Oral Health Attitudes among Preclinical and Clinical Dental Students: A Pilot Study and Self-Assessment in an Egyptian State-Funded University





Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Methodology
2.2. Calculation of Sample Size
2.3. Scores and Statistical Analysis of the Hiroshima University-Dental Behavioural Inventory
3. Results
3.1. Oral Health Attitudes
3.2. Oral Health Behaviour and Self-Reported Oral Health
3.3. Mean HU-DBI Scores and Statistical Significance
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Peres, M.A.; Daly, B.; Guarnizo-Herreño, C.C.; Benzian, H.; Watt, R.G. Oral diseases: A global public health challenge—Authors’ reply. Lancet 2020, 395, 186–187. [Google Scholar] [CrossRef]
- Menegaz, A.M.; Silva, A.E.R.; Cascaes, A.M. Educational interventions in health services and oral health: Systematic review. Rev. Saúde Pública 2018, 52, 52. [Google Scholar] [CrossRef] [PubMed]
- Mekhemar, M.; Conrad, J.; Attia, S.; Dorfer, C. Oral Health Attitudes among Preclinical and Clinical Dental Students in Germany. Int. J. Environ. Res. Public Health 2020, 17, 4253. [Google Scholar] [CrossRef] [PubMed]
- Radovich, E.; El-Shitany, A.; Sholkamy, H.; Benova, L. Rising up: Fertility trends in Egypt before and after the revolution. PLoS ONE 2018, 13, e0190148. [Google Scholar] [CrossRef]
- United Nations. United Nations Demographic Yearbook 2018; United Nations Publications: New York, NY, USA, 2019. [Google Scholar] [CrossRef]
- Moussa, A.; Ibrahim, E.; Esmat, A.; Eissa, S.; Ramzy, M. An overview of oral health status, socio-economic and behavioral risk factors, and the pattern of tooth loss in a sample of Egyptian rural population. Bull. Natl. Res. Cent. 2020, 44, 16. [Google Scholar] [CrossRef]
- Seif El-Nasr, E. Oral health intervention program among primary school children at El-Qalyubia Governorate. Egypt. Nurs. J. 2017, 14, 100–108. [Google Scholar] [CrossRef]
- Aly, N.M.; Mohamed, A.A.; Abdelaziz, W.E. Parenting practices and oral health status in rural areas in Egypt: A household survey. BMC Oral Health 2020, 20, 134. [Google Scholar] [CrossRef]
- Abdelaziz, A.; Kassab, S.E.; Abdelnasser, A.; Hosny, S. Medical Education in Egypt: Historical Background, Current Status, and Challenges. Health Prof. Educ. 2018, 4, 236–244. [Google Scholar] [CrossRef]
- Barnard, H. Medical education in Egypt. Ned. Tijdschr. Geneeskd. 2002, 146, 1147–1149. [Google Scholar]
- Serrano, C.M.; Botelho, M.G.; Wesselink, P.R.; Vervoorn, J.M. Challenges in the transition to clinical training in dentistry: An ADEE special interest group initial report. Eur. J. Dent. Educ. 2018, 22, e451–e457. [Google Scholar] [CrossRef]
- Yildiz, S.; Dogan, B. Self reported dental health attitudes and behaviour of dental students in Turkey. Eur. J. Dent. 2011, 5, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Al-wesabi, A.A.; Abdelgawad, F.; Sasahara, H.; El Motayam, K. Oral health knowledge, attitude and behaviour of dental students in a private university. BDJ Open 2019, 5, 16. [Google Scholar] [CrossRef] [PubMed]
- Alam Moheet, I.; Farooq, I. Self-reported differences between oral health attitudes of pre-clinical and clinical students at a dental teaching institute in Saudi Arabia. Saudi Dent. J. 2013, 25, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Ahamed, S.; Moyin, S.; Punathil, S.; Patil, N.A.; Kale, V.T.; Pawar, G. Evaluation of the Oral Health Knowledge, Attitude and Behavior of the Preclinical and Clinical Dental Students. J. Int. Oral Health 2015, 7, 65–70. [Google Scholar] [PubMed]
- Badovinac, A.; Božić, D.; Vučinac, I.; Vešligaj, J.; Vražić, D.; Plancak, D. Oral health attitudes and behavior of dental students at the University of Zagreb, Croatia. J. Dent. Educ. 2013, 77, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Peker, K.; Uysal, O.; Bermek, G. Dental training and changes in oral health attitudes and behaviors in Istanbul dental students. J. Dent. Educ. 2010, 74, 1017–1023. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Camino, J.; Oyakawa, H.R.; Rodriguez, L.; Tong, L.; Ahn, C.; Bird, W.F.; Komabayashi, T. Effect of dental education on Peruvian dental students’ oral health-related attitudes and behavior. J. Dent. Educ. 2013, 77, 1179–1184. [Google Scholar] [CrossRef]
- Muthu, J.; Priyadarshini, G.; Muthanandam, S.; Ravichndran, S.; Balu, P. Evaluation of oral health attitude and behavior among a group of dental students in Puducherry, India: A preliminary cross-sectional study. J. Indian Soc. Periodontol. 2015, 19, 683–686. [Google Scholar] [CrossRef]
- Ali, D.A. Assessment of oral health attitudes and behavior among students of Kuwait University Health Sciences Center. J. Int. Soc. Prev. Community Dent. 2016, 6, 436–446. [Google Scholar] [CrossRef]
- Komabayashi, T.; Kawamura, M.; Kim, K.-J.; Wright, F.A.C.; Declerck, D.; Goiâs, M.d.C.M.F.; Hu, D.-Y.; Honkala, E.; Lévy, G.; Kalwitzki, M.; et al. The hierarchical cluster analysis of oral health attitudes and behaviour using the Hiroshima University—Dental Behavioural Inventory (HU-DBI) among final year dental students in 17 countries. Int. Dent. J. 2006, 56, 310–316. [Google Scholar] [CrossRef]
- Viechtbauer, W.; Smits, L.; Kotz, D.; Budé, L.; Spigt, M.; Serroyen, J.; Crutzen, R. A simple formula for the calculation of sample size in pilot studies. J. Clin. Epidemiol. 2015, 68, 1375–1379. [Google Scholar] [CrossRef] [PubMed]
- Jaramillo, J.A.; Jaramillo, F.; Kador, I.; Masuoka, D.; Tong, L.; Ahn, C.; Komabayashi, T. A comparative study of oral health attitudes and behavior using the Hiroshima University-Dental Behavioral Inventory (HU-DBI) between dental and civil engineering students in Colombia. J. Oral Sci. 2013, 55, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Alrmaly, B.; Assery, M. Need of oral health promotion through schools among developing countries. J. Int. Oral Health 2018, 10, 1–3. [Google Scholar] [CrossRef]
- Abbass, M.M.S.; Mahmoud, S.A.; El Moshy, S.; Rady, D.; AbuBakr, N.; Radwan, I.A.; Ahmed, A.; Abdou, A.; Al Jawaldeh, A. The prevalence of dental caries among Egyptian children and adolescences and its association with age, socioeconomic status, dietary habits and other risk factors. A cross-sectional study. F1000Res 2019, 8, 8. [Google Scholar] [CrossRef] [PubMed]
- Abbass, M.M.S.; Rady, D.; Radwan, I.A.; El Moshy, S.; AbuBakr, N.; Ramadan, M.; Yussif, N.; Al Jawaldeh, A. The occurrence of periodontal diseases and its correlation with different risk factors among a convenient sample of adult Egyptian population: A cross-sectional study. F1000Res 2019, 8, 1740. [Google Scholar] [CrossRef]
- Eid, S.A.; Khattab, N.M.A.; Elheeny, A.A.H. Untreated dental caries prevalence and impact on the quality of life among 11 to14-year-old Egyptian schoolchildren: A cross-sectional study. BMC Oral Health 2020, 20, 83. [Google Scholar] [CrossRef]
- Haslach, S.D.; Aytepe, Z.; Kokkari, A.; Azrak, B.; Ehlers, V.; Herz, M.M.; Jerg-Bretzke, L.; Geibel, M.-A. Country and gender differences in the motivation of dental students—An international comparison. Eur. J. Dent. Educ. 2018, 22, e724–e729. [Google Scholar] [CrossRef]
- Zaghloul, N.M.; Megahed, H.M. A descriptive medico-legal study of female deaths in cairo governorate, Egypt. J. Forensic Leg. Med. 2019, 66, 25–32. [Google Scholar] [CrossRef]
- El Ansari, W.; Labeeb, S.; Moseley, L.; Kotb, S.; El-Houfy, A. Physical and Psychological Well-being of University Students: Survey of Eleven Faculties in Egypt. Int. J. Prev. Med. 2013, 4, 293–310. [Google Scholar]
- Almutairi, K.M.; Alonazi, W.B.; Vinluan, J.M.; Almigbal, T.H.; Batais, M.A.; Alodhayani, A.A.; Alsadhan, N.; Tumala, R.B.; Moussa, M.; Aboshaiqah, A.E.; et al. Health promoting lifestyle of university students in Saudi Arabia: A cross-sectional assessment. BMC Public Health 2018, 18, 1093. [Google Scholar] [CrossRef]
- Halboub, E.S.; Al-Maweri, S.A.; Al-Jamaei, A.A.; Al-Wesabi, M.A.; Shamala, A.; Al-Kamel, A.; Alsharani, A.; Eissa, N. Self-Reported Oral Health Attitudes and Behavior of Dental and Medical students, Yemen. Glob. J. Health Sci. 2016, 8, 56676. [Google Scholar] [CrossRef] [PubMed]
- Hamasha, A.A.-H.; Alshehri, A.; Alshubaiki, A.; Alssafi, F.; Alamam, H.; Alshunaiber, R. Gender-specific oral health beliefs and behaviors among adult patients attending King Abdulaziz Medical City in Riyadh. Saudi Dent. J. 2018, 30, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Mamai-Homata, E.; Koletsi-Kounari, H.; Margaritis, V. Gender differences in oral health status and behavior of Greek dental students: A meta-analysis of 1981, 2000, and 2010 data. J. Int. Soc. Prev. Community Dent. 2016, 6, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Komabayashi, T.; Kwan, S.Y.L.; Hu, D.-Y.; Kajiwara, K.; Sasahara, H.; Kawamura, M. A comparative study of oral health attitudes and behaviour using the Hiroshima University—Dental Behavioural Inventory (HU-DBI) between dental students in Britain and China. J. Oral Sci. 2005, 47, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Benova, L.; Campbell, O.M.; Ploubidis, G.B. Socio-economic inequalities in curative health-seeking for children in Egypt: Analysis of the 2008 Demographic and Health Survey. BMC Health Serv. Res. 2015, 15, 482. [Google Scholar] [CrossRef] [PubMed]
- Pacauskiene, I.M.; Smailiene, D.; Siudikienė, J.; Savanevskyte, J.; Nedzelskiene, I. Self-reported oral health behavior and attitudes of dental and technology students in Lithuania. Stomatologija 2014, 16, 65–71. [Google Scholar] [PubMed]
- Macfarlane, T.V.; Kawecki, M.M.; Cunningham, C.; Bovaird, I.; Morgan, R.; Rhodes, K.; Watkins, R. Mouthwash use in general population: Results from adult dental health survey in grampian, Scotland. J. Oral Maxillofac. Res. 2011, 1, e2. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.M.C.d.; Borges, A.R.; Ezequiel, O.d.S.; Lucchetti, A.L.G.; Lucchetti, G. Comparison of students motivation at different phases of medical school. Rev. Assoc. Méd. Bras. 2018, 64, 902–908. [Google Scholar] [CrossRef]
- Komar, K.; Glavina, A.; Boras, V.V.; Verzak, Ž.; Brailo, V. Impact of Smoking on Oral Health: Knowledge and Attitudes of Croatian Dentists and Dental Students. Acta Stomatol. Croat. 2018, 52, 148–155. [Google Scholar] [CrossRef]
- Mitra, D.; Pawar, S.; Mandal, A.; Shah, R.; Rodrigues, S.; Desai, A.; Pathare, P.; Shingnapurkar, S.; Vijayakar, H. Attitudes of dental professionals toward tobacco use. J. Indian Soc. Periodontol. 2015, 19, 317–321. [Google Scholar] [CrossRef]
- World Health, O. WHO Report on the Global Tobacco Epidemic, 2013: Enforcing Bans on Tobacco Advertising, Promotion and Sponsorship; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Khan, A.A.; Dey, S.; Taha, A.H.; Huq, F.S.; Moussawi, A.H.; Omar, O.S.; Soliman, A.S. Attitudes of Cairo University medical students toward smoking: The need for tobacco control programs in medical education. J. Egypt. Public Health Assoc. 2012, 87, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.R.; Leggat, P.A. An international review of tobacco smoking among dental students in 19 countries. Int. Dent. J. 2007, 57, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Fujita, Y.; Maki, K. Associations of smoking behavior with lifestyle and mental health among Japanese dental students. BMC Med. Educ. 2018, 18, 264. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.; Kumar, R.V.; Akhil, S.; Saji, A.M.; Iype, A.K.; Antony, D. Prevalence of smoking among dental students and gauging their knowledge about tobacco cessation methods: An original study. J. Fam. Med. Prim. Care 2019, 8, 1562–1566. [Google Scholar] [CrossRef]
- Balogh, E.; Faubl, N.; Riemenschneider, H.; Balázs, P.; Bergmann, A.; Cseh, K.; Horváth, F.; Schelling, J.; Terebessy, A.; Wagner, Z.; et al. Cigarette, waterpipe and e-cigarette use among an international sample of medical students. Cross-sectional multicenter study in Germany and Hungary. BMC Public Health 2018, 18, 591. [Google Scholar] [CrossRef]
- Gignon, M.; Havet, E.; Ammirati, C.; Traullé, S.; Manaouil, C.; Balcaen, T.; Loas, G.; Dubois, G.; Ganry, O. Alcohol, cigarette, and illegal substance consumption among medical students: A cross-sectional survey. Workplace Health Saf. 2015, 63, 54–63. [Google Scholar] [CrossRef]
- Sharareh, P.; Leili, T.; Abbas, M.; Jalal, P.; Ali, G. Determining correlates of the average number of cigarette smoking among college students using count regression models. Sci. Rep. 2020, 10, 8874. [Google Scholar] [CrossRef]
- Shaik, P.; Pachava, S.; Palli, C. Factors affecting stress among students in dental colleges of neo-capital state in India. J. Indian Assoc. Public Health Dent. 2019, 17, 41–47. [Google Scholar] [CrossRef]
- Monteiro, N.M.; Balogun, S.K.; Oratile, K.N. Managing stress: The influence of gender, age and emotion regulation on coping among university students in Botswana. Int. J. Adolesc. Youth 2014, 19, 153–173. [Google Scholar] [CrossRef]
- Basudan, S.; Binanzan, N.; Alhassan, A. Depression, anxiety and stress in dental students. Int. J. Med. Educ. 2017, 8, 179–186. [Google Scholar] [CrossRef]
- Ersan, N.; Dolekoglu, S.; Fisekcioglu, E.; Ilguy, M.; Oktay, I. Perceived sources and levels of stress, general self-efficacy and coping strategies in preclinical dental students. Psychol. Health Med. 2018, 23, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Ravishankar, T.L.; Ain, T.S.; Gowhar, O. Effect of academic stress on plaque and gingival health among dental students of Moradabad, India. J. Int. Acad. Periodontol. 2014, 16, 115–120. [Google Scholar] [PubMed]
- Yamane-Takeuchi, M.; Ekuni, D.; Mizutani, S.; Kataoka, K.; Taniguchi-Tabata, A.; Azuma, T.; Furuta, M.; Tomofuji, T.; Iwasaki, Y.; Morita, M. Associations among oral health-related quality of life, subjective symptoms, clinical status, and self-rated oral health in Japanese university students: A cross-sectional study. BMC Oral Health 2016, 16, 127. [Google Scholar] [CrossRef] [PubMed]
- Balaji, N.K.; Murthy, P.S.; Kumar, D.N.; Chaudhury, S. Perceived stress, anxiety, and coping states in medical and engineering students during examinations. Ind. Psychiatry J. 2019, 28, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Halboub, E.; Alhajj, M.N.; AlKhairat, A.M.; Sahaqi, A.M.; Quadri, M.F.A. Perceived Stress among Undergraduate Dental Students in Relation to Gender, Clinical Training and Academic Performance. Acta Stomatol. Croat. 2018, 52, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Al-Zarea, B.K. Oral Health Knowledge of Periodontal Disease among University Students. Int. J. Dent. 2013, 2013, 647397. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Gupta, G.; Thomas, B.; Bhat, K.M.; Bhat, G.S. Stress and periodontal disease: The link and logic!! Ind. Psychiatry J. 2013, 22, 4–11. [Google Scholar] [CrossRef]
- Arowojolu, M.O.; Onyeaso, C.O.; Dosumu, E.B.; Idaboh, G.K. Effect of academic stress on periodontal health in Nigerians. Odontostomatol. Trop. 2006, 29, 9–13. [Google Scholar]
- Elani, H.W.; Allison, P.J.; Kumar, R.A.; Mancini, L.; Lambrou, A.; Bedos, C. A systematic review of stress in dental students. J. Dent. Educ. 2014, 78, 226–242. [Google Scholar] [CrossRef]
- Bourgeois, D.; Saliasi, I.; Dussart, C.; Llodra, J.C.; Tardivo, D.; Laforest, L.; Bravo, M.; Viennot, S.; Foti, B.; Carrouel, F. Educational outcomes of a new curriculum on interproximal oral prophylaxis for dental students. PLoS ONE 2018, 13, e0204564. [Google Scholar] [CrossRef]
- Park, S.E.; Donoff, R.B.; Saldana, F. The Impact of Integrating Oral Health Education into a Medical Curriculum. Med. Princ. Pract. 2017, 26, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Neville, P.; Zahra, J.; Pilch, K.; Jayawardena, D.; Waylen, A. The behavioural and social sciences as hidden curriculum in UK dental education: A qualitative study. Eur. J. Dent. Educ. 2019, 23, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Conrad, J.; Retelsdorf, J.; Attia, S.; Dörfer, C.; Mekhemar, M. German Dentists’ Preferences for the Treatment of Apical Periodontitis: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 7447. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Item 1 | I live with my family now | Agree | Disagree |
| Item 2 | I had been to a dentist office before | Agree (C) | Disagree |
| Item 3 | I do not go to the dentist unless I feel pain | Agree | Disagree (C) |
| Item 4 | I brush my teeth at least twice a day | Agree (C) | Disagree |
| Item 5 | I brush my teeth after every meal | Agree (C) | Disagree |
| Item 6 | My gums bleed when I brush my teeth | Agree | Disagree (C) |
| Item 7 | I have been taught a professional brushing technique and I use it | Agree (C) | Disagree |
| Item 8 | I use a toothbrush with hard bristles | Agree | Disagree (C) |
| Item 9 | I brush each of my teeth carefully | Agree (C) | Disagree |
| Item10 | I think my teeth are getting worse despite my daily brushing | Agree | Disagree (C) |
| Item 11 | I use dental floss regularly | Agree (C) | Disagree |
| Item 12 | I use a mouthwash regularly | Agree (C) | Disagree |
| Item 13 | I worry about having bad breath | Agree (C) | Disagree |
| Item 14 | I think I can clean my teeth without toothpaste | Agree | Disagree (C) |
| Item 15 | I am bothered by the colour of my gums | Agree | Disagree (C) |
| Item 16 | I worry about the colour of my teeth | Agree (C) | Disagree |
| Item 17 | I am a smoker | Agree | Disagree (C) |
| Item 18 | I smoke 10 or more cigarettes a day | Agree | Disagree (C) |
| Item 19 | I have been smoking for a year or more | Agree | Disagree (C) |
| Item 20 | I like snacking on sweets during the day | Agree | Disagree (C) |
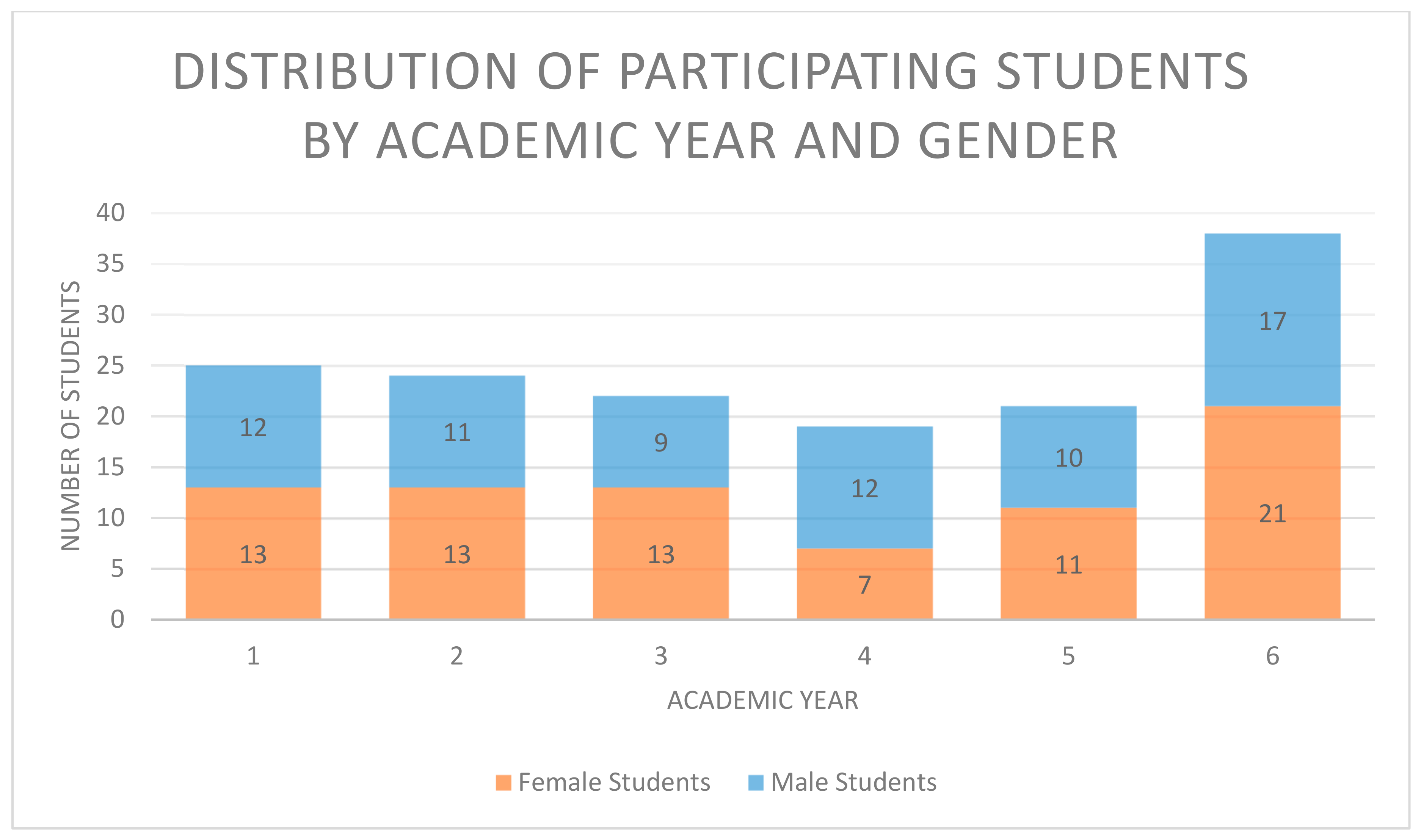
| Academic Year (AY) | Total Number of Students (%) | Female Students (%) | Male Students (%) |
|---|---|---|---|
| 1 | 25 (16.8) | 13 (16.7) | 12 (16.9) |
| 2 | 24 (16.1) | 13 (16.7) | 11 (15.5) |
| 3 | 22 (14.8) | 13 (16.7) | 9 (12.7) |
| 4 | 19 (12.8) | 7 (9.0) | 12 (16.9) |
| 5 | 21 (14.1) | 11 (14.1) | 10 (14.1) |
| 6 | 38 (25.5) | 21 (26.9) | 17 (23.9) |
| Total number | 149 (100) | 78 (100) | 71 (100) |
| Study Phase | Total Number of Students (%) | Female Students (%) | Male Students (%) |
|---|---|---|---|
| Preclinical (AY 1–3) | 71 (47.7) | 39 (54.9) | 32 (45.1) |
| Clinical (AY 3–6) | 78 (52.3) | 39 (50.0) | 39 (50.0) |
| Total number | 149 (100) | 78 (52.3) | 71 (47.7) |
| Item Number and “Keyword” | Number of Responses Favouring Correct Oral Health (%) | Number of Responses Contradicting Correct Oral Health (%) | p-Value | ||
|---|---|---|---|---|---|
| Preclinical | Clinical | Preclinical | Clinical | ||
| 1 “Living with family” (sociodemographic) (For statistical analysis, correct answers were matched with “agree” and incorrect answers with “disagree”) | 54 (76.1) | 61 (78.2) | 17 (23.9) | 17 (21.8) | 0.76 |
| 2 “Visits to the dentist” (OHA) | 47 (66.2) | 56 (71.8) | 24 (33.8) | 22 (28.2) | 0.46 |
| 3 “Visiting the dentist only when in pain” (OHA) | 32 (45.1) | 41 (52.6) | 39 (54.9) | 37 (47.4) | 0.36 |
| 4 “Toothbrushing twice a day” (OHB) | 44 (62.0) | 52 (66.7) | 27 (38.0) | 26 (33.3) | 0.55 |
| 5 “Brushing after every meal” (OHB) | 29 (40.8) | 41 (52.6) | 42 (59.2) | 37 (47.4) | 0.15 |
| 6 “Bleeding gums when brushing” (OHB) | 40 (56.3) | 50 (64.1) | 31 (43.7) | 28 (35.9) | 0.33 |
| 7 “Professional brushing technique” (OHB) | 40 (56.3) | 49 (62.8) | 31 (43.7) | 29 (38.2) | 0.42 |
| 8 “Toothbrush with hard bristles” (OHB) | 37 (52.1) | 51 (65.4) | 34 (47.9) | 27 (34.6) | 0.10 |
| 9 “Brushing each tooth” (OHB) | 40 (56.3) | 50 (64.1) | 31 (43.7) | 28 (35.9) | 0.34 |
| 10 “Teeth get worse despite brushing” (OHB) | 32 (45.1) | 39 (50.0) | 39 (54.9) | 39 (50.0) | 0.55 |
| 11 “Regular dental floss” (OHB) | 29 (40.8) | 41 (52.6) | 42 (59.2) | 37 (47.4) | 0.15 |
| 12 “Regular mouth wash” (OHB) | 35 (49.3) | 34 (43.6) | 36 (50.7) | 44 (56.4) | 0.49 |
| 13 “Worrying about bad breath” (OHA) | 53 (74.6) | 57 (73.1) | 18 (25.4) | 21 (26.9) | 0.83 |
| 14 “Tooth cleaning without toothpaste” (OHA) | 36 (50.7) | 40 (51.3) | 35 (49.3) | 38 (48.7) | 0.94 |
| 15 “Bothered by the colour of gums” (OHB) | 27 (38.0) | 44 (56.4) | 44 (62.0) | 34 (43.6) | 0.03 |
| 16 “Worrying about the colour of teeth” (OHA) | 51 (71.8) | 51 (65.4) | 20 (28.2) | 27 (34.6) | 0.40 |
| 17 “Smoker” (OHB) | 49 (69.0) | 56 (71.8) | 22 (31.0) | 22 (28.2) | 0.71 |
| 18 “10 or more cigarettes a day” (OHB) | 58 (81.7) | 64 (82.1) | 13 (18.3) | 14 (17.9) | 0.96 |
| 19 “Smoking for a year or more” (OHB) | 54 (76.1) | 61 (78.2) | 17 (23.9) | 17 (21.8) | 0.76 |
| 20 “Snacking on sweets during day” (OHB) | 22 (31.0) | 20 (25.6) | 49 (69.0) | 58 (74.4) | 0.47 |
| HU-DBI score | Preclinical Students | Clinical Students | p-Value |
| 10.63 ± 2.64 | 11.50 ± 3.25 | 0.03 | |
| Female Students | Male Students | p-Value | |
| 11.76 ± 2.79 | 10.35 ± 3.06 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mekhemar, M.; Ebeid, K.; Attia, S.; Dörfer, C.; Conrad, J. Oral Health Attitudes among Preclinical and Clinical Dental Students: A Pilot Study and Self-Assessment in an Egyptian State-Funded University. Int. J. Environ. Res. Public Health 2021, 18, 234. https://doi.org/10.3390/ijerph18010234
Mekhemar M, Ebeid K, Attia S, Dörfer C, Conrad J. Oral Health Attitudes among Preclinical and Clinical Dental Students: A Pilot Study and Self-Assessment in an Egyptian State-Funded University. International Journal of Environmental Research and Public Health. 2021; 18(1):234. https://doi.org/10.3390/ijerph18010234
Chicago/Turabian StyleMekhemar, Mohamed, Kamal Ebeid, Sameh Attia, Christof Dörfer, and Jonas Conrad. 2021. "Oral Health Attitudes among Preclinical and Clinical Dental Students: A Pilot Study and Self-Assessment in an Egyptian State-Funded University" International Journal of Environmental Research and Public Health 18, no. 1: 234. https://doi.org/10.3390/ijerph18010234
APA StyleMekhemar, M., Ebeid, K., Attia, S., Dörfer, C., & Conrad, J. (2021). Oral Health Attitudes among Preclinical and Clinical Dental Students: A Pilot Study and Self-Assessment in an Egyptian State-Funded University. International Journal of Environmental Research and Public Health, 18(1), 234. https://doi.org/10.3390/ijerph18010234