
Rating of Perceived Exertion as a Method to Determine Training Loads in Strength Training in Elderly Women: A Randomized Controlled Study


 , , and
, , and
Abstract
:1. Introduction
2. Methods
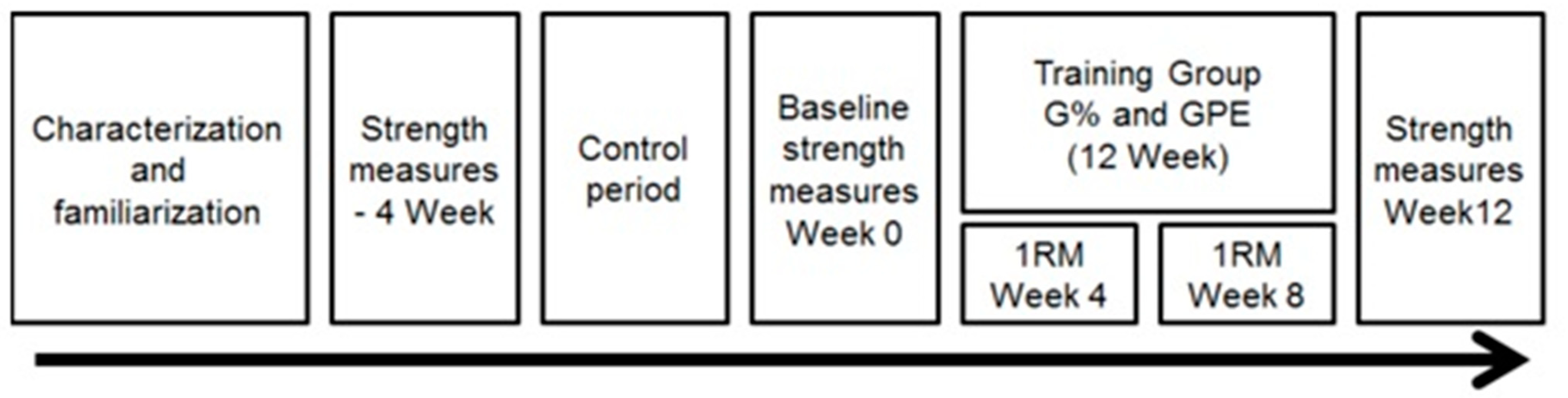
2.1. Experimental Approach to the Problem
2.2. Subjects
2.3. Procedures
2.4. Characterization and Familiarization Stages
2.5. Maximum Dynamic Strength
2.6. Muscular Endurance
2.7. Strength Training Programs
2.8. Statistical Analysis
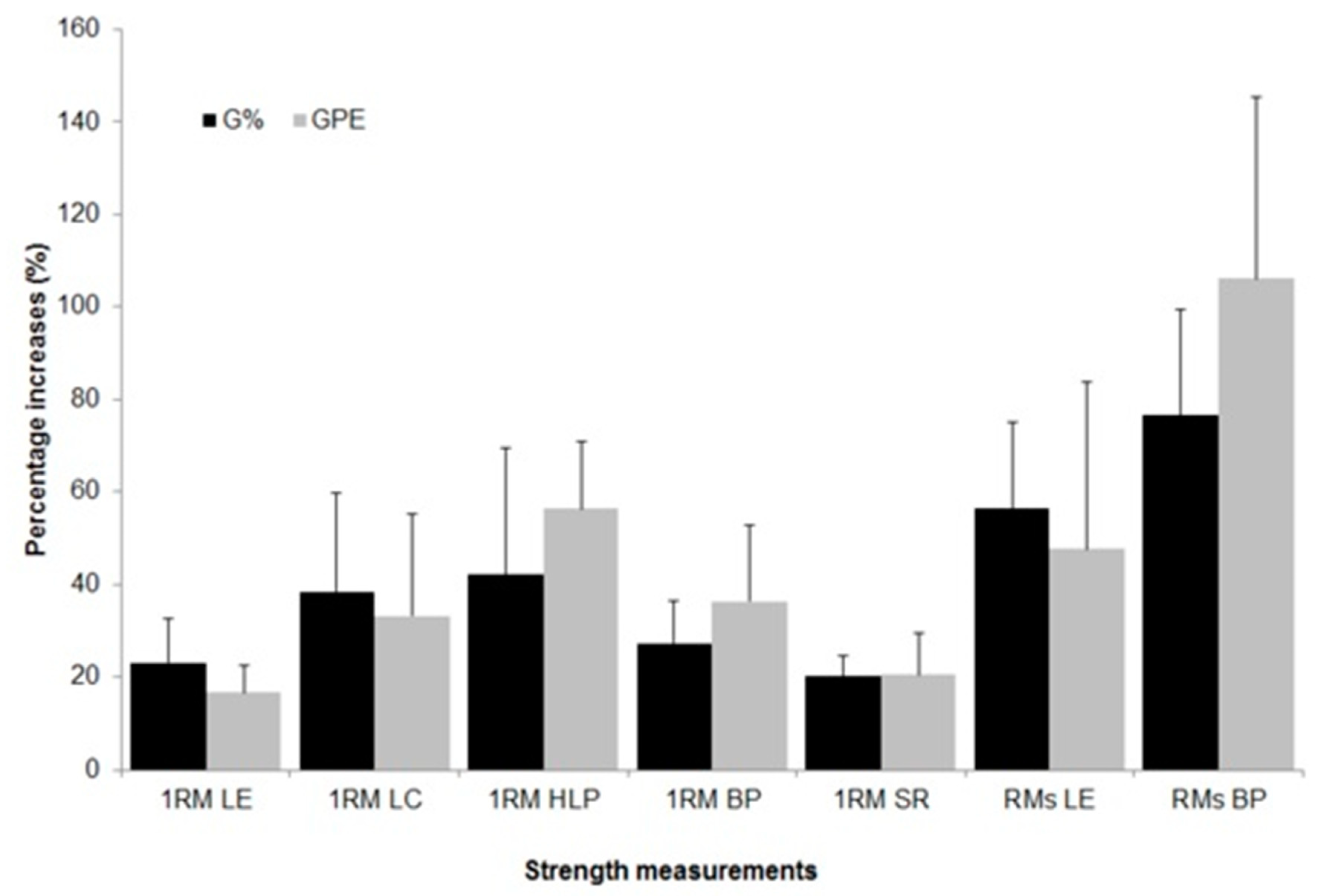
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tiggemann, C.L.; Dias, C.P.; Radaelli, R.; Massa, J.C.; Bortoluzzi, R.; Schoenell, M.C.W.; Noll, M.; Alberton, C.L.; Kruel, L.F.M. Effect of traditional resistance and power training using rated perceived exertion for enhancement of muscle strength, power, and functional performance. Age 2016, 38, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bemben, D.A.; Fetters, N.L.; Bemben, M.G.; Nabavi, N.; Koh, E.T. Musculoskeletal responses to high- and low-intensity resistance training in early postmenopausal women. Med. Sci. Sports Exerc. 2000, 32, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Dias, C.P.; Toscan, R.; de Camargo, M.; Pereira, E.P.; Griebler, N.; Baroni, B.M.; Tiggemann, C.L. Effects of eccentric-focused and conventional resistance training on strength and functional capacity of older adults. Age 2015, 37, 99. [Google Scholar] [CrossRef] [Green Version]
- Tan, B. Manipulating Resistance Training Program Variables to Optimize Maximum Strength in Men: A Review. J. Strength Cond. Res. 1999, 13, 289–304. [Google Scholar] [CrossRef]
- Bottaro, M.; Machado, S.N.; Nogueira, W.; Scales, R.; Veloso, J. Effect of high versus low-velocity resistance training on muscular fitness and functional performance in older men. Eur. J. Appl. Physiol. 2007, 99, 257–264. [Google Scholar] [CrossRef]
- Robertson, R.J.; Noble, B.J. Perception of physical exertion: Methods, mediators, and applications. Exerc. Sport Sci. Rev. 1997, 25, 407–452. [Google Scholar] [CrossRef]
- Tiggemann, C.L.; Korzenowski, A.L.; Brentano, M.A.; Tartaruga, M.P.; Alberton, C.L.; Kruel, L.F.M. Perceived Exertion in Different Strength Exercise Loads in Sedentary, Active, and Trained Adults. J. Strength Cond. Res. 2010, 24, 2032–2041. [Google Scholar] [CrossRef]
- Feigenbaum, M.S.; Pollock, M.L. Prescription of resistance training for health and disease. Med. Sci. Sports Exerc. 1999, 31, 38–45. [Google Scholar] [CrossRef]
- Bjarnason-Wehrens, B.; Mayer-Berger, W.; Meister, E.R.; Baum, K.; Hambrecht, R.; Gielen, S. Recommendations for resistance exercise in cardiac rehabilitation. Recommendations of the German Federation for Cardiovascular Prevention and Rehabilitation. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 352–361. [Google Scholar] [CrossRef]
- Tomporowski, P.D. Men’s and women’s perceptions of effort during progressive-resistance strength training. Percept. Mot. Skills 2001, 92, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Vincent, K.R.; Braith, R.W.; Feldman, R.A.; Kallas, H.E.; Lowenthal, D.T. Improved cardiorespiratory endurance following 6 months of resistance exercise in elderly men and women. Arch. Intern. Med. 2002, 162, 673–678. [Google Scholar] [CrossRef]
- Barrett, C.J.; Smerdely, P. A comparison of community-based resistance exercise and flexibility exercise for seniors. Aust. J. Physiother. 2002, 48, 215–219. [Google Scholar] [CrossRef] [Green Version]
- Bean, J.F.; Kiely, D.K.; LaRose, S.; O’Neill, E.; Goldstein, R.; Frontera, W.R. Increased velocity exercise specific to task training versus the National Institute on Aging’s strength training program: Changes in limb power and mobility. J. Gerontol. A. Biol. Sci. Med. Sci. 2009, 64, 983–991. [Google Scholar] [CrossRef] [Green Version]
- De Vreede, P.L.; Samson, M.M.; Van Meeteren, N.L.U.; Duursma, S.A.; Verhaar, H.J.J. Functional-Task Exercise Versus Resistance Strength Exercise to Improve Daily Function in Older Women: A Randomized, Controlled Trial. J. Am. Geriatr. Soc. 2005, 53, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Nelson, M.E.; Fiatarone, M.A.; Morganti, C.M.; Trice, I.; Greenberg, R.A.; Evans, W.J. Effects of high-intensity strength training on multiple risk factors for osteoporotic fractures. A randomized controlled trial. JAMA 1994, 272, 1909–1914. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults. Med. Sci. Sport. Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Tiggemann, C.L.; Pinto, R.S.; Kruel, L.F.M. Perceived Exertion in Strength Training. Rev. Bras. Med. Esporte 2010, 16, 301–309. [Google Scholar] [CrossRef]
- Pincivero, D.M.; Coelho, A.J.; Erikson, W.H. Perceived exertion during isometric quadriceps contraction. A comparison between men and women. J. Sports Med. Phys. Fitness 2000, 40, 319–326. [Google Scholar]
- Grant, S.; Mayo-Wilson, E.; Montgomery, P.; Macdonald, G.; Michie, S.; Hopewell, S.; Moher, D. CONSORT-SPI 2018 Explanation and Elaboration: Guidance for reporting social and psychological intervention trials. Trials 2018, 19, 406. [Google Scholar] [CrossRef] [Green Version]
- Henwood, T.R.; Taaffe, D.R. Improved physical performance in older adults undertaking a short-term programme of high-velocity resistance training. Gerontology 2005, 51, 108–115. [Google Scholar] [CrossRef]
- IPAQ. Guidelines for data processing and analysis of the International Physical Activity Questionnaire 2005. In: IPAQ. 2005. Available online: http://www.ipaq.ki.se (accessed on 14 November 2018).
- Borg, G. Escalas de Borg para a Dor e Esforço Percebido; Manole: São Paulo, Brazil, 2000. [Google Scholar]
- Gearhart, R.E.; Goss, F.L.; Lagally, K.M.; Jakicic, J.M.; Gallagher, J.; Robertson, R.J. Standardized scaling procedures for rating perceived exertion during resistance exercise. J. Strength Cond. Res. 2001, 15, 320–325. [Google Scholar]
- Lagally, K.M.; McCaw, S.T.; Young, G.T.; Medema, H.C.; Thomas, D.Q. Ratings of perceived exertion and muscle activity during the bench press exercise in recreational and novice lifters. J. Strength Cond. Res. 2004, 18, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Lagally, K.M.; Robertson, R.J. Construct validity of the OMNI resistance exercise scale. J. Strength Cond. Res. 2006, 20, 252–256. [Google Scholar] [CrossRef]
- Brown, L.E.; Weir, J.P. ASEP procedures recommendation I: Accurate assessment of muscular strength and power. J. Exerc. Physiol. Online 2001, 4, 1–21. [Google Scholar]
- Deschenes, M.R.; Kraemer, W.J. Performance and Physiologic Adaptations to Resistance Training. Am. J. Phys. Med. Rehabil. 2002, 81, S3–S16. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Grgic, J.; Van Every, D.W.; Plotkin, D.L. Loading Recommendations for Muscle Strength, Hypertrophy, and Local Endurance: A Re-Examination of the Repetition Continuum. Sports 2021, 9, 32. [Google Scholar] [CrossRef] [PubMed]
- Sweet, T.W.; Foster, C.; McGuigan, M.R.; Brice, G. Quantitation of resistance training using the session rating of perceived exertion method. J. Strength Cond. Res. 2004, 18, 796–802. [Google Scholar] [CrossRef] [Green Version]
- de Vos, N.J.; Singh, N.A.; Ross, D.A.; Stavrinos, T.M.; Orr, R.; Fiatarone Singh, M.A. Optimal load for increasing muscle power during explosive resistance training in older adults. J. Gerontol. A. Biol. Sci. Med. Sci. 2005, 60, 638–647. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, J.; Soares, J. Envelhecimento e força muscular—Breve revisão. Rev. Port. Ciênc. Desporto 2004, 4, 79–93. [Google Scholar] [CrossRef]
- Liu, C.-J.; Latham, N.K. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst. Rev. 2009, 2009, CD002759. [Google Scholar] [CrossRef] [Green Version]
- Schoenfeld, B.J.; Wilson, J.M.; Lowery, R.P.; Krieger, J.W. Muscular adaptations in low- versus high-load resistance training: A meta-analysis. Eur. J. Sport Sci. 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Steib, S.; Schoene, D.; Pfeifer, K. Dose-response relationship of resistance training in older adults: A meta-analysis. Med. Sci. Sports Exerc. 2010, 42, 902–914. [Google Scholar] [CrossRef] [PubMed]
- Galvão, D.A.; Taaffe, D.R. Resistance exercise dosage in older adults: Single- versus multiset effects on physical performance and body composition. J. Am. Geriatr. Soc. 2005, 53, 2090–2097. [Google Scholar] [CrossRef]
- Hunter, G.R.; Treuth, M.S. Relative training intensity and increases in strength in older women. J. Strength Cond. Res. 1995, 9, 188–191. [Google Scholar] [CrossRef]
- Taaffe, D.R.; Pruitt, L.; Pyka, G.; Guido, D.; Marcus, R. Comparative effects of high- and low-intensity resistance training on thigh muscle strength, fiber area, and tissue composition in elderly women. Clin. Physiol. 1996, 16, 381–392. [Google Scholar] [CrossRef]
- Fiatarone, M.A.; O’Neill, E.F.; Ryan, N.D.; Clements, K.M.; Solares, G.R.; Nelson, M.E.; Roberts, S.B.; Kehayias, J.J.; Lipsitz, L.A.; Evans, W.J. Exercise training and nutritional supplementation for physical frailty in very elderly people. N. Engl. J. Med. 1994, 330, 1769–1775. [Google Scholar] [CrossRef] [Green Version]
- Kraemer, W.J.; Adams, K.; Cafarelli, E.; Dudley, G.A.; Dooly, C.; Feigenbaum, M.S.; Fleck, S.J.; Franklin, B.; Fry, A.C.; Hoffman, J.R.; et al. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2002, 34, 364–380. [Google Scholar] [CrossRef]
- Sale, D.G. Influence of exercise and training on motor unit activation. Exerc. Sport Sci. Rev. 1987, 15, 95–151. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.H.; Chandler, T.J.; Conley, M.S.; Kramer, J.B.; Stone, M.E. Training to muscular failure: Is it necessary? Strength Cond. J. 1996, 18, 44–48. [Google Scholar] [CrossRef]
- Willardson, J.M. The application of training to failure in periodized multiple-set resistance exercise programs. J. Strength Cond. Res. 2007, 21, 628–631. [Google Scholar] [CrossRef]
- Nóbrega, S.R.; Libardi, C.A. Is Resistance Training to Muscular Failure Necessary? Front. Physiol. 2016, 7, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izquierdo, M.; Ibañez, J.; González-Badillo, J.J.; Häkkinen, K.; Ratamess, N.A.; Kraemer, W.J.; French, D.N.; Eslava, J.; Altadill, A.; Asiain, X.; et al. Differential effects of strength training leading to failure versus not to failure on hormonal responses, strength, and muscle power gains. J. Appl. Physiol. 2006, 100, 1647–1656. [Google Scholar] [CrossRef] [PubMed]
- Folland, J.P.; Irish, C.S.; Roberts, J.C.; Tarr, J.E.; Jones, D.A. Fatigue is not a necessary stimulus for strength gains during resistance training. Br. J. Sports Med. 2002, 36, 370–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glass, S.C.; Stanton, D.R. Self-selected resistance training intensity in novice weightlifters. J. Strength Cond. Res. 2004, 18, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Perri, M.G.; Anton, S.D.; Durning, P.E.; Ketterson, T.U.; Sydeman, S.J.; Berlant, N.E.; Kanasky, W.F.J.; Newton, R.L.J.; Limacher, M.C.; Martin, A.D. Adherence to exercise prescriptions: Effects of prescribing moderate versus higher levels of intensity and frequency. Heal. Psychol.Off. J. Div. Heal. Psychol. Am. Psychol. Assoc. 2002, 21, 452–458. [Google Scholar] [CrossRef]
- Lagally, K.M.; Costigan, E.M. Anchoring procedures in reliability of ratings of perceived exertion during resistance exercise. Percept. Mot. Skills 2004, 98 Pt 2, 1285–1295. [Google Scholar] [CrossRef]
- Williams, M.A.; Haskell, W.L.; Ades, P.A.; Amsterdam, E.A.; Bittner, V.; Franklin, B.A.; Gulanick, M.; Laing, S.T.; Stewart, K.J. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: A scientific statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 2007, 116, 572–584. [Google Scholar] [CrossRef] [Green Version]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| G% (n = 12) Mean ± SD | GPE (n = 13) Mean ± SD | p Value | |
|---|---|---|---|
| Body mass (kg) | 70.2 ± 8.5 | 65.2 ± 8.9 | 0.167 |
| Height (cm) | 157.6 ± 4.9 | 155.8 ± 5.0 | 0.351 |
| BMI (kg.m−2) | 28.3 ± 3.7 | 26.8 ± 3.1 | 0.291 |
| Age (years) | 66.4 ± 4.5 | 65.6 ± 5.4 | 0.691 |
| Training frequency (%) | 98.1 ± 2.3 | 99.0 ± 2.0 | 0.340 |
| Self-assement health (0 a 10) | 8.3 ± 1.1 | 8.3 ± 1.0 | 0.965 |
| IPAQ–rating (%) | |||
| Sedentary | 16.7 | 23.1 | |
| Moderately active | 75.0 | 53.8 | |
| Very active | 8.3 | 23.1 | |
| Participation in support groups (%) | 58.3 | 69.2 |
| Meso | Micro | Week | SET × REP | %1RM for G% | RPE for GPE |
|---|---|---|---|---|---|
| 1 | 1 | 1–2 | 2 × 15 | 45 | 13 ± 1 |
| 2 | 3–4 | 2 × 15 | 50 | 14 ± 1 | |
| 2 | 3 | 5–6 | 2 × 12 | 55 | 15 ± 1 |
| 4 | 7–8 | 2 × 12 | 60 | 16 ± 1 | |
| 3 | 5 | 9–10 | 3 × 8 | 65 | 17 ± 1 |
| 6 | 11–12 | 3 × 8 | 70 | 18 ± 1 |
| Micro Cycle | G% | GPE | ||
|---|---|---|---|---|
| %1RM | RPE | %1RM | RPE | |
| 1 | 45.1 ± 0.3 | 12.5 ± 1.1 | 45.7 ± 3.7 | 12.5 ± 1.0 |
| 2 | 50.1 ± 0.2 | 13.0 ± 1.1 | 51.6 ± 9.2 | 13.3 ± 1.0 |
| 3 | 55.1 ± 0.3 | 13.5 ± 0.9 | 60.4 ± 4.6 | 13.9 ± 0.8 |
| 4 | 60.0 ± 0.3 | 14.1 ± 1.0 | 68.8 ± 9.9 | 16.3 ± 0.7 |
| 5 | 65.1 ± 0.3 | 14.6 ± 1.1 | 67.5 ± 3.3 | 15.9 ± 1.1 |
| 6 | 70.0 ± 0.2 | 16.2 ± 1.8 | 73.5 ± 7.2 | 17.4 ± 0.8 |
| Week 0 Mean ± SD | Week 4 Mean ± SD | Week 8 Mean ± SD | Week 12 Mean ± SD | Time factor | Group Factor | Time × Group Interaction | |
|---|---|---|---|---|---|---|---|
| 1RM LE (kg) G% GPE | 23.50 ± 3.55 a 24.50 ± 3.08 a | 25.25 ± 3.28 b 26.08 ± 3.03 b | 26.67 ± 2.93 c 27.28 ± 2.49 c | 28.78 ± 3.67 d 28.48 ± 3.30 d | < 0.001 | 0.659 | 0.272 |
| 1RM LC (kg) G% GPE | 14.67 ± 3.23 a 14.31 ± 3.09 a | 16.79 ± 2.63 b 16.48 ± 2.99 b | 18.23 ± 2.11 c 17.68 ± 2.91 c | 19.71 ± 1.96 d 18.56 ± 2.28 d | < 0.001 | 0.565 | 0.454 |
| 1RM HLP(kg) G% GPE | 64.58 ± 12.02 a 61.33 ± 10.46 a | 70.75 ± 11.04 b 70.92 ± 10.09 b | 77.74 ± 14.37 c 82.74 ± 15.66 c | 89.96 ± 16.37 d 95.75 ± 18.33 d | < 0.001 | 0.715 | 0.083 |
| 1RM BP (kg) G% GPE | 28.35 ± 5.22 a 26.63 ± 5.49 a | 31.45 ± 6.00 b 29.71 ± 5.25 b | 32.75 ± 6.33 c 33.13 ± 5.72 c | 36.11 ± 7.23 d 35.71 ± 5.28 d | < 0.001 | 0.721 | 0.120 |
| 1RM SR (kg) G%$$GPE | 40.64 ± 5.92 a 41.08 ± 5.72 a | 44.18 ± 6.37 b 43.85 ± 5.35 b | 47.33 ± 7.07 c 46.08 ± 4.98 c | 48.69 ± 6.45 d 49.19 ± 5.27 d | < 0.001 | 0.946 | 0.193 |
| RMs LE (reps) G% GPE | 8.91 ± 1.45 a 10.46 ± 2.40 a | 13.82 ± 1.99 b 14.92 ± 2.84 b | < 0.001 | 0.102 | 0.665 | ||
| RMs BP (reps) G% GPE | 9.89 ± 1.45 a 10.42 ± 3.26 a | 17.44 ± 3.21 b 20.67 ± 4.52 b | < 0.001 | 0.190 | 0.034 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiggemann, C.L.; Pietta-Dias, C.; Schoenell, M.C.W.; Noll, M.; Alberton, C.L.; Pinto, R.S.; Kruel, L.F.M. Rating of Perceived Exertion as a Method to Determine Training Loads in Strength Training in Elderly Women: A Randomized Controlled Study. Int. J. Environ. Res. Public Health 2021, 18, 7892. https://doi.org/10.3390/ijerph18157892
Tiggemann CL, Pietta-Dias C, Schoenell MCW, Noll M, Alberton CL, Pinto RS, Kruel LFM. Rating of Perceived Exertion as a Method to Determine Training Loads in Strength Training in Elderly Women: A Randomized Controlled Study. International Journal of Environmental Research and Public Health. 2021; 18(15):7892. https://doi.org/10.3390/ijerph18157892
Chicago/Turabian StyleTiggemann, Carlos Leandro, Caroline Pietta-Dias, Maira Cristina Wolf Schoenell, Matias Noll, Cristine Lima Alberton, Ronei Silveira Pinto, and Luiz Fernando Martins Kruel. 2021. "Rating of Perceived Exertion as a Method to Determine Training Loads in Strength Training in Elderly Women: A Randomized Controlled Study" International Journal of Environmental Research and Public Health 18, no. 15: 7892. https://doi.org/10.3390/ijerph18157892
APA StyleTiggemann, C. L., Pietta-Dias, C., Schoenell, M. C. W., Noll, M., Alberton, C. L., Pinto, R. S., & Kruel, L. F. M. (2021). Rating of Perceived Exertion as a Method to Determine Training Loads in Strength Training in Elderly Women: A Randomized Controlled Study. International Journal of Environmental Research and Public Health, 18(15), 7892. https://doi.org/10.3390/ijerph18157892