
Systematic Review on Outbreaks of SARS-CoV-2 on Cruise, Navy and Cargo Ships

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Question and Objectives
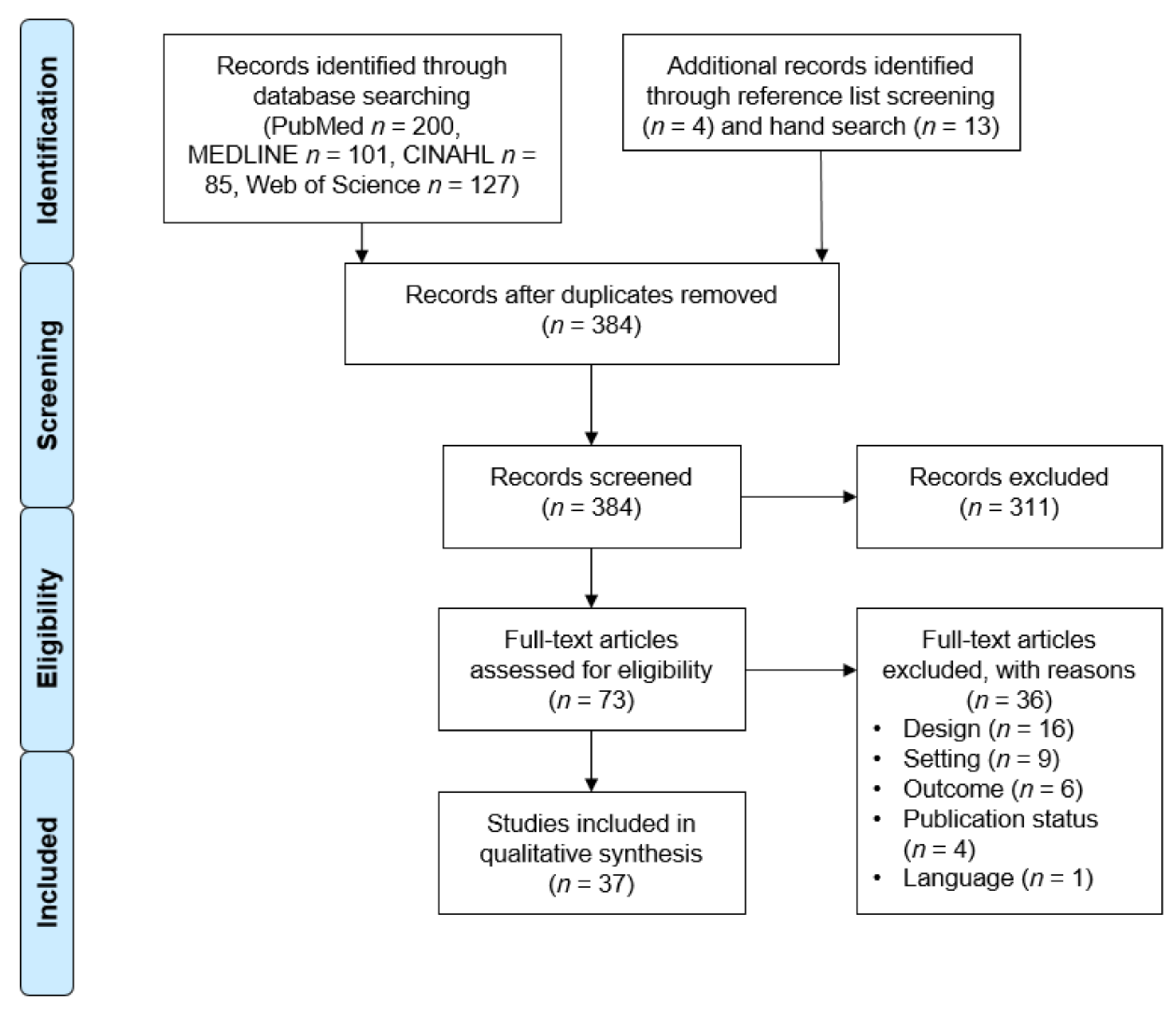
2.2. Search Strategy and Identification of Relevant Studies
2.3. Study Selection
2.4. Data Extraction and Analysis
3. Results
3.1. Study Characteristcs
3.2. COVID-19 on Cruise Ships
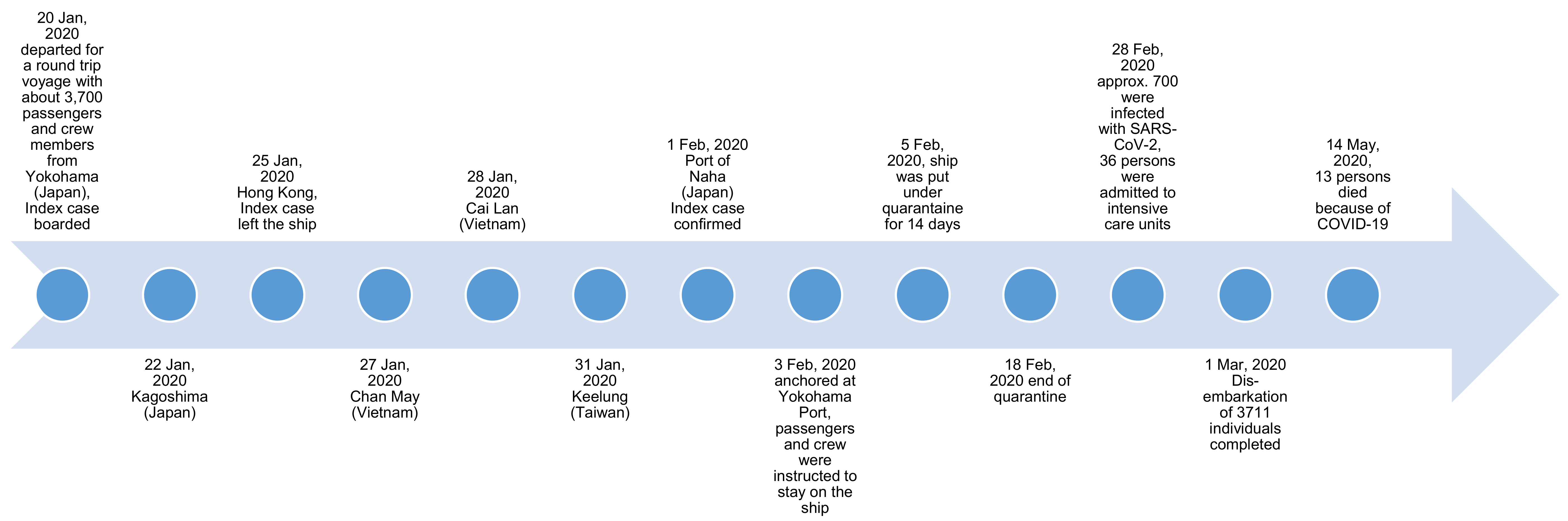
3.2.1. Diamond Princess
Course of the Outbreak
Analysis of Asymptomatic and Symptomatic Cases
Mathematical Modelling
Medical Transport
3.2.2. Grand Princess
3.2.3. MS Westerdam
3.2.4. Nile River Cruises
3.3. COVID-19 on Navy Vessels
3.4. COVID-19 on Cargo Ships
3.5. Problems Related to Identified Outbreaks on Ships Sailing Worldwide
4. Discussion
4.1. Identified Outbreaks on Cruise Ships Sailing Worldwide
4.2. Identified Outbreaks on Navy Vessels Sailing Worldwide
4.3. Identified Outbreaks on Cargo Ships Sailing Worldwide
4.4. Recommendations
4.4.1. Recommendations for Cruise Ships
4.4.2. Recommendations for Cargo and Navy Ships
4.4.3. Recommendations on Mental Health
4.4.4. Recommendations on Training Practices
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Robert Koch-Institut. Die Internationalen Gesundheitsvorschriften der Weltgesundheitsorganisation. Available online: https://www.rki.de/DE/Content/Infekt/IGV/igv_node.html#doc2391006bodyText8 (accessed on 16 July 2020).
- Cruise Lines International Association (CLIA). State of the Cruise Industry Outlook. Available online: https://cruising.org/-/media/research-updates/research/2021-state-of-the-cruise-industry_optimized.ashx (accessed on 3 March 2021).
- Statista. Anzahl der Passagiere auf dem Europäischen Kreuzfahrtmarkt von 2001 bis 2019. Available online: https://de.statista.com/statistik/daten/studie/217087/umfrage/kreuzfahrtpassagiere-in-europa/ (accessed on 5 May 2021).
- Cruise Lines International Association (CLIA). Cruise Trends and Industry Outlook. 2019. Available online: https://cruising.org/-/media/research-updates/research/clia-2019-state-of-the-industry-presentation-(1).pdf (accessed on 16 July 2020).
- Mouchtouri, V.A.; Nichols, G.; Rachiotis, G.; Kremastinou, J.; Arvanitoyannis, I.S.; Riemer, T.; Jaremin, B.; Hadjichristodoulou, C. State of the art: Public health and passenger ships. Int. Marit. Health 2010, 61, 49–98. [Google Scholar] [PubMed]
- Cramer, E.H.; Slaten, D.D.; Guerreiro, A.; Robbins, D.; Ganzon, A. Management and control of varicella on cruise ships: A collaborative approach to promoting public health. J. Travel Med. 2012, 19, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Statista. Containertransportmenge in der weltweiten Seeschifffahrt von 2015 bis 2023 (in Millionen TEU). Available online: https://de.statista.com/statistik/daten/studie/259570/umfrage/containertransportmenge-weltweit/ (accessed on 3 March 2021).
- United Nations Conference on Trade and Development (UNCTAD). Review of Maritime Transport; United Nations: Geneva, Switzerland, 2020. [Google Scholar]
- Chimonas, M.A.R.; Vaughan, G.H.; Andre, Z.; Ames, J.T.; Tarling, G.A.; Beard, S.; Widdowson, M.A.; Cramer, E. Passenger behaviors associated with norovirus infection on board a cruise ship-Alaska, May to June 2004. J. Travel Med. 2008, 15, 177–183. [Google Scholar] [CrossRef]
- Qi, L.; Xiang, X.Z.; Xiong, Y.; Ling, H.; Shen, H.C.; Deng, W.W.; Tang, W.G.; Shen, T.; Li, Q. Outbreak of Acute Gastroenteritis Caused by Norovirus Genogroup II Attributed to Contaminated Cold Dishes on a Cruise Ship in Chongqing, China, 2017. Int. J. Environ. Res. Public Health 2018, 15, 2823. [Google Scholar] [CrossRef] [PubMed]
- Verhoef, L.; Boxman, I.L.; Duizer, E.; Rutjes, S.A.; Vennema, H.; Friesema, I.H.; de Roda Husman, A.M.; Koopmans, M. Multiple exposures during a norovirus outbreak on a river-cruise sailing through Europe, 2006. Euro Surveill. 2008, 13, 12. [Google Scholar] [CrossRef]
- Vivancos, R.; Keenan, A.; Sopwith, W.; Smith, K.; Quigley, C.; Mutton, K.; Dardamissis, E.; Nichols, G.; Harris, J.; Gallimore, C.; et al. Norovirus outbreak in a cruise ship sailing around the British Isles: Investigation and multi-agency management of an international outbreak. J. Infect. 2010, 60, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Wikswo, M.E.; Cortes, J.; Hall, A.J.; Vaughan, G.; Howard, C.; Gregoricus, N.; Cramer, E.H. Disease Transmission and Passenger Behaviors during a High Morbidity Norovirus Outbreak on a Cruise Ship, January 2009. Clin. Infect. Dis. 2011, 52, 1116–1122. [Google Scholar] [CrossRef]
- Verhoef, L.; Depoortere, E.; Boxman, I.L.; Duizer, E.; van Duynhoven, Y.; Harris, J.; Johnsen, C.; Kroneman, A.; Le Guyader, S.; Lim, W.; et al. Emergence of new norovirus variants on spring cruise ships and prediction of winter epidemics. Emerg. Infect. Dis. 2008, 14, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Brotherton, J.M.; Delpech, V.C.; Gilbert, G.L.; Hatzi, S.; Paraskevopoulos, P.D.; McAnulty, J.M. A large outbreak of influenza A and B on a cruise ship causing widespread morbidity. Epidemiol. Infect. 2003, 130, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Dill, C.E.; Favata, M.A. Novel influenza A (H1N1) outbreak on board a US navy vessel. Disaster Med. Public Health Prep. 2009, 3 Suppl. S2, 117–120. [Google Scholar] [CrossRef]
- Fernandes, E.G.; de Souza, P.B.; de Oliveira, M.E.; Lima, G.D.; Pellini, A.C.; Ribeiro, M.C.; Sato, H.K.; Ribeiro, A.F.; Yu, A.L. Influenza B outbreak on a cruise ship off the Sao Paulo Coast, Brazil. J. Travel Med. 2014, 21, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Tarabbo, M.; Lapa, D.; Castilletti, C.; Tommaselli, P.; Guarducci, R.; Luca, G.; Emanuele, A.; Zaccaria, O.; La Gioia, V.F.; Girardi, E.; et al. Retrospective investigation of an influenza A/H1N1pdm outbreak in an Italian military ship cruising in the Mediterranean Sea, May–September 2009. PLoS ONE 2011, 6, e15933. [Google Scholar] [CrossRef] [PubMed]
- Ward, K.A.; Armstrong, P.; McAnulty, J.M.; Iwasenko, J.M.; Dwyer, D.E. Outbreaks of pandemic (H1N1) 2009 and seasonal influenza A (H3N2) on cruise ship. Emerg. Infect. Dis. 2010, 16, 1731–1737. [Google Scholar] [CrossRef]
- Acevedo, F.; Diskin, A.L.; Dahl, E. Varicella at sea: A two-year study on cruise ships. Int. Marit. Health 2011, 62, 254–261. [Google Scholar]
- Lanini, S.; Capobianchi, M.R.; Puro, V.; Filia, A.; Del Manso, M.; Karki, T.; Nicoletti, L.; Magurano, F.; Derrough, T.; Severi, E.; et al. Measles outbreak on a cruise ship in the western Mediterranean, preliminary report. Euro Surveill. 2014, 19, 20735. [Google Scholar] [PubMed]
- Mitruka, K.; Felsen, C.B.; Tomianovic, D.; Inman, B.; Street, K.; Yambor, P.; Reef, S.E. Measles, rubella, and varicella among the crew of a cruise ship sailing from Florida, United States 2006. J. Travel Med. 2012, 19, 233–237. [Google Scholar] [CrossRef]
- Farr, W.; Gonzalez, M.J.; Garbauskas, H.; Zinderman, C.E.; LaMar, J.E. Suspected meningococcal meningitis on an aircraft carrier. Mil. Med. 2004, 169, 684–686. [Google Scholar] [CrossRef] [PubMed][Green Version]
- ProMED mail. Meningitis, Meningococcal—Italy: Cruise Ship, Exposure, Archive Number: 20121009.1333637. 2012. [Google Scholar]
- Bogoch, I.I.; Watts, A.; Thomas-Bachli, A.; Huber, C.; Kraemer, M.U.G.; Khan, K. Potential for global spread of a novel coronavirus from China. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Zhao, S.; Zhuang, Z.; Cao, P.; Ran, J.; Gao, D.; Lou, Y.; Yang, L.; Cai, Y.; Wang, W.; He, D.; et al. Quantifying the association between domestic travel and the exportation of novel coronavirus (2019-nCoV) cases from Wuhan, China in 2020: A correlational analysis. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef]
- Robert Koch-Institut. Epidemiologischer Steckbrief zu SARS-CoV-2 und COVID-19. Stand: 8 January 2021. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Steckbrief.html;jsessionid=D94FD261A8E816F3EA13A0F9500C4EF7.internet101?nn=13490888 (accessed on 14 January 2021).
- Potere, N.; Valeriani, E.; Candeloro, M.; Tana, M.; Porreca, E.; Abbate, A.; Spoto, S.; Rutjes, A.W.; Di Nisio, M. Acute complications and mortality in hospitalized patients with coronavirus disease 2019: A systematic review and meta-analysis. Crit. Care 2020, 24, 389. [Google Scholar] [CrossRef] [PubMed]
- Bundeszentrale für gesundheitliche Aufklärung. Mutation des Coronavirus SARS-CoV-2. Available online: https://www.infektionsschutz.de/coronavirus/basisinformationen/mutation-des-coronavirus-sars-cov-2.html (accessed on 16 April 2021).
- Robert Koch-Institut. Informationen zu neuen SARS-CoV-2-Virusvarianten aus Großbritannien und Südafrika. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Virusvariante_Grossbritannien.html (accessed on 14 January 2021).
- World Health Organization (WHO). The Effects of Virus Variants on COVID-19 Vaccines. Available online: https://www.who.int/news-room/feature-stories/detail/the-effects-of-virus-variants-on-covid-19-vaccines (accessed on 16 April 2021).
- Röcklöv, J.; Sjödin, H.; Wilder-Smith, A. COVID-19 outbreak on the Diamond Princess cruise ship: Estimating the epidemic potential and effectiveness of public health countermeasures. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services; Centers for Disease Control and Prevention (CDC). Order Under Sections 361 & 365 Of the Public Health Service Act (42 U.S.C. 264, 268) And Part 70 (Interstate) And Part 71 (Foreign). In Modification and Extension of No Sail Order and Other Measures Related to Operations; Centers for Disease Control and Prevention (CDC): Washington, DC, USA, 2020. [Google Scholar]
- World Health Organization (WHO). Handbook for Management of Public Health Events on Board Ships; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Khan, K.S.; Kunz, R.; Kleijnen, J.; Antes, G. Five steps to conducting a systematic review. J. R. Soc. Med. 2003, 96, 118–121. [Google Scholar] [CrossRef]
- Mouchtouri, V.A.; Lewis, H.C.; Hadjichristodoulou, C.; the EU SHIPSAN ACT Joint Action Partnership. A Systematic Review for Vaccine-Preventable Diseases on Ships: Evidence for Cross-Border Transmission and for Pre-Employment Immunization Need. Int. J. Environ. Res. Public Health 2019, 16, 2713. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Inui, S.; Fuhjikawa, A.; Jitsu, M.; Kunishima, N.; Watanabe, S.; Suzuki, Y.; Umeda, S.; Uwabe, Y. Chest CT Findings in Cases from the Cruise Ship “Diamond Princess” with Coronavirus Disease 2019 (COVID-19). J. Thorac. Imaging 2020, 2, e200110. [Google Scholar] [CrossRef] [PubMed]
- Jimi, H.; Hashimoto, G. Challenges of COVID-19 outbreak on the cruise ship Diamond Princess docked at Yokohama, Japan: A real-world story. Glob. Health Med. 2020, 2, 63–65. [Google Scholar] [CrossRef]
- Kakimoto, K.; Kamiya, H.; Yamagishi, T.; Matsui, T.; Suzuki, M.; Wakita, T. Initial Investigation of Transmission of COVID-19 Among Crew Members During Quarantine of a Cruise Ship—Yokohama, Japan, February 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 312–313. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, L.F.; Plucinski, M.M.; Marston, B.J.; Kurbatova, E.V.; Knust, B.; Murray, E.L.; Pesik, N.; Rose, D.; Fitter, D.; Kobayashi, M.; et al. Public Health Responses to COVID-19 Outbreaks on Cruise Ships—Worldwide, February–March 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, E.; Ino, H.; Akabayashi, A. Chronology of COVID-19 Cases on the Diamond Princess Cruise Ship and Ethical Considerations: A Report from Japan. Disaster Med. Public Health Prep. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Plucinski, M.M.; Wallace, M.; Uehara, A.; Kurbatova, E.V.; Tobolowsky, F.A.; Schneider, Z.D.; Ishizumi, A.; Bozio, C.H.; Kobayashi, M.; Toda, M.; et al. COVID-19 in Americans aboard the Diamond Princess cruise ship. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Tabata, S.; Imai, K.; Kawano, S.; Ikeda, M.; Kodama, T.; Miyoshi, K.; Obinata, H.; Mimura, S.; Kodera, T.; Kitagaki, M.; et al. Clinical characteristics of COVID-19 in 104 people with SARS-CoV-2 infection on the Diamond Princess cruise ship: A retrospective analysis. Lancet Infect. Dis. 2020, 20, 1043–1050. [Google Scholar] [CrossRef]
- Yamagishi, T.; Kamiya, H.; Kakimoto, K.; Suzuki, M.; Wakita, T. Descriptive study of COVID-19 outbreak among passengers and crew on Diamond Princess cruise ship, Yokohama Port, Japan, 20 January to 9 February 2020. Euro Surveill. 2020, 25, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Yamahata, Y.; Shibata, A. Preparation for Quarantine on the Cruise Ship Diamond Princess in Japan due to COVID-19. JMIR Public Health Surveill. 2020, 6, e18821. [Google Scholar] [CrossRef]
- Expert Taskforce for the COVID-19 Cruise Ship Outbreak, Epidemiology of COVID-19 Outbreak on Cruise Ship Quarantined at Yokohama, Japan, February 2020. Emerg. Infect. Dis. 2020, 26, 2591–2597. [CrossRef] [PubMed]
- National Institute of Infectious Diseases (NIID). Field Briefing: Diamond Cases; National Institute of Infectious Diseases (NIID): Tokio, Japan, 2020.
- Arashiro, T.; Nakamura, S.; Asami, T.; Mikuni, H.; Fujiwara, E.; Sakamoto, S.; Miura, R.; Shionoya, Y.; Honda, R.; Furukawa, K.; et al. SARS-CoV-2 and Legionella co-infection in a person returning from a Nile cruise. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- Leung, W.S.; Chan, J.M.C.; Chik, T.S.H.; Lau, D.P.L.; Choi, C.Y.C.; Lau, A.W.T.; Tsang, O.T.Y. Presumed COVID-19 index case on diamond princess cruise ship and evacuees to Hong Kong. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, Y.; Sasaki, H.; Horiuchi, H.; Miyata, N.; Tachikawa, N. Clinical characteristics of the coronavirus disease 2019 (COVID-19) outbreak on a cruise ship. J. Infect. Chemother. 2020, 26, 1177–1180. [Google Scholar] [CrossRef] [PubMed]
- Salducci, M.; La Torre, G. COVID-19 emergency in the cruise’s ship: A case report of conjunctivitis. Clin. Ter. 2020, 171, e189–e191. [Google Scholar]
- Kato, H.; Shimizu, H.; Shibue, Y.; Hosoda, T.; Iwabuchi, K.; Nagamine, K.; Saito, H.; Sawada, R.; Oishi, T.; Tsukiji, J.; et al. Clinical course of 2019 novel coronavirus disease (COVID-19) in individuals present during the outbreak on the Diamond Princess cruise ship. J. Infect. Chemother. 2020, 26, 865–869. [Google Scholar] [CrossRef]
- Sekizuka, T.; Itokawa, K.; Kageyama, T.; Saito, S.; Takayama, I.; Asanuma, H.; Nao, N.; Tanaka, R.; Hashino, M.; Takahashi, T.; et al. Haplotype networks of SARS-CoV-2 infections in the Diamond Princess cruise ship outbreak. Proc. Natl. Acad. Sci. USA 2020, 117, 20198–20201. [Google Scholar] [CrossRef] [PubMed]
- Hung, I.F.-N.; Chi-Chung Cheng, V.; Li, X.; Tam, A.R.; Hung, D.L.-L.; Hei-Yeung Chiu, K.; Chik-Yan Yip, C.; Cai, J.-P.; Tip-Yin Ho, D.; Wong, S.-C.; et al. SARS-CoV-2 shedding and seroconversion among passengers quarantined after disembarking a cruise ship: A case series. Lancet Infect. Dis. 2020, 2020, 1051–1060. [Google Scholar] [CrossRef]
- Miyamae, Y.; Hayashi, T.; Yonezawa, H.; Fujihara, J.; Matsumoto, Y.; Ito, T.; Tsubota, T.; Ishii, K. Duration of viral shedding in asymptomatic or mild cases of novel coronavirus disease 2019 (COVID-19) from a cruise ship: A single-hospital experience in Tokyo, Japan. Int. J. Infect. Dis. 2020, 97, 293–295. [Google Scholar] [CrossRef]
- Emery, J.C.; Russel, T.W.; Liu, Y.; Hellewell, J.; Pearson, C.A.B.; CMMID Covid-Working Group; Knight, G.M.; Eggo, R.M.; Kucharski, A.J.; Funk, S.; et al. The contribution of asymptomatic SARS-CoV-2 infections to transmission on the Diamond Princess cruise ship. Elife 2020, 9, e58699. [Google Scholar] [CrossRef]
- Liu, S.F.; Kuo, N.Y.; Kuo, H.C. Three Taiwan’s domestic family cluster infections of coronavirus disease 2019. J. Med Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Euro Surveill. 2020, 25. [Google Scholar] [CrossRef]
- Nishiura, H.; Kobayashi, T.; Yang, Y.C.; Hayashi, K.; Miyama, T.; Kinoshita, R.; Linton, N.M.; Jung, S.M.; Yuan, B.; Suzuki, A.; et al. The Rate of Underascertainment of Novel Coronavirus (2019-nCoV) Infection: Estimation Using Japanese Passengers Data on Evacuation Flights. Clin. Med. 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Diao, M.; Yu, W.; Pei, L.; Lin, Z.; Chen, D. Estimation of the reproductive number of novel coronavirus (COVID-19) and the probable outbreak size on the Diamond Princess cruise ship: A data-driven analysis. Int. J. Infect. Dis. 2020, 93, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, K.; Chowell, G. Transmission potential of the novel coronavirus (COVID-19) onboard the diamond Princess Cruises Ship, 2020. Infect. Dis. Model 2020, 5, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Anan, H.; Kondo, H.; Takeuchi, I.; Nakamori, T.; Ikeda, Y.; Akasaka, O.; Koido, Y. Medical Transport for 769 COVID-19 Patients on a Cruise Ship by Japan Disaster Medical Assistance Team. Disaster Med. Public Health Prep. 2020, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Arashiro, T.; Furukawa, K.; Nakamura, A. COVID-19 in 2 Persons with Mild Upper Respiratory Tract Symptoms on a Cruise Ship, Japan. Emerg. Infect. Dis. 2020, 26, 1345–1348. [Google Scholar] [CrossRef]
- Jorden, M.A.; Rudman, S.L.; Villarino, E.; Hoferka, S.; Patel, M.T.; Bemis, K.; Simmons, C.R.; Jespersen, M.; Iberg Johnson, J.; Mytty, E.; et al. Evidence for Limited Early Spread of COVID-19 Within the United States, January-February 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 680–684. [Google Scholar]
- Sekizuka, T.; Kuramoto, S.; Nariai, E.; Taira, M.; Hachisu, Y.; Tokaji, A.; Shinohara, M.; Kishimoto, T.; Itokawa, K.; Kobayashi, Y.; et al. SARS-CoV-2 Genome Analysis of Japanese Travelers in Nile River Cruise. Front. Microbiol. 2020, 11. [Google Scholar] [CrossRef]
- Schuchat, A. Public Health Response to the Initiation and Spread of Pandemic COVID-19 in the United States, February 24-April 21, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Palafox, N.A.; Best, B.R.; Hixon, A.; Alik, W.C. Viewpoint: Pacific Voyages-Ships-Pacific Communities: A Framework for COVID-19 Prevention and Control. Hawaii J. Health Soc. Welf. 2020, 79 (Suppl. S2), 120–123. [Google Scholar]
- Payne, D.C.; Smith-Jeffcoat, S.E.; Nowak, G.; Chukwuma, U.; Geibe, J.R.; Hawkins, R.J.; Johnson, J.A.; Thornburg, N.J.; Schiffer, J.; Weiner, Z.; et al. SARS-CoV-2 Infections and Serologic Responses from a Sample of U.S. Navy Service Members—USS Theodore Roosevelt, April 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, G.R.; Pierson, B.C.; Teemer, E.S.; Gama, H.J.; Cole, R.D.; Jang, S.S. Symptom Characterization and Outcomes of Sailors in Isolation After a COVID-19 Outbreak on a US Aircraft Carrier. Jama 2020, 3, e2020981. [Google Scholar] [CrossRef]
- Dai, Q.; Hu, S.; Yan, K.; Chen, Z.; Chen, B.; Cai, T.; Zhang, S.; Zhang, J.; Zheng, J. Reflection on SARS-CoV-2 infection of container ship seafarers. Travel Med. Infect. Dis. 2020, 36, 101787. [Google Scholar] [CrossRef] [PubMed]
- COVID-19, Australia. Epidemiology Report 19 (Fortnightly reporting period ending 21 June 2020). Commun. Dis. Intell. 2018 2020, 44. [Google Scholar] [CrossRef]
- Draper, A.D.; Dempsey, K.E.; Boyd, R.H.; Childs, E.M.; Black, H.M.; Francis, L.A.; Markey, P.G.; Krause, V.L. The first 2 months of COVID-19 contact tracing in the Northern Territory of Australia, March-April 2020. Commun. Dis. Intell. (2018) 2020, 44. [Google Scholar] [CrossRef] [PubMed]
- Dahl, E. Coronavirus (Covid-19) outbreak on the cruise ship Diamond Princess. Int. Marit. Health 2020, 71, 5–8. [Google Scholar] [CrossRef]
- Sawano, T.; Ozaki, A.; Rodriguez-Morales, A.J.; Tanimoto, T.; Sah, R. Limiting spread of COVID-19 from cruise ships: Lessons to be learnt from Japan. QJM Int. J. Med. 2020, 113, 309–310. [Google Scholar] [CrossRef] [PubMed]
- Buitrago-Garcia, D.; Egli-Gany, D.; Counotte, M.J.; Hossmann, S.; Imeri, H.; Ipceki, A.M.; Salanti, G.; Low, N. Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: A living systematic review and meta-analysis. PLoS Med 2020, 17. [Google Scholar] [CrossRef]
- European Centre for Disease and Control (ECDC). COVID-19: EU Guidance for Cruise Ship Operations. Guidance on the Gradual and Safe Resumption of Operations of Cruise Ships in the European Union Relation to the COVID-19 Pandemic. Date: 27 July 2020; European Maritime Safety Agency (EMSA): Lisbon, Portugal, 2020. [Google Scholar]
- Healthy GateWays. Interim Guidance for Preparedness and Response to Cases of COVID-19 at Points of Entry in the European Union (EU)/ EEA Member States (MS). Interim Advice for Restarting Cruise Ship Operations after Lifting Restrictive Measures in Response to the COVID-19 Pandemic. Version 1. 30 June 2020, Version 1 ed. 2020. Available online: https://www.healthygateways.eu/Portals/0/plcdocs/EU_HEALTHY_GATEWAYS_COVID-19_RESTARTING_CRUISES.pdf?ver=2020-07-08-131911-653 (accessed on 16 April 2021).
- World Health Organization (WHO). Operational Considerations for Managing COVID-19 Cases or Outbreaks on Board Ships. Interim Guidance; WHO/2019-nCoV/Ships/2020.2; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Zhang, X.; Wang, C. Prevention and Control of COVID-19 Pandemic on International Cruise Ships: The Legal Controversies. Healthcare 2021, 9, 281. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease and Control (ECDC). Heating, ventilation and air-conditioning systems in the context of COVID-19: First update. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Heating-ventilation-air-conditioning-systems-in-the-context-of-COVID-19-first-update.pdf (accessed on 16 April 2021).
- Speake, H.; Phillips, A.; Chong, T.; Sikazwe, C.; Levy, A.; Lang, J.; Scalley, B.; Speers, D.J.; Smith, D.W.; Effler, P.; et al. Flight-associated transmission of severe acute respiratory syndrome coronavirus 2 corroborated by whole-genome sequencing. Emerg. Infect. Dis. 2020, 26, 2872–2880. [Google Scholar] [CrossRef] [PubMed]
- Cruise Industry News. World Dream Turned Away from Taiwan Due to Coronavirus Concern. Available online: https://www.cruiseindustrynews.com/cruise-news/22386-world-dream-turned-away-from-taiwan-due-to-coronavirus-concern.html (accessed on 16 December 2020).
- Tagesschau. Coronavirus auf Schiff. Trump will im Fall “Zaandam” Vermitteln. Available online: https://www.tagesschau.de/ausland/usa-kreuzfahrtschiff-zaandam-103.html (accessed on 16 December 2020).
- Prime Minister of Australia. Coronavirus Measures Endorsed by National Cabinet; Department of the Prime Minister and Cabinet: Canberra, Australia, 2020.
- Doumbia-Henry, C. Shipping and COVID-19: Protecting seafarers as frontline workers. WMU J. Marit. Aff. 2020, 19, 279–293. [Google Scholar] [CrossRef]
- World Health Organization (WHO). International Health Regulations (IHR), 3rd ed.; WHO Library Cataloguing-in-Publication Data: Geneva, Switzerland, 2005. [Google Scholar]
- Kasper, M.R.; Geibe, J.R.; Sears, C.L.; Riegodedios, A.J.; Luse, T.; Von Thun, A.M.; McGinnis, M.B.; Olson, N.; Houskamp, D.; Fenequito, R.; et al. An Outbreak of Covid-19 on an Aircraft Carrier. N. Engl. J. Med. 2020, 2417–2426. [Google Scholar] [CrossRef]
- Letizia, A.G.; Ramos, I.; Obla, A.; Goforth, C.; Weir, D.L.; Ge, Y.; Bamman, M.M.; Dutta, J.; Ellis, E.; Estrella, L.; et al. SARS-CoV-2 Transmission among Marine Recruits during Quarantine. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- von Münster, T.; Kleine-Kampmann, S.; Hewelt, E.; Boldt, M.; Schlaich, C.; Strölin, P.; Oldenburg, M.; Dirksen-Fischer, M.; Harth, V. When the ship comes in–COVID-19-Ausbrüche an Bord von Frachtschiffen im Hamburger Hafen. Flugmed. Trop. Reisemedizin FTR 2021, 28, 13–24. [Google Scholar]
- Fernandes, E.G.; Santos, J.D.S.; Sato, H.K. Outbreak investigation in cargo ship in times of COVID-19 crisis, Port of Santos, Brazil. Rev. Saude Publica 2020, 54, 34. [Google Scholar] [CrossRef]
- ICAO-ILO-IMO. A Joint Statement on Designation of Seafarers, Marine Personnel, Fishing Vessel Personnel, Offshore Energy Sector Personnel, Aviation Personnel, Air Cargo Supply Chain Personnel, and Service Provider Personnel at Airports and Ports as Key Workers, and on Facilitation of Crew Changes in Ports and Airports in the Context of the COVID-19 Pandemic. Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_dialogue/---sector/documents/genericdocument/wcms_745870.pdf (accessed on 16 December 2020).
- World Health Organization (WHO). Promoting Public Health Measures in Response to COVID-19 on Cargo Ships and Fishing Vessels. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Non-passenger_ships-2020.1 (accessed on 16 April 2021).
- Stannard, S. COVID-19 in the maritime setting: The challenges, regulations and the international response. Int. Marit. Health 2020, 71, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R. Viking becomes the first cruise line to install PCR testing lab on a ship. Available online: https://www.cruiseandferry.net/articles/viking-becomes-the-first-cruise-line-to-install-pcr-testing-lab-on-a-ship (accessed on 3 March 2021).
- Centers for Disease Control and Prevention (CDC). Technical Instructions for Mitigation of COVID-19 Among Cruise Ship Crew. Available online: https://www.cdc.gov/quarantine/cruise/management/technical-instructions-for-cruise-ships.html (accessed on 3 March 2021).
- Dinnes, J.; Deeks, J.J.; Adriano, A.; Berhane, S.; Davenport, C.; Dittrich, S.; Emperador, D.; Takwoingi, Y.; Cunningham, J.; Beese, S.; et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst. Rev. 2020, 8. [Google Scholar] [CrossRef]
- Arbeitsschutzausschüsse beim BMAS. SARS-CoV-2-Arbeitsschutzregel. Available online: https://www.baua.de/DE/Angebote/Rechtstexte-und-Technische-Regeln/Regelwerk/AR-CoV-2/pdf/AR-CoV-2.pdf?__blob=publicationFile&v=6 (accessed on 16 April 2021).
- Battineni, G.; Sagaro, G.G.; Chintalapudi, N.; Di Canio, M.; Amenta, F. Assessment of Awareness and Knowledge on Novel Coronavirus (COVID-19) Pandemic among Seafarers. Healthcare 2021, 9, 120. [Google Scholar] [CrossRef] [PubMed]
- International Maritime Organization. Industry recommended framework of protocols for ensuring safe ship crew changes and travel during the coronavirus (COVID-19) pandemic. Available online: https://wwwcdn.imo.org/localresources/en/MediaCentre/HotTopics/Documents/MSC%201636%20protocols/MSC.1-Circ.1636%20-%20Industry%20Recommended%20Framework%20Of%20Protocols%20For%20Ensuring%20Safe%20Ship%20Crew%20Changes%20And%20Travel.pdf (accessed on 21 April 2021).
- International Chamber of Shipping. Coronavirus (COVID-19). Guidance for Ship Operators for the Protection of the Health of Seafarers. Available online: https://www.ics-shipping.org/wp-content/uploads/2020/11/covid19-guidance-for-ship-operators-for-the-protection-of-the-health-of-seafarers-v3-min.pdf (accessed on 16 April 2021).
- Deutsche Flagge. Funkärztliche Beratung. Available online: https://www.deutsche-flagge.de/de/maritime-medizin/funkaerztliche-beratung (accessed on 16 December 2020).
- Kleine-Kampmann, S.; Schöll, M.; Ehlers, L.; Hewelt, E.; Götsch, U.; Göbels, K.; Ippisch, S.; Seidel, J.; Thanheiser, M.; Schindler, B.; et al. Air and maritime transport during the COVID-19 pandemic in Germany: Challenges for the public health service. Bundesgesundheitsblatt Gesundh. Gesundh. 2021, 64, 454–462. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Seemannsmission, e.V. DSM.Care–Seelsorge Online. Available online: https://www.seemannsmission.org/index.php?option=com_content&view=article&id=1302:deutsche-seemannsmission-bietet-online-hilfe-fur-seeleute&catid=32:newsblog&Itemid=70&lang=de (accessed on 17 December 2020).
- Institut für Hygiene und Umwelt der Behörde für Gesundheit und Verbraucherschutz; Hamburg Port Health Center-Hafen-und Flughafenärztlicher Dienst. ARMIHN–Adaptives Resilienz Management im Hafen. Available online: https://armihn.de/ (accessed on 3 March 2021).



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Population on board of ships sailing worldwide | No reference to maritime context |
| Exposure | SARS-CoV-2 | Exposure to other pathogens |
| Outcome | Reports of seroprevalences of SARS-CoV-2 antibodies or clinically/laboratory confirmed cases or outbreaks of SARS-CoV-2 infections on board ships | No confirmed SARS-CoV-2 infections on board. |
| n | % | |
|---|---|---|
| Country of port called | ||
| Japan | 27 | 69.2 |
| U.S.A | 5 | 12.8 |
| Egypt | 3 | 7.7 |
| Cambodia | 1 | 2.6 |
| China | 1 | 2.6 |
| unknown | 2 | 5.1 |
| Setting | ||
| Cruise ship | 33 | 89.2 |
| Navy vessel | 3 | 8.1 |
| Cargo ship | 1 | 2.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kordsmeyer, A.-C.; Mojtahedzadeh, N.; Heidrich, J.; Militzer, K.; von Münster, T.; Belz, L.; Jensen, H.-J.; Bakir, S.; Henning, E.; Heuser, J.; et al. Systematic Review on Outbreaks of SARS-CoV-2 on Cruise, Navy and Cargo Ships. Int. J. Environ. Res. Public Health 2021, 18, 5195. https://doi.org/10.3390/ijerph18105195
Kordsmeyer A-C, Mojtahedzadeh N, Heidrich J, Militzer K, von Münster T, Belz L, Jensen H-J, Bakir S, Henning E, Heuser J, et al. Systematic Review on Outbreaks of SARS-CoV-2 on Cruise, Navy and Cargo Ships. International Journal of Environmental Research and Public Health. 2021; 18(10):5195. https://doi.org/10.3390/ijerph18105195
Chicago/Turabian StyleKordsmeyer, Ann-Christin, Natascha Mojtahedzadeh, Jan Heidrich, Kristina Militzer, Thomas von Münster, Lukas Belz, Hans-Joachim Jensen, Sinan Bakir, Esther Henning, Julian Heuser, and et al. 2021. "Systematic Review on Outbreaks of SARS-CoV-2 on Cruise, Navy and Cargo Ships" International Journal of Environmental Research and Public Health 18, no. 10: 5195. https://doi.org/10.3390/ijerph18105195
APA StyleKordsmeyer, A.-C., Mojtahedzadeh, N., Heidrich, J., Militzer, K., von Münster, T., Belz, L., Jensen, H.-J., Bakir, S., Henning, E., Heuser, J., Klein, A., Sproessel, N., Ekkernkamp, A., Ehlers, L., de Boer, J., Kleine-Kampmann, S., Dirksen-Fischer, M., Plenge-Bönig, A., Harth, V., & Oldenburg, M. (2021). Systematic Review on Outbreaks of SARS-CoV-2 on Cruise, Navy and Cargo Ships. International Journal of Environmental Research and Public Health, 18(10), 5195. https://doi.org/10.3390/ijerph18105195