Public Health Innovation through Cloud Adoption: A Comparative Analysis of Drivers and Barriers in Japan, South Korea, and Singapore




Abstract
1. Introduction
2. Cloud Computing
3. Cloud Adoption in Healthcare
4. Cases
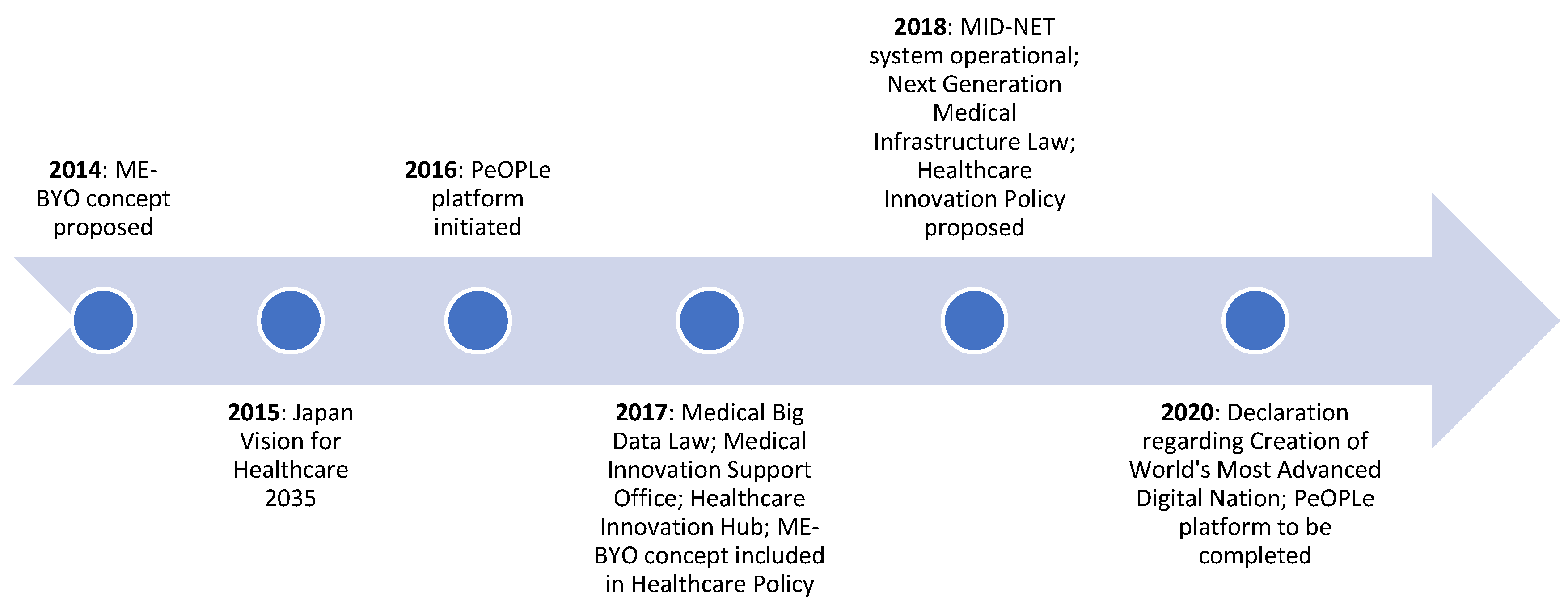
4.1. Japan
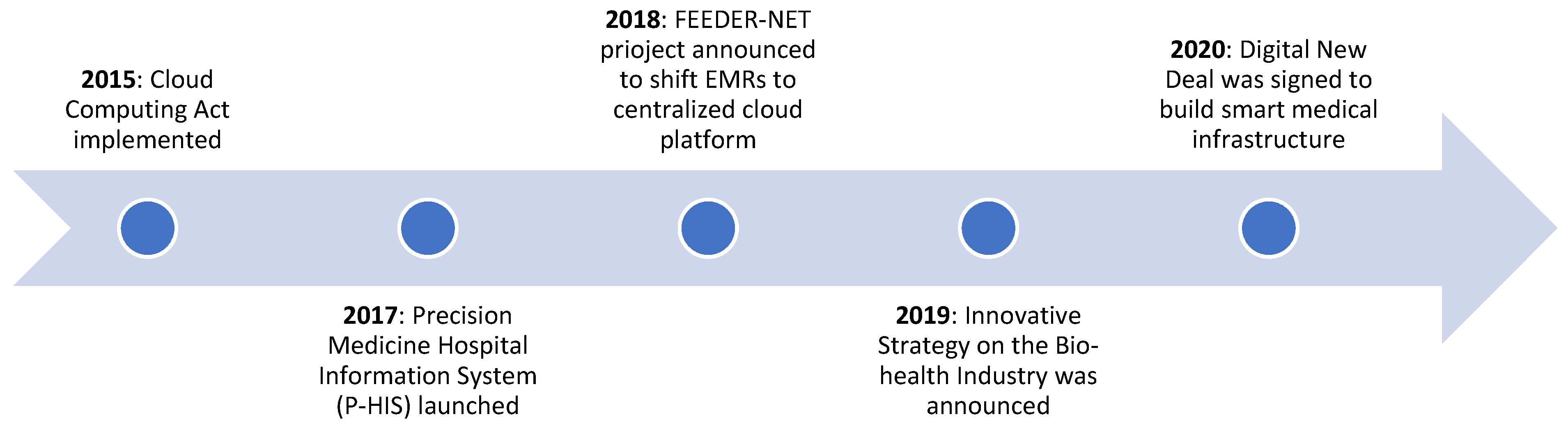
4.2. South Korea
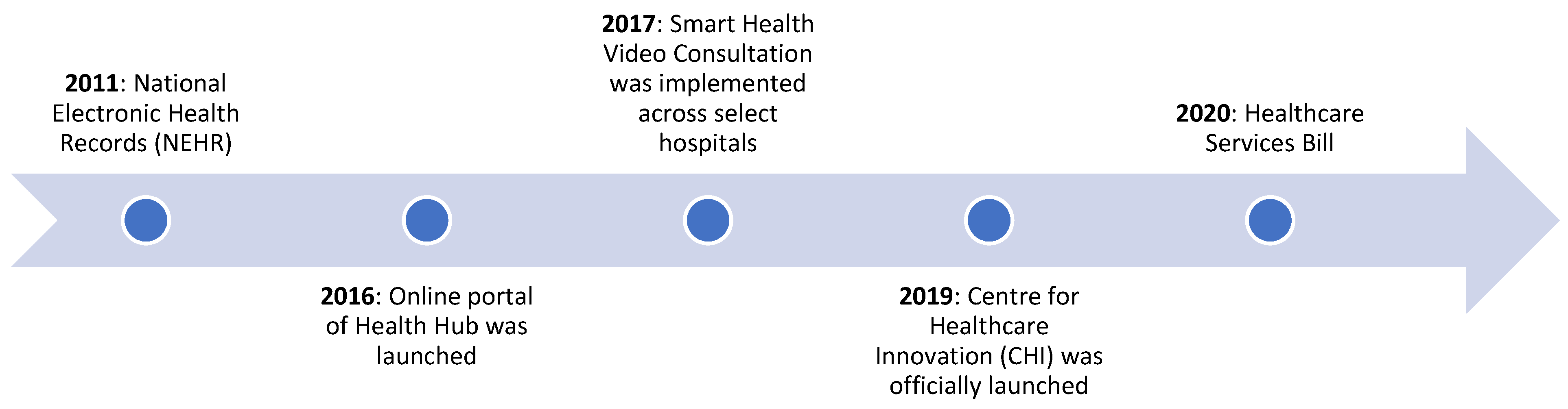
4.3. Singapore
5. Drivers of Cloud Adoption in Healthcare
5.1. Contextual Factors
5.1.1. Demographic and Economic Factors
5.1.2. Nature of the Healthcare System
5.1.3. Technology Readiness and Innovation Mindset
5.2. Policy Factors
5.2.1. National Policy Frameworks that Promote Digitization of Healthcare
5.2.2. Cloud-Specific Policies
Data Standardization
Data Storage
Data Privacy
Cybersecurity
5.2.3. Incentives for Cloud Adoption
5.3. Human Factors
Public Trust and Acceptance
6. Barriers to Cloud Adoption in Healthcare
6.1. Contextual Factors
6.1.1. Healthcare Status
6.1.2. Technology Readiness
6.2. Organizational Factors
6.2.1. Cost of Cloud Adoption
6.2.2. Technical Expertise
6.3. Policy Factors
6.3.1. Lack of Data Standards
6.3.2. Strict Data Storage Requirements
6.3.3. Data Privacy Concerns
6.3.4. Weak Cloud Security Infrastructure
7. Discussion
7.1. Policy Recommendations
7.1.1. Undertaking Sustained Policy Approach for Cloud Adoption
7.1.2. Incentivizing Cloud Adoption for Healthcare Institutions
7.1.3. Standardizing Health Data for Largescale Adoption
7.1.4. Enabling Flexible Data Storage Policies
7.1.5. Strengthening Data Protection
7.1.6. Improving Cybersecurity Architecture of Health Cloud
7.1.7. Encouraging and Supporting Public Healthcare Innovations
7.2. Study Limitations and Future Research Directions
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | Artificial intelligence |
| CAGR | Compounded annual growth rate |
| CC | Cloud computing |
| CD | Compact disk |
| CDM | Common data module |
| CHI | Centre for Healthcare Innovation |
| CHILD | CHI Learning and Development |
| CiEHR | Center for Interoperable Electronic Health Records |
| CMIS | Critical Medical Information Store |
| CSP | Cloud service provider |
| EHR | Electronic health records |
| EMR | Electronic medical record |
| EMRX | Electronic Medical Record Exchange |
| GDP | Gross domestic product |
| HAQ | Healthcare Access and Quality |
| HCNF | Healthcare New Frontier |
| HIE | Health Information Exchange |
| ICT | Information and communication technology |
| IHIS | Integrated Health Information Systems |
| IoT | Internet of things |
| KUMC | Korea University Medical Center |
| MHLW | Ministry of Health, Labor and Welfare |
| METI | The Ministry of Economy, Trade and Industry |
| MML | Medical Markup Language |
| MOH | Ministry of Health |
| MOHW | Ministry of Health and Welfare |
| MoKE | Ministry of Knowledge Economy |
| MSIP | Ministry of Science, Information and Communications Technology and Future Planning |
| MTCS | Multi-Tier Cloud Security Standard for Singapore |
| NCB | National Computer Board |
| NEHR | National Electronic Health Record |
| NHG | National Health Group |
| NHIS | National Health Insurance Service |
| NIST | National Institute of Standards and Technology |
| NRIC | National Registration Identity Card |
| NUHS | National University Healthcare System |
| PDPA | Personal Data Protection Act |
| PDPC | Personal Data Protection Commission |
| PHR | Personal health records |
| PIPA | Personal Information Protection Act |
| SHVC | Smart Health Video Consultation |
| SSTN | Social Society and Tax Number |
| WHO | World Health Organization |
References
- Das, R.K.; Patnaik, S.; Misro, A.K. Adoption of cloud computing in e-Governance. In Communications in Computer and Information Science; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Dash, S.; Pani, S.K. E-Governance Paradigm Using Cloud Infrastructure: Benefits and Challenges. Procedia Comput. Sci. 2016, 85, 843–855. [Google Scholar] [CrossRef]
- Vu, K.; Hartley, K.; Kankanhalli, A. Predictors of cloud computing adoption: A cross-country study. Telemat. Inform. 2020, 52, 101426. [Google Scholar] [CrossRef]
- Polyviou, A.; Pouloudi, N. Understanding cloud adoption decisions in the public sector. In Proceedings of the Annual Hawaii International Conference on System Sciences, Kauai, HI, USA, 5–8 January 2015; pp. 2085–2094. [Google Scholar]
- Alonso, J.; Escalante, M.; Orue-Echevarria, L. Transformational Cloud Government (TCG): Transforming Public Administrations with a Cloud of Public Services. In Cloud Forward; Elsevier: Madrid, Spain, 2016. [Google Scholar]
- Tweneboah-Koduah, S.; Endicott-Popovsky, B.; Tsetse, A. Barriers to government cloud adoption. Int. J. Manag. Inf. Technol. 2014, 6, 1–16. [Google Scholar] [CrossRef]
- Hameduddin, T.; Fernandez, S.; Demircioglu, M.A. Conditions for open innovation in public organizations: Evidence from Challenge. gov. Asia Pac. J. Public Adm. 2020, 42, 111–131. [Google Scholar]
- Lee, S.M.; Hwang, T.; Choi, D. Open innovation in the public sector of leading countries. Manag. Decis. 2020, 50, 147–162. [Google Scholar] [CrossRef]
- Prpić, J.; Taeihagh, A.; Melton, J. The fundamentals of policy crowdsourcing. Policy Internet 2015, 7, 340–361. [Google Scholar] [CrossRef]
- Taeihagh, A. Crowdsourcing: A new tool for policymaking? Policy Sci. 2017, 50, 629–647. [Google Scholar] [CrossRef]
- Alghatani, K.; Abdelmounaam, R. A cloud-based intelligent remote patient monitoring architecture. In Proceedings of the International Conference on Health Informatics & Medical Systems HIMS2019, Las Vegas, NV, USA, July 29–1 August 2019; Volume 19. Available online: http://wpage.unina.it/giuseppe.aceto/pub/aceto2020industry40eHealth__JII.pdf (accessed on 2 July 2020).
- Kuo, M.H.; Kushniruk, A.; Borycki, E. Can cloud computing benefit health services?-a SWOT analysis. Stud. Health Technol. Inform. 2011, 169, 379–383. [Google Scholar]
- Sultan, N. Making use of cloud computing for healthcare provision: Opportunities and challenges. Int. J. Inf. Manag. 2014, 34, 177–184. [Google Scholar] [CrossRef]
- Jin, Z.; Chen, Y. Telemedicine in the cloud era: Prospects and challenges. IEEE Pervasive Comput. 2015, 14, 54–61. [Google Scholar] [CrossRef]
- Hoang, D.B.; Chen, L. Mobile cloud for assistive healthcare (MoCAsH). In Proceedings of the 2010 IEEE Asia-Pacific Services Computing Conference, Hangzhou, China, 6–10 December 2010; IEEE: Piscataway, NJ, USA, 2010; pp. 325–332. [Google Scholar]
- Lo’ai, A.T.; Mehmood, R.; Benkhlifa, E.; Song, H. Mobile cloud computing model and big data analysis for healthcare applications. IEEE Access 2016, 4, 6171–6180. [Google Scholar]
- Bahga, A.; Madisetti, V.K. A cloud-based approach for interoperable electronic health records (EHRs). IEEE J. Biomed. Health Inform. 2013, 17, 894–906. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, S.P.; Mani, S.; Zambrano, J. A Survey of the State of Cloud Computing in Healthcare. Netw. Commun. Technol. 2012, 1, 12. [Google Scholar] [CrossRef]
- Kuo, A.M.H. Opportunities and challenges of cloud computing to improve health care services. J. Med. Internet Res. 2011, 13, e67. [Google Scholar] [CrossRef]
- The NIST Definition of Cloud Computing. Available online: https://csrc.nist.gov/publications/detail/sp/800-145/final (accessed on 15 May 2020).
- Who Coined Cloud Computing? Available online: https://www.technologyreview.com/2011/10/31/257406/who-coined-cloud-computing/ (accessed on 25 May 2020).
- Gartner Forecasts Worldwide Public Cloud Revenue to Grow 17% in 2020. Available online: https://www.gartner.com/en/newsroom/press-releases/2019-11-13-gartner-forecasts-worldwide-public-cloud-revenue-to-grow-17-percent-in-2020 (accessed on 30 May 2020).
- Government in The Cloud: Adoption Has Become Safer and Smarter. Available online: https://www.forbes.com/sites/forbestechcouncil/2019/04/19/government-in-the-cloud-adoption-has-become-safer-and-smarter/#6807047323b4 (accessed on 3 July 2020).
- Understanding Cloud Adoption in Government. Available online: https://www.gartner.com/smarterwithgartner/understanding-cloud-adoption-in-government/ (accessed on 1 June 2020).
- Federal Cloud Computing Strategy. The White House. Available online: https://marketplace.vion.com/order/uploads/VIONMP5/federal-cloud-computing-strategy.pdf (accessed on 3 July 2020).
- Millard, J. ICT-enabled public sector innovation: Trends and prospects. In Proceedings of the 7th International Conference on Theory and Practice of Electronic Governance, Seoul, Korea, 22–25 October 2013; pp. 77–86. [Google Scholar]
- Kuiper, E.; Van Dam, F.; Reiter, A.; Janssen, M. Factors influencing the adoption of and business case for Cloud computing in the public sector. In Proceedings of the e-Challenges e-2014 Conference Proceedings, Belfast, UK, 29 October 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 1–10. [Google Scholar]
- Zwattendorfer, B.; Stranacher, K.; Tauber, A.; Reichstädter, P. Cloud computing in e-government across Europe. In Proceedings of the International Conference on Electronic Government and the Information Systems Perspective, Prague, Czech Republic, 25 August 2013; Springer: Berlin/Heidelberg, Germany, 2013; pp. 181–195. [Google Scholar]
- Advancing Cloud Adoption in Asia. Available online: https://www.refinitiv.com/perspectives/big-data/advancing-cloud-adoption-in-asia/ (accessed on 25 August 2020).
- Better Late than Never: Governments Move to the Cloud. Available online: https://thrive.dxc.technology/anz/2019/07/10/better-late-than-never-governments-move-to-the-cloud/ (accessed on 10 July 2019).
- Korean Government to Accelerate Growth of Cloud Computing. Available online: http://www.businesskorea.co.kr/news/articleView.html?idxno=14251 (accessed on 12 June 2020).
- State of Cloud Adoption in Asia-Pacific. Available online: https://www.csaapac.org/uploads/8/4/7/7/84773638/cloud_adoption_in_apac_17.pdf (accessed on 15 June 2020).
- Albury, D. Fostering innovation in public services. Public Money Manag. 2005, 25, 51–56. [Google Scholar]
- Windrum, P.; Koch, P.M. (Eds.) Innovation in Public Sector Services: Entrepreneurship, Creativity and Management; Edward Elgar Publishing: Cheltenham, UK, 2008. [Google Scholar]
- Currie, W.; Seddon, J. A cross-country study of cloud computing policy and regulation in healthcare. In Proceedings of the ECIS 2014 Proceedings—22nd European Conference on Information Systems, Tel Aviv, Israel, 9–11 June 2014; ISBN 978-0-9915567-0-0. [Google Scholar]
- Lin, A.; Chen, N.C. Cloud computing as an innovation: Percepetion, attitude, and adoption. Int. J. Inf. Manag. 2012, 32, 533–540. [Google Scholar] [CrossRef]
- Chou, C.Y.; Chen, J.S.; Liu, Y.P. Inter-firm relational resources in cloud service adoption and their effect on service innovation. Serv. Ind. J. 2017, 37, 256–276. [Google Scholar] [CrossRef]
- Willcocks, L.P.; Venters, W.; Whitley, E.A. Cloud sourcing and innovation: Slow train coming? A composite research study. Strateg. Outsourcing Int. J. 2013, 6, 184–202. [Google Scholar] [CrossRef]
- Japan to Hire Amazon to Build Government Cloud. Available online: https://asia.nikkei.com/Business/Technology/Japan-to-hire-Amazon-to-build-government-cloud (accessed on 21 August 2020).
- Microsoft Publishes New Guide for Public-Sector Adoption of Cloud Solutions. Available online: https://news.microsoft.com/apac/2019/09/02/microsoft-publishes-new-guide-for-public-sector-adoption-of-cloud-solutions/ (accessed on 23 July 2020).
- Google Cloud Seeks Big Government Contracts to Script India Growth. Available online: https://inc42.com/buzz/google-cloud-looks-to-sign-up-government-contracts-for-india-growth/ (accessed on 23 July 2020).
- Alibaba Partners with Shanghai Municipal Government to Develop Yangtze River Delta Region. Available online: https://www.alibabacloud.com/blog/alibaba-partners-with-shanghai-municipal-government-to-develop-yangtze-river-delta-region_594208 (accessed on 1 June 2020).
- Chandrasekaran, A.; Kapoor, M. State of Cloud Computing in the Public Sector—A Strategic Analysis of the Business Case and Overview of Initiatives across Asia Pacific; Frost Sullivan: San Antonio, TX, USA, 2011; pp. 1–17. [Google Scholar]
- A Cloud for Doing Good: A Technology Revolution for all in ASEAN. Available online: https://3er1viui9wo30pkxh1v2nh4w-wpengine.netdna-ssl.com/wp-content/uploads/2017/10/A-Cloud-for-Doing-Good-FINAL.pdf (accessed on 18 May 2020).
- Haini, S.I.; Rahim, N.Z.A.; Zainuddin, N.M.M. Citizen Centric Impact on Success Factors of Digital Government Maturity in Malaysian Public Sector. In Proceedings of the Pacific Asia Conference on Information Systems (PACIS), Langkawi, Malaysia, 16–20 July 2017; Association for Information Systems: Langkawi Island, Malaysia, 2017. [Google Scholar]
- Dey, P.K.; Hariharan, S.; Brookes, N. Managing Healthcare Quality Using Logical Framework Analysis. Manag. Serv. Qual. 2006, 16, 203–222. [Google Scholar] [CrossRef]
- Jessup, R.L.; O’Connor, D.A.; Polina, P.; Rischin, K.; Nezon, J.; Cyril, S.; Shepperd, S.; Buchbinder, R. Alternative service models for delivery of healthcare services in high-income countries: A scoping review of systematic reviews. BMJ Open 2019, 9. [Google Scholar] [CrossRef]
- Misra, A.; Gopalan, H.; Jayawardena, R.; Hills, A.P.; Soares, M.; Reza-Albarrán, A.A.; Ramaiya, K.L. Diabetes in developing countries. J. Diabetes 2019, 11, 522–539. [Google Scholar] [CrossRef] [PubMed]
- Faezipour, M.; Ferreira, S. A System Dynamics Perspective of Patient Satisfaction in Healthcare. In Proceedings of the Conference on Systems Engineering Research, Atlanta, GA, USA, 19–22 March 2013; pp. 148–156. [Google Scholar]
- Shah, S.; Abbas, G.; Hanif, M.; Anees-Ur-Rehman, Z.M.; Riaz, N.; Altaf, A.; Hassan, S.L.; Saleem, U.; Shah, A. Increased burden of disease and role of health economics: Asia-pacific region. Expert Rev. Pharm. Outcomes Res. 2019, 19, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Countries Are Spending More on Health, but People Are Still Paying too much Out of Their Own Pockets. Available online: https://www.who.int/news/item/20-02-2019-countries-are-spending-more-on-health-but-people-are-still-paying-too-much-out-of-their-own-pockets (accessed on 14 September 2020).
- Sukkird, V.; Shirahada, K. Technology challenges to healthcare service innovation in aging Asia: Case of value co-creation in emergency medical support system. Technol. Soc. 2015, 43, 122–128. [Google Scholar] [CrossRef]
- World Population Ageing 2015: Highlights. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2015_Highlights.pdf (accessed on 22 August 2020).
- Meyer, S.B.; Luong, T.C.; Mamerow, L.; Ward, P.R. Inequities in access to healthcare: Analysis of national survey data across six Asia-Pacific countries. BMC Health Serv. Res. 2013, 13, 238. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Li, W.; Hao, Y.; Qian, Y.; Humar, I. Edge cognitive computing based smart healthcare system. Future Gener. Comput. Syst. 2018, 86, 403–411. [Google Scholar] [CrossRef]
- Shekelle, P.G.; Morton, S.C.; Keeler, E.B. Costs and benefits of health information technology. Evid. Rep. Technol. Assess (Full Rep.) 2006, 132, 1–71. [Google Scholar]
- The Digital Healthcare Leap. Available online: https://www.pwc.com/gx/en/issues/high-growth-markets/assets/the-digital-healthcare-leap.pdf (accessed on 25 May 2020).
- Dornan, L.; Pinyopornpanish, K.; Jiraporncharoen, W.; Hashmi, A.; Dejkriengkraikul, N.; Angkurawaranon, C. Utilisation of Electronic Health Records for Public Health in Asia: A Review of Success Factors and Potential Challenges. BioMed Res. Int. 2019, 2019, 1–9. [Google Scholar] [CrossRef]
- Ali, F.; El-Sappagh, S.; Islam, S.R.; Ali, A.; Attique, M.; Imran, M.; Kwak, K.S. An intelligent healthcare monitoring framework using wearable sensors and social networking data. Future Gener. Comput. Syst. 2020, 114, 23–43. [Google Scholar] [CrossRef]
- GBD. Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990–2015: A novel analysis from the Global Burden of Disease Study 2015. Lancet 2017, 390, 231–266. [Google Scholar] [CrossRef]
- Top 5 Healthcare Systems in Asia-Pacific. Available online: https://www.valuechampion.sg/top-5-healthcare-systems-asia-pacific (accessed on 20 June 2020).
- 2020 Global Healthcare Outlook: Laying a Foundation for the Future. Available online: https://www2.deloitte.com/us/en/insights/industry/health-care/global-health-care-outlook.html (accessed on 5 June 2020).
- Global Innovation Index. 2019. Available online: https://www.wipo.int/edocs/pubdocs/en/wipo_pub_gii_2019.pdf (accessed on 23 July 2020).
- New IDC Report Expects Asia/Pacific Healthcare Sector IT Spending to Reach USD 12.2 Billion in 2019. Available online: https://www.idc.com/getdoc.jsp?containerId=prAP45118019 (accessed on 22 June 2020).
- The Big-Data Revolution in US Health Care: Accelerating Value and Innovation. Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/the-big-data-revolution-in-us-health-care (accessed on 5 July 2020).
- How does Cloud Create Innovation? Available online: https://cloudcomputingtechnologies.com/how-does-cloud-create-innovation/ (accessed on 9 June 2020).
- Fukawa, T. Macro evaluation of the Japanese healthcare system in comparison with Germany. Jpn. J. Soc. Secur. Policy 2007, 6, 31–42. [Google Scholar]
- Nomura, H.; Nakayama, T. The Japanese healthcare system. BMJ 2005, 331, 648. [Google Scholar] [CrossRef] [PubMed]
- Anders, R.L. Japan’s healthcare system. JONA J. Nurs. Adm. 2000, 30, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Fukawa, T.; Izumida, N. Japanese healthcare expenditures in a comparative context. Jpn. J. Soc. Secur. Policy 2004, 3, 51–61. [Google Scholar]
- Yoshihara, K.; Wada, M. The History of Japan’s Health Insurance Systems; Toyo Keizai Inc.: Tokyo, Japan, 2008. [Google Scholar]
- Public Health Insurance in Japan. Available online: http://documents1.worldbank.org/curated/en/834961468756344156/pdf/330560JP0wbi37201.pdf (accessed on 20 June 2020).
- Tiessen, J.H.; Kato, K. Japanese healthcare: Fostering competition and controlling costs. Healthc. Manag. Forum 2017, 30, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Onaya, T.; Taketomi, M.; Fujii, H.; Negishi, T. ICT Trends in Japan’s Healthcare Policy. FUJITSU Sci. Tech. J. 2015, 51, 10–17. [Google Scholar]
- Aging and the Governance of the Healthcare System in Japan. Available online: https://www.bruegel.org/wp-content/uploads/imported/publications/WP_2014_14-2.pdf (accessed on 20 August 2020).
- OECD Economic Surveys: Japan 2019. Available online: https://www.oecd.org/economy/surveys/Japan-2019-OECD-economic-survey-overview.pdf (accessed on 30 August 2020).
- Abraham, C.; Nishihara, E.; Akiyama, M. Transforming healthcare with information technology in Japan: A review of policy, people, and progress. Int. J. Med. Inform. 2011, 80, 157–170. [Google Scholar] [CrossRef]
- An Age of Digital Healthcare Opportunity. Available online: https://cancerandageing.eiu.com/age-of-digital-healthcare-opportunity/ (accessed on 2 September 2020).
- Japan Health System Review. Available online: https://apps.who.int/iris/bitstream/handle/10665/259941/9789290226260-eng.pdf?sequence=1&isAllowed=y (accessed on 7 August 2020).
- Yasunaga, H.; Imamura, T.; Yamaki, S.; Endo, H. Computerizing medical records in Japan. Int. J. Med Inform. 2008, 77, 708–713. [Google Scholar] [CrossRef]
- Yoshida, Y.; Imai, T.; Ohe, K. The trends in EMR and CPOE adoption in Japan under the national strategy. Int. J. Med Inform. 2013, 82, 1004–1011. [Google Scholar] [CrossRef]
- Healthcare Policy (Revised). Available online: https://www.kantei.go.jp/jp/singi/kenkouiryou/en/pdf/2017_policy.pdf (accessed on 10 September 2020).
- The Japan Vision: Health Care 2035. Available online: https://www.mhlw.go.jp/seisakunitsuite/bunya/hokabunya/shakaihoshou/hokeniryou2035/assets/file/healthcare2035_proposal_150703_summary_en.pdf (accessed on 10 September 2020).
- Is Digital Health Finally Taking Off in Japan? Available online: https://www.intralinkgroup.com/en-GB/News/Blog/April-2019/Is-digital-health-finally-taking-off-in-Japan (accessed on 12 September 2020).
- Kajiyama, K.; Horiguchi, H.; Okumura, T.; Morita, M.; Kano, Y. De-identifying free text of Japanese dummy electronic health records. In Proceedings of the Ninth International Workshop on Health Text Mining and Information Analysis, Brussels, Belgium, 31 October 2018; pp. 65–70. [Google Scholar]
- Karako, K.; Chen, Y.; Song, P.; Tang, W. Super-aged society: Constructing an integrated information platform of self-recording lifelogs and medical records to support health care in Japan. Biosci. Trends 2019, 13, 276–278. [Google Scholar] [CrossRef]
- Transforming Healthcare Based on ME-BYO. Available online: http://s3-service-broker-live-19ea8b98-4d41-4cb4-be4c-d68f4963b7dd.s3.amazonaws.com/uploads/ckeditor/attachments/8444/293854_01_Kanagawa_Pref.pdf (accessed on 10 August 2020).
- World Health Organization (WHO). Interview with Yuji Kuroiwa: A novel approach to the ageing challenge. Bull. World Health Organ. 2017, 95, 736–737. [Google Scholar] [CrossRef]
- Japan’s Healthcare Innovation Policy. Available online: https://www.uschamber.com/sites/default/files/2018_japans_healthcare_innovation_policy_healthcare_industries_division_ministry_of_economy_trade_and_industry-june_2018.pdf (accessed on 11 September 2020).
- How the Japanese Government’s New “Sandbox” Program is Testing Innovations in Mobility and Technology. Available online: https://hbr.org/sponsored/2020/02/how-the-japanese-governments-new-sandbox-program-is-testing-innovations-in-mobility-and-technology (accessed on 10 October 2020).
- Medical Big Data to be Pooled for Disease Research and Drug Development in Japan. Available online: https://www.japantimes.co.jp/news/2017/05/15/reference/medical-big-data-pooled-disease-research-drug-development-japan/ (accessed on 10 October 2020).
- Yamaguchi, M.; Inomata, S.; Harada, S.; Matsuzaki, Y.; Kawaguchi, M.; Ujibe, M.; Kishiba, M.; Fujimura, Y.; Kimura, M.; Murata, K.; et al. Establishment of the MID-NET® medical information database network as a reliable and valuable database for drug safety assessments in Japan. Pharmacoepidemiol. Drug Saf. 2019, 28, 1395–1404. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.J. The South Korean health care system. JMAJ 2009, 52, 206–209. [Google Scholar]
- Jin, D.Y. Smartland Korea: Mobile Communication, Culture, and Society; University of Michigan Press: Ann Arbor, MI, USA, 2017. [Google Scholar]
- Nam, D.J.; Kwon, H.W.; Lee, H.; Ahn, E.K. National healthcare service and its big data analytics. Healthc. Inform. Res. 2018, 24, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Hyun, K.R.; Kang, S.; Lee, S. Population aging and healthcare expenditure in Korea. Health Econ. 2016, 25, 1239–1251. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J. The reform of the developmental welfare state in East Asia. Int. J. Soc. Welf. 2009, 18, S12–S21. [Google Scholar] [CrossRef]
- Connect to Care: The Future of Healthcare IT in South Korea. Available online: http://graphics.eiu.com/upload/eb/GESouthKoreaHealthcare.pdf (accessed on 15 June 2020).
- Republic of Korea: Health System Review. Asia Pacific Observatory on Public Health Systems and Policies. Available online: https://apps.searo.who.int/PDS_DOCS/B5326.pdf (accessed on 12 June 2020).
- Chae, Y.M. National Health Information Systems in Korea; Asia Pacific Association for Medical Informatics: Taipei, Taiwan, 2006. [Google Scholar]
- Park, H.; Lee, S.I.; Kim, Y.; Heo, E.Y.; Lee, J.; Park, J.H.; Ha, K. Patients’ perceptions of a health information exchange: A pilot program in South Korea. Int. J. Med. Inform. 2013, 82, 98–107. [Google Scholar] [CrossRef]
- Digital Health South Korea: Market Intelligence Report. Available online: https://www.intralinkgroup.com/getmedia/3153c79b-463d-47c7-84e6-56848c98aab7/Intralink-Report_Life-Sciences_June2019 (accessed on 19 June 2020).
- Yoon, B.C.; Chang, S.W.; Kang, H.; Bae, R.W. Park Adoption of electronic health records in Korean tertiary teaching and general hospitals. Int. J. Med. Inform. 2012, 81, 196–203. [Google Scholar] [CrossRef]
- Act on the Development of Cloud Computing and Protection of its Users. Available online: https://elaw.klri.re.kr/eng_mobile/viewer.do?hseq=35630&type=part&key=43 (accessed on 25 June 2020).
- South Korea to Move 750 e-Government Services to Cloud Computing by 2017 for Improved and Cost-Efficient Public Service. Available online: http://en.koreaportal.com/articles/4349/20151113/south-korea-move-750-e-government-services-cloud-computing-2017.htm (accessed on 5 June 2020).
- Data Standardization. Available online: https://www.ohdsi.org/data-standardization/#:~:text=Data%20standardization%20is%20the%20critical,one%20organization%20to%20the%20next (accessed on 25 September 2020).
- Korea: Cloud in Healthcare Services. Available online: https://www.microsoft.com/en-sg/apac/trustedcloud/korea-healthcare-service.aspx (accessed on 6 June 2020).
- First Look at Cloud-Based Medical Records. Available online: https://media.nature.com/original/magazine-assets/d42473-019-00098-4/d42473-019-00098-4.pdf (accessed on 23 July 2020).
- Clinerion and the P-HIS Development Group of Korea University Medical Center Collaborate. Available online: http://www.appliedclinicaltrialsonline.com/clinerion-and-p-his-development-group-korea-university-medical-center-collaborate (accessed on 5 June 2020).
- Bio-Health Industry to Achieve People-Centered Innovative Growth: Press Release. Available online: http://www.mohw.go.kr/eng/nw/nw0101vw.jsp?PAR_MENU_ID=1007&MENU_ID=100701&page=1&CONT_SEQ=349515 (accessed on 6 June 2020).
- South Korea Commits US$4bn to Bolster Tech Sectors. Available online: https://www.globalgovernmentforum.com/south-korea-commits-us4bn-to-bolster-tech-sectors/ (accessed on 3 July 2020).
- Shum, E.; Lee, C.E. Population-based healthcare: The experience of a regional health system. Ann. Acad. Med. Singap. 2014, 43, 564–565. [Google Scholar]
- Tan, S.Y.; Taeihagh, A. Governing the adoption of robotics and autonomous systems in long-term care in Singapore. Policy Soc. 2020, 1–21. [Google Scholar] [CrossRef]
- Haseltine, W. Affordable Excellence: The Singapore Healthcare Story: How to Create and Manage Sustainable Healthcare Systems; Brookings Institution Press: Washington, DC, USA, 2013. [Google Scholar]
- Current Health Expenditure (% of GDP)—Singapore. Available online: https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS?locations=SG (accessed on 29 July 2020).
- Phua, K.H.; Pocock, N.S. Transforming the ASEAN Economic Community (AEC) into a Global Services Hub: Enhancing the competitiveness of the health services sector in Singapore. In Developing Asean Economic Community (AEC) into a Global Services Hub; ERIA: Jakarta, Indonesia, 2012; pp. 1–63. [Google Scholar]
- Reisman, D.A. Medical savings and medical cost: Healthcare and age in a changing Singapore. Int. J. Sociol. Soc. Policy 2005, 25, 1–26. [Google Scholar] [CrossRef]
- Bai, Y.; Shi, C.; Li, X.; Liu, F. Healthcare System in Singapore; Columbia University: New York, NY, USA, 2012. [Google Scholar]
- Manoharan, A.P.; McQuiston, J. Innovative Perspectives on Public Administration in the Digital Age; IGI Global: Hershey, PA, USA, 2018. [Google Scholar]
- Luk, C.Y. The Impact of Digital Health on Traditional Healthcare Systems and Doctor-Patient Relationships: The case study of Singapore. In Innovative Perspectives on Public Administration in the Digital Age; IGI Global: Hershey, PA, USA, 2018; pp. 143–167. [Google Scholar]
- Milestones. Available online: https://www.ihis.com.sg/About_IHiS/Pages/milestones.aspx (accessed on 15 July 2020).
- H-Cloud. Available online: https://www.ihis.com.sg/Project_Showcase/Healthcare_Systems/Pages/H-Cloud.aspx (accessed on 30 July 2020).
- In Brief: Digital Healthcare in Singapore. Available online: https://www.lexology.com/library/detail.aspx?g=43360ad2-b8c4-4aae-ab66-358155529afa (accessed on 30 July 2020).
- Singapore Healthcare Providers Must Soon Contribute to National Electronic Records. Available online: https://www.zdnet.com/article/singapore-healthcare-providers-must-soon-contribute-to-national-electronic-records/ (accessed on 30 July 2020).
- Singapore Regulatory Update: Healthcare Services Bill. Available online: https://www.twobirds.com/~/media/pdfs/singapore/2020/legal-update-singapore-regulatory-update-january-2020.pdf?la=en&hash=8309B1B3619BC36B24C70804ED8264DA81D069FE (accessed on 27 July 2020).
- Hardcopy Medical Certs will Soon be no More with DigiMC. Available online: https://www.tech.gov.sg/media/technews/hardcopy-medical-certs-will-soon-be-no-more-with-digimc (accessed on 27 July 2020).
- New Healthcare Innovation Centre will Mean Faster Admissions, Better Solutions for Patients. Available online: https://www.todayonline.com/singapore/new-healthcare-innovation-centre-faster-admissions-better-solutions-patients (accessed on 1 August 2020).
- Ng, R. Cloud computing in Singapore: Key drivers and recommendations for a smart nation. Politics Gov. 2018, 6, 39–47. [Google Scholar] [CrossRef]
- Centre for Healthcare Innovation Opens. Available online: https://www.channelnewsasia.com/news/singapore/centre-for-healthcare-innovation-opens-11516444 (accessed on 1 August 2020).
- Licensing Experimentation and Adaptation Programme (LEAP)—A MOH Regulatory Sandbox. Available online: https://www.moh.gov.sg/home/our-healthcare-system/licensing-experimentation-and-adaptation-programme-(leap)-a-moh-regulatory-sandbox (accessed on 1 August 2020).
- Singapore—Government Driven Approach for AI in Healthcare. Available online: https://www.rvo.nl/sites/default/files/2020/11/28%20okt%20Singapore%20-%20Government%20driven%20approach%20for%20AI%20in%20healthcare.pdf (accessed on 2 August 2020).
- Addressing the Challenges of Population Ageing in Asia and the Pacific. Available online: https://www.unescap.org/sites/default/files/publications/Addressing%20the%20Challenges%20of%20Population%20Ageing%20in%20Asia%20and%20the%20Pacific.pdf (accessed on 3 July 2020).
- Japan Agetech: Seize Opportunities in a Growing Market. Available online: https://tokyoesque.com/japan-agetech-healthcare/ (accessed on 23 July 2020).
- Amron, M.T.; Ibrahim, R.; Chuprat, S. A review on cloud computing acceptance factors. Procedia Comput. Sci. 2017, 124, 639–646. [Google Scholar] [CrossRef]
- Parasuraman, A.; Colby, C.L. An updated and streamlined technology readiness index: TRI 2.0. J. Serv. Res. 2015, 18, 59–74. [Google Scholar] [CrossRef]
- Iida, J. Digital transformation vs. COVID-19: The case of Japan. Digit. Law J. 2020, 1, 8–16. [Google Scholar] [CrossRef]
- Cloud Computing in Japan. Available online: https://www.lexology.com/library/detail.aspx?g=42f7c33e-8bb4-4eda-afe3-b06c42a5bf93 (accessed on 12 June 2020).
- Cloud Computing in South Korea. Available online: https://www.lexology.com/library/detail.aspx?g=cbdef3bc-6cd5-46fa-b86e-e1a5f212c8e6 (accessed on 30 June 2020).
- National Telemedicine Guidelines. 2015. Available online: https://www.moh.gov.sg/docs/librariesprovider5/resources-statistics/guidelines/moh-cir-06_2015_30jan15_telemedicine-guidelines-rev.pdf (accessed on 12 August 2020).
- Cybersecurity in Singapore. Available online: https://www.lexology.com/library/detail.aspx?g=14b899f0-e590-4acf-8bfc-d6229590acac (accessed on 12 August 2020).
- Cybersecurity Act. Available online: https://www.csa.gov.sg/legislation/cybersecurity-act (accessed on 23 September 2020).
- Casola, V.; Castiglione, A.; Choo, K.K.; Esposito, C. Healthcare-related data in the cloud: Challenges and opportunities. IEEE Cloud Comput. 2016, 3, 10–14. [Google Scholar] [CrossRef]
- SingPass Mobile App to Become Main Gateway to Access Government Services. Available online: https://opengovasia.com/singpass-mobile-app-to-become-main-gateway-to-access-government-services/ (accessed on 29 August 2020).
- Wolf, L.; Harvell, J.; Jha, A.K. Hospitals ineligible for federal meaningful-use incentives have dismally low rates of adoption of electronic health records. Health Aff. 2012, 31, 505–513. [Google Scholar] [CrossRef]
- Cloud Computing in Singapore. Available online: https://tanthiamhuat.files.wordpress.com/2015/04/cloud-computing-in-singapore-2015-edition.pdf (accessed on 15 August 2020).
- Sánchez-Polo, M.T.; Cegarra-Navarro, J.-G.; Cillo, V.; Wensley, A. Overcoming knowledge barriers to health care through continuous learning. J. Knowl. Manag. 2019, 23, 508–526. [Google Scholar] [CrossRef]
- ‘Korean New Deal’ to Kick Off Telemedicine Platform. Available online: https://www.koreabiomed.com/news/articleView.html?idxno=8756 (accessed on 15 September 2020).
- Lee, T.D.; Park, H.; Lee, J. Collaborative accountability for sustainable public health: A Korean perspective on the effective use of ICT-based health risk communication. Gov. Inf. Q. 2019, 36, 226–236. [Google Scholar] [CrossRef]
- Toward Realization of the New Economy and Society. Available online: http://www.keidanren.or.jp/en/policy/2016/029_outline.pdf (accessed on 2 September 2020).
- Melas, C.D.; Zampetakis, L.A.; Dimopoulou, A.; Moustakis, V.S. An empirical investigation of technology readiness among medical staff based in Greek hospitals. Eur. J. Inf. Syst. 2014, 23, 672–690. [Google Scholar] [CrossRef]
- Leung, L.; Chen, C. E-health/m-health adoption and lifestyle improvements: Exploring the roles of technology readiness, the expectation-confirmation model, and health-related information activities. Telecommun. Policy 2019, 43, 563–575. [Google Scholar] [CrossRef]
- Iyer, E.K.; Krishnan, A.; Sareen, G.; Panda, T. Sectorial adoption analysis of cloud computing by examining the dissatisfier landscape. Electron. J. Inf. Syst. Eval. 2013, 16, 212. [Google Scholar]
- Skills Shortage and Poor IT Infrastructure Hinder Tech Adoption by ASEAN Governments. Available online: https://www.computerweekly.com/news/450300895/Skills-shortage-and-poor-IT-infrastructure-hinder-tech-adoption-by-Asean-governments (accessed on 11 September 2020).
- Alharbi, F. Holistic Approach Framework for Cloud Computing Strategic Decision-Making in the Healthcare Sector (HAF-CCS). Ph.D. Thesis, Staffordshire University, Staffs, UK, 2017. [Google Scholar]
- New Services Realized with the ‘My Number’ System. Available online: https://www.nec.com/en/global/techrep/journal/g14/n01/pdf/140104.pdf (accessed on 8 August 2020).
- Telehealth: Breaking Down Adoption Barriers. Available online: https://www.infosys.com/industries/healthcare/insights/Documents/breaking-down-adoption-barriers.pdf (accessed on 3 October 2020).
- Standardizing Healthcare Terms: Challenges, Benefits and Future. Available online: https://blogs.perficient.com/2019/07/09/standardizing-healthcare-terms-challenges-benefits-future/ (accessed on 3 October 2020).
- Olaronke, I.; Oluwaseun, O. Big data in healthcare: Prospects, challenges and resolutions. In Proceedings of the Future Technologies Conference (FTC) IEEE, San Francisco, CA, USA, 6–7 December 2016; pp. 1152–1157. [Google Scholar]
- Guidelines for De-Identification of Personal Data. Available online: http://www.privacy.go.kr (accessed on 27 July 2020).
- Bhuyan, S.S.; Kabir, U.Y.; Escareno, J.M.; Ector, K.; Palakodeti, S.; Wyant, D.; Kumar, S.; Levy, M.; Kedia, S.; Dasgupta, D.; et al. Transforming healthcare cybersecurity from reactive to proactive: Current status and future recommendations. J. Med. Syst. 2020, 44, 1–9. [Google Scholar] [CrossRef]
- Lian, J.W. Establishing a cloud computing success model for hospitals in Taiwan. INQUIRY 2017, 54, 0046958016685836. [Google Scholar] [CrossRef]
- Masrom, M.; Rahimly, A. Overview of data security issues in hospital information systems. Pac. Asia J. Assoc. Inf. Syst. 2020, 7, 5. [Google Scholar] [CrossRef]
- Arundel, A.; Bloch, C.; Ferguson, B. Advancing innovation in the public sector: Aligning innovation measurement with policy goals. Res. Policy 2019, 48, 789–798. [Google Scholar] [CrossRef]
- The Challenge of Innovating in Government. Available online: http://www.businessofgovernment.org/sites/default/files/BorinsInnovatingInGov.pdf (accessed on 2 October 2020).
- Taeihagh, A. Crowdsourcing, sharing economies and development. J. Dev. Soc. 2017, 33, 191–222. [Google Scholar] [CrossRef]
- Demircioglu, M.A.; Audretsch, D.B. Conditions for innovation in public sector organizations. Res. Policy 2017, 46, 1681–1691. [Google Scholar] [CrossRef]
- Tan, S.Y.; Taeihagh, A. Smart City Governance in Developing Countries: A Systematic Literature Review. Sustainability 2020, 12, 899. [Google Scholar] [CrossRef]
- Cinar, E.; Trott, P.; Simms, C. A systematic review of barriers to public sector innovation process. Public Manag. Rev. 2019, 21, 264–290. [Google Scholar] [CrossRef]
- D’Este, P.; Iammarino, S.; Savona, M.; von Tunzelmann, N. What hampers innovation? Revealed barriers versus deterring barriers. Res. Policy 2012, 41, 482–488. [Google Scholar] [CrossRef]
- Torugsa, N.; Arundel, A. Complexity of innovation in the public sector: A workgroup-level analysis of related factors and outcomes. Public Manag. Rev. 2016, 18, 392–416. [Google Scholar] [CrossRef]
- Arundel, A. Rethinking the effect of risk aversion on the benefits of service innovations in public administration agencies. Res. Policy 2017, 46, 900–910. [Google Scholar]
- Cloud Computing in Asia Is Growing. Pacific Bridge Medical. Available online: https://www.pacificbridgemedical.com/ameing-for-asia/cloud-computing-asia-growing/ (accessed on 27 June 2020).
- Cloud Initiative Helps Promote Health Service. China Daily. Available online: http://www.chinadaily.com.cn/business/2014-07/31/content_18220529.htm (accessed on 28 June 2020).
- National Health Stack: Strategy and Approach. Available online: https://niti.gov.in/writereaddata/files/document_publication/NHS-Strategy-and-Approach-Document-for-consultation.pdf (accessed on 9 December 2020).
- Govt to Implement Electronic Medical Record Structure by Mid-2020. Available online: https://themalaysianreserve.com/2019/10/15/govt-to-implement-electronic-medical-record-structure-by-mid-2020/ (accessed on 6 June 2020).
- Microsoft Thailand: Cloud in Healthcare Services. Available online: https://www.microsoft.com/en-sg/apac/trustedcloud/thailand-healthcare-service.aspx (accessed on 15 May 2020).
- Capano, G.; Howlett, M.; Jarvis, D.S.; Ramesh, M.; Goyal, N. Mobilizing Policy (In) Capacity to Fight COVID-19: Understanding Variations in State Responses. Policy Soc. 2020, 39, 285–308. [Google Scholar] [CrossRef]
- Lee, S.; Hwang, C.; Moon, M.J. Policy learning and crisis policymaking: Quadruple-loop learning and COVID-19 responses in South Korea. Policy Soc. 2020, 39, 363–381. [Google Scholar] [CrossRef]
- How Did Coronavirus Start and where Did it Come from? Was it Really Wuhan’s Animal Market? Available online: https://www.theguardian.com/world/2020/apr/28/how-did-the-coronavirus-start-where-did-it-come-from-how-did-it-spread-humans-was-it-really-bats-pangolins-wuhan-animal-market (accessed on 25 May 2020).
- Tackling the Fallout from the Coronavirus. Available online: https://oecdecoscope.blog/2020/03/02/tackling-the-fallout-from-the-coronavirus/ (accessed on 9 June 2020).
- Comfort, L.; Kapucu, N.; Ko, K.; Menoni, S.; Siciliano, M. Crisis Decision Making on a Global Scale: Transition from Cognition to Collective Action under Threat of COVID-19. Public Adm. Rev. 2020, 80, 616–622. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Pandemic: Humanity Needs Leadership and Solidarity to Defeat the Coronavirus. United Nations Development Programme. Available online: https://www.undp.org/content/undp/en/home/coronavirus.html (accessed on 1 June 2020).
- OGP. Collecting Open Government Approaches to COVID-19. 2020. Available online: https://www.opengovpartnership.org/collecting-open-government-approaches-to-covid-19/ (accessed on 12 October 2020).
- Digital Engagement and Transformation of Healthcare in Singapore. Available online: https://www.healthcareitnews.com/news/asia-pacific/digital-engagement-and-transformation-healthcare-singapore (accessed on 2 October 2020).
- Moon, M.J. Fighting Against COVID-19 with Agility, Transparency, and Participation: Wicked Policy Problems and New Governance Challenges. Public Adm. Rev. 2020, 80, 651–656. [Google Scholar] [CrossRef]
- Google has Opened its Cloud Healthcare API to Allow Doctors to Analyze Data Using Cloud-Computing Technologies. Available online: https://www.zdnet.com/article/google-wants-to-make-it-easier-to-analyse-health-data-in-the-cloud/ (accessed on 10 July 2020).
- The Johns Hopkins Coronavirus Dashboard Gets 1.2 Billion Interactions a Day. Available online: https://nymag.com/intelligencer/2020/04/jhus-coronavirus-site-gets-1-2-billion-interactions-a-day.html (accessed on 10 July 2020).
- With Apps and Remote Medicine, Japan Offers a Glimpse of Doctor Visits in Post-Corona Era. Available online: https://in.reuters.com/article/us-health-coronavirus-japan-telehealth/with-apps-and-remote-medicine-japan-offers-glimpse-of-doctor-visits-in-post-corona-era-idINKBN24A01K (accessed on 1 July 2020).
- Accenture: A New Era for the Healthcare Industry. Available online: https://www.accenture.com/us-en/~/media/Accenture/Conversion-Assets/DotCom/Documents/Global/PDF/Technology_2/Accenture-New-Era-Healthcare-Industry-Cloud-Computing-Changes-Game.pdf (accessed on 10 July 2020).
- Makri, M.; Lane, P.J.; Gomez-Mejia, L.R. CEO incentives, innovation, and performance in technology-intensive firms: A reconciliation of outcome and behavior-based incentive schemes. Strateg. Manag. J. 2006, 27, 1057–1080. [Google Scholar] [CrossRef]
- Roessner, J.D. Incentives to innovate in public and private organizations. Adm. Soc. 1977, 9, 341–365. [Google Scholar] [CrossRef]
- Zandberg, T.; Morales, F.N. Public managers’ networking and innovative work behavior: The importance of career incentives. Int. Rev. Adm. Sci. 2019, 85, 286–303. [Google Scholar] [CrossRef]
- Li, Y.; Taeihagh, A.; De Jong, M. The governance of risks in ridesharing: A revelatory case from Singapore. Energies 2018, 11, 1277. [Google Scholar] [CrossRef]
- Acs, Z.J.; Audretsch, D.B.; Lehmann, E.E.; Licht, G. National systems of innovation. J. Technol. Transfer. 2017, 42, 997–1008. [Google Scholar] [CrossRef]
- Demircioglu, M.A. Why does innovation in government occur and persist? Evidence from the Australian government. Asia Pac. J. Public Adm. 2019, 41, 217–229. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Japan | South Korea | Singapore |
|---|---|---|---|
| 1961 | National Health Insurance system completed | ||
| 1977 | Standardization and automation of medical claims processing in 1970s | National Health Insurance Act | |
| 1983 | National Health Plan | ||
| 1989 | Development of electronic health records (EHRs) in 1980s | National Health Insurance Service | MediNet |
| 1990 | Development of medical markup language (MML) in 1990s | 10-year Information Strategy Plan for NHIS | Central Claims Processing System Physician Data Query System for Cancer |
| 1994 | National Patient Master Index (NPMI) | ||
| 2001 | E-Japan Strategy Grand Design for Informatization of Healthcare Field | Second 10-year Information Strategy Plan Medical Services Act | |
| 2003 | E-Japan Strategy 2 Electronic medical records (EMR) systems defined | Electronic medical records legalized Centre for Interoperable Electronic Health Records | Singapore Personal Access (SingPass) Electronic Medical Record Exchange (EMRX) |
| 2005 | EMRX data expanded | ||
| 2006 | New IT reform strategy | NPMI migrated to Critical Medical Information Store EMRX data expanded | |
| 2007 | Grand design for information utilization in medical care, healthcare, long-term care, and welfare sectors | 3-year Health Information Exchange (HIE) Program pilot | EMRX expanded to community hospitals |
| 2008 | Concept of U-Health emerged | ||
| 2009 | i-Japan Strategy 2015 launched National Database of Health Insurance Claims and Specific Health Checkups of Japan | HIE updated with needs of private sector addressed | National Electronic Health Record (NEHR) initiated |
| 2010 | A New Strategy in Information and Communications Technology | NEHR conceptualized Centre for Healthcare Innovation (CHI) conceptualized | |
| 2011 | Personal Information Protection Act (PIPA) enacted | NEHR officially launched | |
| 2012 | Personal Data Protection Act (PDPA) enacted | ||
| 2013 | Declaration to be the World’s Most Advanced IT Nation Japan Revitalization Strategy Social Society and Tax Number (SSTN) System was established | Genome Technology to Business Translation Program | CHI finalized |
| 2014 | Healthcare New Frontier (HCNF) policy package Revision of Personal Data Protection Law Committee to decide on the use of SSTN System in healthcare | Application of the PDPA for the healthcare sector H-Cloud launched | |
| 2015 | Japan Revitalization Strategy Updated Working group on information and technology usage in the area of healthcare The Japan Vision: Health Care 2035 Data Health Project launched | ME-BYO registered as a trademark Cloud Computing Act passed Ministry of Science, Information and Communications Technology and Future Planning (MSIP) announced plans to move over 400 e-government services to the cloud | Information Protection Measures for Vitalization of Cloud Services announced Health data from across hospitals migrated to the H-Cloud |
| 2016 | Japan Revitalization Strategy Updated Person-centered Open Platform for Wellbeing (PeOPLe) started Healthcare Business Contest by METI | Guidelines for the De-Identification of Personal Information (GDPI) MSIP to move 350 more e-government services to the cloud | IHIS standardized applications across health clusters HealthHub launched |
| 2017 | Medical Big Data Law Next Generation Medical Infrastructure Law passed Administrative reform promotion office for health data Medical Innovation Support Office Healthcare Innovation Hub ME-BYO included in Healthcare Policy Personal Information Protection Act | Precision Medicine Hospital Information System (P-HIS) launched | Smart Health Video Consultation (SHVC) implemented |
| 2018 | Next Generation Medical Infrastructure Law comes into force Medical Information Database Network (MID-NET) Japan Healthcare Innovation Policy (draft) Sandbox framework to promote health innovations | FEEDER-NET announced Common Data Module (CDM) implemented Government announced a plan to build a national database of genetic and biometric data | Cyberattack on SingHealth Licensing Experimentation and Adaptation Programme Personal Data Protection Commission (PDPC) established |
| 2019 | 2019 Growth Strategy | Innovative Strategy on the Bio-health Industry | DigiMC launched CHI launched CHI Learning and Development (CHILD) system launched |
| 2020 | PeOPLe expected to be completed Declaration regarding Creation of World’s Most Advanced Digital Nation | Digital New Deal policy | Healthcare Services Bill passed |
| Drivers for Cloud Adoption in Healthcare |
|---|
|
| Barriers to Cloud Adoption in Healthcare |
|---|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raghavan, A.; Demircioglu, M.A.; Taeihagh, A. Public Health Innovation through Cloud Adoption: A Comparative Analysis of Drivers and Barriers in Japan, South Korea, and Singapore. Int. J. Environ. Res. Public Health 2021, 18, 334. https://doi.org/10.3390/ijerph18010334
Raghavan A, Demircioglu MA, Taeihagh A. Public Health Innovation through Cloud Adoption: A Comparative Analysis of Drivers and Barriers in Japan, South Korea, and Singapore. International Journal of Environmental Research and Public Health. 2021; 18(1):334. https://doi.org/10.3390/ijerph18010334
Chicago/Turabian StyleRaghavan, Aarthi, Mehmet Akif Demircioglu, and Araz Taeihagh. 2021. "Public Health Innovation through Cloud Adoption: A Comparative Analysis of Drivers and Barriers in Japan, South Korea, and Singapore" International Journal of Environmental Research and Public Health 18, no. 1: 334. https://doi.org/10.3390/ijerph18010334
APA StyleRaghavan, A., Demircioglu, M. A., & Taeihagh, A. (2021). Public Health Innovation through Cloud Adoption: A Comparative Analysis of Drivers and Barriers in Japan, South Korea, and Singapore. International Journal of Environmental Research and Public Health, 18(1), 334. https://doi.org/10.3390/ijerph18010334