Exposure to Heavy Metals in Electronic Waste Recycling in Thailand

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
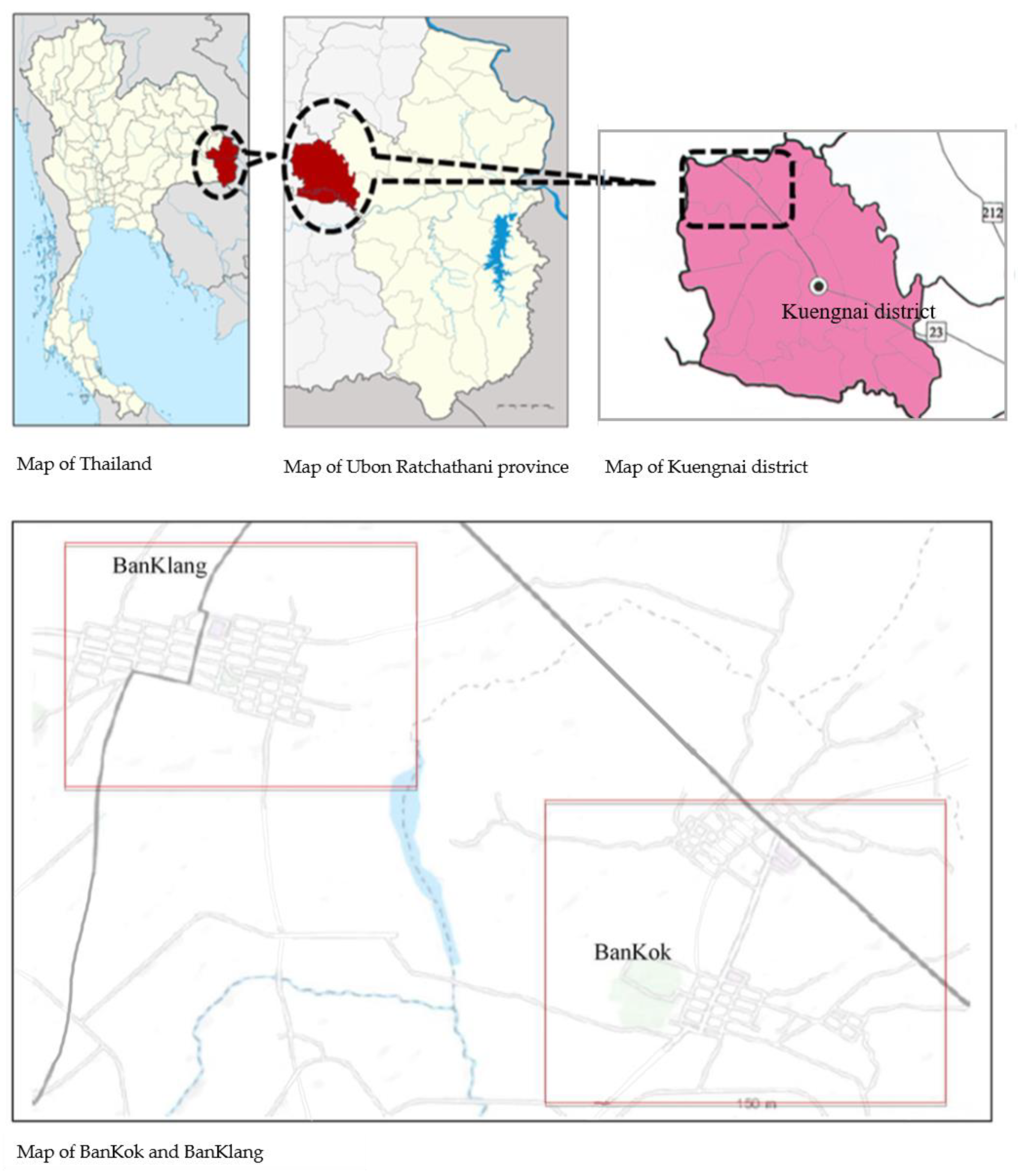
2.1. Study Sites
2.2. Study Design and Population
2.3. Environmental and Biological Sample Collection and Analysis
2.3.1. House Dust and Airborne Dust Collection and Analysis
2.3.2. Blood and Urine Sample Collection
2.3.3. Analysis of Heavy Metals
2.3.4. Questionnaires
2.4. Data Analysis
3. Results
3.1. General Characteristics of Study Subjects
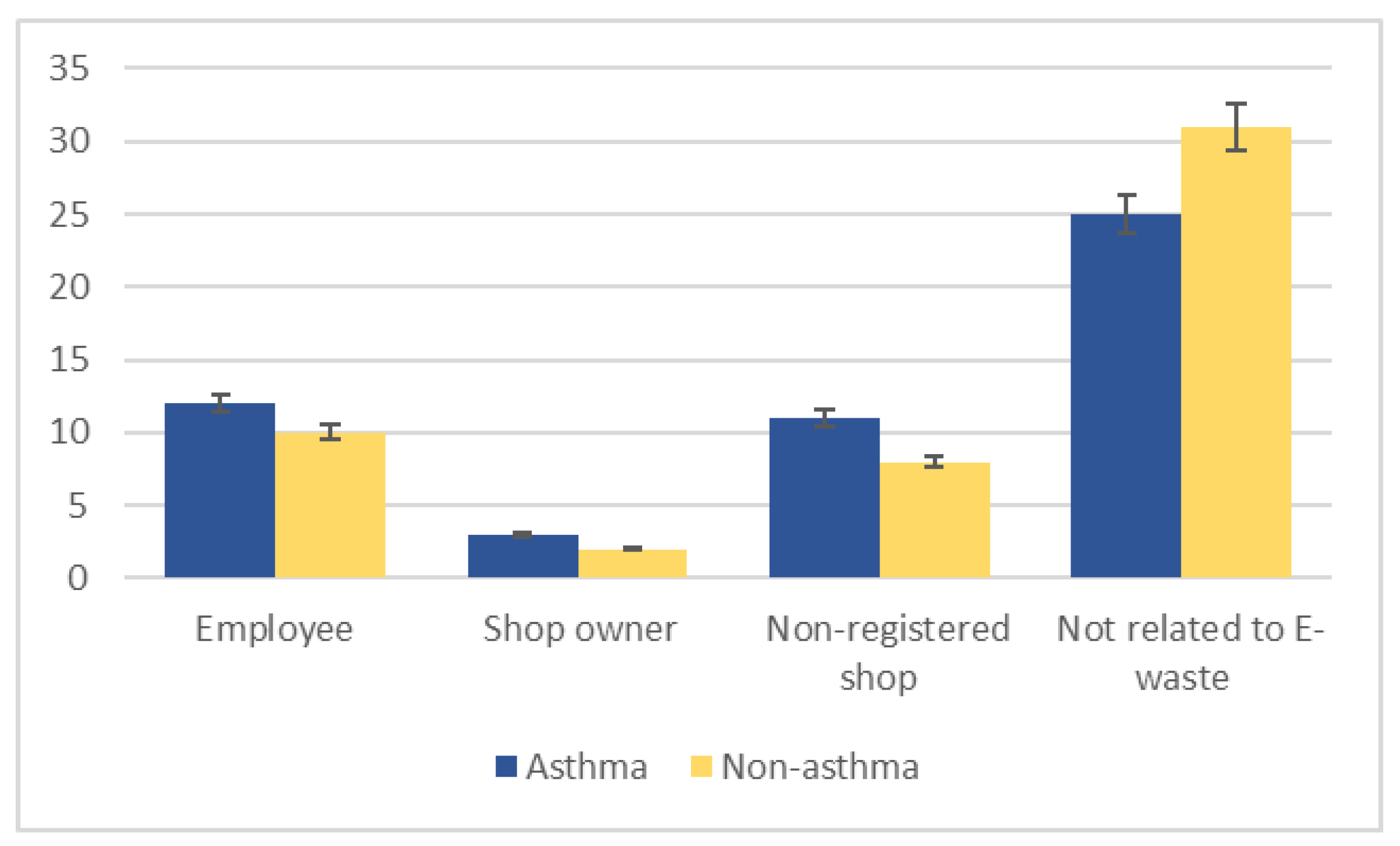
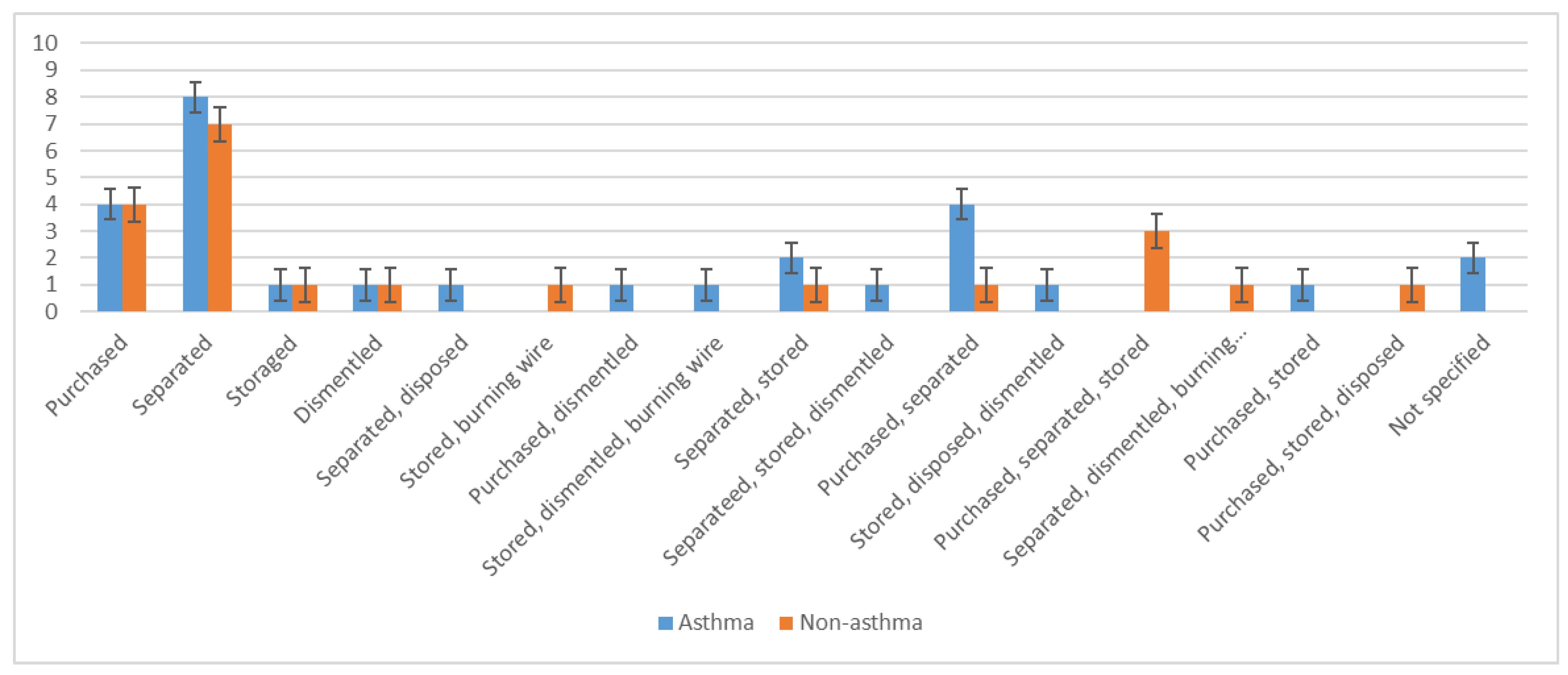
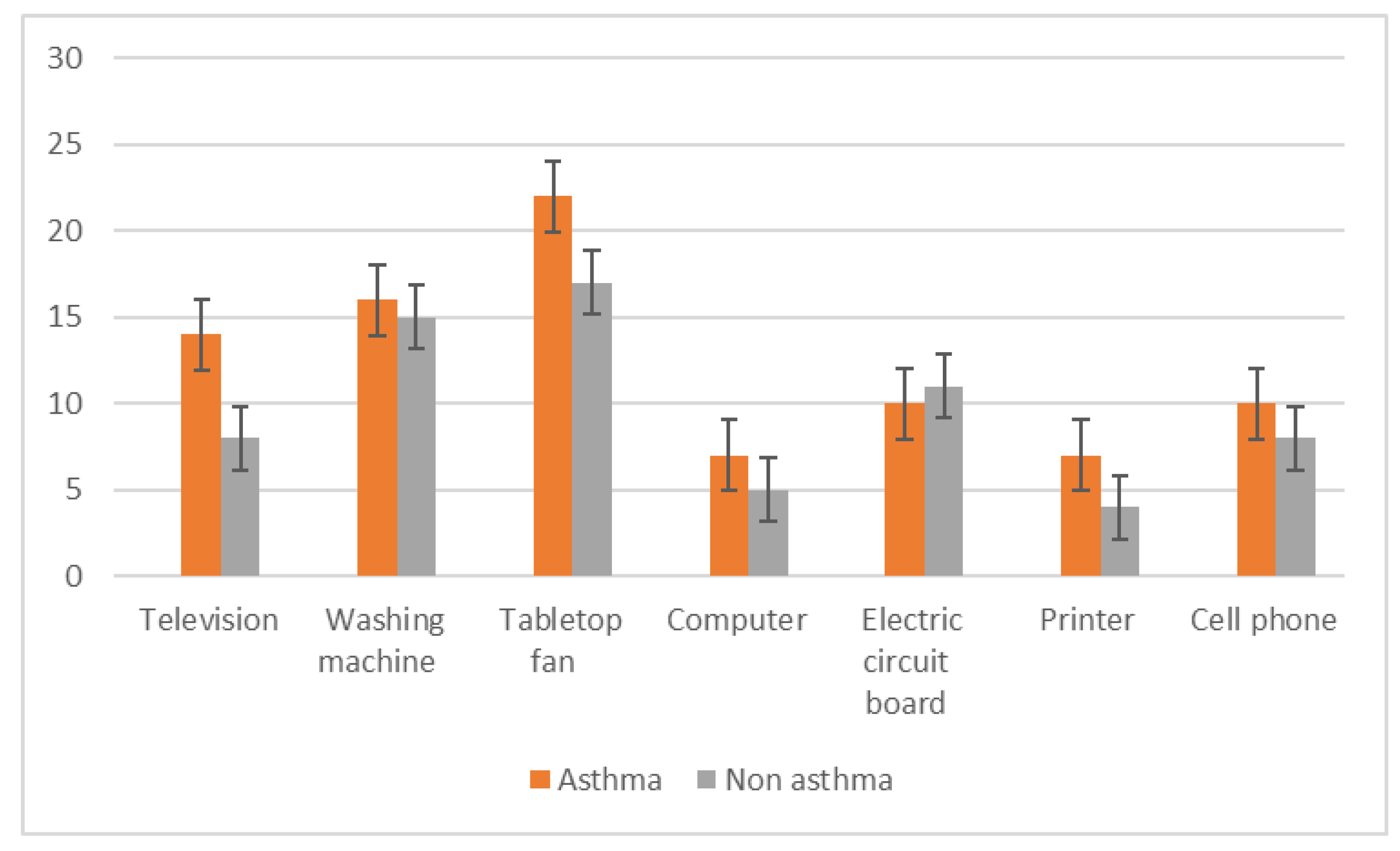
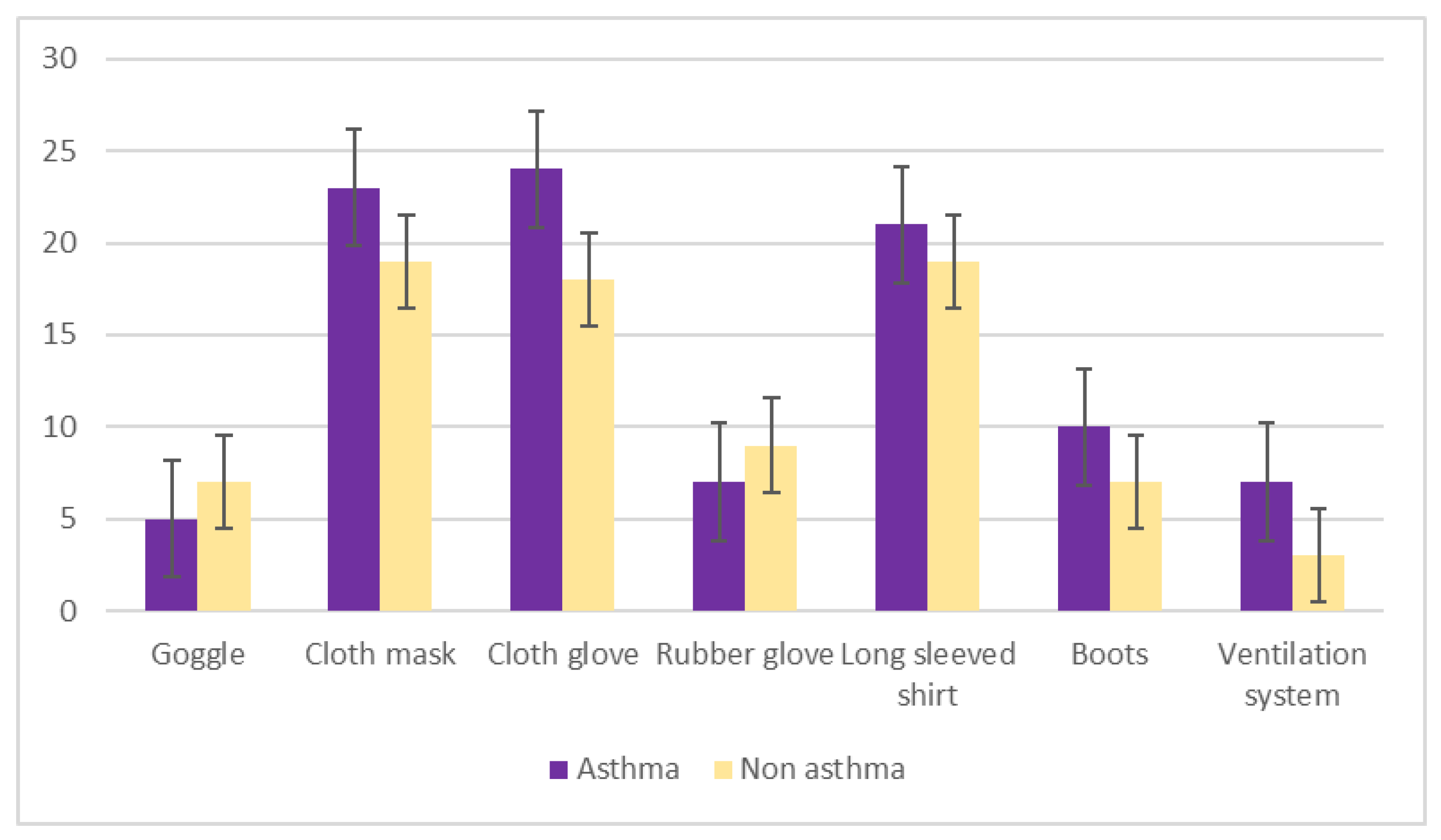
3.2. Occupational and Environmental Factors Related to E-Waste Handling
3.3. Heavy Metal Concentrations in House Dust and Airborne Dust of E-Waste and Non-E-Waste Related House
3.4. Heavy Metal Concentrations in House Dust and Airborne Dust Stratified by Village
3.5. Heavy Metal. Levels in Blood and Urine
3.6. Association with Asthma
4. Discussion
4.1. Heavy Metal Concentrations in Air and Dust
4.2. Heavy Metal. Concentrations in Blood and Urine
4.3. Association with Asthma
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ravi, V. Evaluating the overall quality of recycling of e-waste from end of life computers. J. Clean Prod. 2012, 20, 145–151. [Google Scholar] [CrossRef]
- Kiddee, P.; Naidu, R.; Wong, M.H. Electronic waste management approaches: An overview. Waste Manag. 2013, 33, 1237–1250. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.; Dietmar, R.; Eugster, M. The recycling and disposal of electrical and electronic waste in China-legislative and market responses. Environ. Impact. Assess Rev. 2005, 25, 459–471. [Google Scholar] [CrossRef]
- Robinson, B.H. E-waste: An assessment of global production and environmental impacts. Sci. Total Environ. 2009, 408, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Perkins, D.N.; Drisse, M.N.B.; Nxele, T.; Sly, P.D. E-waste: A global hazard. Ann. Glob. Health 2014, 80, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Chareonsong, P. E-Waste Management in Thailand. In Proceedings of the 4th International E-Waste Management Network (IEMN) Workshop, Hanoi, Vietnam, 14–17 July 2014; Available online: https://www.epa.gov/sites/production/files/2014-08/documents/thailand_country_presentation.Pdf (accessed on 15 January 2016).
- Schluep, M.; Hagelueken, C.; Kuehr, R.; Magalini, F.; Maurer, C.; Meskers, C.; Mueller, E.; Wang, F. Recycling-From E-Waste to Resources; UNEP–DTIE: Paris, France, 2009. [Google Scholar]
- Luo, C.; Liu, C.; Wang, Y.; Liu, X.; Li, F.; Zhang, G.; Li, X. Heavy metal contamination in soils and vegetables near an e-waste processing site, South China. J. Hazard. Mater. 2011, 186, 481–490. [Google Scholar] [CrossRef]
- Tang, X.; Shen, C.; Shi, D.; Cheema, S.A.; Khan, M.I.; Zhang, C.; Chen, Y. Heavy metal and persistent organic compound contamination in soil from Wenling: An emerging e-waste recycling city in Taizhou area, China. J. Hazard. Mater. 2010, 173, 653–660. [Google Scholar] [CrossRef]
- Lui, M.; Huang, B.; Bi, X.; Ren, Z.; Sheng, G.; Fu, J. Heavy metals and organic compounds contamination in soil from an e-waste region in South China. Environ. Sci. Process. Impacts 2013, 15, 919–929. [Google Scholar]
- Vetrivel, P.; Devi, P.K. A Focus on E-waste: Effects on Environment and Human Health. IJNTPS 2012, 2, 47–51. [Google Scholar]
- Obeng-Gyasi, E.; Armijos, R.X.; Weigel, M.M.; Filippelli, G.; Sayegh, M.A. Hepatobiliary-related outcomes in US adults exposed to Lead. Environments 2018, 5, 46. [Google Scholar] [CrossRef]
- Harari, F.; Sallsten, G.; Christensson, A.; Petkovic, M.; Hedblad, B.; Forsgard, N.; Melander, O.; Nilsson, P.M.; Borne, Y.; Engström, G.; et al. Blod lead levels and devreased kidney function on a population-based cohort. Am. J. Kidney Dis. 2018, 72, 381–389. [Google Scholar] [CrossRef]
- Bellinger, D.C. Very low lead exposures and children’s neurodevelopment. Curr. Opin. Pediatr. 2008, 20, 172–177. [Google Scholar] [CrossRef] [PubMed]
- ATSDR. Public Statement for Chromium. Available online: http://https://www.atsdr.cdc.gov/ToxProfiles/tp7-c1-b.pdf (accessed on 3 January 2018).
- Xu, X.; Zeng, X.; Boezen, H.M.; Huo, X. E-waste environmental contamination and harm to public health in China. Front. Med. 2015, 9, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Moira, C.Y.; Stephen, L. Occupational Asthma. Am. Rev. Respir. Dis. 1986, 133, 686–703. [Google Scholar]
- Costa, L.G.; Giordano, G. Developmental neurotoxicity of polybrominated diphenyl ether (PBDE) flame retardants. Neurotoxicology 2007, 28, 1047–1067. [Google Scholar] [CrossRef] [PubMed]
- Shy, C.G.; Huang, H.L.; Chang-Chien, G.P.; Chao, H.R.; Tsou, T.C. Neurodevelopment of infants with prenatal exposure to polybrominated diphenyl esters. Bull. Environ. Contam. Toxicol. 2011, 87, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Frazzoli, C.; Orisakwe, O.E.; Dragone, R.; Mantovani, A. Diagnostic health risk assessment of electronic waste on the general population in developing countries’ scenarios. Environ. Impact Assess. Rev. 2010, 30, 388–399. [Google Scholar] [CrossRef]
- Realff, M.J.; Raymond, M.; Ammons, J.C. E-waste: An opportunity. Mater. Today 2004, 7, 40–45. [Google Scholar] [CrossRef]
- Wang, J.; Cen, H.; Xia, W.; Chen, L.; Zhao, J.; Li, G. Heavy metal pollution in the surface dust from E-waste disposal place and its ecological risk assessment. Adv. Mater. Res. 2012, 347–353, 2360–2364. [Google Scholar] [CrossRef]
- Zahir, F.; Rizwi, S.J.; Haq, S.K.; Khan, R.H. Low dose mercury toxicity and human health. Environ. Toxicol. Pharmacol. 2005, 20, 351–360. [Google Scholar] [CrossRef]
- Umesh, K.; Singh, D.N. Electronic Waste: Concerns & Hazardous Threats. IJCET 2014, 4, 801–811. [Google Scholar]
- Park, S.; Lee, E.H.; Kho, Y. The association of asthma, total IgE, and blood lead and cadmium levels. J. Allergy Clin. Immuniol. 2016, 138, 1702–1703.e6. [Google Scholar] [CrossRef] [PubMed]
- Bureau of Environmental Health, Department of Health, Ministry of Public Health. Report of the Surveillance Risk Area: Case of E-Waste: BanKok Sub-Distric, Kuenagnai District, Ubon Ratchthani Province; Department of Health: Bangkok, Thailand, 2015. [Google Scholar]
- Apter, A.J. Advances in the care of adults with asthma and allergy. J. Allergy Clin. Immunol. 2008, 121, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Lin, R.L. Heavy metals zinc, cadmium, and copper stimulate pulmonary sensory neurons via direct activation of TRPA1. J. Appl. Physiol. 2010, 108, 891–897. [Google Scholar] [CrossRef] [PubMed]
- BanKok Health Care Center. 43 Profile Report of Public Health Service in Heath Care Center; BanKok Health Care Center: Ubon Ratchathani, Thailand, 2016. [Google Scholar]
- BanKlang Health Care Center. 43 Profile Report of Public Health Service in Heath Care Center; BanKlang Health Care Center: Ubon Ratchathani, Thailand, 2016. [Google Scholar]
- American Society for Testing and Materials (ASTM). Standard Practice for Collection of Settled Dust Samples Using Wipe Sampling Methods for Subsequent Determination of Metals. Available online: https://www.astm.org/Standards/D6966.htm (accessed on 20 January 2016).
- Seaton, A.; Godden, D.J.; Brown, K. Increase in asthma: A more toxic environment or a more susceptible population? Thorax 1994, 49, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.L.; Wong, W.H.; Lau, Y.L. Association between air pollution and asthma admission among children in Hong Kong. Clin. Exp. Allergy 2006, 36, 1138–1146. [Google Scholar] [CrossRef]
- Patel, M.M.; Hoepner, L.; Garfinkel, R.; Chillrud, S.; Reyes, A.; Quinn, J.W.; Perera, F.; Miller, R.L. Ambient metals, elemental carbon, and wheeze and cough in New York City children through 24 months of Age. Am. J. Respir. Critl. Care Med. 2009, 180, 1107–1113. [Google Scholar] [CrossRef]
- Leung, A.O.W.; Duzgoren-Aydin, N.S.; Cheung, K.C.; Wong, M.H. Heavy metals concentrations of surface dust from e-waste recycling and its human health implications in Southeast China. Environ. Sci. Technol. 2008, 42, 2674–2680. [Google Scholar] [CrossRef]
- Adaramodu, A.A.; Osuntogun, A.O.; Ehi-Eromosele, C.O. Heavy metal concentration of surface dust present in e-waste components: The Westminister electronis market, Lagos case study. Resour. Environ. 2012, 2, 9–13. [Google Scholar] [CrossRef]
- Guo, Y.; Huang, C.J.; Zhang, H.; Dong, Q.X. Heavy metal contamination from electronic waste recycling at Guiyu, Southeastern China. J. Environ. Qual. 2009, 38, 1617–1626. [Google Scholar] [CrossRef]
- Uchida, N.; Matsukami, H.; Someya, M.; Tue, N.M.; Tuyen, L.H.; Viet, P.H.; Takahashi, S.; Tanabe, S.; Suzuki, G. Hazardous metals emissions from e-waste-processing sites in a village in northern Vietnam. Emerg. Contam. 2018, 4, 11–21. [Google Scholar] [CrossRef]
- Igharo, G.O.; Anetor, J.I.; Osibanjo, O.O.; Osadolor, H.B.; Dike, K.C. Toxic metal levels in Nigerian electronic waste workers indicate occupational metal toxicity associated with crude electronic waste management practices. Biokemistri 2015, 26, 107–113. [Google Scholar]
- Zeng, X.; Xu, X.; Zheng, X.; Reponen, T.; Chen, A.; Huo, X. Heavy metals in PM2.5 and in blood, and children’s respiratory symptoms and asthma from an e-waste recycling area. Environ. Pollut. 2016, 210, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Chen, K.H.; Yan, X.; Chen, S.J.; Hu, G.C.; Peng, X.W.; Yuan, J.G.; Mai, B.X.; Yang, Z.Y. Heavy metals in food, house dust, and water from an e-waste recycling area in South China and the potential risk to human health. Ecotoxicol. Environ. Saf. 2013, 96, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Wittsiepe, J.; Feldt, T.; Till, H.; Burchard, G.; Wilhelm, M.; Fobil, J.N. Pilot study on the internal exposure to heavy metals of informal-level electronic waste workers in Agbogbloshie, Accra, Ghana. Environ. Sci. Pollut. Res. 2017, 24, 3097–3107. [Google Scholar] [CrossRef]
- Prachachat. Inhibition of Electronics Waste Import from China, Ministry of Commerce Issued a Ban on Import. 2018. Available online: https://www.prachachat.net/economy/news-404099 (accessed on 20 December 2019). (In Thai).
- Huang, X.; Xie, J.; Cui, X.; Zhou, Y.; Wu, X.; Lu, W.; Shen, Y.; Yuan, J.; Chen, W. Association between Concentrations of Metals in Urine and Adult Asthma: A Case-Control Study in Wuhan, China. PLoS ONE 2016, 11, e0155818. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristic | BanKok | BanKlang | Total | |||
|---|---|---|---|---|---|---|
| Asthma (n = 42) | Non-Asthma (n = 42) | Asthma (n = 9) | Non- Asthma (n = 9) | Asthma (n = 51) | Non- Asthma (n = 51) | |
| Age (years) | ||||||
| 24–46 | 14 | 14 | 1 | 0 | 15 | 14 |
| 47–68 | 25 | 25 | 7 | 8 | 32 | 33 |
| ≥ 68 | 3 | 3 | 1 | 1 | 4 | 4 |
| Mean ± SD | 51.5 ± 12.1 | 51.5 ± 11.3 | 58.8 ± 6.8 | 57.8 ± 8.6 | 52.8 ± 11.6 | 52.8 ± 11.0 |
| Gender | ||||||
| Male | 17 | 18 | 4 | 3 | 21 | 21 |
| Female | 25 | 24 | 5 | 6 | 30 | 30 |
| Education | ||||||
| Primary | 34 | 33 | 6 | 7 | 40 | 40 |
| Secondary | 1 | 5 | 1 | 1 | 2 | 6 |
| High school | 7 | 4 | 1 | 1 | 8 | 5 |
| Income (unit: Thai Baht) | ||||||
| 1000–5699 | 22 | 31 | 6 | 5 | 28 | 36 |
| 5700–10,399 | 18 | 11 | 3 | 3 | 21 | 14 |
| ≥ 10,400 | 7 | 0 | 0 | 0 | 7 | 0 |
| Mean ± SD | 6095.2 ± 3621.1 | 4542.9 ± 2474.6 | 4433.3 ± 3651.0 | 6444.4 ± 4186.6 | 5801.9 ± 3646.2 | 4878.4 ± 2891.7 |
| Smoking | ||||||
| None | 33 | 30 | 7 | 5 | 40 | 35 |
| Ex-smoke | 1 | 2 | 1 | 2 | 2 | 4 |
| Smoker | 8 | 10 | 1 | 2 | 9 | 12 |
| Frequency of asthma symptom | ||||||
| 1 time per week | 4 | - | 2 | - | 6 | - |
| 1 time per month | 10 | - | 2 | - | 12 | - |
| 1 time per six months | 28 | - | 5 | - | 33 | - |
| E-Waste Related House (46) | Non-E-Waste Related House (56) | p | |||||
|---|---|---|---|---|---|---|---|
| Range | Mean ± SD | Median IQR | Range | Mean ± SD | Median IQR | ||
| House dust (mg/kg) | |||||||
| Cr | ND–6.33 | 1.69 ± 1.29 | 1.52 | 0.02–5.87 | 0.99 ± 1.05 | 0.94 | 0.000 |
| Hg | ND–1.04 | 0.09 ± 0.20 | 0.10 | ND–0.79 | 0.04 ± 0.11 | 0.04 | 0.077 |
| Ni | ND–7.88 | 1.46 ± 1.42 | 1.23 | ND–12.00 | 0.92 ± 1.61 | 0.79 | 0.005 |
| Pb | ND–79.27 | 7.53 ± 13.46 | 6.94 | ND–16.93 | 3.00 ± 3.86 | 0.94 | 0.001 |
| Air dust (µg/m3) | |||||||
| Cr | ND–0.13 | 0.03 ± 0.03 | 0.03 | ND–0.14 | 0.03 ± 0.04 | 0.05 | 0.318 |
| Hg | ND–0.25 | 0.14 ± 0.06 | 0.09 | ND–0.26 | 0.11 ± 0.07 | 0.12 | 0.013 |
| Ni | ND–0.11 | 0.03 ± 0.03 | 0.05 | ND–0.13 | 0.03 ± 0.03 | 0.05 | 0.842 |
| Pb | ND–1.66 | 0.09 ± 0.25 | 0.11 | ND–0.23 | 0.06 ± 0.07 | 0.12 | 0.620 |
| BanKok (84) | BanKlang (18) | p | |||||
|---|---|---|---|---|---|---|---|
| Range | Mean ± SD | Median IQR | Range | Mean ± SD | Median IQR | ||
| House dust (mg/kg) | |||||||
| Cr | ND–6.33 | 1.51 ± 1.24 | 1.56 | 0.06–1.11 | 0.37 ± 0.30 | 0.40 | 0.000 |
| Hg | ND–1.04 | 0.07 ± 0.17 | 0.08 | ND–0.10 | 0.02 ± 0.03 | 0.04 | 0.328 |
| Ni | ND–12.00 | 1.32 ± 1.65 | 1.11 | ND–1.55 | 0.45 ± 0.42 | 0.51 | 0.000 |
| Pb | ND–79.27 | 5.86 ± 10.49 | 6.49 | ND–5.43 | 1.24 ± 1.66 | 2.09 | 0.000 |
| Air dust (µg/m3) | |||||||
| Cr | ND–0.14 | 0.03 ± 0.04 | 0.05 | ND–0.06 | 0.01 ± 0.02 | 0.01 | 0.001 |
| Hg | ND–0.26 | 0.14 ± 0.06 | 0.09 | ND–0.12 | 0.05 ± 0.03 | 0.02 | 0.000 |
| Ni | ND–0.13 | 0.04 ± 0.04 | 0.06 | ND | ND | ND | 0.000 |
| Pb | ND–1.66 | 0.09 ± 0.19 | 1.24 | ND–0.12 | 0.01 ± 0.03 | ND | 0.000 |
| Asthma (51) | Non Asthma (51) | p | |||||
|---|---|---|---|---|---|---|---|
| Range | Mean ± SD | Median IQR | Range | Mean ± SD | Median IQR | ||
| House dust (mg/kg) | |||||||
| Cr | ND–6.33 | 1.31 ± 1.23 | 1.35 | 0.03–5.87 | 1.30 ± 1.21 | 1.48 | 0.894 |
| Hg | ND–0.79 | 0.06 ± 0.16 | 0.07 | ND–1.04 | 0.07 ± 0.16 | 0.08 | 0.944 |
| Ni | ND–4.60 | 1.02 ± 0.87 | 0.87 | ND–12.00 | 1.31 ± 1.99 | 1.41 | 0.671 |
| Pb | ND–23.47 | 3.83 ± 4.64 | 4.64 | ND–79.27 | 6.26 ± 12.76 | 6.00 | 0.955 |
| Air dust (µg/m3) | |||||||
| Cr | ND–0.14 | 0.03 ± 0.03 | 0.05 | ND–0.13 | 0.02 ± 0.03 | 0.04 | 0.049 |
| Hg | 0.02–0.25 | 0.13 ± 0.07 | 0.13 | ND–0.26 | 0.12 ± 0.07 | 0.08 | 0.651 |
| Ni | ND–0.13 | 0.03 ± 0.03 | 0.06 | ND–0.13 | 0.03 ± 0.03 | 0.05 | 0.294 |
| Pb | ND–0.23 | 0.07 ± 0.07 | 0.12 | ND–1.66 | 0.08 ± 0.23 | 0.12 | 0.629 |
| Heavy Metal in Biological Sample Heading | Asthma (51) | Non Asthma (51) | p | ||||
|---|---|---|---|---|---|---|---|
| Range | Mean ± SD | Median IQR | Range | Mean ± SD | Median IQR | ||
| Blood Pb (µg/dL) | 0.89–8.50 | 4.80± 1.97 | 3.14 | 1.61–9.67 | 4.83 ± 2.16 | 3.23 | 0.857 * |
| Urinary Cr (µg/g creatinine) | ND–4.99 | 0.69 ± 0.99 | 0.53 | 0.06–5.03 | 0.71 ± 0.89 | 0.64 | 0.410 ** |
| Urinary Hg (µg/g creatinine) | 0.07–52.64 | 3.69± 8.60 | 1.51 | 0.31–24.16 | 3.06 ± 4.43 | 1.81 | 0.933 ** |
| Urinary Ni (µg/g creatinine) | 0.73–29.82 | 5.63 ± 6.66 | 3.33 | 0.25–99.96 | 6.81 ± 14.44 | 3.76 | 0.960 ** |
| Heavy Metal in Biological Sample | E-Waste (46) | Non E-Waste (56) | p | ||||
|---|---|---|---|---|---|---|---|
| Range | Mean ± SD | Median IQR | Range | Mean ± SD | Median IQR | ||
| Blood Pb (µg/dL) | 0.89–9.67 | 4.69 ± 2.16 | 3.24 | 1.94–9.41 | 4.91± 1.90 | 3.11 | 0.749 * |
| Urinary Cr (µg/g creatinine) | 0.02–5.03 | 0.71 ±1.05 | 0.52 | 0.06–4.51 | 0.69 ± 0.84 | 0.59 | 0.574 ** |
| Urinary Hg (µg/g creatinine) | 0.07–52.64 | 4.64 ± 9.36 | 2.29 | 0.25–24.16 | 2.34 ± 3.35 | 1.04 | 0.382 * |
| Urinary Ni (µg/g creatinine) | 0.44–99.96 | 8.34 ± 15.87 | 4.99 | 0.25–23.54 | 4.48 ± 4.53 | 2.91 | 0.352 ** |
| Heavy Metal in Biological Sample | BanKok (84) | BanKlang (18) | p | ||||
|---|---|---|---|---|---|---|---|
| Range | Mean ± SD | Median IQR | Range | Mean ± SD | Median IQR | ||
| Blood Pb (µg/dL) | 0.89–9.67 | 4.70 ± 2.11 | 3.27 | 2.74–7.98 | 5.34± 1.39 | 1.68 | 0.608 * |
| Urinary Cr (µg/g creatinine) | ND–5.03 | 0.68 ±0.99 | 0.49 | 0.15–2.54 | 0.80 ± 0.64 | 0.75 | 0.040 ** |
| Urinary Hg (µg/g creatinine) | 0.07–52.64 | 3.78 ± 7.45 | 1.86 | 0.33–3.36 | 1.50 ± 0.73 | 1.05 | 0.2260 ** |
| Urinary Ni (µg/g creatinine) | 0.30–99.96 | 6.48 ± 12.16 | 3.57 | 0.25–23.54 | 4.99 ± 5.55 | 4.47 | 0.629 ** |
| Variables | Dependent Variables | p-Value | ||
|---|---|---|---|---|
| Asthma (%) | Non Asthma (%) | |||
| Subject characteristics | ||||
| Age group (years) | ||||
| 24–46.99 | 14 | 16 | 0.907 | |
| 47–68.99 | 33 | 31 | ||
| ≥69 | 4 | 4 | ||
| Income (Thai baht) | ||||
| 1000–5699 | 28 | 35 | 0.236 | |
| 5700–10,399 | 22 | 14 | ||
| ≥10,400 | 1 | 2 | ||
| Education | ||||
| Primary | 41 | 39 | 0.405 | |
| Higher than primary | 40 | 12 | ||
| Smoking behavior | ||||
| None smoker | 40 | 37 | 0.730 | |
| Ex-smoker | 2 | 4 | ||
| Smoker | 9 | 10 | ||
| Occupational factors | ||||
| Current work | ||||
| Related to E-waste | 26 | 20 | 0.233 | |
| Not related to E-waste | 25 | 31 | ||
| Position in E-waste activity | ||||
| Employee | 12 | 10 | 0.683 | |
| Registered owner | 3 | 2 | ||
| Non registered owner | 11 | 8 | ||
| Not related to E-waste | 25 | 31 | ||
| Work hours (Hours per day) | ||||
| 1–2.99 | 8 | 11 | 0.736 | |
| 2–5.99 | 18 | 16 | ||
| ≥6 | 25 | 24 | ||
| Years of work | ||||
| 1–2.99 | 30 | 31 | 0.035 | |
| 3–5.99 | 7 | 12 | ||
| ≥6 | 14 | 8 | ||
| Family member works in e-waste activity | ||||
| yes | 22 | 13 | 0.061 | |
| no | 29 | 38 | ||
| House beside e-waste shop | ||||
| yes | 16 | 12 | 0.375 | |
| no | 35 | 35 | ||
| House cleaning | ||||
| 7 days per week | 26 | 24 | 0.912 | |
| 2–3 days per week | 18 | 20 | ||
| 1 day per week | 7 | 7 | ||
| Kitchen in E-waste related activities area | ||||
| yes | 9 | 3 | 0.065 | |
| no | 42 | 48 | ||
| Blood lead level (µg/dL) | ||||
| 0.89–5.29 | 28 | 31 | 0.574 | |
| ≥5.30 | 23 | 20 | ||
| Urinary chromium (µg/g creatinine) | ||||
| 0.06–2.59 | 49 | 49 | 1.000 | |
| ≥2.60 | 2 | 2 | ||
| Urinary nickel (µg/g creatinine) | ||||
| 0.30–33.39 | 51 | 49 | 0.361 | |
| 33.40–66.49 | 0 | 1 | ||
| ≥66.50 | 0 | 1 | ||
| Urinary mercury (µg/g creatinine) | ||||
| 0.07–29.99 | 49 | 51 | 0.153 | |
| ≥30 | 2 | 0 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuntawee, C.; Tantrakarnapa, K.; Limpanont, Y.; Lawpoolsri, S.; Phetrak, A.; Mingkhwan, R.; Worakhunpiset, S. Exposure to Heavy Metals in Electronic Waste Recycling in Thailand. Int. J. Environ. Res. Public Health 2020, 17, 2996. https://doi.org/10.3390/ijerph17092996
Kuntawee C, Tantrakarnapa K, Limpanont Y, Lawpoolsri S, Phetrak A, Mingkhwan R, Worakhunpiset S. Exposure to Heavy Metals in Electronic Waste Recycling in Thailand. International Journal of Environmental Research and Public Health. 2020; 17(9):2996. https://doi.org/10.3390/ijerph17092996
Chicago/Turabian StyleKuntawee, Chalermkhwan, Kraichat Tantrakarnapa, Yanin Limpanont, Saranath Lawpoolsri, Athit Phetrak, Rachaneekorn Mingkhwan, and Suwalee Worakhunpiset. 2020. "Exposure to Heavy Metals in Electronic Waste Recycling in Thailand" International Journal of Environmental Research and Public Health 17, no. 9: 2996. https://doi.org/10.3390/ijerph17092996
APA StyleKuntawee, C., Tantrakarnapa, K., Limpanont, Y., Lawpoolsri, S., Phetrak, A., Mingkhwan, R., & Worakhunpiset, S. (2020). Exposure to Heavy Metals in Electronic Waste Recycling in Thailand. International Journal of Environmental Research and Public Health, 17(9), 2996. https://doi.org/10.3390/ijerph17092996