
Higher 90-Day Mortality after Surgery for Hip Fractures in Patients with COVID-19: A Case–Control Study from a Single Center in Italy

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Case Definition
2.3. Control Definition
2.4. Statistical Analysis
3. Results
3.1. Patient Demographic
3.2. COVID-19 Patients Characteristics
3.3. Case–Control Comparison
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). COVID-19 Dashboard. 2021. Available online: https://coronavirus.jhu.edu/map.html (accessed on 7 May 2021).
- Yanez, N.D.; Weiss, N.S.; Romand, J.A.; Treggiari, M.M. COVID-19 mortality risk for older men and women. BMC Public Health 2020, 20, 1742. [Google Scholar] [CrossRef]
- Mallapaty, S. The coronavirus is most deadly if you are older and male-new data reveal the risks. Nature 2020, 585, 16–17. [Google Scholar] [CrossRef]
- Tarantino, U.; Cariati, I.; Tancredi, V.; Casamassima, D.; Piccirilli, E.; Iundusi, R.; Gasbarra, E. State of Fragility Fractures Management during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7732. [Google Scholar] [CrossRef]
- Macera, M.; De Angelis, G.; Sagnelli, C.; Coppola, N.; Vanvitelli Covid-Group. Clinical Presentation of COVID-19: Case Series and Review of the Literature. Int. J. Environ. Res. Public Health 2020, 17, 5062. [Google Scholar] [CrossRef]
- Beaupre, L.; Khong, H.; Smith, C.; Kang, S.; Evens, L.; Jaiswal, P.; Powell, J. The impact of time to surgery after hip fracture on mortality at 30- and 90-days: Does a single benchmark apply to all? Injury 2019, 50, 950–955. [Google Scholar] [CrossRef] [PubMed]
- Haentjens, P. Meta-analysis: Excess mortality after hip fracture among older women and men. Ann. Intern. Med. 2010, 152, 380–390. [Google Scholar] [CrossRef] [PubMed]
- Hansen, L.; Mathiesen, A.S.; Vestergaard, P.; Ehlers, L.H.; Petersen, K.D. A health economic analysis of osteoporotic fractures: Who carries the burden? Arch. Osteoporos. 2013, 8, 126. [Google Scholar] [CrossRef]
- Canton, G.; Moghnie, A.; Cleva, M.; Kostoris, F.M.; Murena, L. Dual mobility total hip arthroplasty in the treatment of femoral neck fractures: A retrospective evaluation at mid-term follow-up. Acta Biomed. 2019, 90, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Moja, L.; Piatti, A.; Pecoraro, V.; Ricci, C.; Virgili, G.; Salanti, G.; Germagnoli, L.; Liberati, A.; Banfi, G. Timing matters in hip fracture surgery: Patients operated within 48 h have better outcomes. A meta-analysis and meta-regression of over 190,000 patients. PLoS ONE 2012, 7, e46175. [Google Scholar] [CrossRef]
- Braithwaite, R.S.; Col, N.F.; Wong, J.B. Estimating hip fracture morbidity, mortality and costs. J. Am. Geriatr. Soc. 2003, 51, 364–370. [Google Scholar] [CrossRef]
- Pincus, D.; Ravi, B.; Wasserstein, D.; Huang, A.; Paterson, J.M.; Nathens, A.B.; Kreder, H.J.; Jenkinson, R.J.; Wodchis, W.P. Association between wait time and 30-day mortality in adults undergoing hip fracture surgery. J. Am. Med. Assoc. 2017, 318, 1994–2003. [Google Scholar] [CrossRef]
- Moran, C.G.; Wenn, R.T.; Sikand, M.; Taylor, A.M. Early mortality after hip fracture: Is delay before surgery important? J. Bone Jt. Surg. Am. 2005, 87, 483–489. [Google Scholar]
- Menéndez-Colino, R.; Misis, A.G.; Alarcon, T.; Díez-Sebastián, J.; De Bustamante, M.D.; Queipo, R.; Otero, A.; González-Montalvo, J.I. Development of a new comprehensive preoperative risk score for predicting 1-year mortality in patients with hip fracture: The HULP-HF score. Comparison with 3 other risk prediction models. HIP Int. 2020. Epub ahead of print. [Google Scholar] [CrossRef]
- Clement, N.D.; Ng, N.; Simpson, C.J.; Patton, R.F.L.; Hall, A.J.; Simpson, A.H.R.W.; Duckworth, A.D. The prevalence, mortality, and associated risk factors for developing COVID-19 in hip fracture patients: A systematic review and meta-analysis. Bone Jt. Res. 2020, 9, 873–883. [Google Scholar] [CrossRef]
- Clement, N.D.; Hall, A.J.; Makaram, N.S.; Robinson, P.G.; Patton, R.F.L.; Moran, M.; MacPherson, G.J.; Duckworth, A.D.; Jenkins, P.J. IMPACT-Restart: The influence of COVID-19 on postoperative mortality and risk factors associated with SARS-CoV-2 infection after orthopaedic and trauma surgery. Bone Jt. J. 2020, 102, 1774–1781. [Google Scholar] [CrossRef]
- Haj Bloukh, S.; Edis, Z.; Shaikh, A.A.; Pathan, H.M. A Look Behind the Scenes at COVID-19: National Strategies of Infection Control and Their Impact on Mortality. Int. J. Environ. Res. Public Health 2020, 17, 5616. [Google Scholar] [CrossRef]
- Cross, M.; Ng, S.K.; Scuffham, P. Trading Health for Wealth: The Effect of COVID-19 Response Stringency. Int. J. Environ. Res. Public Health 2020, 17, 8725. [Google Scholar] [CrossRef] [PubMed]
- Benazzo, F.; Rossi, S.M.P.; Maniscalco, P.; Moretti, B.; Vaienti, E.; Ruggieri, P.; Massè, A.; Medici, A.; Formica, A.; Di Maggio, B.; et al. The orthopaedic and traumatology scenario during Covid-19 outbreak in Italy: Chronicles of a silent war. Int. Orthop. 2020, 44, 1453–1459. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; Lidgren, L.; Bottinelli, E.; Villafañe, J.H.; Berjano, P.; Banfi, G.; Romanò, C.L.; Sculco, T.P. Mapping of 303 Microbiological Procedures by the Members of the International Society of Orthopaedic Centers (ISOC) for Diagnosis of Periprosthetic Infections. J. Clin. Microbiol. 2016, 54, 1402–1403. [Google Scholar] [CrossRef]
- Chinese Clinical Guidance for COVID-19 Pneumonia Diagnosis and Treatment. Available online: https://www.acc.org/latest-in-cardiology/articles/2020/03/17/11/22/chinese-clinical-guidance-for-covid-19-pneumonia-diagnosis-and-treatment (accessed on 7 May 2021).
- WHO Reference Number: WHO/COVID-19/laboratory/2020.5. Available online: https://mca.essensys.ro/publications/m/item/molecular-assays-to-diagnose-covid-19-summary-table-of-available-protocols (accessed on 7 May 2021).
- Menendez, M.E.; Neuhaus, V.; van Dijk, N.C.; Ring, D. The Elixhauser Comorbidity Method Outperforms the Charlson Index in Predicting Inpatient Death after Orthopaedic Surgery. Clin. Orthop. Relat. Res. 2014, 472, 2878–2886. [Google Scholar] [CrossRef] [PubMed]
- Miguel, A.; Hernán, M.A. The hazards of hazard ratios. Epidemiology 2010, 21, 13–15. [Google Scholar] [CrossRef]
- Hirschmann, M.T.; Hart, A.; Henckel, J.; Sadoghi, P.; Seil, R.; Mouton, C. COVID-19 coronavirus: Recommended personal protective equipment for the orthopaedic and trauma surgeon. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 1690–1698. [Google Scholar] [CrossRef]
- Karia, M.; Gupta, V.; Zahra, W.; Dixon, J.; Tayton, E. The effect of COVID-19 on the trauma burden, theatre efficiency and training opportunities in a district general hospital: Planning for a future outbreak. Bone Jt. Open. 2020, 1, 494–499. [Google Scholar] [CrossRef]
- Catellani, F.; Coscione, A.; D’Ambrosi, R.; Usai, L.; Roscitano, C.; Fiorentino, G. Treatment of Proximal Femoral Fragility Fractures in Patients with COVID-19 during the SARS-CoV-2 Outbreak in Northern Italy. J. Bone Jt. Surg. Am. 2020, 17, e58. [Google Scholar] [CrossRef]
- Maestre-Muñiz, M.M.; Arias, Á.; Arias-González, L.; Angulo-Lara, B.; Lucendo, A.J. Prognostic Factors at Admission for In-Hospital Mortality from COVID-19 Infection in an Older Rural Population in Central Spain. J. Clin. Med. 2021, 16, 318. [Google Scholar] [CrossRef]
- Maniscalco, P.; Poggiali, E.; Quattrini, F. Proximal femur fractures in COVID-19 emergency: The experience of two Orthopedics and Traumatology Departments in the first eight weeks of the Italian epidemic. Acta Biomed. 2020, 91, 89–96. [Google Scholar] [CrossRef]
- Kayani, B.; Onochie, E.; Patil, V.; Begum, F.; Cuthbert, R.; Ferguson, D.; Bhamra, J.S.; Sharma, A.; Bates, P.; Haddad, F.S. The effects of COVID-19 on perioperative morbidity and mortality in patients with hip fractures. Bone Jt. J. 2020, 102, 1136–1145. [Google Scholar] [CrossRef]
- Hall, A.J.; Clement, N.D.; MacLullich, A.M.J.; White, T.O.; Duckworth, A.D. IMPACT-Scot 2 report on COVID-19 in hip fracture patients. Bone Jt. J. 2021, 25, 1–10. [Google Scholar] [CrossRef]
- Wang, K.C.; Xiao, R.; Cheung, Z.B.; Barbera, J.P.; Forsh, D.A. Early mortality after hip fracture surgery in COVID-19 patients: A systematic review and meta-analysis. J. Orthop. 2020, 22, 584–591. [Google Scholar] [CrossRef]
- Citizens of the Metropolitan City of Bologna, Capital of the Emilia Romagna Region in Italy. Available online: https://statistica.regione.emilia-romagna.it/servizi-online/statistica-self-service/popolazione/popolazione-residente-dal-1861 (accessed on 7 May 2021).
- Tedesco, D.; Gibertoni, D.; Rucci, P.; Hernandez-Boussard, T.; Rosa, S.; Bianciardi, L.; Rolli, M.; Fantini, M.P. Impact of rehabilitation on mortality and readmissions after surgery for hip fracture. BMC Health Serv. Res. 2018, 18, 701. [Google Scholar] [CrossRef]
- Italian Health Ministry Report. Available online: https://www.epicentro.iss.it/coronavirus/bollettino/Report-COVID-2019_18_giugno.pdf (accessed on 7 May 2021).
- D’Ascanio, M.; Innammorato, M.; Pasquariello, L.; Pizzirusso, D.; Guerrieri, G.; Castelli, S.; Pezzuto, A.; De Vitis, C.; Anibaldi, P.; Marcolongo, A.; et al. Age is not the only risk factor in COVID-19: The role of comorbidities and of long staying in residential care homes. BMC Geriatr. 2021, 21, 63. [Google Scholar] [CrossRef]
- Grasselli, G.; Greco, M.; Zanella, A. COVID-19 Lombardy ICU Network. Risk Factors Associated with Mortality among Patients with COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Lohia, P.; Kapur, S.; Benjaram, S.; Pandey, A.; Mir, T.; Seyoum, B. Metabolic Syndrome and clinical outcomes in patients infected with COVID-19: Does age, sex and race of the patient with Metabolic Syndrome matter? J. Diabetes 2021, 13, 420–429. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Lim, M.A.; Pranata, R. Coronavirus disease 2019 (COVID-19) markedly increased mortality in patients with hip fracture—A systematic review and meta-analysis. J. Clin. Orthop. Trauma 2020. Epub ahead of print. [Google Scholar] [CrossRef]
- Vives, J.M.M.; Jornet-Gibert, M.; Cámara-Cabrera, J.; Esteban, P.L.; Brunet, L.; Delgado-Flores, L.; Camacho-Carrasco, P.; Torner, P.; Marcano-Fernández, F. Mortality Rates of Patients with Proximal Femoral Fracture in a Worldwide Pandemic: Preliminary Results of the Spanish HIP-COVID Observational Study. J. Bone Jt. Surg. Am. 2020, 102, e69. [Google Scholar] [CrossRef]
- Grassi, A.; Pizza, N.; Tedesco, D.; Zaffagnini, S. The COVID-19 outbreak in Italy: Perspectives from an orthopaedic hospital. Int. Orthop. 2020, 44, 1543–1547. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables Types | Variables | COVID-19 (n = 14) | Non-COVID-19 (n = 42) | p-Value |
|---|---|---|---|---|
| Matching variables | Sex; n (%) | 13 (93%), F | 39 (93%), F | >0.05 |
| 1 (7%), M | 3 (7%), M | |||
| Age; mean (SD), year | 82.9 (7.1) | 83.1 (6.6) | >0.05 | |
| ECI; n (%), comorbidities | 5 (36%), 0–1 | 15 (36%), 0–1 | >0.05 | |
| 9 (64%), ≥2 | 27 (64%), ≥2 | |||
| ICD-9-CM; n (%), code | 1 (7%), 79.15 | 3 (7%), 79.15 | >0.05 | |
| 6 (43%), 79.35 | 18 (43%), 79.35 | |||
| 2 (14%), 81.51 | 6 (4%), 81.51 | |||
| 5 (36%), 81.52 | 15 (36%), 81.52 | |||
| Descriptive variables | Diagnosis; n (%) | 7 (50%) femoral neck fractures | 21 (50%) femoral neck fractures | 1.000 |
| 7 (50%) intertrochanteric fractures | 21 (50%) intertrochanteric fractures | |||
| Procedure; n (%) | 5 (36%) hip endoprosthesis | 14 (33%) hip endoprosthesis | 0.856 | |
| 6 (43%) intramedullary femoral nail | 20 (47%) intramedullary femoral nail | |||
| 2 (14%) THA | 7 (17%) THA | |||
| 1 (7%) ORIF | 1 (3%) ORIF | |||
| Surgery time; mean (SD), minutes | 67.6 (25.0) | 69.0 (20.2) | 0.844 | |
| ASA; n (%) | 12 (86%) ASA 3 | 37 (88%) ASA 3 | 0.943 | |
| 1 (7%) ASA 4 | 2 (5%) ASA 4 | |||
| 1 (7%) ASA 2 | 3 (7%) ASA 2 | |||
| Fracture–surgery interval; mean (SD), days | 3.2 (2.4) | 2.8 (2.4) | 0.584 | |
| Admission–surgery interval; mean (SD), days | 2.7 (2.6) | 1.9 (1.5) | 0.168 | |
| Smokers; n (%) | 4 (29%) | 9 (21%) | 0.415 |
| Main Comorbidity | COVID-19 (n = 14) | Non-COVID-19 (n = 42) | p-Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Cardiac arrhythmia | 6 | 42.9% | 8 | 19.0% | 0.080 |
| Chronic pulmonary disease | 4 | 28.6% | 3 | 7.1% | 0.058 |
| Hypertension uncomplicated | 3 | 21.4% | 16 | 38.1% | 0.210 |
| Dementia | 3 | 21.4% | 11 | 26.2% | 0.512 |
| Congestive heart failure | 2 | 14.3% | 6 | 14.3% | 0.651 |
| Solid tumor without metastasis | 1 | 7.1% | 7 | 16.7% | 0.349 |
| Diabetes uncomplicated | 1 | 7.1% | 4 | 9.5% | 0.633 |
| Depression | 1 | 7.1% | 4 | 9.5% | 0.633 |
| Hypothyroidism | 1 | 7.1% | 3 | 7.1% | 0.695 |
| Fluid and electrolyte disorders | 1 | 7.1% | 2 | 4.8% | 0.586 |
| Diabetes complicated | 1 | 7.1% | 0 | 0.0% | 0.250 |
| Liver disease | 1 | 7.1% | 0 | 0.0% | 0.250 |
| Deficiency anemia | 1 | 7.1% | 0 | 0.0% | 0.250 |
| Other neurological disorders | 0 | 0.0% | 6 | 14.3% | 0.162 |
| Valvular disease | 0 | 0.0% | 5 | 11.9% | 0.223 |
| Renal failure | 0 | 0.0% | 3 | 7.1% | 0.414 |
| Blood loss anemia | 0 | 0.0% | 3 | 7.1% | 0.414 |
| Hypertension complicated | 0 | 0.0% | 3 | 7.1% | 0.414 |
| Metastatic cancer | 0 | 0.0% | 1 | 2.4% | 0.750 |
| Rheumatoid arthritis/collagen | 0 | 0.0% | 1 | 2.4% | 0.750 |
| Obesity | 0 | 0.0% | 1 | 2.4% | 0.750 |
| Peripheral vascular disorders | 0 | 0.0% | 1 | 2.4% | 0.750 |
| Patient | ASA | Comorbidities | Orthopedic Diagnosis and Treatment | Admission–Surgery Interval | Length of Hospitalization | COVID-19 Diagnosis | Timing of Diagnosis | Clinical Symptoms | Laboratory Test Alterations | ABG Results | HRCT | Treatment | Exitus |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F, 90 y | II | HT, CHD, K | Femoral neck fracture Hip endoprosthesis | 1 day | 9 | Positive RT-PCR molecular test | Admission | Fever for 5 days | LC: Y; LP: N; LyP: N; PLT: 227; C: 0.73; IL-6: NA; LDH: NA; PCR: 15 | NA | NEG | O2, LMWH, Antibiotic | no |
| F, 81 y | III | HT, COPD, D | Femoral neck fracture THA | 1 day | 22 | Positive RT-PCR molecular test | 22 days | Asymptomatic | LC: Y; LP: N; LyP: N; PLT: 400; C: 1.6; IL-6: NA; LDH: NA; PCR: 1.6 | NA | NEG | LMWH, Antibiotic | no |
| F, 90 y | II | HT, DM, CHD | Intertrochanteric fracture Femoral intramedullary nail | 1 day | 10 | Positive RT-PCR molecular test | 11 days | Asymptomatic | LC: N; LP: N; LyP: N; PLT: 265; C: 0.58; IL-6: NA; LDH: NA; PCR: 5.9 | SaO2: 93; PaO2: 52; PaCO2: 34; PF: 267 | NEG | LMWH | no |
| F, 73 y | III | HT, COPD, K | Femoral neck fracture THA | 2 days | 8 | Positive RT-PCR molecular test | Admission | Fever for 3 days Cough Desaturation | LC: Y; LP: N; LyP: Y; PLT: 248; C: 0.74; IL-6: NA; LDH: 336; PCR: 3.7 | SaO2: 96; PaO2: 60; PaCO2: 33; PF: 286 | NEG | O2, CPAP, HCQ, LMWH | no |
| F, 70 y | III | K | Intertrochanteric fracture Femoral intramedullary nail | 2 days | 11 | Clinical criteria | 2 days | Desaturation | LC: Y; LP: N; LyP: N; PLT: 420; C: 0.53; IL-6: NA; LDH: 232; PCR: 1.6 | SaO2: 91; PaO2: 80; PaCO2: 23; PF: 857 | POS | O2, HCQ, AZA, LMWH, Antibiotic | no |
| F, 72 y | III | HT, COPD | Femoral neck fracture Hip endoprosthesis | 8 days | 14 | Positive RT-PCR molecular test | 11 days | Asymptomatic | LC: N; LP: N; LyP: N; PLT: 87; C: 1.27; IL-6: NA; LDH: 228; PCR: 24 | NA | NEG | LMWH, Antibiotic | no |
| F, 86 y | IV | HT, D, K | Intertrochanteric fracture Femoral intramedullary nail | 3 days | 8 | Positive RT-PCR molecular test | Admission | Fever Cough | LC: N; LP: N; LyP: Y; PLT: 260; C: 0.85; IL-6: 66.6; LDH: NA; PCR: 4.6 | SaO2: 98; PaO2: 69; PaCO2: 32; PF: 328 | POS | O2, HCQ, AZA, LMWH, Antibiotic | no |
| F, 80 y | III | HT, S, COPD, D | Femoral neck fracture Hip endoprosthesis | 2 days | 11 | Positive RT-PCR molecular test | 2 days | Asymptomatic | LC: N; LP: N; LyP: N; PLT: 123; C: 0.89; IL-6: NA; LDH: NA; PCR: 5.6 | SaO2: 91; PaO2: 68; PaCO2: 45; PF: 283 | NEG | O2, HCQ, LMWH | no |
| F, 86 y | III | HT | Intertrochanteric fracture Femoral intramedullary nail | 1 day | 8 | Positive RT-PCR molecular test | Admission | Asymptomatic | LC: N; LP: N; LyP: N; PLT: 278; C: 0.64; IL-6: NA; LDH: NA; PCR: NA | SaO2: 98; PaO2: 94; PaCO2: 34; PF: 448 | NEG | HCQ, LMWH | no |
| F, 90 y | IV | HT, COPD, D, K | Femoral neck fracture Hip endoprosthesis | 7 days | 10 | Positive RT-PCR molecular test | Admission | Cough | LC: N; LP: N; LyP: Y; PLT: 368; C: 0.53; IL-6: NA; LDH: NA; PCR: NA | SaO2: 98; PaO2: 71;PaCO2: 44; PF: 371 | NEG | O2, LMWH | Yes (14-day postop) |
| F, 89 y | III | DM, CHD, COPD, D | Intertrochanteric fracture Femoral intramedullary nail | 1 day | 7 | Positive RT-PCR molecular test | 8 days | Asymptomatic | LC: N; LP: N; LyP: N; PLT: 272; C: 0.73; IL-6: NA; LDH: NA; PCR: 5.6 | NA | NEG | LMWH | Yes (33-day postop) |
| F, 87 y | IV | CHD, COPD, D | Intertrochanteric fracture Femoral intramedullary nail | 9 days | 10 | Clinical criteria | 2 days | Fever for 3 days | LC: Y; LP: N; LyP: Y; PLT: 189; C: 0.69; IL-6: NA; LDH: 379; PCR: 26 | SaO2: 83; PaO2: 48; PaCO2: 68; PF: 229 | POS | O2, CPAP, HCQ, AZA, LMWH, Antibiotic | Yes (1-day postop) |
| F, 88 y | III | HT, DM, CHD, D, K | Femoral neck fracture Hip endoprosthesis | 1 day | 10 | Positive RT-PCR molecular test | 4 days | Dyspnea for 6 days | LC: N; LP: N; LyP: Y; PLT: 186; C: 1.20; IL-6: NA; LDH: NA; PCR: 8 | SaO2: 86; PaO2: 44; PaCO2: 31; PF: 210 | NEG | O2, LMWH | Yes (9-day postop) |
| M, 79 y | III | COPD, D | Femoral neck fracture ORIF | 0 days | 21 | Clinical criteria | 10 days | Fever for 11 days Dyspnea Desaturation | LC: Y; LP: N; LyP: Y; PLT: 300; C: 1.6; IL-6: 78; LDH: NA; PCR: 40 | SaO2: 80; PaO2: 53; PaCO2: 31; PF: 252 | POS | O2, CPAP, LMWH, Antibiotic | Yes (21-day postop) |
| Time Points and Outcome Measures | Mortality Rates and Risk Measures | |||||
|---|---|---|---|---|---|---|
| 7-Day | 14-Day | 30-Day | 45-Day | 90-Day | ||
| Mortality rate | COVID-19 Positive | |||||
| Time from Admission | 0.0% | 14.3% | 28.6% | 35.7% | 35.7% | |
| Time from Surgery | 7.1% | 21.4% | 28.6% | 35.7% | 35.7% | |
| Time from COVID-19 Diagnosis | 7.1% | 21.4% | 35.7% | 35.7% | 35.7% | |
| Control Group | ||||||
| Admission | 2.4% | 2.4% | 7.1% | 9.5% | 9.5% | |
| Surgery | 2.4% | 2.4% | 7.1% | 9.5% | 9.5% | |
| 7-day | 14-day | 30-day | 45-day | 90-day | ||
| Risk Measures | Hazard Ratios | |||||
| Value | 3.1 | 9.6 | 4.5 | 4.5 | 4.5 | |
| 95% CI | 0.12–78.0 | 0.9–95.6 | 1.0–20.2 | 1.2–16.7 | 1.2–16.7 | |
| p-Value | =0.3972 | =0.0766 | =0.0490 * | =0.0250 * | =0.0250 * | |
| Odds Ratios | ||||||
| Value | 3.1 | 11.2 | 5.2 | 5.2 | 5.2 | |
| 95% CI | 0.2–54.0 | 1.1–119.3 | 1.0–27.1 | 1.2–23.7 | 1.2–23.7 | |
| p-Value | =0.4281 | =0.0449 * | =0.0502 | =0.0300 * | =0.0300 * | |
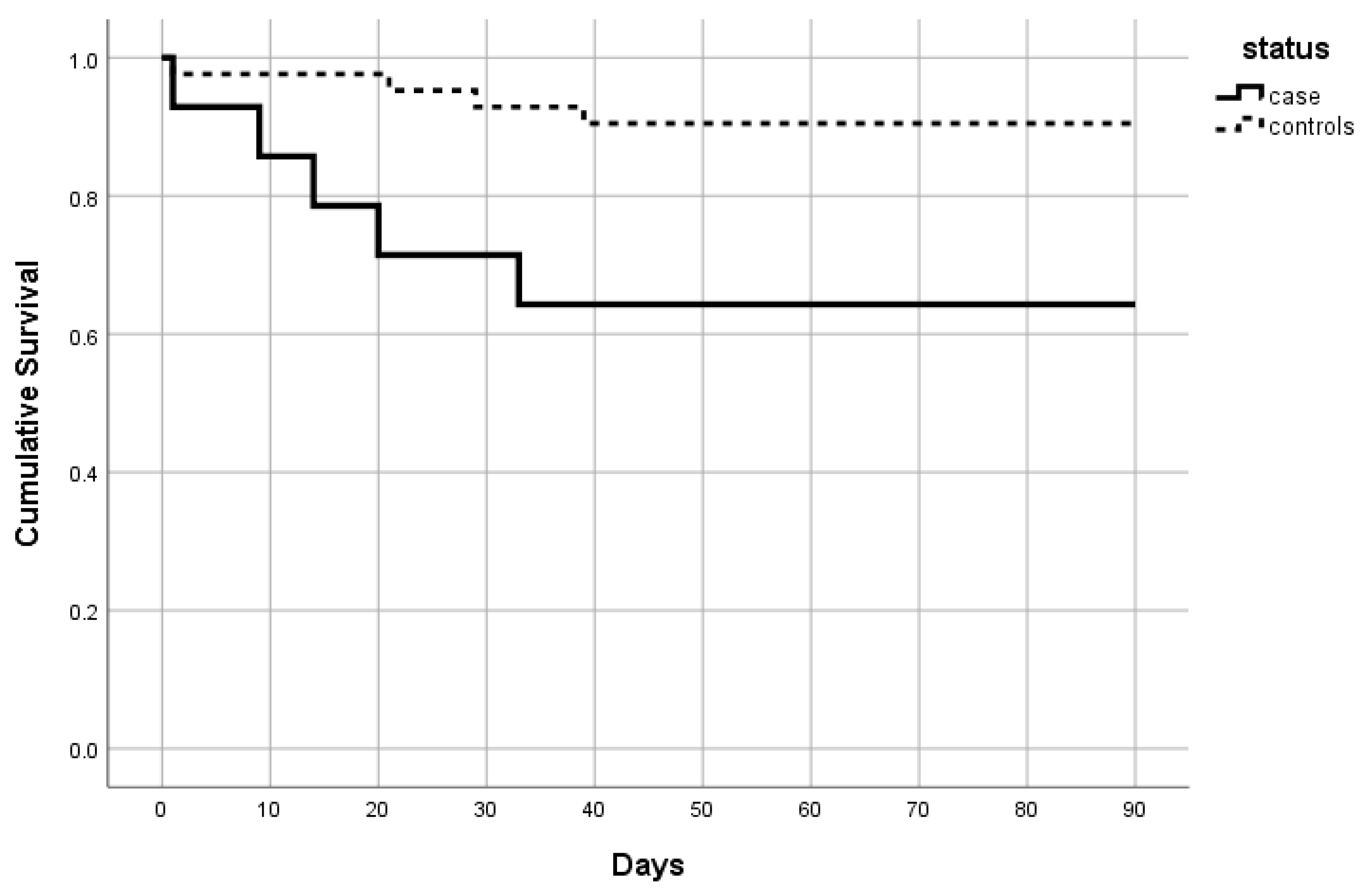
| 90-Day Survival | Patients’ Characteristics | COVID-19 Cases (n = 14) | Controls (n = 42) |
|---|---|---|---|
| Alive (%) | 9 (64.3) | 38 (90.5) | |
| Mean age (SD) | 80.8 (7.7) | 82.5 (6.6) | |
| Female (%) | 9 (100) | 35 (92.1) | |
| Mean ECI (SD) | 1.7 (1.5) | 2.1 (1.9) | |
| Deceased (%) | 5 (35.7) | 4 (9.5) | |
| Mean age (±SD) | 86.6 (4.4) | 89.0 (1.4) | |
| Female (%) | 4 (80) | 4 (100) | |
| Mean ECI (SD) | 2.2 (1.1) | 1.5 (1.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grassi, A.; Andriolo, L.; Golinelli, D.; Tedesco, D.; Rosa, S.; Gramegna, P.; Ciaffi, J.; Meliconi, R.; Landini, M.P.; Filardo, G.; et al. Higher 90-Day Mortality after Surgery for Hip Fractures in Patients with COVID-19: A Case–Control Study from a Single Center in Italy. Int. J. Environ. Res. Public Health 2021, 18, 5205. https://doi.org/10.3390/ijerph18105205
Grassi A, Andriolo L, Golinelli D, Tedesco D, Rosa S, Gramegna P, Ciaffi J, Meliconi R, Landini MP, Filardo G, et al. Higher 90-Day Mortality after Surgery for Hip Fractures in Patients with COVID-19: A Case–Control Study from a Single Center in Italy. International Journal of Environmental Research and Public Health. 2021; 18(10):5205. https://doi.org/10.3390/ijerph18105205
Chicago/Turabian StyleGrassi, Alberto, Luca Andriolo, Davide Golinelli, Dario Tedesco, Simona Rosa, Pasquale Gramegna, Jacopo Ciaffi, Riccardo Meliconi, Maria Paola Landini, Giuseppe Filardo, and et al. 2021. "Higher 90-Day Mortality after Surgery for Hip Fractures in Patients with COVID-19: A Case–Control Study from a Single Center in Italy" International Journal of Environmental Research and Public Health 18, no. 10: 5205. https://doi.org/10.3390/ijerph18105205
APA StyleGrassi, A., Andriolo, L., Golinelli, D., Tedesco, D., Rosa, S., Gramegna, P., Ciaffi, J., Meliconi, R., Landini, M. P., Filardo, G., Fantini, M. P., & Zaffagnini, S. (2021). Higher 90-Day Mortality after Surgery for Hip Fractures in Patients with COVID-19: A Case–Control Study from a Single Center in Italy. International Journal of Environmental Research and Public Health, 18(10), 5205. https://doi.org/10.3390/ijerph18105205