
Can Social Prescribing Foster Individual and Community Well-Being? A Systematic Review of the Evidence


Abstract
1. Introduction
1.1. Key Outcomes
1.2. Effects at Multiple Levels
1.3. The Need for Evidence
2. Materials and Methods
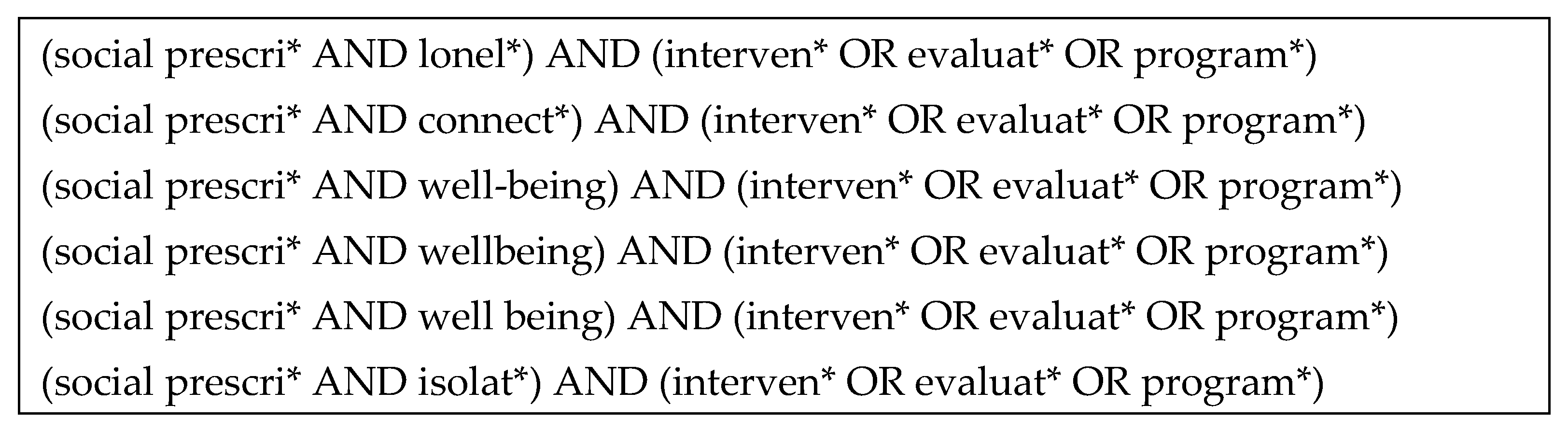
2.1. Research Strategy
2.2. Data Synthesis
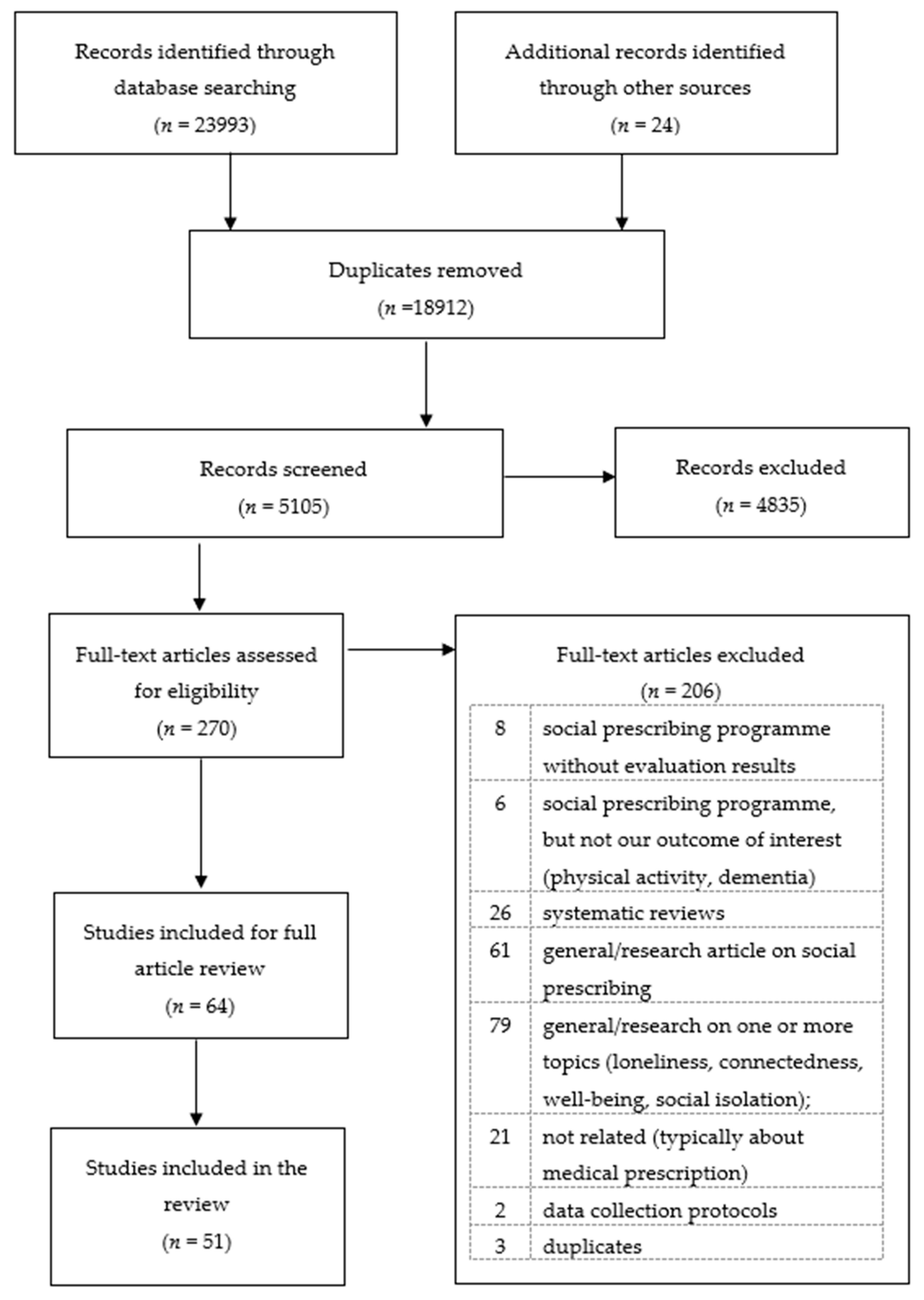
2.3. Inclusion Criteria and Study Identification
3. Results
3.1. Study Characteristics
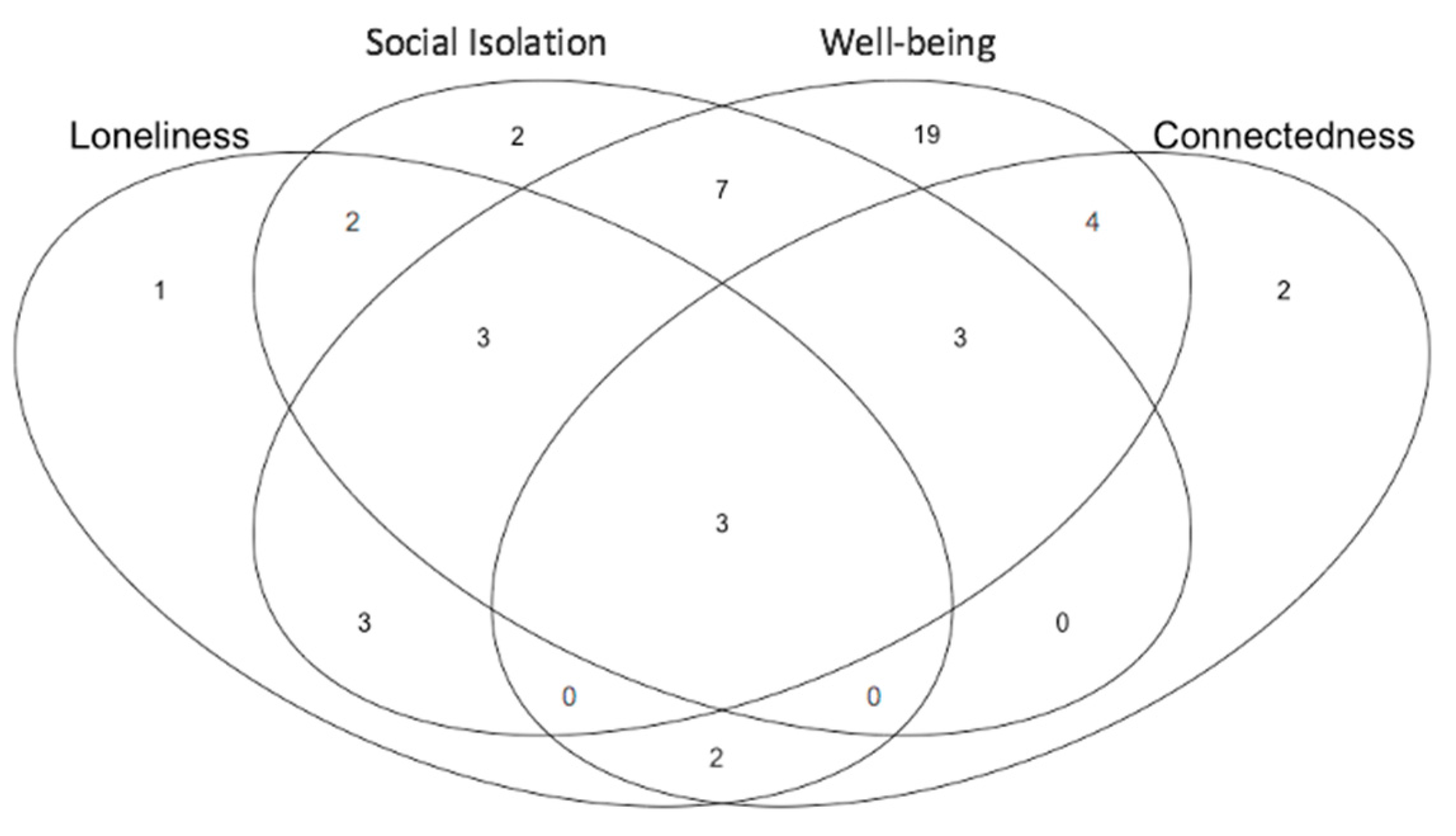
3.2. Outcome Measures
3.3. Impact on the Individual
3.4. Impact on the System
3.5. Impact on the Community
4. Discussion
4.1. Programme and Design and Measurement Selection
4.2. Programme Delivery
4.3. COVID-19
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. Health. United Nations Sustainable Development Goals: Health. Available online: https://www.un.org/sustainabledevelopment/health/ (accessed on 16 February 2021).
- Tierney, S.; Mahtani, K.R.; Turk, A. Can Social Prescribing Support the COVID-19 Pandemic? The Centre for Evidence-Based Medicine. 2020. Available online: https://www.cebm.net/covid-19/can-social-prescribing-support-the-covid-19-pandemic/ (accessed on 16 November 2020).
- Drinkwater, C.; Wildman, J.; Moffatt, S. Social prescribing. BMJ 2019, 364, l1285. [Google Scholar] [CrossRef]
- Polley, M.; Chatterjee, H.; Clayton, G. Social Prescribing: Community-based referral in public health. Perspect. Public Health 2017, 138, 18–19. [Google Scholar]
- NHS England. Universal Personalised Care: Implementing the Comprehensive Model. 2019. Available online: https://www.england.nhs.uk/publication/universal-personalised-care-implementing-the-comprehensive-model/ (accessed on 10 February 2020).
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Lang, I.; Byng, R.; Garside, R. What approaches to social prescribing work, for whom, and in what circumstances? A realist review. Health Soc. Care Community 2019, 28, 309–324. [Google Scholar] [CrossRef] [PubMed]
- Perlman, D.; Peplau, L.A. Toward a Social Psychology of Loneliness. In Personal Relationships: Personal Relationships in Disorder; Gilmour, R., Duck, S., Eds.; Academic Press: London, UK, 1981; pp. 31–56. [Google Scholar]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness Matters: A Theoretical and Empirical Review of Consequences and Mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef] [PubMed]
- New Economics Foundation and Coop. The Cost of Loneliness to UK Employers. 2017. Available online: https://www.campaigntoendloneliness.org/wp-content/uploads/cost-of-loneliness-2017.pdf (accessed on 27 July 2020).
- Fulton and Jupp. Investing to Tackle Loneliness: A Discussion Paper. Social Finance UK. 2015. Available online: https://www.socialfiac.og.uk/sis/dfaul/fils/publicaios/ivsig_o_ackl_loliss.pdf (accessed on 27 July 2020).
- HM Government. A Connected Society: A Strategy for Tackling Loneliness. GOV.UK. 2018. Available online: https://www.gov.uk/government/publications/a-connected-society-a-strategy-for-tackling-loneliness (accessed on 10 February 2020).
- HM Government. Loneliness Annual Report January 2020. GOV.UK. 2020. Available online: https://www.gov.uk/government/publications/loneliness-annual-report-the-first-year/loneliness-annual-report-january-2020--2 (accessed on 26 January 2020).
- The Commonwealth Fund. Solutions from around the World: Tackling Loneliness and Social Isolation During COVID-19 | Commonwealth Fund. 2020. Available online: https://www.commonwealthfund.org/blog/2020/solutions-around-world-tackling-loneliness-and-social-isolation-during-covid-19 (accessed on 25 November 2020).
- Mansfield, L.; Daykin, N.; Meads, C.; Tomlinson, A.; Gray, K.; Lane, J.; Victor, C. A Conceptual Review of Loneliness Across the Adult Life Course (16+ years). Synthesis of Qualitative Studies. 2019. Available online: https://whatworkswellbeing.org/wp-content/uploads/2020/02/V3-FINAL-Loneliness-conceptual-review.pdf (accessed on 8 June 2020).
- Achterbergh, L.; Pitman, A.; Birken, M.; Pearce, E.; Sno, H.; Johnson, S. The experience of loneliness among young people with depression: A qualitative meta-synthesis of the literature. BMC Psychiatry 2020, 20, 415. [Google Scholar] [CrossRef]
- VanderWeele, T.J.; Trudel-Fitzgerald, C.; Allin, P.; Farrelly, C.; Fletcher, G.; Frederick, D.E.; Hall, J.; Helliwell, J.F.; Kim, E.S.; Lauinger, W.A.; et al. Current recommendations on the selection of measures for well-being. Prev. Med. 2020, 133, 106004. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, K.; Abdallah, S.; Quick, A. Europeans’ Personal and Social Wellbeing. 2015. Available online: http://www.europeansocialsurvey.org/docs/findings/ESS6_toplines_issue_5_personal_and_social_wellbeing.pdf (accessed on 18 November 2020).
- Diener, E.; Chan, M.Y. Happy People Live Longer: Subjective Well-Being Contributes to Health and Longevity. Appl. Psychol. Health Well Being 2011, 3, 1–43. [Google Scholar] [CrossRef]
- Frijters, P.; Clark, A.E.; Krekel, C.; Layard, R. A happy choice: Wellbeing as the goal of government. Behav. Public Policy 2020, 4, 126–165. [Google Scholar] [CrossRef]
- New Economics Foundation National Accounts of Well-Being: Bringing Real Wealth onto the Balance Sheet. 2009. Available online: https://neweconomics.org/uploads/files/2027fb05fed1554aea_uim6vd4c5.pdf (accessed on 17 November 2020).
- Ministry of Social Development(MSD). Social Connectedness and Wellbeing—Ministry of Social Development. Available online: https://www.msd.govt.nz/about-msd-and-our-work/publications-resources/literature-reviews/social-connectedness-and-wellbeing.html (accessed on 20 November 2020).
- Lee, R.; Robbins, S. Measuring Belongingness: The Social Connectedness and the Social Assurance Scales. J. Couns. Psychol. 1995, 42, 232–241. [Google Scholar] [CrossRef]
- Halder, M.M.; Wakefield, J.R.; Bowe, M.; Kellezi, B.; Mair, E.; McNamara, N.; Wilson, I.; Stevenson, C. Evaluation and exploration of a social prescribing initiative: Study protocol. J. Health Psychol. 2018. [Google Scholar] [CrossRef]
- Stickley, T.; Hui, A. Social prescribing through arts on prescription in a U.K. city: Participants’ perspectives (part 1). Public Health 2012, 126, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Batt-Rawden, K.; Andersen, S. ‘Singing has empowered, enchanted and enthralled me’-choirs for wellbeing? Health Promot. Int. 2020, 35, 140–150. [Google Scholar] [CrossRef]
- Wigfield, A.; Kispeter, E.; Alden, S.; Turner, R.; Clarke, T. Age UK’s Fit for the Future Project: Evaluation report. Circ Leeds Available Www Ageuk Org Ukhealth-Wellbeingfit—Fiddlefit—Futur 27 Sept 2016. 2015. Available online: https://www.sheffield.ac.uk/polopoly_fs/1.569567!/file/fit-for-the-future-Final-Evaluation.pdf (accessed on 6 October 2020).
- Wakefield, J.R.H.; Kellezi, B.; Stevenson, C.; McNamara, N.; Bowe, M.; Wilson, I.; Halder, M.M.; Mair, E. Social Prescribing as ‘Social Cure’: A longitudinal study of the health benefits of social connectedness within a Social Prescribing pathway. J. Health Psychol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sears, L.E.; Shi, Y.; Coberley, C.R.; Pope, J.E. Overall Well-Being as a Predictor of Health Care, Productivity, and Retention Outcomes in a Large Employer. Popul. Health Manag. 2013, 16, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Makridis, C.A.; Wu, C. How social capital helps communities weather the COVID-19 pandemic. PLoS ONE 2021, 16, e0245135. [Google Scholar] [CrossRef] [PubMed]
- Reinhardt, G.Y. Race, Trust, and Return Migration: The Political Drivers of Post-disaster Resettlement. Polit. Res. Q. 2015, 68, 350–362. [Google Scholar] [CrossRef]
- Ziglio, E.; Azzopardi-Muscat, N.; Briguglio, L. Resilience and 21st century public health. Eur. J. Public Health 2017, 27, 789–790. [Google Scholar] [CrossRef]
- NHS England. Social Prescribing and Community-Based Support: Summary Guide. Available online: https://www.england.nhs.uk/wp-content/uploads/2019/01/social-prescribing-community-based-support-summary-guide.pdf (accessed on 26 January 2020).
- Cerb The Cost of Disconnected Communities Executive Summary—Eden Project Communities. Available online: https://www.edenprojectcommunities.com/sites/default/files/The%20Cost%20of%20Disconnected%20Communities%20Executive%20Summary%20-%20Eden%20Project%20Communities%20and%20Cebr.pdf (accessed on 27 January 2020).
- NHS England NLT. The NHS Long Term Plan. Available online: https://www.longtermplan.nhs.uk/publication/nhs-long-term-plan/ (accessed on 20 November 2020).
- Husk, K.; Elston, J.; Gradinger, F.; Callaghan, L.; Asthana, S. Social prescribing: Where is the evidence? Br. J. Gen. Pract. 2019, 69, 6–7. [Google Scholar] [CrossRef]
- Heijnders, M.L.; Meijs, J.J. ‘Welzijn op Recept’ (Social Prescribing): A helping hand in re-establishing social contacts—An explorative qualitative study. Prim. Health Care Res. Dev. 2018, 19, 223–231. [Google Scholar] [CrossRef]
- Aggar, C.; Thomas, T.; Gordon, C.; Bloomfield, J.; Baker, J. Social Prescribing for Individuals Living with Mental Illness in an Australian Community Setting: A Pilot Study. Community Ment. Health J. 2021, 57, 189–195. [Google Scholar] [CrossRef]
- Poulos, R.G.; Marwood, S.; Harkin, D.; Opher, S.; Clift, S.; Cole, A.M.D.; Rhee, J.; Beilharz, K.; Poulos, C.J. Arts on prescription for community-dwelling older people with a range of health and wellness needs. Health Soc. Care Community 2018, 27, 483–492. [Google Scholar] [CrossRef]
- Raynor, A.J.; Iredale, F.; Crowther, R.; White, J.; Dare, J. It’s Not Just Physical: Exercise Physiologist-Led Exercise Program Promotes Functional and Psychosocial Health Outcomes in Aged Care. J. Aging Phys. Act. 2020, 28, 104–113. [Google Scholar] [CrossRef]
- Jensen, A. Culture Vitamins—An Arts on Prescription project in Denmark. Perspect. Public Health 2019. [Google Scholar] [CrossRef]
- Alliance for Healthier Communities. Rx: Community—Social Prescribing in Ontario | Alliance for Healthier Communities. Available online: https://www.allianceon.org/Social-Prescribing (accessed on 16 February 2021).
- Whitelaw, S.; Thirlwall, C.; Morrison, A.; Osborne, J.; Tattum, L.; Walker, S. Developing and implementing a social prescribing initiative in primary care: Insights into the possibility of normalisation and sustainability from a UK case study. Prim. Health Care Res. Dev. 2017, 18, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Wildman, J.M.; Moffatt, S.; Steer, M.; Laing, K.; Penn, L.; O’Brien, N. Service-users’ perspectives of link worker social prescribing: A qualitative follow-up study. BMC Public Health 2019, 19, 98. [Google Scholar] [CrossRef]
- Hanlon, P.; Gray, C.M.; Chng, N.R.; Mercer, S.W. Does Self-Determination Theory help explain the impact of social prescribing? A qualitative analysis of patients’ experiences of the Glasgow ‘Deep-End’ Community Links Worker Intervention. Chronic Illn. 2019. [Google Scholar] [CrossRef] [PubMed]
- Bickerdike, L.; Booth, A.; Wilson, P.M.; Farley, K.; Wright, K. Social prescribing: Less rhetoric and more reality. A systematic review of the evidence. BMJ Open 2017, 7, e013384. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, H.J.; Camic, P.M.; Lockyer, B.; Thomson, L.J.M. Non-clinical community interventions: A systematised review of social prescribing schemes. Arts Health 2018, 10, 97–123. [Google Scholar] [CrossRef]
- Reinhardt, G.Y.; Vidovic, D.; Hammerton, C. Understanding loneliness: A systematic review of the impact of social prescribing initiatives on loneliness. Perspect. Public Health 2020. [Google Scholar] [CrossRef]
- Petticrew, M.; Roberts, H. Systematic Reviews in the Social Sciences: A Practical Guide; John Wiley & Sons: Padstow, Cornwall, UK, 2008; ISBN 978-1-4051-5014-9. [Google Scholar]
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Available online: https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000097 (accessed on 27 January 2020).
- HM Government. Our Health, Our Care, Our Say: A New Direction for Community Services. 2006. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/272238/6737.pdf (accessed on 2 February 2021).
- World Health Organization (WHO). WHO | The world Health Report 2000—Health Systems: Improving Performance. Available online: https://www.who.int/whr/2000/en/ (accessed on 24 February 2021).
- World Health Organization (WHO). WHO | World Health Assembly Concludes: Adopts Key Resolutions Affecting Global Public Health. Available online: https://www.who.int/mediacentre/news/releases/2005/pr_wha06/en/ (accessed on 16 November 2020).
- World Health Organization (WHO). Health Agenda for the 21st Century. WHO | Executive Summary. Available online: https://www.who.int/whr/1998/media_centre/executive_summary9/en/ (accessed on 14 January 2021).
- NHS England. FutureNHS Collaboration Platform. Available online: https://future.nhs.uk/index.cfm (accessed on 12 February 2020).
- Dayson, C.; Bennett, E. Evaluation of Doncaster Social Prescribing Service: Understanding Outcomes and Impact. Available online: https://www4.shu.ac.uk/research/cresr/sites/shu.ac.uk/files/eval-doncaster-social-prescribing-service.pdf (accessed on 9 December 2019).
- Jani, A.; Liyanage, H.; Hoang, U.; Moore, L.; Ferreira, F.; Yonova, I.; Brown, V.T.; de Lusignan, S. Use and impact of social prescribing: A mixed-methods feasibility study protocol. BMJ Open 2020, 10, e037681. [Google Scholar] [CrossRef]
- Mercer, S.W.; Fitzpatrick, B.; Grant, L.; Chng, N.R.; McConnachie, A.; Bakhshi, A.; James-Rae, G.; O’Donnell, C.A.; Wyke, S. Effectiveness of Community-Links Practitioners in Areas of High Socioeconomic Deprivation. Ann. Fam. Med. 2019, 17, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Sheffield Hallam University and Sport Industry Research Centre. Dance to Health “Phase 1 Rollout [test and learn]” Evaluation. 2019. Available online: https://ae-sop.org/wp-content/uploads/sites/63/2019/06/SHU-SIRC-1st-report-FINAL.pdf (accessed on 6 October 2020).
- Bird, E.L.; Biddle, M.S.Y.; Powell, J.E. General practice referral of ‘at risk’ populations to community leisure services: Applying the RE-AIM framework to evaluate the impact of a community-based physical activity programme for inactive adults with long-term conditions. BMC Public Health 2019, 19, 1308. [Google Scholar] [CrossRef]
- Grant, C.; Goodenough, T.; Harvey, I.; Hine, C. A randomised controlled trial and economic evaluation of a referrals facilitator between primary care and the voluntary sector. BMJ 2000, 320, 419–423. [Google Scholar] [CrossRef]
- Carnes, D.; Sohanpal, R.; Frostick, C.; Hull, S.; Mathur, R.; Netuveli, G.; Tong, J.; Hutt, P.; Bertotti, M. The impact of a social prescribing service on patients in primary care: A mixed methods evaluation. BMC Health Serv. Res. 2017, 17, 835. [Google Scholar] [CrossRef] [PubMed]
- Bell, A.; Gandy, R.J.; Roe, B. Benefits and impacts of Active Lives groups for older people living in the community. Res. Policy Plan. J. Soc. Serv. Res. Group 2017, 32, 97–112. [Google Scholar]
- Elston, J.; Gradinger, F.; Asthana, S.; Lilley-Woolnough, C.; Wroe, S.; Harman, H.; Byng, R. Does a social prescribing ‘holistic’ link-worker for older people with complex, multimorbidity improve well-being and frailty and reduce health and social care use and costs? A 12-month before-and-after evaluation. Prim. Health Care Res. Dev. 2019, 20, e135. [Google Scholar] [CrossRef]
- Dayson, C.; Bennett, E. Evaluation of the Rotherham Mental Health Social Prescribing Service 2015/16–2016/17. 2017. Available online: https://www4.shu.ac.uk/research/cresr/sites/shu.ac.uk/files/eval-rotherham-mental-health-social-prescribing.pdf (accessed on 6 October 2020).
- Dayson, C.; Damm, C. Evaluation of the Rotherham Social Prescribing Service for Long Term Conditions. Available online: http://shura.shu.ac.uk/27312/2/eval-rotherham-social-prescribing-long-term-conditions-17-18.pdf (accessed on 6 October 2020).
- Woodall, J.; Trigwell, J.; Bunyan, A.-M.; Raine, G.; Eaton, V.; Davis, J.; Hancock, L.; Cunningham, M.; Wilkinson, S. Understanding the effectiveness and mechanisms of a social prescribing service: A mixed method analysis. BMC Health Serv. Res. 2018, 18, 604. [Google Scholar] [CrossRef] [PubMed]
- Kimberlee, R. Gloucestershire Clinical Commissioning Group Social Prescribing Service: Evaluation Report. 2016. Available online: https://future.nhs.uk/connect.ti/socialprescribing/view?objectId=40784069 (accessed on 14 May 2021).
- Wessex Academic Health Science Network (WAHSN) and R-Outcomes. Social Prescribing in Wessex Understanding Its Impact and Supporting Spread. 2017. Available online: https://wessexahsn.org.uk (accessed on 6 October 2020).
- Farenden, C.; Mitch, C.; Feast, S.; Verdenicci, S. Community Navigation in Brighton & Hove Evaluation of a Social Prescribing Pilot. Available online: https://ihub.scot/media/1656/cn-full-evaluation-nov-2015.pdf (accessed on 6 October 2020).
- Vogelpoel, N.; Jarrold, K. Social prescription and the role of participatory arts programmes for older people with sensory impairments. J. Integr. Care 2014, 22, 39–50. [Google Scholar] [CrossRef]
- Pescheny, J.; Pappas, Y.; Randhawa, G. Service user outcomes of a social prescribing programme in general practice. Int. J. Integr. Care 2018, 18, 215. [Google Scholar] [CrossRef]
- Jacob, C.; Roff, K.; Fleet, J.; Jones, J.; Wood, C.A.; Jensen, H.; Allen, S.; Bryan, A.; Romero, D.; Ray, L.; et al. Can volunteers improve thewell-being, participation and activity of patients on an acute older-persons’ unit in hospital? In Proceedings of the British Geriatrics Society Autumn Meeting, Leicester, UK, 6–8 November 2019.
- Envoy Partnership Self-Care Social Prescribing. 2018. Available online: https://www.kcsc.org.uk/sites/kcsc.org.uk/civi_files/files/civicrm/persist/contribute/files/Self%20Care/7641_SROI-Report_DIGITAL_AW.pdf (accessed on 6 October 2020).
- Dayson, C.; Bashir, N. The Social and Economic Impact of the Rotherham Social Prescribing Pilot: Main Evaluation Report. Available online: https://www4.shu.ac.uk/research/cresr/sites/shu.ac.uk/files/social-economic-impact-rotherham.pdf (accessed on 13 February 2020).
- Dayson, C. Evaluating Social Innovations and Their Contribution to Social Value: The Benefits of A “Blended Value” Approach. Available online: https://www.ingentaconnect.com/content/tpp/pap/2017/00000045/00000003/art00006;jsessionid=5ffokecerfpb6.x-ic-live-03 (accessed on 12 February 2020).
- Kimberlee, R.; Ward, R.; Jones, M.; Powell, J. Measuring The Economic Impact of Wellspring Healthy Living Centre’s Social Prescribing Wellbeing Programme for Low Level Mental Health Issues Encountered by GP Services. 2014, p. 111. Available online: http://www.wellspringhlc.org.uk/reports/POV_Final_Report_March_2014.pdf (accessed on 9 December 2019).
- Holt, N.J. Tracking momentary experience in the evaluation of arts-on-prescription services: Using mood changes during art workshops to predict global wellbeing change. Perspect. Public Health 2020, 140, 270–276. [Google Scholar] [CrossRef]
- Waterfall, D. Dudley CVS: Integrated Plus Impact Evaluation. 2019, p. 107. Available online: https://future.nhs.uk/socialprescribing/view?objectId=48482725 (accessed on 9 December 2019).
- Kellezi, B.; Wakefield, J.R.H.; Stevenson, C.; McNamara, N.; Mair, E.; Bowe, M.; Wilson, I.; Halder, M.M. The social cure of social prescribing: A mixed-methods study on the benefits of social connectedness on quality and effectiveness of care provision. BMJ Open 2019, 9, e033137. [Google Scholar] [CrossRef]
- Coop and British Red Cross Tackling-Loneliness-and-Isolation-Connecting-Communities. 2019. Available online: https://www.sheffield.ac.uk/media/6027/download (accessed on 13 February 2020).
- Callaghan, L.; Thompson, T.P.; Creanor, S.; Quinn, C.; Senior, J.; Green, C.; Hawton, A.; Byng, R.; Wallace, G.; Sinclair, J.; et al. Individual health trainers to support health and well-being for people under community supervision in the criminal justice system: The STRENGTHEN pilot RCT. Public Health Res. 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Thomson, L.J.; Morse, N.; Elsden, E.; Chatterjee, H.J. Art, nature and mental health: Assessing the biopsychosocial effects of a “creative green prescription” museum programme involving horticulture, artmaking and collections. Perspect. Public Health 2020, 140, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Dayson, C.; Leather, D. Evaluation of Hale Community Connectors Social Prescribing Service. 2017. Available online: https://www4.shu.ac.uk/research/cresr/sites/shu.ac.uk/files/eval-HALE-community-connectors-social-prescribing.pdf (accessed on 6 October 2020).
- Bolton CVS. Community Asset Navigator Programme: Reach, Progress and Outcomes Report. 2019. Available online: https://www.boltoncvs.org.uk/sites/boltoncvs.org.uk/files/CANs%20Q4%20Report%20-Print.pdf (accessed on 6 October 2020).
- Todd, C.; Camic, P.M.; Lockyer, B.; Thomson, L.J.M.; Chatterjee, H.J. Museum-based programs for socially isolated older adults: Understanding what works. Health Place 2017, 48, 47–55. [Google Scholar] [CrossRef]
- Wilkinson, E.K.; Lees, A.; Weekes, S.; Duncan, G.; Meads, G.; Tapson, K. A collaborative, multi-sectoral approach to implementing a social prescribing initiative to alleviate social isolation and enhance well-being amongst older people. J. Integr. Care 2020, 29, 37–47. [Google Scholar] [CrossRef]
- Leslie, C.; McGill, G.; Kiernan, M.D.; Wilson, G. Social isolation and loneliness of UK veterans: A Delphi study. Occup. Med. Oxf. Engl. 2020, 70, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Moffatt, S.; Steer, M.; Lawson, S.; Penn, L.; O’Brien, N. Link Worker social prescribing to improve health and well-being for people with long-term conditions: Qualitative study of service user perceptions. BMJ Open 2017, 7, e015203. [Google Scholar] [CrossRef] [PubMed]
- Holding, E.; Thompson, J.; Foster, A.; Haywood, A. Connecting communities: A qualitative investigation of the challenges in delivering a national social prescribing service to reduce loneliness. Health Soc. Care Community 2020, 28, 1535–1543. [Google Scholar] [CrossRef]
- Payne, K.; Walton, E.; Burton, C. Steps to benefit from social prescription: A qualitative interview study. Br. J. Gen. Pract. 2020, 70, e36–e44. [Google Scholar] [CrossRef]
- Malyn, B. Reading and Writing for Well-Being: A Qualitative Exploration of the Therapeutic Experience of Older Adult Participants in a Bibliotherapy and Creative Writing Group. 2018. Available online: https://uwe-repository.worktribe.com/output/866482/reading-and-writing-for-well-being-a-qualitative-exploration-of-the-therapeutic-experience-of-older-adult-participants-in-a-bibliotherapy-and-creative-writing-group (accessed on 29 November 2020).
- Alden, S.; Wigfield, A.; Kispeter, E. Age UK’s Cascade Training Programme Evaluation Report. Circ. Cent. Int. Res. Care Labour Equal. Univ. Leeds. 2015, p. 60. Available online: https://www.sheffield.ac.uk/polopoly_fs/1.546406!/file/AgeUKs-Cascade-Training-Programme.pdf (accessed on 9 December 2019).
- Redmond, M.; Sumner, R.C.; Crone, D.M.; Hughes, S. ‘Light in dark places’: Exploring qualitative data from a longitudinal study using creative arts as a form of social prescribing. Arts Health 2018, 11, 232–245. [Google Scholar] [CrossRef] [PubMed]
- Primary Care@Veor. Live Lively ‘What Matters to Me’, Not ‘What is the Matter with ME’. 2019. Available online: https://future.nhs.uk/socialprescribing/view?objectId=40784869 (accessed on 6 October 2020).
- Dayson, C.; Damm, C. The Rotherham Social Prescribing Service for People with Long-term Conditions: Evaluation Update. 2017. Available online: https://www4.shu.ac.uk/research/cresr/sites/shu.ac.uk/files/rotherham-social-prescribing-evaluation-update.pdf (accessed on 6 October 2020).
- The Government’s Response to COVID-19: Human Rights Implications—Committees—UK Parliament. Available online: https://committees.parliament.uk/work/218/the-governments-response-to-covid19-human-rights-implications/ (accessed on 20 April 2020).
- Bu, F.; Steptoe, A.; Fancourt, D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. medRxiv 2020, 186, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Connected Communities. About the Project. May 2021. Available online: https://connected-communities.net/about-us/ (accessed on 13 May 2021).
- Connected Communities Newsletter: November 2020. Available online: http://www.greatglemham.onesuffolk.net/assets/Uploads/November-Connected-Communities-Newsletter.pdf (accessed on 23 February 2021).
- Connected Communities Newsletter: January 2021. Available online: http://greatglemham.onesuffolk.net/assets/Uploads/Jan-2021-CC-newsletter.pdf (accessed on 23 February 2021).
- Younan, H.-C.; Junghans, C.; Harris, M.; Majeed, A.; Gnani, S. Maximising the impact of social prescribing on population health in the era of COVID-19. J. R. Soc. Med. 2020, 113, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social Relationships and Mortality Risk: A Meta-analytic Review. PLoS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Impact Concept | Concept Measure (Number of Studies Utilising the Measure) | Evidence of Change # | Means of Causal Inference ## |
|---|---|---|---|
| Loneliness (14) | UCLA (7) Delphi Method (1) Hawthorne Friendship Scale (1) Scale developed for a study purpose (1) Unspecified measure (4) | 4 [27,37,79,85] † 1 [80] | Serial mediation analysis, Coeff = (−0.23), p = 0.003 [27] † Serial mediation analysis, Coeff = (−0.31), p = 0.0001 [79] † |
| Social Isolation (20) | Conf. with loneliness (3) Conf. with connectedness (1) Interview quotations (2) Thematic analysis (2) Hawthorne Friendship Scale (1) Duke-UNC (1) Adult Social Care/Public Outcome (1) Unspecified measure (9) | 2 [60,66] † 1 [76] | Randomised controlled trial (RCT), non sig. mean between group diff., DUKE-UNC: confidant support (−0.9), p = 0.221) and affective support (−0.3), p = 0.594 [60] † |
| Well-being (42) | WEMWBS (14) ONS4 (2) UCL Museum well-being (2) Scale developed for a study purpose (8) Thematic analysis (4) The Kessler Psychological Distress Scale K10 and The World Health Organization Quality of Life (1) Medical outcome profile (MYMOP) (1) Investigating Choice Experiments for the Preferences of Older People Capability Measure for Adults (ICECAP-A) (1) Unspecified measure (9) | 15 [26,37,38,44,55,57,59,60,61,63,64,65,66,67,68,69,70,71,73,75,76,77,78,80,81,82,83,85] † 13 [26,55,64,65,67,68,69,73,75,76,78,80,83] | Randomised controlled trial (RCT), sig. mean score between group diff. (−1.9), p = 0.002) [60] † Randomised controlled trial (RCT), mean between-group diff., the WEMWBS score at 3-month follow-up 4.6 (−1.7 to 10.8), and 1.9 (95% CI −4.6 to 8.4) at 6 months. [81] † Cluster-RCT, Coeff = (–0.011), p = 0.411 [57] † |
| Connectedness (14) | Thematic analysis (4) Scale developed for a study purpose (2) Adult Social Care/Public Outcome (1) Campaign to End Loneliness (1) Interview quotations (1) Revised UCLA loneliness scale (1) Unspecified measure (4) | 3 [27,79,82] † | Serial mediation analysis, community belonging (Coeff = 0.09, p = 0.01); social support (Coeff = 0.33, p < 0.001) [27] † Serial mediation analysis, Coeff = 0.09, p = 0.01 [79] † |
| Impact Concept | Concept Measure (Number of Studies Utilising the Measure) | Evidence of Change # | Means of Causal Inference ## |
|---|---|---|---|
| Health Care (21) | GP care visits (9) A&E attendance (9) Inpatient admissions (7) Cost savings (5) Outpatient appointments (3) Referral pathways effectiveness (2) Hospital discharge (1) Mental health services discharge (1) Mental health services visits (1) | 7 [60,61,63,66,72,79] † 14 [26,55,58,64,67,68,69,73,74,75,76,78,83,95] | Randomised controlled trial (RCT), no diff. between groups, mean = 4.4 [60] † Serial mediation analysis, Coeff = 1.41, p = 0.002 [79] † |
| Social Care (3) | Contact with social care worker (1) Cost savings (1) Impact on care home services (1) | 1 [63] † 1 [55] |
| Impact Concept | Concept Measure (Number of Studies Utilising the Measure) | Evidence of change * | Means of Causal Inference ## |
|---|---|---|---|
| Community Resources (14) | Societal Return on Investment (SROI) (4) Building capacity in a community (4) VCSE improvements and funding access (3) Increase in usage of community resources: groups, services, activities (1) Increase in the number of community activities and groups available in a community/make services more available (1) Social prescribing volunteers securing paid employment (2) Integrating services and creating infrastructure to support service delivery (2) | 1 [44] † 7 [26,55,58,67,73,76,80] | |
| Community Connectedness (3) | Community belonging (2) Promoting value of social connection (1) | 1 [27,79] 1 [69] | Serial mediation analysis, community belonging Coeff = 0.09, p = 0.01 [79] Serial mediation analysis, community belonging Coeff = 0.09, p = 0.01; social support Coeff = 0.33, p < 0.001 [27] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vidovic, D.; Reinhardt, G.Y.; Hammerton, C. Can Social Prescribing Foster Individual and Community Well-Being? A Systematic Review of the Evidence. Int. J. Environ. Res. Public Health 2021, 18, 5276. https://doi.org/10.3390/ijerph18105276
Vidovic D, Reinhardt GY, Hammerton C. Can Social Prescribing Foster Individual and Community Well-Being? A Systematic Review of the Evidence. International Journal of Environmental Research and Public Health. 2021; 18(10):5276. https://doi.org/10.3390/ijerph18105276
Chicago/Turabian StyleVidovic, Dragana, Gina Yannitell Reinhardt, and Clare Hammerton. 2021. "Can Social Prescribing Foster Individual and Community Well-Being? A Systematic Review of the Evidence" International Journal of Environmental Research and Public Health 18, no. 10: 5276. https://doi.org/10.3390/ijerph18105276
APA StyleVidovic, D., Reinhardt, G. Y., & Hammerton, C. (2021). Can Social Prescribing Foster Individual and Community Well-Being? A Systematic Review of the Evidence. International Journal of Environmental Research and Public Health, 18(10), 5276. https://doi.org/10.3390/ijerph18105276