
Increased Risk of Sub-Clinical Blood Lead Levels in the 20-County Metro Atlanta, Georgia Area—A Laboratory Surveillance-Based Study

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population and Variables
2.3. Spatial Analyses
2.4. Data Analyses
3. Results
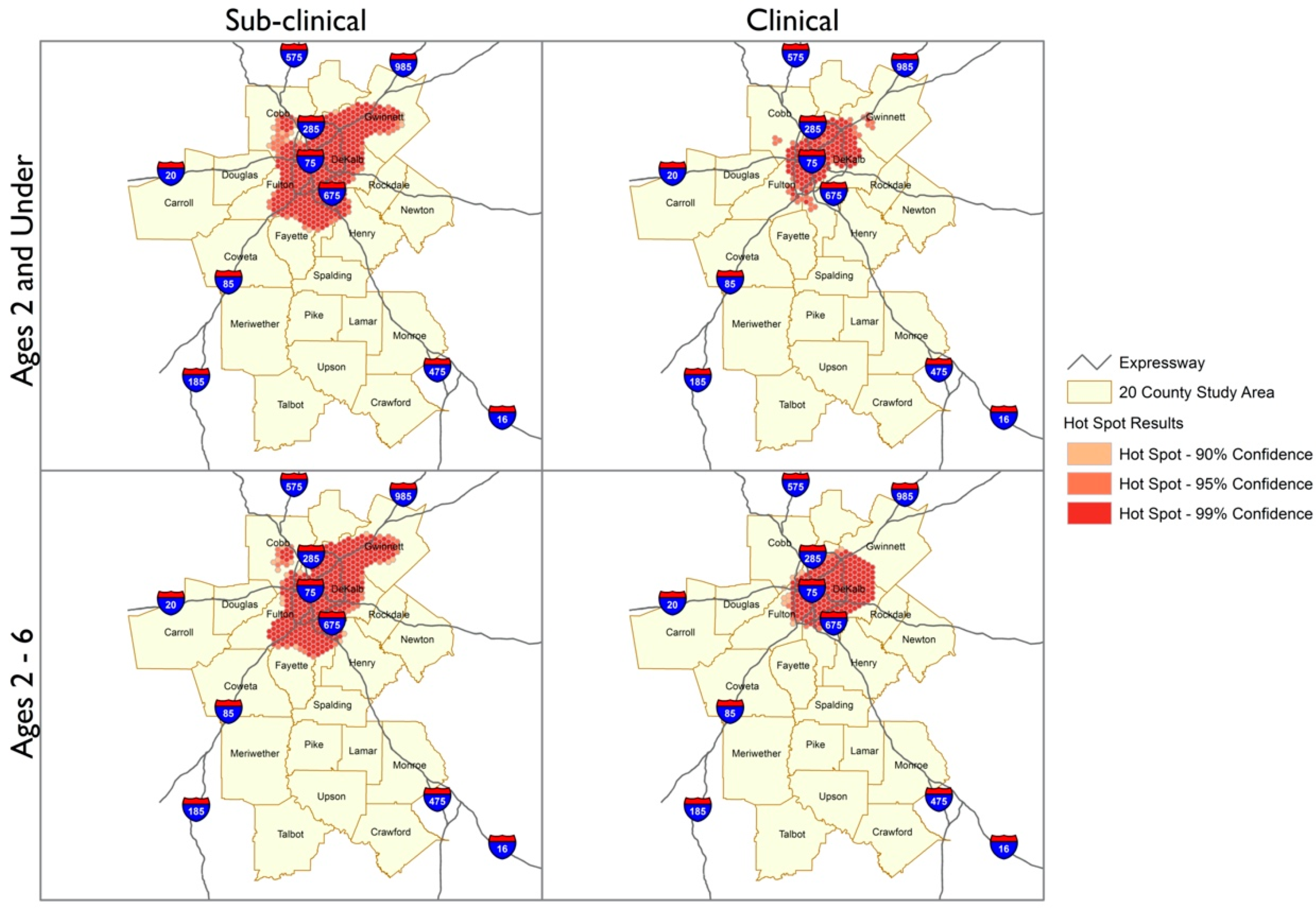
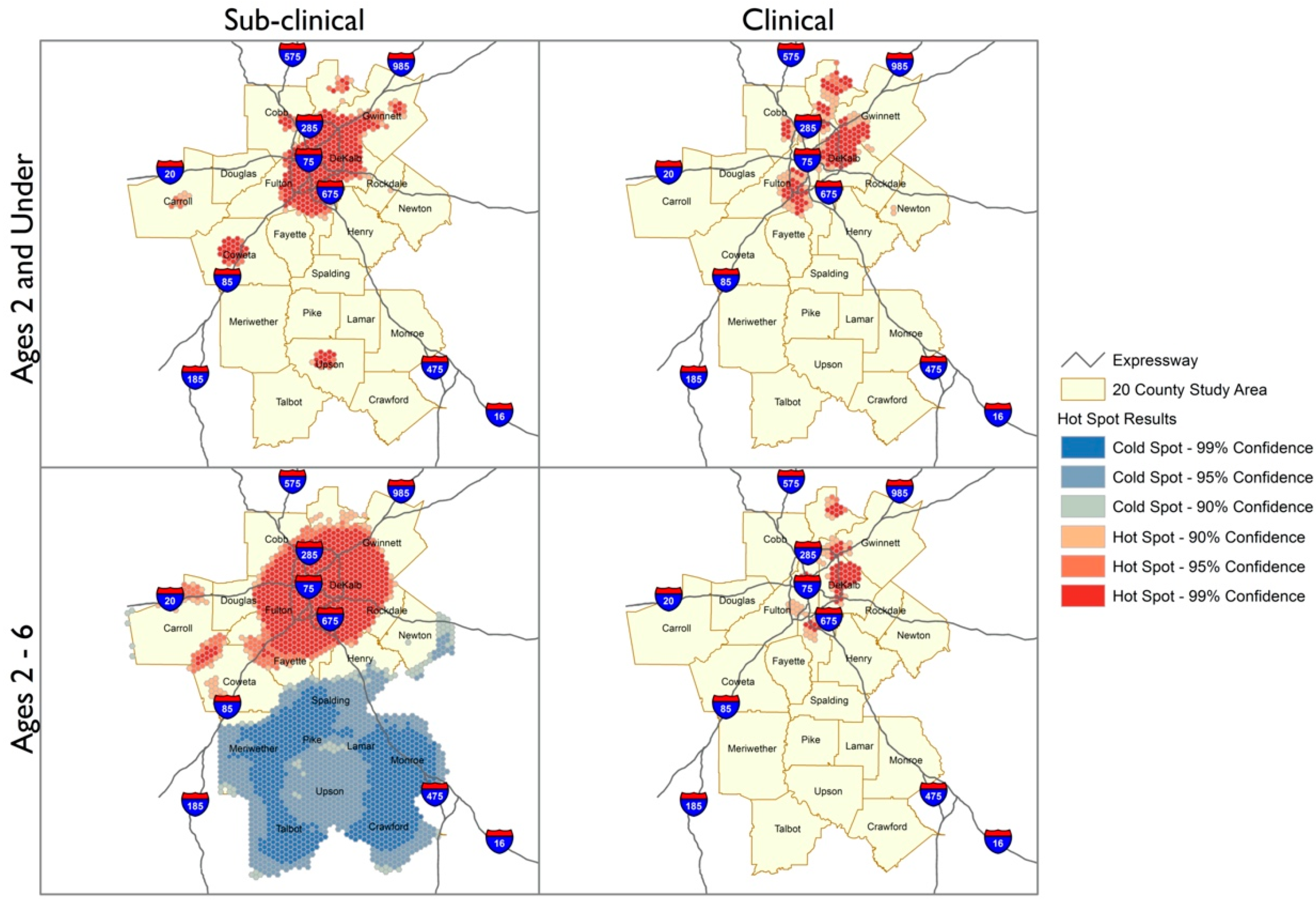
3.1. Spatial Analyses
3.2. Participant Characteristics, by Lead Status
3.3. Predictors of BLL 2 to <5 and BLL ≥ 5 µg/dL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dignam, T.; Kaufmann, R.B.; LeStourgeon, L.; Brown, M.J. Control of Lead Sources in the United States, 1970–2017: Public Health Progress and Current Challenges to Eliminating Lead Exposure. J. Public Health Manag. Pract. 2019, 25 (Suppl. 1), S13–S22. [Google Scholar] [CrossRef]
- Arora, M.; Austin, C.; Sarrafpour, B.; Hernández-Ávila, M.; Hu, H.; Wright, R.O.; Tellez-Rojo, M.M. Determining prenatal, early childhood and cumulative long-term lead exposure using micro-spatial deciduous dentine levels. PLoS ONE 2014, 9, e97805. [Google Scholar] [CrossRef] [PubMed]
- Cassidy-Bushrow, A.E.; Sitarik, A.R.; Havstad, S.; Park, S.K.; Bielak, L.F.; Austin, C.; Johnson, C.C.; Arora, M. Burden of higher lead exposure in African-Americans starts in utero and persists into childhood. Environ. Int. 2017, 108, 221–227. [Google Scholar] [CrossRef]
- Needleman, H.L.; McFarland, C.; Ness, R.B.; Fienberg, S.E.; Tobin, M.J. Bone lead levels in adjudicated delinquents: A case control study. Neurotoxicol. Teratol. 2002, 24, 711–717. [Google Scholar] [CrossRef]
- Abadin, H.; Ashizawa, A.; Stevens, Y.W.; Llados, F.; Diamond, G.; Sage, G.; Citra, M.; Quinones, A.; Bosch, S.J.; Swarts, S.G. Toxicological Profile for Lead; Agency for Toxic Substances and Disease Registry (US): Atlanta, GA, USA, 2007.
- Levin, R.; Brown, M.J.; Kashtock, M.E.; Jacobs, D.E.; Whelan, E.A.; Rodman, J.; Schock, M.R.; Padilla, A.; Sinks, T. Lead exposures in U.S. Children, 2008: Implications for prevention. Environ. Health Perspect. 2008, 116, 1285–1293. [Google Scholar] [CrossRef]
- Bellinger, D.C.; Stiles, K.M.; Needleman, H.L. Low-level lead exposure, intelligence and academic achievement: A long-term follow-up study. Pediatrics 1992, 90, 855–861. [Google Scholar]
- Lanphear, B.P.; Hornung, R.; Khoury, J.; Yolton, K.; Baghurst, P.; Bellinger, D.C.; Canfield, R.L.; Dietrich, K.N.; Bornschein, R.; Greene, T.; et al. Low-level environmental lead exposure and children’s intellectual function: An international pooled analysis. Environ. Health Perspect. 2005, 113, 894–899. [Google Scholar] [CrossRef] [PubMed]
- Canfield, R.L.; Henderson, C.R., Jr.; Cory-Slechta, D.A.; Cox, C.; Jusko, T.A.; Lanphear, B.P. Intellectual impairment in children with blood lead concentrations below 10 microg per deciliter. N. Engl. J. Med. 2003, 348, 1517–1526. [Google Scholar] [CrossRef]
- No authors listed. NTP monograph on health effects of low-level lead. NTP Monogr. 2012, xiii, xv-148. [Google Scholar]
- Binns, H.J.; Campbell, C.; Brown, M.J. Interpreting and managing blood lead levels of less than 10 microg/dL in children and reducing childhood exposure to lead: Recommendations of the Centers for Disease Control and Prevention Advisory Committee on Childhood Lead Poisoning Prevention. Pediatrics 2007, 120, e1285–e1298. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.M.; Kahn, R.S.; Froehlich, T.; Auinger, P.; Lanphear, B.P. Exposures to environmental toxicants and attention deficit hyperactivity disorder in U.S. children. Environ. Health Perspect. 2006, 114, 1904–1909. [Google Scholar] [CrossRef] [PubMed]
- Chiodo, L.M.; Jacobson, S.W.; Jacobson, J.L. Neurodevelopmental effects of postnatal lead exposure at very low levels. Neurotoxicol. Teratol. 2004, 26, 359–371. [Google Scholar] [CrossRef]
- Lanphear, B.P.; Dietrich, K.; Auinger, P.; Cox, C. Cognitive deficits associated with blood lead concentrations <10 microg/dL in US children and adolescents. Public Health Rep. 2000, 115, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Georgia Department of Public Health. Lead Screening Guidelines for Children. Available online: https://dph.georgia.gov/lead-screening-guidelines-children (accessed on 12 February 2018).
- Needleman, H.L.; Schell, A.; Bellinger, D.; Leviton, A.; Allred, E.N. The long-term effects of exposure to low doses of lead in childhood. An 11-year follow-up report. N. Engl. J. Med. 1990, 322, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Beidinger-Burnett, H.; Ahern, L.; Ngai, M.; Filippelli, G.; Sisk, M. Inconsistent screening for lead endangers vulnerable children: Policy lessons from South Bend and Saint Joseph County, Indiana, USA. J. Public Health Policy 2019, 40, 103–113. [Google Scholar] [CrossRef] [PubMed]
- State Lead Screening Policies and Reporting Requirements. Available online: https://saferchemicals.org/get-the-facts/children-at-risk/state-lead-screening-policies/ (accessed on 5 May 2021).
- State Strategies to Improve Childhood Lead Screening and Treatment Services under Medicaid and CHIP. Available online: https://www.nashp.org/wp-content/uploads/2018/04/Childhood-Lead-Screening.pdf (accessed on 5 May 2021).
- Wengrovitz, A.M.; Brown, M.J. Recommendations for blood lead screening of Medicaid-eligible children aged 1–5 years: An updated approach to targeting a group at high risk. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2009, 58, 1–11. [Google Scholar]
- Ossiander, E.M. A systematic review of screening questionnaires for childhood lead poisoning. J. Public Health Manag. Pract. 2013, 19, E21–E29. [Google Scholar] [CrossRef]
- Caldwell, K.L.; Cheng, P.Y.; Jarrett, J.M.; Makhmudov, A.; Vance, K.; Ward, C.D.; Jones, R.L.; Mortensen, M.E. Measurement Challenges at Low Blood Lead Levels. Pediatrics 2017, 140. [Google Scholar] [CrossRef] [PubMed]
- Gould, E. Childhood lead poisoning: Conservative estimates of the social and economic benefits of lead hazard control. Environ. Health Perspect. 2009, 117, 1162–1167. [Google Scholar] [CrossRef]
- Vaidyanathan, A.; Staley, F.; Shire, J.; Muthukumar, S.; Kennedy, C.; Meyer, P.A.; Brown, M.J. Screening for lead poisoning: A geospatial approach to determine testing of children in at-risk neighborhoods. J. Pediatr. 2009, 154, 409–414. [Google Scholar] [CrossRef]
- Rustin, R.; Kuriantnyk, C.; Lobsinger, B.; Charles, S. Use of geographical information systems to identify counties in Georgia with high risk for childhood lead poisoning. J. Georg. Public Health Assoc. 2015, 5, 170–176. [Google Scholar]
- Jones, R.L.; Homa, D.M.; Meyer, P.A.; Brody, D.J.; Caldwell, K.L.; Pirkle, J.L.; Brown, M.J. Trends in blood lead levels and blood lead testing among US children aged 1 to 5 years, 1988–2004. Pediatrics 2009, 123, e376–e385. [Google Scholar] [CrossRef] [PubMed]
- Kaplowitz, S.A.; Perlstadt, H.; Perlstadt, H.; Post, L.A. Comparing lead poisoning risk assessment methods: Census block group characteristics vs. zip codes as predictors. Public Health Rep. 2010, 125, 234–245. [Google Scholar] [CrossRef] [PubMed]
- Ali, F.; Immergluck, L.C.; Leong, T.; Waller, L.; Malhotra, K.; Jerris, R.C.; Edelson, M.; Rust, G.S. A Spatial Analysis of Health Disparities Associated with Antibiotic Resistant Infections in Children Living in Atlanta (2002–2010). EGEMS 2019, 7, 50. [Google Scholar] [CrossRef]
- Akkus, C.; Ozdenerol, E. Exploring Childhood Lead Exposure through GIS: A Review of the Recent Literature. Int. J. Environ. Res. Public Health 2014, 11, 6314–6334. [Google Scholar] [CrossRef]
- Aelion, C.M.; Davis, H.T. Blood lead levels in children in urban and rural areas: Using multilevel modeling to investigate impacts of gender, race, poverty, and the environment. Sci. Total Environ. 2019, 694, 133783. [Google Scholar] [CrossRef]
- McClure, L.F.; Niles, J.K.; Kaufman, H.W. Blood Lead Levels in Young Children: US, 2009–2015. J. Pediatr. 2016, 175, 173–181. [Google Scholar] [CrossRef]
- CMS. Early and Periodic Screening, Diagnostic, and Treatment. Available online: https://www.medicaid.gov/medicaid/benefits/early-and-periodic-screening-diagnostic-and-treatment/lead-screening/index.html (accessed on 5 May 2021).
- NCQA. Lead Screening in Children (LSC). HEDIS Measures and Technical Resources. Available online: https://www.ncqa.org/hedis/measures/lead-screening-in-children/ (accessed on 5 May 2021).
- Children at Risk: Gaps in State Lead Screening Policies. Available online: https://saferchemicals.org/wp-content/uploads/2017/01/saferchemicals.org_children-at-risk-report.pdf (accessed on 5 May 2021).
- Haboush-Deloye, A.; Marquez, E.R.; Gerstenberger, S.L. Determining Childhood Blood Lead Level Screening Compliance Among Physicians. J. Community Health 2017, 42, 779–784. [Google Scholar] [CrossRef]
- Council on Environmental Health. Prevention of Childhood Lead Toxicity. Pediatrics 2016, 138, e20161493. [Google Scholar] [CrossRef]
- White, B.M.; Bonilha, H.S.; Ellis, C., Jr. Racial/Ethnic Differences in Childhood Blood Lead Levels Among Children <72 Months of Age in the United States: A Systematic Review of the Literature. J. Racial Ethn. Health Disparities 2016, 3, 145–153. [Google Scholar] [CrossRef]
- Tsoi, M.F.; Cheung, C.L.; Cheung, T.T.; Cheung, B.M. Continual Decrease in Blood Lead Level in Americans: United States National Health Nutrition and Examination Survey 1999–2014. Am. J. Med. 2016, 129, 1213–1218. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.; Dodd, A.H.; Neuman, M. Availability of data to measure disparities in leading health indicators at the state and local levels. J. Public Health Manag. Pract. 2008, 14, S36–S44. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Individual-Level Variables | Total | BLLs < 2 µg/dL (n = 38,265) 41.1% | BLLs 2 to <5 µg/dL (n = 52,739) 56.6% | BLLs ≥ 5 µg/dL (n = 2158) 2.3% |
|---|---|---|---|---|
| Frequency (%) | Frequency (%) | Frequency (%) | ||
| Age | ||||
| 0–24 months | 50,993(54.7) | 22,292(58.3) | 27,719(52.6) | 982(45.5) |
| 25–72 months | 42,169(45.3) | 15,973(41.7) | 25,020(47.4) | 1176(54.5) |
| Gender | ||||
| Female | 45,268(48.7) | 18,665(48.8) | 25,577(48.6) | 1026(47.7) |
| Male | 47,782(51.4) | 19,564(51.2) | 27,092(51.4) | 1126(52.3) |
| Race | ||||
| Black | 31,731(34.6) | 19,049(49.9) | 12,073(23.5) | 609(28.5) |
| White | 9049(9.9) | 5308(13.9) | 3548(6.9) | 193(9.0) |
| Other | 10,248(11.2) | 6302(16.5) | 3542(6.9) | 404(18.9) |
| Unknown | 40,669(44.3) | 7518(19.7) | 32,222(62.7) | 929(43.5) |
| Black | 31,731(34.6) | 19,049(49.9) | 12,073(23.5) | 609(28.5) |
| White | 9049(9.9) | 5308(13.9) | 3548(6.9) | 193(9.0) |
| Other | 10,248(11.2) | 6302(16.5) | 3542(6.9) | 404(18.9) |
| Unknown | 40,669(44.3) | 7518(19.7) | 32,222(62.7) | 929(43.5) |
| Medicaid status | ||||
| No | 24,472(26.3) | 10,629(27.8) | 13,150(24.9) | 693(32.1) |
| Yes | 68,690(73.7) | 27,636(72.2) | 39,589(75.1) | 1465(67.9) |
| Place of residence status | ||||
| Rural | 334(0.4) | 132(0.4) | 191(0.4) | 11(0.5) |
| Sub-urban | 71,877(77.3) | 30,169(78.9) | 39,957(75.9) | 1751(81.6) |
| Urban | 20,835(22.4) | 7941(20.8) | 12,509(23.8) | 385(17.9) |
| Area-Level Variables | BLLs < 2 µg/dL | BLLs 2 to <5 µg/dL | BLLs ≥ 5 µg/dL |
|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |
| Block-level | |||
| Number of blocks | 2075 | 2091 | 876 |
| Number of individuals in the block (median, range) | 11(1–177) | 15(1–513) | 1(1–118) |
| Ages of children in the block | |||
| Under 5 years old (%) | 7.7 ± 4.7 | 7.8 ± 4.6 | 8.4 ± 4.8 |
| Racial composition | |||
| White (%) | 33.2 ± 27.7 | 31.6 ± 26.3 | 29.4 ± 26.3 |
| Black (%) | 55.3 ± 32.2 | 55.3 ± 31.4 | 50.8 ± 30.4 |
| Poverty Status | |||
| Income-Below Poverty (%) | 22.9 ± 15.9 | 23.1 ± 15.8 | 26.6 ± 17.4 |
| Educational Attainment (adults 25+ years) | |||
| No High School Diploma (%) | 16.6 ± 12.5 | 17.3 ± 12.8 | 21.1 ± 14.8 |
| High School Diploma or equivalent (%) | 29.0 ± 11.1 | 28.9 ± 10.6 | 27.1 ± 11.2 |
| College Degree (%) | 55.6 ± 17.0 | 55.1 ± 16.3 | 53.6 ± 17.3 |
| Housing | |||
| House Built before 1980 (%) | 44.1 ± 27.7 | 43.3 ± 27.8 | 52.6 ± 28.2 |
| Total Housing Units/100 | 10.4 ± 6.0 | 10.3 ± 6.1 | 9.2 ± 5.3 |
| 2010 Homeowner (%) | 51.7 ± 27.2 | 51.9 ± 27.2 | 45.1 ± 27.3 |
| 2010 Renter (%) | 48.3 ± 27.2 | 48.1 ± 27.2 | 54.9 ± 27.3 |
| Single Family Home (%) | 61.2 ± 31.1 | 61.8 ± 30.8 | 54.7 ± 31.4 |
| Multi-unit homes (%) | 38.8 ± 31.0 | 38.2 ± 30.8 | 45.2 ± 31.3 |
| Household single female (%) | 22.6 ± 11.1 | 22.8 ± 10.5 | 22.1 ± 9.7 |
| Crime Status | |||
| 2019 Total Crime Index | 173.1 ± 86.2 | 171.7 ± 87.6 | 164.7 ± 79.6 |
| Individual-and Area-Level Characteristics | AOR (95% CI) | ||||
|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | ||
| Fixed effects | |||||
| Age | 0–2 | – | 0.68(0.65–0.70) | – | 0.68(0.66–0.70) |
| 2–6 | – | 1 | – | 1 | |
| Gender | Female | – | 0.99(0.96–1.03) | – | 0.99(0.96–1.03) |
| Male | – | 1 | – | 1 | |
| Race | Black | – | 1 | – | 1 |
| White | – | 1.20(1.13–1.28) | – | 1.31(1.22–1.39) | |
| Other | – | 0.83(0.79–0.88) | – | 0.85(0.80–0.90) | |
| Unknown | – | 9.78(9.36–10.23) | – | 10.05(9.61–10.51) | |
| Medicaid status | No | – | 0.42(0.40–0.44) | – | 0.42(0.40–0.44) |
| Yes | – | 1 | – | 1 | |
| Area | Suburban | – | 0.91(0.85–0.98) | – | 0.91(0.85–0.98) |
| Rural | – | 1.25(0.89–1.75) | – | 1.48(1.06–2.07) | |
| Urban | – | 1 | – | 1 | |
| Age under 5 (%) | – | – | 1.06(0.99–1.14) | 1.03(0.96–1.11) | |
| Houses Built pre-1980 (%) | – | – | 0.98(0.97–1.00) | 1.01(0.99–1.02) | |
| 2019 Total Crime Index | – | – | 1.00(0.99–1.00) | 1.00(0.99–1.00) | |
| 2010 Renter (%) | – | – | 0.98(0.97–0.99) | 0.98(0.96–0.99) | |
| GED/High School Diploma (%) | – | – | 1.02(0.99–1.04) | 1.02(0.99–1.04) | |
| White (%) | – | – | 0.97(0.96–0.98) | 0.93(0.92–0.95) | |
| Block Random effects | |||||
| Block variance (SE) | 0.30(0.02) | 0.26(0.02) | 0.29(0.01) | 0.24(0.01) | |
| ICC (%) | 8.4 | 7.3 | 8.1 | 6.8 | |
| PCV (%) | Ref | 13.3 | 3.3 | 20.0 | |
| Model fit statistics | |||||
| Log-likelihood | 120,633.5 | 81,475.32 | 120,574.7 | 81,349.43 | |
| AIC | 120,637.5 | 81,495.32 | 120,590.7 | 81,381.43 | |
| Individual-and Area-Level Characteristics | AOR (95% CI) | |||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |||
| Fixed effects | ||||||
| Age | 0–2 | – | 1.13(1.03–1.25) | – | 1.13(1.02–1.25) | |
| 2–6 | – | 1 | – | 1 | ||
| Gender | Female | – | 0.98(0.89–1.08) | – | 0.97(0.88–1.10) | |
| Male | – | 1 | – | 1 | ||
| Race | Black | – | 1 | – | 1 | |
| White | – | 0.85(0.70–1.03) | – | 0.90(0.73–1.10) | ||
| Other | – | 0.80(0.68–0.94) | – | 0.83(0.71–0.98) | ||
| Unknown | – | 1.77(1.57–2.00) | – | 1.83(1.62–2.06) | ||
| Medicaid status | No | – | 0.64(0.58–0.72) | – | 0.66(0.59–0.73) | |
| Yes | – | 1 | – | 1 | ||
| Area | Suburban | – | 0.79(0.66–0.95) | – | 0.92(0.76–1.11) | |
| Rural | – | 0.78(0.32–1.94) | – | 0.78(0.32–1.85) | ||
| Urban | – | 1 | – | 1 | ||
| Age under 5 (%) | – | – | 1.08(0.91–1.27) | 1.12(0.95–1.33) | ||
| Houses Built pre-1980 (%) | – | – | 0.92(0.90–0.95) | 0.92(0.90–0.95) | ||
| 2019 Total Crime Index | – | – | 1.01(1.00–1.02) | 1.01(1.00–1.02) | ||
| 2010 Renter (%) | – | – | 0.96(0.93–0.99) | 0.96(0.93–0.99) | ||
| GED/High School Diploma (%) | – | – | 1.08(1.02–1.15) | 1.10(1.02–1.17) | ||
| White (%) | – | – | 0.98(0.95–1.01) | 0.99(0.96–1.03) | ||
| Block Random effects | ||||||
| Block variance (SE) | 0.79(0.07) | 0.72(0.08) | 0.70(0.07) | 0.63(0.07) | ||
| ICC (%) | 19.4 | 18.0 | 17.5 | 16.1 | ||
| PCV (%) | Ref | 8.8 | 11.4 | 20.3 | ||
| Model fit statistics | ||||||
| Log-likelihood | 17,029.17 | 14,005.37 | 16,977.06 | 13,966.2 | ||
| AIC | 17,033.17 | 14,025.37 | 16,993.06 | 13,998.2 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dickinson-Copeland, C.M.; Immergluck, L.C.; Britez, M.; Yan, F.; Geng, R.; Edelson, M.; Kendrick-Allwood, S.R.; Kordas, K. Increased Risk of Sub-Clinical Blood Lead Levels in the 20-County Metro Atlanta, Georgia Area—A Laboratory Surveillance-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 5163. https://doi.org/10.3390/ijerph18105163
Dickinson-Copeland CM, Immergluck LC, Britez M, Yan F, Geng R, Edelson M, Kendrick-Allwood SR, Kordas K. Increased Risk of Sub-Clinical Blood Lead Levels in the 20-County Metro Atlanta, Georgia Area—A Laboratory Surveillance-Based Study. International Journal of Environmental Research and Public Health. 2021; 18(10):5163. https://doi.org/10.3390/ijerph18105163
Chicago/Turabian StyleDickinson-Copeland, Carmen M., Lilly Cheng Immergluck, Maria Britez, Fengxia Yan, Ruijin Geng, Mike Edelson, Salathiel R. Kendrick-Allwood, and Katarzyna Kordas. 2021. "Increased Risk of Sub-Clinical Blood Lead Levels in the 20-County Metro Atlanta, Georgia Area—A Laboratory Surveillance-Based Study" International Journal of Environmental Research and Public Health 18, no. 10: 5163. https://doi.org/10.3390/ijerph18105163
APA StyleDickinson-Copeland, C. M., Immergluck, L. C., Britez, M., Yan, F., Geng, R., Edelson, M., Kendrick-Allwood, S. R., & Kordas, K. (2021). Increased Risk of Sub-Clinical Blood Lead Levels in the 20-County Metro Atlanta, Georgia Area—A Laboratory Surveillance-Based Study. International Journal of Environmental Research and Public Health, 18(10), 5163. https://doi.org/10.3390/ijerph18105163