Dental Hygienists’ Practice in Perioperative Oral Care Management According to the Japanese Dental Hygienists Survey 2019

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Survey Method
2.2. Questionnaire
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Dental Hygienists Implementing Perioperative Oral Care Management
3.2. Descriptive Statistics of the Items Investigated in This Study
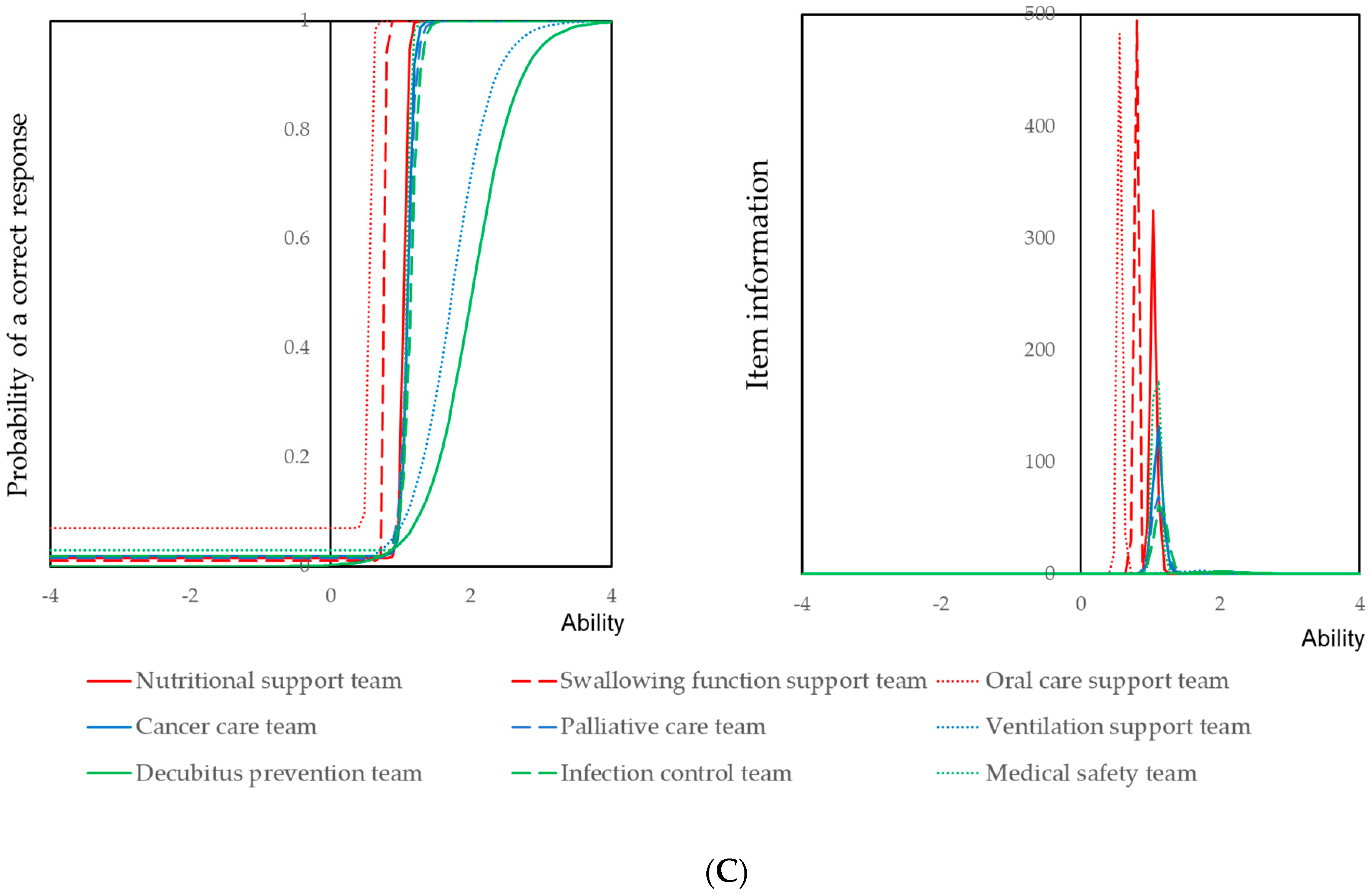
3.3. Item Response Analysis of the Items Concerning Perioperative Oral Management
3.4. Self-Assessed Effects of Perioperative Oral Care Management
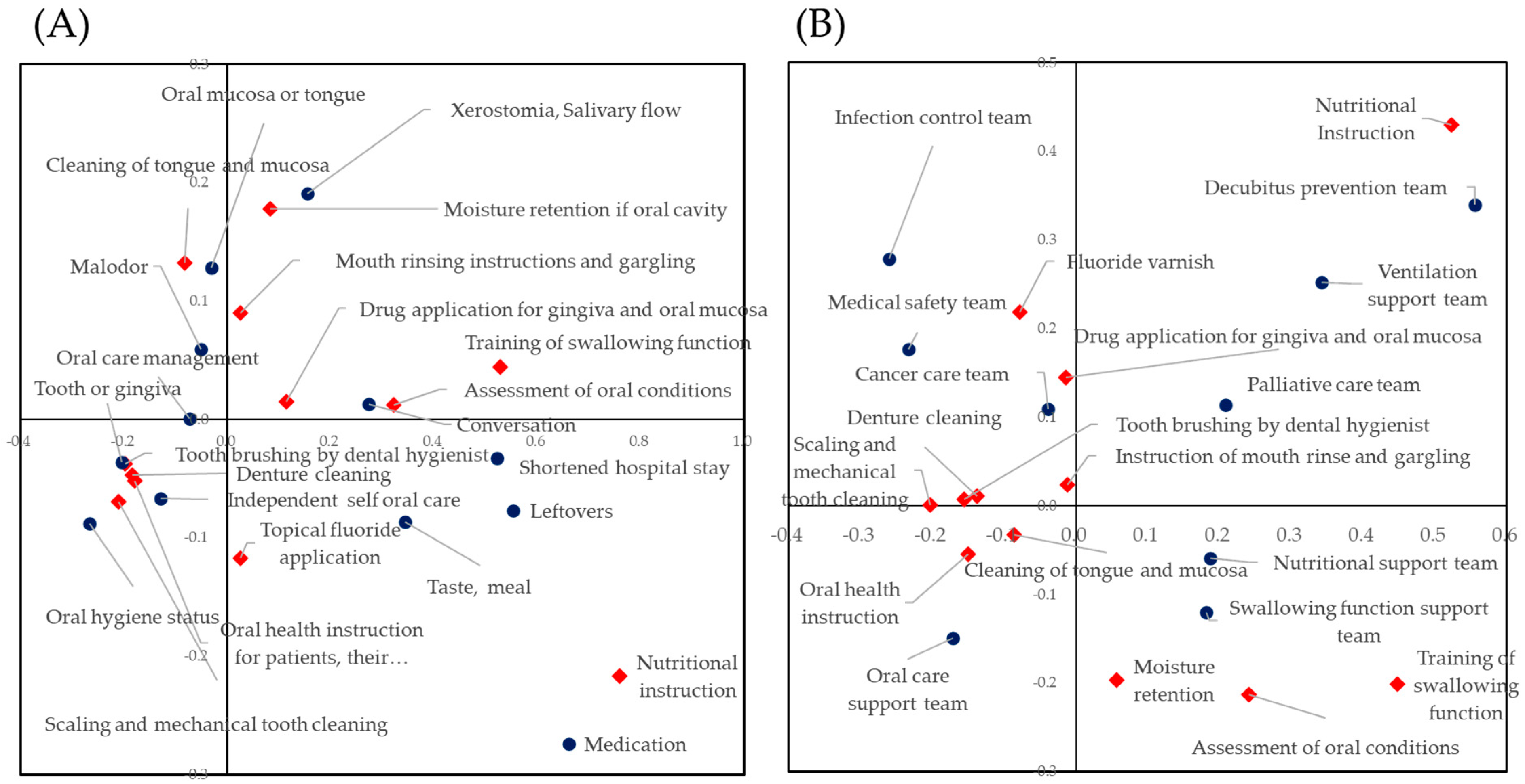
3.5. Correlations between Treatments of Perioperative Oral Care Management, Self-Assessed Perioperative Oral Care Management and Participation in a Medical Team
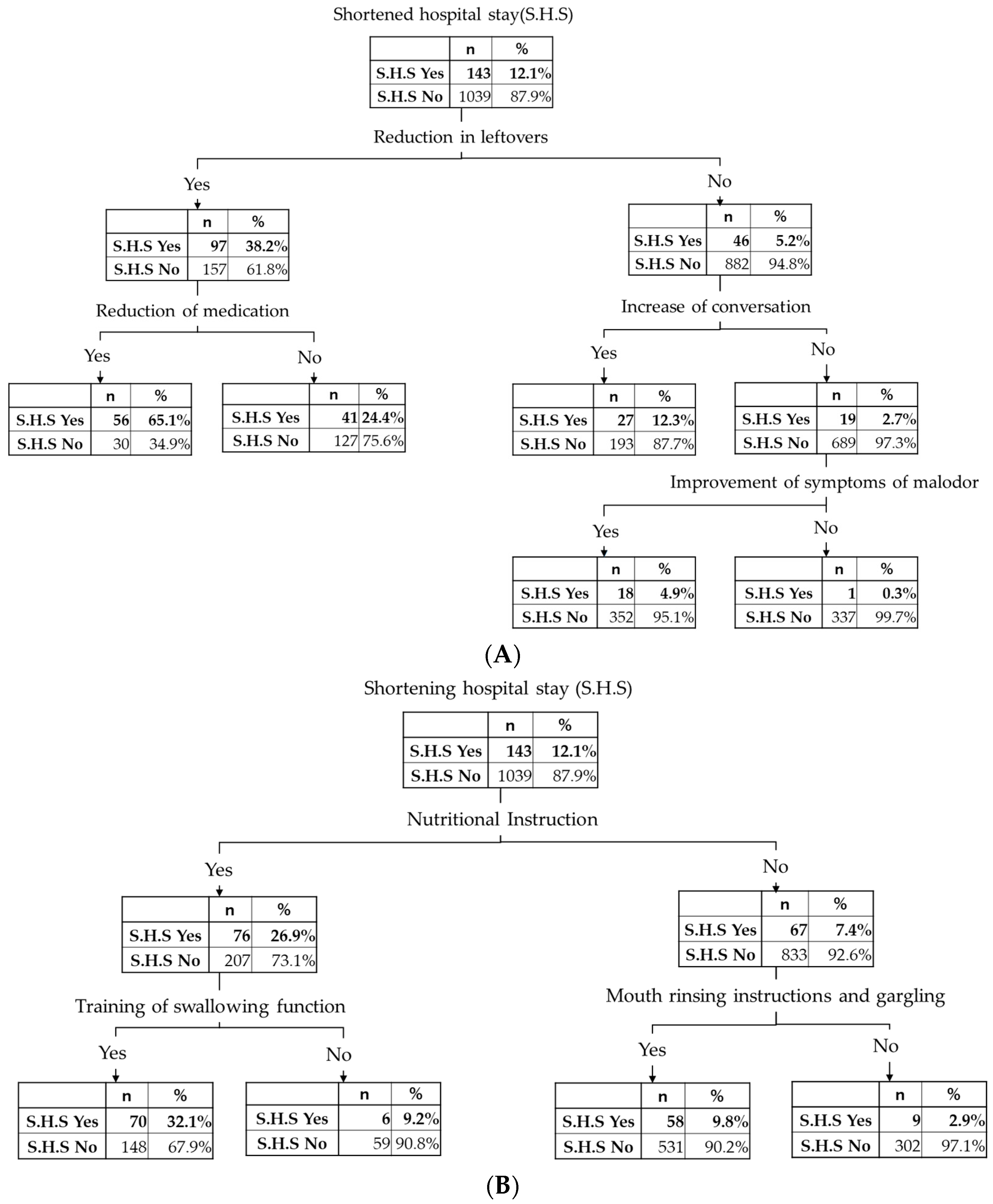
3.6. Treatments and Treatment Effects Led to Shortened Hospital Stay
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sachdev, G.; Napolitano, L.M. Postoperative pulmonary complications: Pneumonia and acute respiratory failure. Surg. Clin. N. Am. 2012, 92, 321–344. [Google Scholar] [CrossRef]
- Chughtai, M.; Gwam, C.U.; Khlopas, A.; Newman, J.M.; Curtis, G.L.; Torres, P.A.; Khan, R.; Mont, M.A. The Incidence of Postoperative Pneumonia in Various Surgical Subspecialties: A Dual Database Analysis. Surg. Technol. Int. 2017, 30, 45–51. [Google Scholar]
- Chughtai, M.; Gwam, C.U.; Mohamed, N.; Khlopas, A.; Newman, J.M.; Khan, R.; Nadhim, A.; Shaffiy, S.; Mont, M.A. The Epidemiology and Risk Factors for Postoperative Pneumonia. J. Clin. Med. Res. 2017, 9, 466–475. [Google Scholar] [CrossRef]
- Pedersen, P.U.; Larsen, P.; Håkonsen, S.J. The effectiveness of systematic perioperative oral hygiene in reduction of postoperative respiratory tract infections after elective thoracic surgery in adults: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2016, 14, 140–173. [Google Scholar] [CrossRef]
- Ishikawa, S.; Yamamori, I.; Takamori, S.; Kitabatake, K.; Edamatsu, K.; Sugano, A.; Oizumi, H.; Kato, H.; Suzuki, J.; Sato, K.; et al. Evaluation of effects of perioperative oral care intervention on hospitalization stay and postoperative infection in patients undergoing lung cancer intervention. Support. Care Cancer 2020, 28, 135–143. [Google Scholar] [CrossRef]
- Ishimaru, M.; Matsui, H.; Ono, S.; Hagiwara, Y.; Morita, K.; Yasunaga, H. Preoperative oral care and effect on postoperative complications after major cancer surgery. Br. J. Surg. 2018, 105, 1688–1696. [Google Scholar] [CrossRef] [PubMed]
- Soutome, S.; Yanamoto, S.; Funahara, M.; Hasegawa, T.; Komori, T.; Yamada, S.I.; Kurita, H.; Yamauchi, C.; Shibuya, Y.; Kojima, Y.; et al. Effect of perioperative oral care on prevention of postoperative pneumonia associated with esophageal cancer surgery: A multicenter case-control study with propensity score matching analysis. Medicine 2017, 96, e7436. [Google Scholar] [CrossRef] [PubMed]
- Iwata, E.; Hasegawa, T.; Yamada, S.I.; Kawashita, Y.; Yoshimatsu, M.; Mizutani, T.; Nakahara, H.; Mori, K.; Shibuya, Y.; Kurita, H.; et al. Effects of perioperative oral care on prevention of postoperative pneumonia after lung resection: Multicenter retrospective study with propensity score matching analysis. Surgery 2019, 165, 1003–1007. [Google Scholar] [CrossRef] [PubMed]
- Kurasawa, Y.; Maruoka, Y.; Sekiya, H.; Negishi, A.; Mukohyama, H.; Shigematsu, S.; Sugizaki, J.; Karakida, K.; Ohashi, M.; Ueno, M.; et al. Pneumonia prevention effects of perioperative oral management in approximately 25,000 patients following cancer surgery. Clin. Exp. Dent. Res. 2020, 6, 165–173. [Google Scholar] [CrossRef]
- Nobuhara, H.; Yanamoto, S.; Funahara, M.; Matsugu, Y.; Hayashida, S.; Soutome, S.; Kawakita, A.; Ikeda, S.; Itamoto, T.; Umeda, M. Effect of perioperative oral management on the prevention of surgical site infection after colorectal cancer surgery: A multicenter retrospective analysis of 698 patients via analysis of covariance using propensity score. Medicine 2018, 97, e12545. [Google Scholar] [CrossRef]
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Tsuji, Y.; Yamaga, M.; Koga, H. Hospital dental hygienist intervention improves activities of daily living, home discharge and mortality in post-acute rehabilitation. Geriatri. Gerontol. Int. 2019, 19, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, R.; Nagano, A.; Wakabayashi, H.; Maeda, K.; Nishioka, S.; Takahashi, M.; Momosaki, R. Assignment of Dental Hygienists Improves Outcomes in Japanese Rehabilitation Wards: A Retrospective Cohort Study. J. Nutr. Health Aging 2020, 24, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Kakuta, E.; Okada, A.; Yamamoto, Y.; Tomonari, H.; Hosoya, N.; Hanada, N.; Yoshida, N.; Takei, N. Prioritization of the Skills to Be Mastered for the Daily Jobs of Japanese Dental Hygienists. Int. J. Dent. 2020, 2020, 4297646. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Survey of Medical Institutions. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/iryosd/m19/dl/is1901_01.pdf (accessed on 26 December 2020).
- Ministry of Health, Labour and Welfare. Survey of Physicians, Dentists and Pharmacists. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/ishi/18/dl/gaikyo.pdf (accessed on 26 December 2020).
- Nomura, Y.; Okada, A.; Yamamoto, Y.; Kakuta, E.; Tomonari, H.; Hosoya, N.; Hanada, N.; Yoshida, N.; Takei, N. Behind Leaving the Job and Rejoining it by the Japanese Dental Hygienist. Open Dent. J. 2020, 14, 355–361. [Google Scholar] [CrossRef]
- Gibson-Howell, J.C.; Hicks, M.J. Dental hygienists’ role in patient assessments and clinical examinations in U.S. dental practices: A review of the literature. J. Allied Health 2010, 39, e1–e5. [Google Scholar]
- Simon, L.; Tobey, M.; Wilson, M. Feasibility of integrating a dental hygienist into an inpatient medical team for patients with diabetes mellitus. J. Public Health Dent. 2019, 79, 188–192. [Google Scholar] [CrossRef]
- Obana, M.; Furuya, J.; Matsubara, C.; Tohara, H.; Inaji, M.; Miki, K.; Numasawa, Y.; Minakuchi, S.; Maehara, T. Effect of a collaborative transdisciplinary team approach on oral health status in acute stroke patients. J. Oral Rehabil. 2019, 46, 1170–1176. [Google Scholar] [CrossRef]
- JDHA. Survey of Working Environment of Japanese Dental Hygienist. Available online: www.jdha.or.jp/aboutdh/chosa.html#datakinmu2020. (accessed on 26 December 2020).
- Nomura, Y.; Kakuta, E.; Okada, A.; Otsuka, R.; Shimada, M.; Tomizawa, Y.; Taguchi, C.; Arikawa, K.; Daikoku, H.; Sato, T.; et al. Effects of self-assessed chewing ability, tooth loss and serum albumin on mortality in 80-year-old individuals: A 20-year follow-up study. BMC Oral Health 2020, 20, 122. [Google Scholar] [CrossRef]
- Nomura, Y.; Tsutsumi, I.; Nagasaki, M.; Tsuda, H.; Koga, F.; Kashima, N.; Uraguchi, M.; Okada, A.; Kakuta, E.; Hanada, N. Supplied Food Consistency and Oral Functions of Institutionalized Elderly. Int. J. Dent. 2020, 2020, 1–7. [Google Scholar] [CrossRef]
- Nomura, Y.; Matsuyama, T.; Fukai, K.; Okada, A.; Ida, M.; Yamauchi, N.; Hanamura, H.; Yabuki, Y.; Watanabe, K.; Sugawara, M.; et al. PRECEDE-PROCEED model based questionnaire and saliva tests for oral health checkup in adult. J. Oral Sci. 2019, 61, 544–548. [Google Scholar] [CrossRef]
- Nomura, Y.; Okada, A.; Kakuta, E.; Otsuka, R.; Saito, H.; Maekawa, H.; Daikoku, H.; Hanada, N.; Sato, T. Workforce and Contents of Home Dental Care in Japanese Insurance System. Int. J. Dent. 2020, 2020, 7316796. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Okada, A.; Miyoshi, J.; Mukaida, M.; Akasaka, E.; Saigo, K.; Daikoku, H.; Maekawa, H.; Sato, T.; Hanada, N. Willingness to Work and the Working Environment of Japanese Dental Hygienists. Int. J. Dent. 2018, 2018, 2727193. [Google Scholar] [CrossRef] [PubMed]
- Inai, Y.; Nomura, Y.; Takarada, T.; Hanada, N.; Wada, N. Risk factors for postoperative pneumonia according to examination findings before surgery under general anesthesia. Clin. Oral Investig. 2020, 24, 3577–3585. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Okada, A.; Kakuta, E.; Gunji, T.; Kajiura, S.; Hanada, N. A new screening method for periodontitis: An alternative to the community periodontal index. BMC Oral Health 2016, 16, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Jokiaho, T.L.; Kaakinen, P.; Virtanen, J.I. Does dental hygienist professional education meet the needs of working life? Educators’ views. Int. J. Dent. Hyg. 2018, 16, 134–143. [Google Scholar] [CrossRef]
- Adachi, M.; Ishihara, K.; Abe, S.; Okuda, K. Professional oral health care by dental hygienists reduced respiratory infections in elderly persons requiring nursing care. Int. J. Dent. Hyg. 2007, 5, 69–74. [Google Scholar] [CrossRef]
- Adachi, M.; Ishihara, K.; Abe, S.; Okuda, K.; Ishikawa, T. Effect of professional oral health care on the elderly living in nursing homes. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 191–195. [Google Scholar] [CrossRef]
- Okuda, K.; Kimizuka, R.; Abe, S.; Kato, T.; Ishihara, K. Involvement of periodontopathic anaerobes in aspiration pneumonia. J. Periodontol. 2005, 76, 2154–2160. [Google Scholar] [CrossRef]
- Abe, S.; Ishihara, K.; Adachi, M.; Sasaki, H.; Tanaka, K.; Okuda, K. Professional oral care reduces influenza infection in elderly. Arch. Gerontol. Geriatr. 2006, 43, 157–164. [Google Scholar] [CrossRef]
- Barnes, C.M. Dental hygiene intervention to prevent nosocomial pneumonias. J. Evid. Based Dent. Pract. 2014, 14, 103–114. [Google Scholar] [CrossRef]
- Hua, F.; Xie, H.; Worthington, H.V.; Furness, S.; Zhang, Q.; Li, C. Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia. Cochrane Database Syst. Rev. 2016, 10, Cd008367. [Google Scholar] [CrossRef] [PubMed]
- Akutsu, Y.; Matsubara, H.; Shuto, K.; Shiratori, T.; Uesato, M.; Miyazawa, Y.; Hoshino, I.; Murakami, K.; Usui, A.; Kano, M.; et al. Pre-operative dental brushing can reduce the risk of postoperative pneumonia in esophageal cancer patients. Surgery 2010, 147, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Poisson, P.; Laffond, T.; Campos, S.; Dupuis, V.; Marchasson, B.I. Relationships between oral health, dysphagia and undernutrition in hospitalised elderly patients. Gerodontology 2016, 33, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Ido, Y.; Yoshimura, Y.; Mutai, H. Relationship of Malnutrition during Hospitalization with Functional Recovery and Postdischarge Destination in Elderly Stroke Patients. J. Stroke Cerebrovasc. Dis. 2019, 28, 1866–1872. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, Y. Factors associated with the level of oral intake in hospitalized older adults with dysphagia: The importance of mental activity. Clin. Nutr. ESPEN 2016, 13, e52–e54. [Google Scholar] [CrossRef] [PubMed]
- Okabe, Y.; Furuta, M.; Akifusa, S.; Takeuchi, K.; Adachi, M.; Kinoshita, T.; Kikutani, T.; Nakamura, S.; Yamashita, Y. Swallowing Function and Nutritional Status in Japanese Elderly People Receiving Home-care Services: A 1-year Longitudinal Study. J. Nutr. Health Aging 2016, 20, 697–704. [Google Scholar] [CrossRef]
- Furuta, M.; Komiya-Nonaka, M.; Akifusa, S.; Shimazaki, Y.; Adachi, M.; Kinoshita, T.; Kikutani, T.; Yamashita, Y. Interrelationship of oral health status, swallowing function, nutritional status, and cognitive ability with activities of daily living in Japanese elderly people receiving home care services due to physical disabilities. Community Dent. Oral Epidemiol. 2013, 41, 173–181. [Google Scholar] [CrossRef]
- Kikutani, T.; Enomoto, R.; Tamura, F.; Oyaizu, K.; Suzuki, A.; Inaba, S. Effects of oral functional training for nutritional improvement in Japanese older people requiring long-term care. Gerodontology 2006, 23, 93–98. [Google Scholar] [CrossRef]
- Soutome, S.; Yanamoto, S.; Funahara, M.; Hasegawa, T.; Komori, T.; Oho, T.; Umeda, M. Preventive Effect on Post-Operative Pneumonia of Oral Health Care among Patients Who Undergo Esophageal Resection: A Multi-Center Retrospective Study. Surg. Infect. 2016, 17, 479–484. [Google Scholar] [CrossRef]
- Soutome, S.; Hasegawa, T.; Yamguchi, T.; Aoki, K.; Kanamura, N.; Mukai, T.; Yamazoe, J.; Nishikawa, M.; Isomura, E.; Hoshi, K.; et al. Prevention of postoperative pneumonia by perioperative oral care in patients with esophageal cancer undergoing surgery: A multicenter retrospective study of 775 patients. Support Care Cancer. 2020, 28, 4155–4162. [Google Scholar] [CrossRef]
- Ministry of Health, Labor and Welfare. Report on Public Health Administration and Services. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/eisei/18/ (accessed on 26 December 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | n | % | |
|---|---|---|---|
| Practice of perioperative oral care management | Tooth brushing by dental hygienist | 1371 | 94.6% |
| Scaling and mechanical tooth cleaning | 1405 | 96.9% | |
| Cleaning of tongue and mucosa | 1157 | 79.8% | |
| Moisture retention if oral cavity | 937 | 64.6% | |
| Topical fluoride application | 987 | 68.1% | |
| Mouth rinsing instructions and gargling | 1004 | 69.2% | |
| Drug application for gingiva and oral mucosa | 826 | 57.0% | |
| Oral health instruction for patients, their family or caregivers | 1319 | 91.0% | |
| Denture cleaning | 1352 | 93.2% | |
| Training of swallowing function | 446 | 30.8% | |
| Assessment of oral conditions | 632 | 43.6% | |
| Nutritional instruction | 317 | 21.9% | |
| Self-assessed effect of perioperative oral care | Improvement of symptoms of tongue or oral mucosa | 834 | 57.5% |
| Improvement of symptoms of teeth or gingiva | 1033 | 71.2% | |
| Improvement of symptoms of oral hygiene status | 1165 | 80.3% | |
| Improvement of symptoms of xerostomia, improvement in salivary flow | 626 | 43.2% | |
| Improvement of symptoms of malodor | 859 | 59.2% | |
| Reduction of medication | 129 | 8.9% | |
| Improvement of sensation of taste and patients enjoying their meals | 403 | 27.8% | |
| Reduction of leftovers | 265 | 18.3% | |
| Increase in conversation | 468 | 32.3% | |
| Recognition of importance of oral care management | 882 | 60.8% | |
| Implementation of independent self-oral care | 808 | 55.7% | |
| Shortened hospital stay | 143 | 9.9% | |
| Medical team participation | Nutritional support team | 81 | 5.6% |
| Swallowing function support team | 121 | 8.3% | |
| Oral care support team | 199 | 13.7% | |
| Cancer care team | 57 | 3.9% | |
| Palliative care team | 57 | 3.9% | |
| Ventilation support team | 18 | 1.2% | |
| Decubitus prevention team | 12 | 0.8% | |
| Infection control team | 53 | 3.7% | |
| Medical safety team | 72 | 5.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nomura, Y.; Ohara, Y.; Yamamoto, Y.; Okada, A.; Hosoya, N.; Hanada, N.; Takei, N. Dental Hygienists’ Practice in Perioperative Oral Care Management According to the Japanese Dental Hygienists Survey 2019. Int. J. Environ. Res. Public Health 2021, 18, 114. https://doi.org/10.3390/ijerph18010114
Nomura Y, Ohara Y, Yamamoto Y, Okada A, Hosoya N, Hanada N, Takei N. Dental Hygienists’ Practice in Perioperative Oral Care Management According to the Japanese Dental Hygienists Survey 2019. International Journal of Environmental Research and Public Health. 2021; 18(1):114. https://doi.org/10.3390/ijerph18010114
Chicago/Turabian StyleNomura, Yoshiaki, Yuki Ohara, Yuko Yamamoto, Ayako Okada, Noriyasu Hosoya, Nobuhiro Hanada, and Noriko Takei. 2021. "Dental Hygienists’ Practice in Perioperative Oral Care Management According to the Japanese Dental Hygienists Survey 2019" International Journal of Environmental Research and Public Health 18, no. 1: 114. https://doi.org/10.3390/ijerph18010114
APA StyleNomura, Y., Ohara, Y., Yamamoto, Y., Okada, A., Hosoya, N., Hanada, N., & Takei, N. (2021). Dental Hygienists’ Practice in Perioperative Oral Care Management According to the Japanese Dental Hygienists Survey 2019. International Journal of Environmental Research and Public Health, 18(1), 114. https://doi.org/10.3390/ijerph18010114