
Digital Quantification of Occlusal Contacts: A Methodological Study


Abstract
1. Introduction
2. Subjects and Methods
2.1. Sample Description
- a clinical examination with counting of the total number of occlusal contacts (CE method);
- a practical study cast examination with the measurement of the total number of occlusal contacts on stone casts mounted in an articulator (AE method);
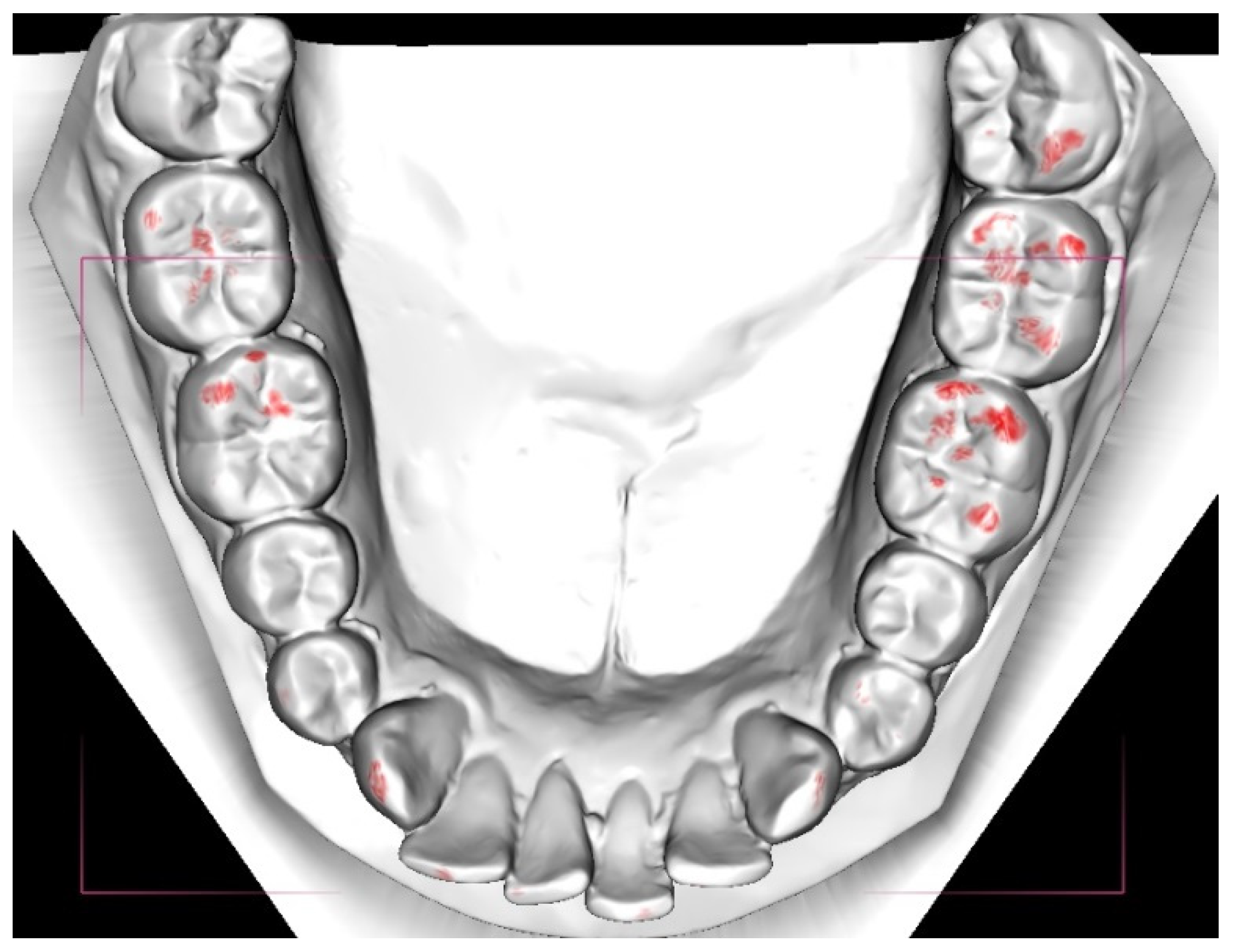
- a digital examination with the measurement of the total occlusal contact area in millimeters (DE method).
2.2. Production and Scanning of Stone Casts
2.3. Clinical Examination (CE)
2.4. Study Cast Examination (AE)
2.5. Digital Examination (DE)
2.6. Statistical Analyses
2.7. Error of Method
3. Results
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Protocol–Clinical measurement of occlusal contacts
- Materials–parotisroll (for moisture control), disposable air/water syringe tip, articulating paper (Trollfolie, 8 µm), articulating foil forceps, camera, mirrors for intraoral photos, dental retractors, mouth mirrors
- Inspection of cleanliness of the participant’s teeth
- Verify that the participant is able to repeat the same intercuspid position
- Moisture control
- 2 parotisrolls
- Verify once more that the participant is able to repeat same intercuspid position (with the parotisrolls in place)
- Blasting with syringe tip
- Occlusal contacts with articulating paper (Trollfolie, 8µm)
- Articulating foil forceps with articulating foil is applied in the following order:
- Molars on the left side
- Premolars on the left side
- Front teeth
- Premolars on the right side
- Molars on the right side
- 2 bites in intercuspid position in every region
- Avoid to drag the articulating foil on the teeth’s surfaces
- Photos on occlusal contacts
- Warming up intraoral mirrors with hot water
- Applying dental retractors
- Photos of the upper and lower jaw
- Clinical measurement of occlusal contacts
- JS & SN counts the occlusal contacts separately and the number of contacts is inserted in to a registration form
- The number of occlusal contacts on each tooth is recorded
- The order of counting contacts is quadrant 1 →2 → 3 → 4
References
- Edward, S. Odontologisk Ordbok; Gothia: Stockholm, Sweden, 2011. [Google Scholar]
- The glossary of prosthodontic terms. J. Prosthet. Dent. 2005, 94, 10–92.
- Angle, E.H. Treatment of Malocclusion of Teeth and Fractures of the Maxillae; Angle’s System; White Dental Manufacturing Co.: Philadelphia, PA, USA, 1900. [Google Scholar]
- Ricketts, R.M. Occlusion–the medium of dentistry. J. Prosthet. Dent. 1969, 21, 39–60. [Google Scholar]
- Andrews, L.F. The six keys to normal occlusion. Am. J. Orthod. 1972, 62, 296–309. [Google Scholar] [CrossRef]
- Turp, J.C.; Greene, C.S.; Strub, J.R. Dental occlusion: A critical reflection on past, present and future concepts. J. Oral Rehabil. 2008, 35, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Holm, A.-K.; Brattström, V.; Hansen, K.; Bondemark, L.; Marké, L.-Å.; Mohlin, B.; Paulin, G.; Pietilä, T.; Svensson, Å. Bettavvikelser och Tandreglering i ett Hälsoperspektiv. Available online: http://www.sbu.se/contentassets/17090202cd864117a22698e16581e177/fulltext_tandreglering.pdf (accessed on 12 March 2020).
- Ramfjord, S.P.; Ash, M.M. Occlusion; Saunders: Philadelphia, PA, USA, 1966. [Google Scholar]
- McNeill, C. Science and Practise of Occlusion; Quintessence: Chicago, IL, USA, 1997. [Google Scholar]
- Riise, C.; Ericsson, S.G. A clinical study of the distribution of occlusal tooth contacts in the intercuspal position at light and hard pressure in adults. J. Oral Rehabil. 1983, 10, 473–480. [Google Scholar]
- Athanasiou, A.E.; Melsen, B.; Kimmel, P. Occlusal tooth contacts in natural normal adult dentition in centric occlusion studied by photocclusion technique. Scand. J. Dent. Res. 1989, 97, 439–445. [Google Scholar] [CrossRef]
- Mohl, N.D. A Textbook of Occlusion; Quintessence Pub. Co.: Chicago, IL, USA, 1988. [Google Scholar]
- Carlsson GE, J.A. Ocklusionens betydelse i klinisk tandvård. Tandläkartidningen 2013, 105, 64–70. [Google Scholar]
- Jokstad, A. Osseointegration and Dental Implants; Wiley-Blackwell: Ames, IA, USA, 2009. [Google Scholar]
- Trulsson, M.; van der Bilt, A.; Carlsson, G.E.; Gotfredsen, K.; Larsson, P.; Muller, F.; Sessle, B.J.; Svensson, P. From brain to bridge: Masticatory function and dental implants. J. Oral Rehabil. 2012, 39, 858–877. [Google Scholar] [CrossRef] [PubMed]
- Millstein, P.L. An evaluation of occlusal contact marking indicators: A descriptive, qualitative method. Quintessence Int. Dent. Dig. 1983, 14, 813–836. [Google Scholar]
- Saad, M.N.; Weiner, G.; Ehrenberg, D.; Weiner, S. Effects of load and indicator type upon occlusal contact markings. J. Biomed. Mater. Res. Part B Appl. Biomater. 2008, 85, 18–22. [Google Scholar] [CrossRef]
- Bozhkova, T.P. Comparative Study of Occlusal Contact Marking Indicators. Folia Med. 2020, 62, 180–184. [Google Scholar] [CrossRef]
- Sjogren, A.P.; Lindgren, J.E.; Huggare, J.A. Orthodontic study cast analysis--reproducibility of recordings and agreement between conventional and 3D virtual measurements. J. Digit. Imaging 2010, 23, 482–492. [Google Scholar] [CrossRef] [PubMed]
- Westerlund, A.; Tancredi, W.; Ransjo, M.; Bresin, A.; Psonis, S.; Torgersson, O. Digital casts in orthodontics: A comparison of 4 software systems. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Fleming, P.S.; Marinho, V.; Johal, A. Orthodontic measurements on digital study models compared with plaster models: A systematic review. Orthod. Craniofacial Res. 2011, 14, 1–16. [Google Scholar] [CrossRef]
- Nalcaci, R.; Topcuoglu, T.; Ozturk, F. Comparison of Bolton analysis and tooth size measurements obtained using conventional and three-dimensional orthodontic models. Eur. J. Dent. 2013, 7, S66–S70. [Google Scholar] [CrossRef]
- Sousa, M.V.; Vasconcelos, E.C.; Janson, G.; Garib, D.; Pinzan, A. Accuracy and reproducibility of 3-dimensional digital model measurements. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Stevens, D.R.; Flores-Mir, C.; Nebbe, B.; Raboud, D.W.; Heo, G.; Major, P.W. Validity, reliability, and reproducibility of plaster vs digital study models: Comparison of peer assessment rating and Bolton analysis and their constituent measurements. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 794–803. [Google Scholar] [CrossRef] [PubMed]
- Leung, C.V.; Yang, Y.; Liao, C.; Hägg, U.; Wong, R.W.K.; McGrath, C.; Gu, M. Digital Models as an Alternative to Plaster Casts in Assessment of Orthodontic Treatment Outcomes. Sci. World J. 2018, 2018, 9819384. [Google Scholar] [CrossRef]
- McCrory, E.; McGuinness, N.J.; Ulhaq, A. Reproducibility of the index of orthognathic functional treatment need scores derived from plaster study casts and their three-dimensional digital equivalents: A pilot study. J. Orthod. 2018, 45, 94–101. [Google Scholar] [CrossRef]
- Ayuso-Montero, R.; Mariano-Hernandez, Y.; Khoury-Ribas, L.; Rovira-Lastra, B.; Willaert, E.; Martinez-Gomis, J. Reliability and Validity of T-scan and 3D Intraoral Scanning for Measuring the Occlusal Contact Area. J. Prosthodont. 2020, 29, 19–25. [Google Scholar] [CrossRef]
- Afrashtehfar, K.I.; Qadeer, S. Computerized occlusal analysis as an alternative occlusal indicator. Cranio 2016, 34, 52–57. [Google Scholar] [CrossRef]
- Solaberrieta, E.; Otegi, J.R.; Goicoechea, N.; Brizuela, A.; Pradies, G. Comparison of a conventional and virtual occlusal record. J. Prosthet. Dent. 2015, 114, 92–97. [Google Scholar] [CrossRef]
- Qadeer, S.; Yang, L.; Sarinnaphakorn, L.; Kerstein, R.B. Comparison of closure occlusal force parameters in post-orthodontic and non-orthodontic subjects using T-Scan(R) III DMD occlusal analysis. Cranio 2016, 34, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Cabral, C.W.L.F.; Silva, F.A.; Silva, W.A.B.; Landulpho, A.B.; Silva, L.B. Comparison between two methods to record occlusal contacts in habitual maximal intercuspation. Braz. J. Oral Sci. 2016, 5, 1239–1243. [Google Scholar] [CrossRef]
- Schelb, E.; Kaiser, D.A.; Brukl, C.E. Thickness and marking characteristics of occlusal registration strips. J. Prosthet. Dent. 1985, 54, 122–126. [Google Scholar] [CrossRef]
- Clark, J.R.; Evans, R.D. Functional occlusion: I. A review. J. Orthod. 2001, 28, 76–81. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intra-examiner | ICC | ICC–CI 95% | |
|---|---|---|---|
| Examiner 1 | - Clinical examination | 0.909 | 0.810–0.956 |
| - Study cast examination | 0.797 | 0.147–0.929 | |
| Examiner 2 | - Clinical examination | 0.939 | 0.799–0.976 |
| - Study cast examination | 0.862 | 0.558–0.945 | |
| Inter-examiner | ICC | ICC–CI 95% | |
| Clinical examination | 0.939 | 0.847–0.973 | |
| Study cast examination | 0.935 | 0.865–0.969 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sigvardsson, J.; Nilsson, S.; Ransjö, M.; Westerlund, A. Digital Quantification of Occlusal Contacts: A Methodological Study. Int. J. Environ. Res. Public Health 2021, 18, 5297. https://doi.org/10.3390/ijerph18105297
Sigvardsson J, Nilsson S, Ransjö M, Westerlund A. Digital Quantification of Occlusal Contacts: A Methodological Study. International Journal of Environmental Research and Public Health. 2021; 18(10):5297. https://doi.org/10.3390/ijerph18105297
Chicago/Turabian StyleSigvardsson, Jacob, Samuel Nilsson, Maria Ransjö, and Anna Westerlund. 2021. "Digital Quantification of Occlusal Contacts: A Methodological Study" International Journal of Environmental Research and Public Health 18, no. 10: 5297. https://doi.org/10.3390/ijerph18105297
APA StyleSigvardsson, J., Nilsson, S., Ransjö, M., & Westerlund, A. (2021). Digital Quantification of Occlusal Contacts: A Methodological Study. International Journal of Environmental Research and Public Health, 18(10), 5297. https://doi.org/10.3390/ijerph18105297