes | 952 | 25.6 | 515 | 54.1 | 437 | 45.9 | ||
| No | 2770 | 74.4 | 1623 | 58.6 | 1147 | 41.4 | ||
| General anesthesia | 3717 | 2136 | 1581 | 0.0763 | ||||
| Yes | 903 | 24.3 | 496 | 54.9 | 407 | 45.1 | ||
| No | 2814 | 75.7 | 1640 | 58.3 | 1174 | 41.7 | ||
| ICU transfer | 3714 | 2134 | 1580 | <0.0001 | ||||
| Yes | 251 | 6.8 | 145 | 57.8 | 106 | 42.2 | ||
| No | 3463 | 93.2 | 1989 | 57.4 | 1474 | 42.6 | ||
| Death | 3713 | 2134 | 1579 | 0.6154 | ||||
| Yes | 19 | 0.5 | 12 | 63.2 | 7 | 36.8 | ||
| No | 3694 | 99.5 | 2122 | 57.4 | 1572 | 42.6 | ||
| Hypertension | 3752 | 2158 | 1594 | 0.0001 | ||||
| Yes | 1328 | 35.4 | 819 | 61.7 | 509 | 38.3 | ||
| No | 2424 | 64.6 | 1339 | 55.2 | 1085 | 44.8 | ||
| Diabetes | 3746 | 2155 | 1591 | 0.0105 | ||||
| Yes | 741 | 19.8 | 457 | 61.7 | 284 | 38.3 | ||
| No | 3005 | 80.2 | 1698 | 56.5 | 1307 | 43.5 | ||
| Hepatitis | 3738 | 2146 | 1592 | 0.0156 | ||||
| Yes | 151 | 4.0 | 101 | 66.9 | 50 | 33.1 | ||
| No | 3587 | 96.0 | 2045 | 57.0 | 1542 | 43.0 | ||
| Tuberculosis | 3739 | 2147 | 1592 | 0.3104 | ||||
| Yes | 145 | 3.9 | 89 | 61.4 | 56 | 38.6 | ||
| No | 3594 | 96.1 | 2058 | 57.3 | 1536 | 42.7 | ||
| Dialysis | 3735 | 2146 | 1589 | 0.8477 | ||||
| Yes | 75 | 2.0 | 43 | 57.3 | 32 | 42.7 | ||
| No | 3660 | 98.0 | 2103 | 57.5 | 1557 | 42.5 | ||
| Charlson’s Comorbidity Index | <0.0001 | |||||||
| 0 | 1075 | 28.4 | 623 | 58 | 452 | 42 | ||
| 1 | 393 | 10.4 | 229 | 58.3 | 164 | 41.7 | ||
| 2 | 1614 | 42.7 | 916 | 56.8 | 698 | 43.2 | ||
| 3+ | 702 | 18.6 | 413 | 58.8 | 289 | 41.2 | ||
| AP’s subjective severity * | <0.0001 | |||||||
| 0~9 | 239 | 6.3 | 99 | 41.4 | 140 | 58.6 | ||
| 10~19 | 444 | 11.7 | 226 | 50.9 | 218 | 49.1 | ||
| 20~29 | 619 | 16.4 | 341 | 55.1 | 278 | 44.9 | ||
| 30~39 | 526 | 13.9 | 276 | 52.5 | 250 | 47.5 | ||
| 40~49 | 541 | 14.3 | 301 | 55.6 | 240 | 44.4 | ||
| 50~59 | 588 | 15.5 | 435 | 74 | 153 | 26 | ||
| 60~69 | 351 | 9.3 | 265 | 75.5 | 86 | 24.5 | ||
| 70~79 | 259 | 6.8 | 144 | 55.6 | 115 | 44.4 | ||
| 80~89 | 195 | 5.2 | 78 | 40 | 117 | 60 | ||
| 90~100 | 22 | 0.6 | 16 | 72.7 | 6 | 27.3 | ||
| Satisfaction | ||
|---|---|---|
| OR | 95% CI | |
| Accessibility to attending physician | ||
| I was able to meet attending physician soon after the admission | 2.57 | (1.99–3.33) |
| I was able to consult with attending physician when I request a consultation | 2.75 | (2.09–3.61) |
| Attending physician has responded quickly upon the pain management request | 2.23 | (1.81–2.75) |
| Attending physician has responded quickly upon medicine and procedure request | 2.25 | (1.82–2.78) |
| I was able to meet attending physician more than twice a day (including rounding) | 3.46 | (2.82–4.24) |
| Attending physician has spent adequate amount of time in consultation, procedure, and care services | 2.42 | (1.88–3.12) |
| I was able to have answer to my question related to care during admission period of time | 2.39 | (1.92–2.98) |
| Attending physician’s consultation and care service skills | ||
| Attending physician let me talk without interrupting | 2.22 | (1.82–2.70) |
| Attending physician checked to be sure I understood everything | 2.08 | (1.68–2.58) |
| Attending physician communicated fully related to my care and possible negative outcomes | 1.78 | (1.45–2.18) |
| Attending physician was not in a rush when he/she was with me | 1.94 | (1.55–2.42) |
| Attending physician’s explanation was easy to understand | 2.33 | (1.89–2.88) |
| Attending physician showed interest in my views and options about my health | 2.25 | (1.83–2.77) |
| How do you rate attending physician’s skill in diagnosing and treating your medical condition? | 1.86 | (1.51–2.31) |
| Attending physician kept me informed of the plans for my care | 2.02 | (1.62–2.53) |
| How do you rate attending physician’s fund of knowledge? | 1.65 | (1.34–2.02) |
| Attending physician effectively prepared me for discharge | 1.58 | (1.25–2.10) |
| Attending physician re-explained discharge guidelines in details at discharge | 1.98 | (1.58–2.49) |
| Overall satisfaction evaluation | ||
| Overall satisfaction on attending physician (beta, p-value) | 0.431 | <0.0001 |
| Overall satisfaction on hospital service (beta, p-value) | 0.371 | <0.0001 |
| Overall satisfaction on my health status prior to the admission (beta, p-value) | 0.263 | 0.0004 |
| I would pay extra cost to admitted in the medical ward where care and services are provided specialist (hospitalist) | 44.07 | (31.69–61.29) |
| Medical Division | ||||
|---|---|---|---|---|
| Internal Medicine | Surgery | |||
| OR | 95% CI | OR | 95% CI | |
| Accessibility to attending physician | ||||
| I was able to meet attending physician soon after the admission | 3.38 | (2.38–4.81) | 1.30 | (0.86–1.97) |
| I was able to consult with attending physician when I request a consultation | 3.59 | (2.48–5.20) | 1.15 | (0.73–1.81) |
| Attending physician has responded quickly upon the pain management request | 3.90 | (2.20–3.84) | 1.06 | (0.74–1.51) |
| Attending physician has responded quickly upon medicine and procedure request | 2.84 | (2.16–3.75) | 1.14 | (0.79–1.63) |
| I was able to meet attending physician more than twice a day (including rounding) | 3.47 | (2.73–4.41) | 3.68 | (2.43–5.55) |
| Attending physician has spent adequate amount of time in consultation, procedure, and care services | 3.19 | (2.26–4.50) | 1.20 | (0.80–1.81) |
| I was able to have answer to my question related to care during admission period of time | 3.09 | (2.31–4.13) | 1.06 | (0.72–1.55) |
| Attending physician’s consultation and care service | ||||
| Attending physician let me talk without interrupting | 2.70 | (2.10–3.47) | 1.19 | (0.79–1.78) |
| Attending physician checked to be sure I understood everything | 2.53 | (1.92–3.32) | 1.15 | (0.74–1.80) |
| Attending physician communicated fully related to my care and possible negative outcomes | 2.01 | (1.56–2.60) | 0.98 | (0.64–1.50) |
| Attending physician was not in a rush when he/she was with me | 2.55 | (1.89–3.43) | 0.82 | (0.52–1.27) |
| Attending physician’s explanation was easy to understand | 2.86 | (2.17–3.77) | 1.20 | (0.79–1.84) |
| Attending physician showed interest in my views and options about my health | 2.88 | (2.20–3.76) | 1.55 | (0.73–1.70) |
| How do you rate attending physician’s skill in diagnosing and treating your medical condition? | 2.29 | (1.72–3.03) | 0.92 | (0.61–1.41) |
| Attending physician kept me informed of the plans for my care | 2.71 | (2.01–3.65) | 0.89 | (0.57–1.38) |
| How do you rate attending physician’s fund of knowledge? | 1.71 | (1.32–2.22) | 1.43 | (0.93–2.19) |
| Attending physician effectively prepared me for discharge | 1.77 | (1.30–2.41) | 1.08 | (0.67–1.74) |
| Attending physician re-explained discharge guidelines in details at discharge | 2.27 | (1.69–3.05) | 1.03 | (0.65–1.62) |
| Surgical patient only | ||||
| I am satisfied with the overall treatment and management after surgery | 1.02 | (0.66–1.60) | ||
| I am received satisfactory care when I requested for pain control at the surgical site | 1.10 | (0.71–1.72) | ||
| I am satisfied with the operation site infection management | 1.17 | (0.75–1.82) | ||
| Satisfaction evaluation | ||||
| Overall satisfaction on attending physician (beta, p-value) | 0.610 | <0.0001 | 0.253 | 0.0117 |
| Overall satisfaction on hospital service (beta, p-value) | 0.554 | <0.0001 | 0.138 | 0.2289 |
| Overall satisfaction on my health status prior to the admission (beta, p-value) | 0.296 | <0.0001 | 0.293 | 0.0156 |
| I would pay extra cost to admitted in the medical ward where care and services are provided specialist (hospitalist) | 37.94 | (23.81–60.47) | 29.65 | (11.24–78.22) |
| Region | ||||
|---|---|---|---|---|
| Capital Area | Rural Area | |||
| OR | 95% CI | OR | 95% CI | |
| Accessibility to attending physician | ||||
| I was able to meet attending physician soon after the admission | 1.69 | (1.27–2.25) | 42.40 | (8.84–203.25) |
| I was able to consult with attending physician when I request a consultation | 1.50 | (1.10–2.04) | 51.51 | (13.58–195.35) |
| Attending physician has responded quickly upon the pain management request | 1.28 | (1.01–1.63) | 35.48 | (12.91–97.49) |
| Attending physician has responded quickly upon medicine and procedure request | 1.43 | (1.13–1.81) | 25.82 | (9.81–67.98) |
| I was able to meet attending physician more than twice a day (including rounding) | 2.08 | (1.63–2.63) | 30.94 | (16.04–68.67) |
| Attending physician has spent adequate amount of time in consultation, procedure, and care services | 1.56 | (1.18–2.05) | 83.43 | (9.93–701.11) |
| I was able to have answer to my question related to care during admission period of time | 1.29 | (1.01–1.65) | 49.76 | (29.74–83.26) |
| Attending physician’s consultation and care service | ||||
| Attending physician let me talk without interrupting | 1.57 | (1.25–1.96) | 6.74 | (3.62–12.58) |
| Attending physician checked to be sure I understood everything | 1.33 | (1.04–1.69) | 15.71 | (6.80–36.29) |
| Attending physician communicated fully related to my care and possible negative outcomes | 1.09 | (0.86–1.37) | 6.34 | (3.45–11.68) |
| Attending physician was not in a rush when he/she was with me | 1.19 | (0.93–1.53) | 16.22 | (5.76–45.69) |
| Attending physician’s explanation was easy to understand | 1.37 | (1.08–1.74) | 15.54 | (6.53–36.99) |
| Attending physician showed interest in my views and options about my health | 1.38 | (1.09–1.75) | 9.14 | (4.44–18.80) |
| How do you rate attending physician’s skill in diagnosing and treating your medical condition? | 1.27 | (1.00–1.61) | 13.79 | (5.65–33.67) |
| Attending physician kept me informed of the plans for my care | 1.34 | (0.97–1.60) | 21.17 | (7.49–58.81) |
| How do you rate attending physician’s fund of knowledge? | 1.20 | (0.94–1.50) | 4.19 | (2.25–7.82) |
| Attending physician effectively prepared me for discharge | 0.92 | (0.70–1.21) | 17.37 | (6.12–49.31) |
| Attending physician re-explained discharge guidelines in details at discharge | 1.07 | (0.82–1.39) | 25.63 | (9.74–67.44) |
| Satisfaction evaluation | ||||
| Overall satisfaction on attending physician (beta, p-value) | 0.247 | 0.0027 | 1.013 | <0.0001 |
| Overall satisfaction on hospital service (beta, p-value) | 0.223 | 0.0099 | 0.748 | <0.0001 |
| Overall satisfaction on my health status prior to the admission (beta, p-value) | 0.173 | 0.0583 | 0.503 | 0.0013 |
| I would pay extra cost to admitted in the medical ward where care and services are provided specialist (hospitalist) | 42.36 | (27.76–6.40) | 102.11 | (39.10–266.67) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chae, W.; Kim, J.; Park, E.-C.; Jang, S.-I. Comparison of Patient Satisfaction in Inpatient Care Provided by Hospitalists and Nonhospitalists in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 8101. https://doi.org/10.3390/ijerph18158101
Chae W, Kim J, Park E-C, Jang S-I. Comparison of Patient Satisfaction in Inpatient Care Provided by Hospitalists and Nonhospitalists in South Korea. International Journal of Environmental Research and Public Health. 2021; 18(15):8101. https://doi.org/10.3390/ijerph18158101
Chicago/Turabian StyleChae, Wonjeong, Juyeong Kim, Eun-Cheol Park, and Sung-In Jang. 2021. "Comparison of Patient Satisfaction in Inpatient Care Provided by Hospitalists and Nonhospitalists in South Korea" International Journal of Environmental Research and Public Health 18, no. 15: 8101. https://doi.org/10.3390/ijerph18158101
APA StyleChae, W., Kim, J., Park, E.-C., & Jang, S.-I. (2021). Comparison of Patient Satisfaction in Inpatient Care Provided by Hospitalists and Nonhospitalists in South Korea. International Journal of Environmental Research and Public Health, 18(15), 8101. https://doi.org/10.3390/ijerph18158101