Patterns of Comorbidity in Hepatocellular Carcinoma: A Network Perspective

Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Preprocessing
2.2. Statistical Analysis
2.3. Network Analysis
3. Results
3.1. Patient Characteristics
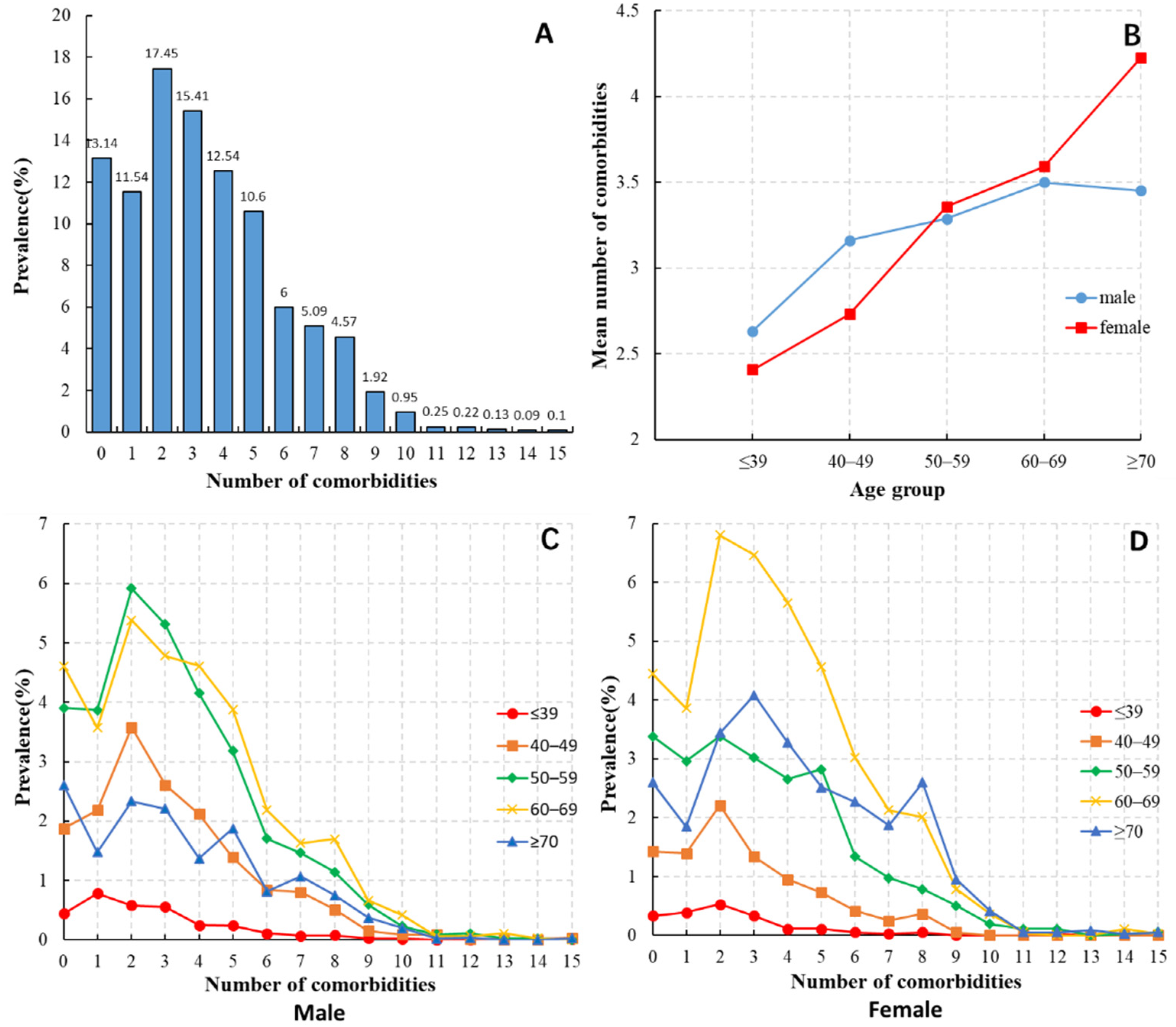
3.2. Distribution of Comorbidities
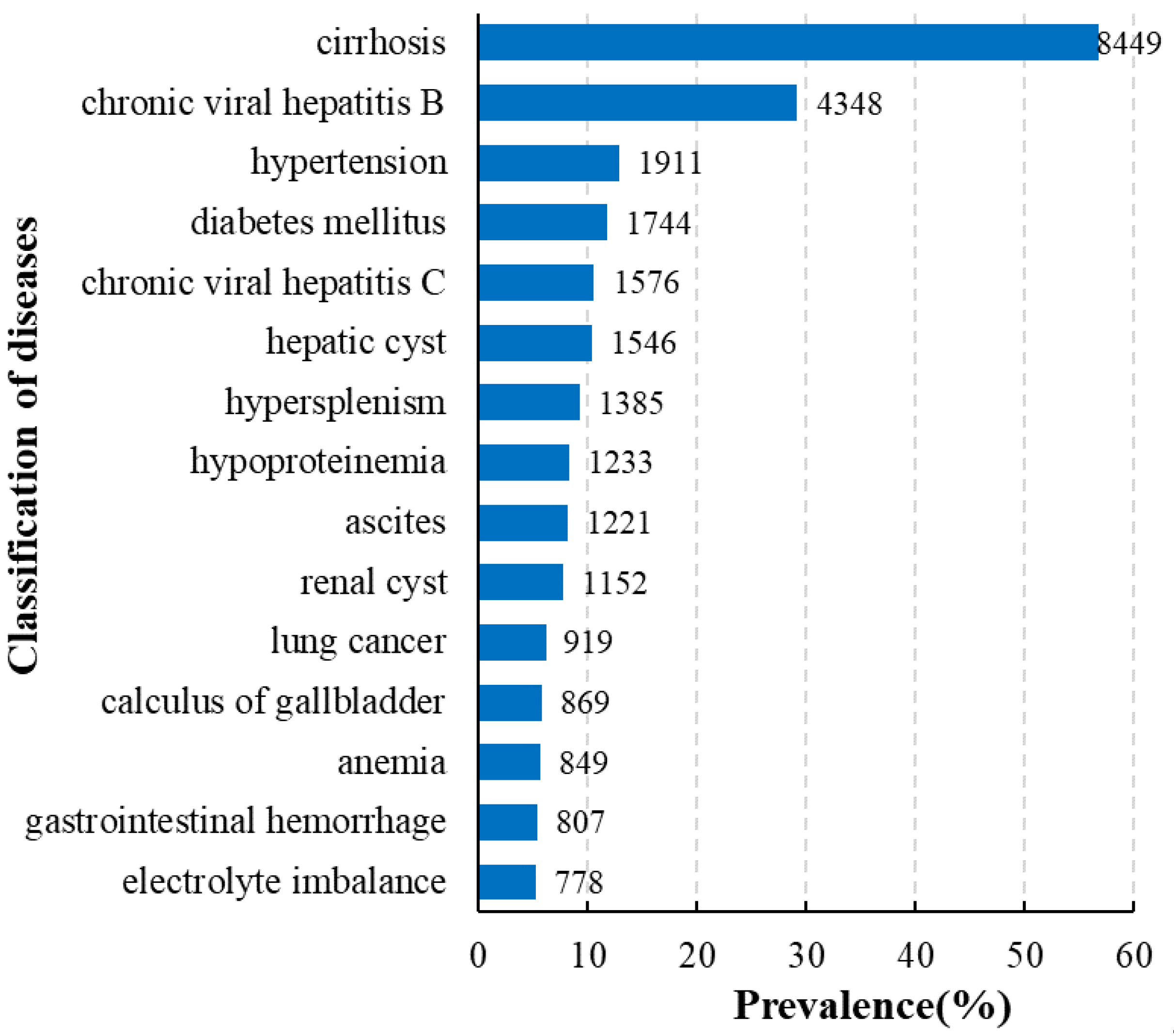
3.3. Diseases Frequently Accompanying HCC
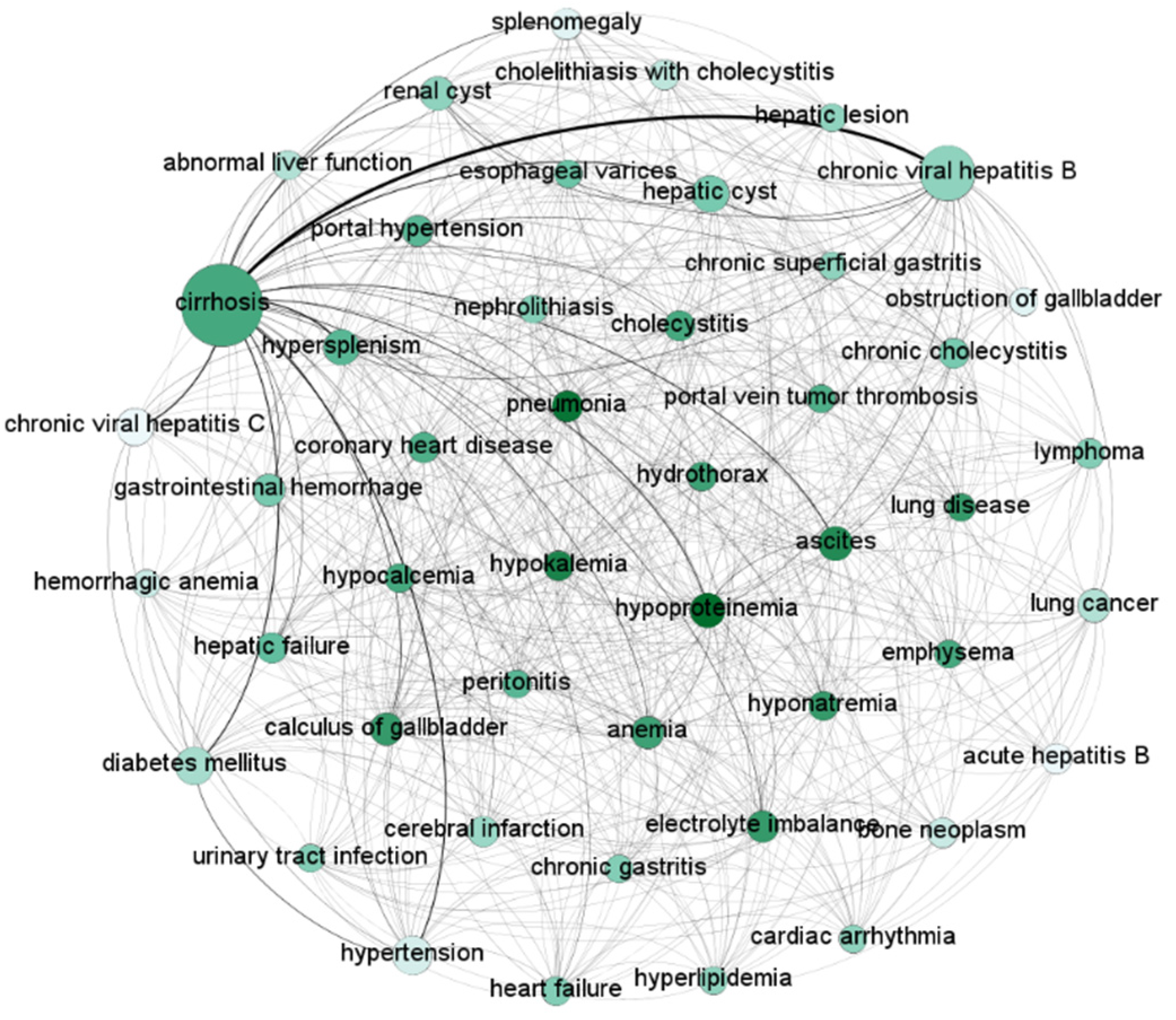
3.4. Comorbidities Network
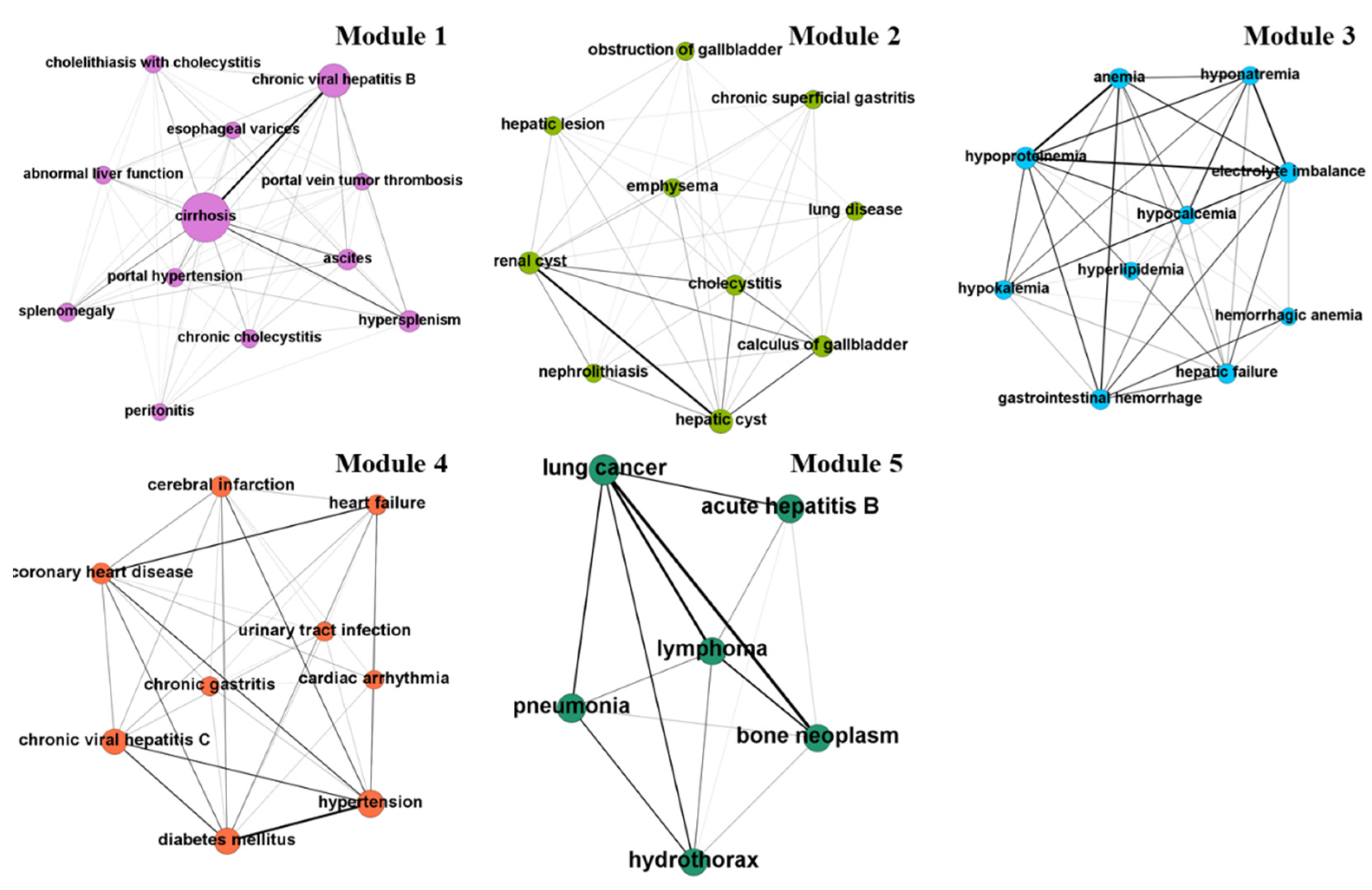
3.5. Network-based Clustering: Comorbidities Modules
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Edwards, B.K.; Noone, A.M.; Mariotto, A.B.; Simard, E.P.; Boscoe, F.P.; Henley, S.J.; Jemal, A.; Cho, H.; Anderson, R.N.; Kohler, B.A.; et al. Annual Report to the Nation on the status of cancer, 1975–2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 2014, 120, 1290–1314. [Google Scholar] [CrossRef] [PubMed]
- Sarfati, D.; Gurney, J.; Lim, B.T.; Bagheri, N.; Simpson, A.; Koea, J.; Dennett, E. Identifying important comorbidity among cancer populations using administrative data: Prevalence and impact on survival. Asia Pac. J. Clin. Oncol. 2016, 12, e47–e56. [Google Scholar] [CrossRef]
- Fan, J.H.; Wang, J.B.; Jiang, Y.; Xiang, W.; Liang, H.; Wei, W.Q.; Qiao, Y.L.; Boffetta, P. Attributable causes of liver cancer mortality and incidence in China. Asian Pac. J. Cancer Prev. 2013, 14, 7251–7256. [Google Scholar] [CrossRef] [PubMed]
- Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; Artaman, A.; et al. The Burden of Primary Liver Cancer and Underlying Etiologies from 1990 to 2015 at the Global, Regional, and National Level: Results From the Global Burden of Disease Study 2015. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar] [PubMed]
- Divo, M.J.; Martinez, C.H.; Mannino, D.M. Number 2 in the series “Multimorbidity and the lung”: Ageing and the epidemiology of multimorbidity. Eur. Respir. J. 2014, 44, 1055–1068. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Sarfati, D.; Koczwara, B.; Jackson, C. The impact of comorbidity on cancer and its treatment. CA Cancer J. Clin. 2016, 66, 337–350. [Google Scholar] [CrossRef]
- Sogaard, M.; Thomsen, R.; Bossen, K.; Sorensen, H.T.; Horgaard, M. The impact of comorbidity on cancer survival: A review. Clin. Epidemiol. 2013, 5, 3–29. [Google Scholar] [CrossRef]
- Drzayich, A.D.; Waldman, C.A.; Khoury, R.; Michael, T.; Renda, A.; Hopson, S.; Parikh, A.; Stein, A.; Costantino, M.; Stemkowski, S.; et al. The relationship between comorbidity medication adherence and health related quality of life among patients with cancer. J. Patient Rep. Outcomes 2018, 2, 29. [Google Scholar] [CrossRef]
- Chuang, S.C.; La, V.C.; Boffetta, P. Liver cancer: Descriptive epidemiology and risk factors other than HBV and HCV infection. Cancer Lett. 2009, 286, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, A.H.; Sadikova, E.; Cheetham, C.; Chiang, K.M.; Shi, J.X.; Caparosa, S.; Younossi, Z.M.; Nyberg, L.M. Increased cancer rates in patients with chronic hepatitis C. Liver Int. Off. J. Int. Assoc. Study Liver 2020, 40, 3685–3693. [Google Scholar] [CrossRef] [PubMed]
- Ninio, L.; Nissani, A.; Meirson, T.; Domovitz, T.; Genna, A.; Twafra, S.; Srikanth, K.D.; Dabour, R.; Avraham, E.; Davidovich, A.; et al. Hepatitis C virus enhances the invasiveness of hepatocellular carcinoma via EGFR-mediated invadopodia formation and activation. Cells 2019, 8, 1395. [Google Scholar] [CrossRef]
- Shau, W.Y.; Shao, Y.Y.; Yeh, Y.C.; Lin, Z.Z.; Kuo, R.; Hsu, C.H.; Hsu, C.; Cheng, A.L.; Lai, M.S. Diabetes mellitus is associated with increased mortality in patients receiving curative therapy for hepatocellular carcinoma. Oncologist 2012, 17, 856–862. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.G.; King, L.Y.; Chong, D.Q.; Nguyen, L.H.; Ma, Y.; VoPham, T.; Giovannucci, E.L.; Fuchs, C.S.; Meyerhardt, J.A.; Corey, K.E.; et al. Diabetes, metabolic comorbidities, and risk of hepatocellular carcinoma: Results from two prospective cohort studies. Hepatology 2018, 67, 1797–1806. [Google Scholar] [CrossRef] [PubMed]
- Saitta, C.; Pollicino, T.; Raimondo, G. Obesity and liver cancer. Ann. Hepatol. 2019, 18, 810–815. [Google Scholar] [CrossRef] [PubMed]
- London, W.T.; Petrick, J.L.; McGlynn, K.A. Liver cancer. In Cancer Epidemiology and Prevention, 4th ed.; Thun, M.J., Linet, M.S., Cerhan, J.R., Haiman, C.A., Schottenfeld, D., Eds.; Oxford University Press: New York, NY, USA, 2018; pp. 635–660. [Google Scholar]
- Hofmann, S.G.; Curtiss, J.; McNally, R.J. A complex network perspective on clinical science. Perspect. Psychol. Sci. 2016, 11, 597–605. [Google Scholar] [CrossRef]
- Borsboom, D. A network theory of mental disorders. World Psychiatry 2017, 16, 5–13. [Google Scholar] [CrossRef]
- Barabási, A.L.; Gulbahce, N.; Loscalzo, J. Network medicine: A network-based approach to human disease. Nat. Rev. Genet. 2011, 12, 56–68. [Google Scholar] [CrossRef]
- Fried, E.I.; van Borkulo, C.D.; Cramer, A.O.J.; Boschloo, L.; Schoevers, R.A.; Borsboom, D. Mental disorders as networks of problems: A review of recent insights. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1–10. [Google Scholar] [CrossRef]
- World Health Organization. ICD-10: International Statistical Classification of Diseases and Related Health Problems 10th Revision; World Health Organization: Geneva, Switzerland, 1992; Volume 56, p. 65. [Google Scholar]
- Guo, M.; Yu, Y.; Wen, T.; Zhang, X.; Liu, B.; Zhang, J.; Zhang, R.; Zhang, Y.; Zhou, X. Analysis of disease comorbidity patterns in a large-scale China population. BMC Med. Genom. 2019, 12, 177. [Google Scholar] [CrossRef]
- Gu, J.; Chao, J.; Chen, W.; Xu, H.; Wu, Z.; Chen, H.; He, T.; Deng, L.; Zhang, R. Multimorbidity in the community-dwelling elderly in urban China. Arch. Gerontol. Geriatr. 2017, 68, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Marengoni, A.; Rizzuto, D.; Wang, H.X.; Winblad, B.; Fratiglioni, L. Patterns of chronic multimorbidity in the elderly population. J. Am. Geriatr. Soc. 2009, 57, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Bastian, M.; Heymann, S.; Jacomy, M. Gephi: An open source software for exploring and manipulating networks. In Proceedings of the International AAAI Conference on Weblogs and Social Media, San Jose, CA, USA, 17–20 May 2009. [Google Scholar]
- Blondel, V.D.; Guillaume, J.L.; Lambiotte, R.; Lefebvre, E. Fast unfolding of communities in large networks. J. Stat. Mech. Theory Exp. 2008, 10, P1000. [Google Scholar] [CrossRef]
- Goldacre, M.J.; Wotton, C.J.; Yeates, D.; Seagroatt, V.; Collier, J. Liver cirrhosis, other liver diseases, pancreatitis and subsequent cancer: Record linkage study. Eur. J. Gastroenterol. Hepatol. 2008, 20, 384–392. [Google Scholar] [CrossRef]
- Persson, E.C.; Quraishi, S.M.; Welzel, T.M.; Carreon, J.D.; Gridley, G.; Graubard, B.I.; McGlynn, K.A. Risk of liver cancer among US male veterans with cirrhosis, 1969–1996. Br. J. Cancer 2012, 107, 195–200. [Google Scholar] [CrossRef]
- Poynard, T.; Peta, V.; Deckmyn, O.; Munteanu, M.; Moussalli, J.; Ngo, Y.; Rudler, M.; Lebray, P.; Pais, R.; Bonyhay, L.; et al. HECAM-FibroFrance Group. LCR1 and LCR2, two multi-analyte blood tests to assess liver cancer risk in patients without or with cirrhosis. Aliment. Pharmacol. Ther. 2019, 49, 308–320. [Google Scholar] [CrossRef]
- Rosmorduc, O. Relationship between hepatocellular carcinoma, metabolic syndrome and non-alcoholic fatty liver disease: Which clinical arguments? Ann. Endocrinol. 2013, 74, 115–120. [Google Scholar] [CrossRef]
- Carrier, P.; Debette-Gratien, M.; Jacques, J.; Loustaud-Ratti, V. Cirrhotic patients and older people. World J. Hepatol. 2019, 11, 678–688. [Google Scholar] [CrossRef]
- Jepsen, P. Comorbidity in cirrhosis. World J. Gastroenterol. 2014, 20, 7223–7230. [Google Scholar] [CrossRef]
- El-Serag, H.B. Current concepts: Hepatocellular carcinoma. N. Engl. J. Med. 2011, 365, 1118–1127. [Google Scholar] [CrossRef]
- Chen, X.P.; Wu, Z.D.; Huang, Z.Y.; Qiu, F.Z. Use of hepatectomy and splenectomy to treat hepatocellular carcinoma with cirrhotic hypersplenism. Br. J. Surg. 2005, 92, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of the People’s Republic of China. Practice guidelines for diagnosis and treatment of primary hepatic carcinoma (v.2011). J. Clin. Hepatol. 2011, 11, 22–40. [Google Scholar]
- Nayak, N.C.; Vasdev, N.; Saigal, S.; Soin, A.S. End-stage nonalcoholic fatty liver disease: Evaluation of pathomorphologic features and relationship to cryptogenic cirrhosis from study of explant livers in a living donor liver transplant program. Hum. Pathol. 2010, 41, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Siegel, A.B.; Zhu, A.X. Metabolic syndrome and hepatocellular carcinoma: Two growing epidemics with a potential link. Cancer 2009, 115, 5651–5661. [Google Scholar] [CrossRef] [PubMed]
- Osaki, Y.; Taniguchi, S.; Tahara, A.; Okamoto, M.; Kishimoto, T. Metabolic syndrome and incidence of liver and breast cancers in Japan. Cancer Epidemiol. 2012, 36, 141–147. [Google Scholar] [CrossRef]
- Yang, Y.; Zhang, B.H.; Gong, J.P. Genes and molecular mechanisms affecting the correlation between liver cancer and diabetes mellitus. Zhonghua gan zang bing za zhi Chin. J. Hepatol. 2018, 26, 718–720. [Google Scholar]
- Kerdsuknirun, J.; Vilaichone, V.; Vilaichone, R.K. Clinical outcome and predictive factors of variceal bleeding in patients with hepatocellular carcinoma in Thailand. Asian Pac. J. Cancer Prev. 2018, 19, 3301–3305. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Patients with HCC (n = 14,891) n (%) |
|---|---|
| Age, year | |
| ≤ 39 | 431 (2.89) |
| 40–49 | 2172 (14.59) |
| 50–59 | 4388 (29.47) |
| 60–69 | 5251 (35.26) |
| ≥70 | 2649 (17.79) |
| Sex | |
| Female | 3572 (23.99) |
| Male | 11,319 (76.01) |
| Nationality | |
| Han | 13,161 (88.38) |
| Korean | 1697 (11.40) |
| Man | 117 (0.79) |
| Other | 84 (0.56) |
| Marital status | |
| Married | 13,987 (93.93) |
| Single | 904 (6.07) |
| Disease | Male Patients (n = 11,319) | Female Patients (n = 3572) | p-Value | ||
|---|---|---|---|---|---|
| n (%) | Rank | n (%) | Rank | ||
| Cirrhosis | 6495 (57.38) | 1 | 1954 (54.70) | 1 | 0.0049 |
| Chronic viral hepatitis B | 3557 (31.43) | 2 | 791 (22.14) | 2 | <0.001 |
| Hypertension | 1389 (17.02) | 3 | 522 (14.61) | 4 | <0.001 |
| Diabetes mellitus | 1365 (11.97) | 4 | 379 (10.61) | 6 | 0.0189 |
| Hepatic cyst | 1179 (10.42) | 5 | 367 (10.27) | 7 | 0.809 |
| Hypersplenism | 989 (10.20) | 6 | 396 (11.09) | 5 | <0.001 |
| Ascites | 971 (8.74) | 7 | 250 (7.0) | 10 | 0.0027 |
| Renal cyst | 961 (8.58) | 8 | 191 (5.35) | 17 | <0.001 |
| Chronic viral hepatitis C | 941 (8.49) | 9 | 635 (17.78) | 3 | <0.001 |
| Hypoproteinemia | 882 (8.31) | 10 | 351 (9.83) | 8 | <0.001 |
| Lung cancer | 700 (7.79) | 11 | 219 (6.13) | 12 | 0.908 |
| Gallbladder stones | 666 (5.88) | 12 | 203 (5.68) | 13 | 0.655 |
| Gastrointestinal hemorrhage | 614 (5.42) | 13 | 193 (5.40) | 15 | 0.961 |
| Anemia | 599 (5.39) | 14 | 250 (7.00) | 9 | <0.001 |
| Electrolyte imbalance | 580 (5.12) | 15 | 198 (5.54) | 14 | 0.327 |
| Coronary heart disease | 393 (3.47) | 25 | 239 (6.69) | 11 | <0.001 |
| Disease | ≤39 (n = 431) n (%) | 40–49 (n = 2172) n (%) | 50–59 (n = 4388) n (%) | 60–69 (n = 5251) n (%) | ≥70 (n = 2649) n (%) | p-Value |
|---|---|---|---|---|---|---|
| Cirrhosis | 206 (47.80) | 1368 (62.98) | 2654 (60.48) | 3008 (57.28) | 1213 (45.79) | <0.001 |
| Chronic viral hepatitis B | 139 (32.25) | 895 (41.21) | 1619 (36.90) | 1351 (25.73) | 344 (12.99) | <0.001 |
| Hypertension | 2 (0.46) | 161 (7.41) | 408 (9.30) | 841 (16.02) | 499 (18.84) | <0.001 |
| Diabetes mellitus | 3 (0.70) | 160 (7.37) | 571 (13.01) | 702 (13.37) | 308 (11.63) | <0.001 |
| Chronic viral hepatitis C | 1 (0.23) | 36 (1.66) | 267 (6.08) | 738 (14.05) | 534 (20.16) | <0.001 |
| Hepatic cyst | 24 (5.57) | 157 (7.23) | 460 (10.48) | 642 (12.23) | 263 (9.93) | <0.001 |
| Hypersplenism | 37 (8.58) | 231 (10.64) | 401 (9.14) | 523 (9.96) | 193 (7.29) | <0.001 |
| Hypoproteinemia | 20 (4.64) | 189 (8.70) | 326 (7.43) | 413 (7.87) | 285 (10.76) | <0.001 |
| Ascites | 35 (8.12) | 171 (7.873) | 418 (9.53) | 393 (7.48) | 204 (7.70) | 0.005 |
| Renal cyst | 12 (2.78) | 125 (5.76) | 347 (7.91) | 443 (8.44) | 225 (8.49) | <0.001 |
| Lung cancer | 66 (15.31) | 149 (6.86) | 246 (5.61) | 316 (6.02) | 142(5.36) | <0.001 |
| Gallbladder stones | 9 (2.09) | 134 (6.17) | 217 (4.95) | 337 (6.42) | 172 (6.49) | <0.001 |
| Anemia | 11 (2.55) | 118 (5.43) | 243 (5.54) | 285 (5.43) | 192 (7.25) | <0.001 |
| Gastrointestinal hemorrhage | 21 (4.87) | 121 (5.57) | 248 (5.65) | 261 (4.97) | 156 (5.89) | 0.404 |
| Electrolyte imbalance | 17 (3.94) | 144 (6.63) | 197 (4.49) | 266 (5.07) | 154 (5.81) | 0.002 |
| Bone neoplasm | 25 (5.80) | 74 (3.41) | 151 (3.44) | 172 (3.28) | 62 (2.34) | 0.002 |
| Lymphoma | 24 (5.57) | 68 (3.13) | 162 (3.69) | 197 (3.75) | 57 (2.15) | <0.001 |
| Splenomegaly | 18 (4.18) | 135 (6.22) | 231 (5.26) | 242 (4.61) | 78 (2.94) | <0.001 |
| Cerebral infarction | NA | 8 (0.37) | 83 (1.89) | 300 (5.71) | 226 (8.53) | <0.001 |
| Coronary heart disease | 2 (0.46) | 9 (0.41) | 94 (2.14) | 260 (4.95) | 267 (10.08) | < 0.001 |
| Heart failure | NA | 2 (0.09) | 58 (1.32) | 144 (2.74) | 175 (6.61) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mu, X.-M.; Wang, W.; Jiang, Y.-Y.; Feng, J. Patterns of Comorbidity in Hepatocellular Carcinoma: A Network Perspective. Int. J. Environ. Res. Public Health 2020, 17, 3108. https://doi.org/10.3390/ijerph17093108
Mu X-M, Wang W, Jiang Y-Y, Feng J. Patterns of Comorbidity in Hepatocellular Carcinoma: A Network Perspective. International Journal of Environmental Research and Public Health. 2020; 17(9):3108. https://doi.org/10.3390/ijerph17093108
Chicago/Turabian StyleMu, Xiao-Min, Wei Wang, Yu-Ying Jiang, and Jia Feng. 2020. "Patterns of Comorbidity in Hepatocellular Carcinoma: A Network Perspective" International Journal of Environmental Research and Public Health 17, no. 9: 3108. https://doi.org/10.3390/ijerph17093108
APA StyleMu, X.-M., Wang, W., Jiang, Y.-Y., & Feng, J. (2020). Patterns of Comorbidity in Hepatocellular Carcinoma: A Network Perspective. International Journal of Environmental Research and Public Health, 17(9), 3108. https://doi.org/10.3390/ijerph17093108