Comorbidities and Outcome of Alcoholic and Non-Alcoholic Liver Cirrhosis in Taiwan: A Population-Based Study


 , and
, and
Abstract
1. Introduction
2. Methods
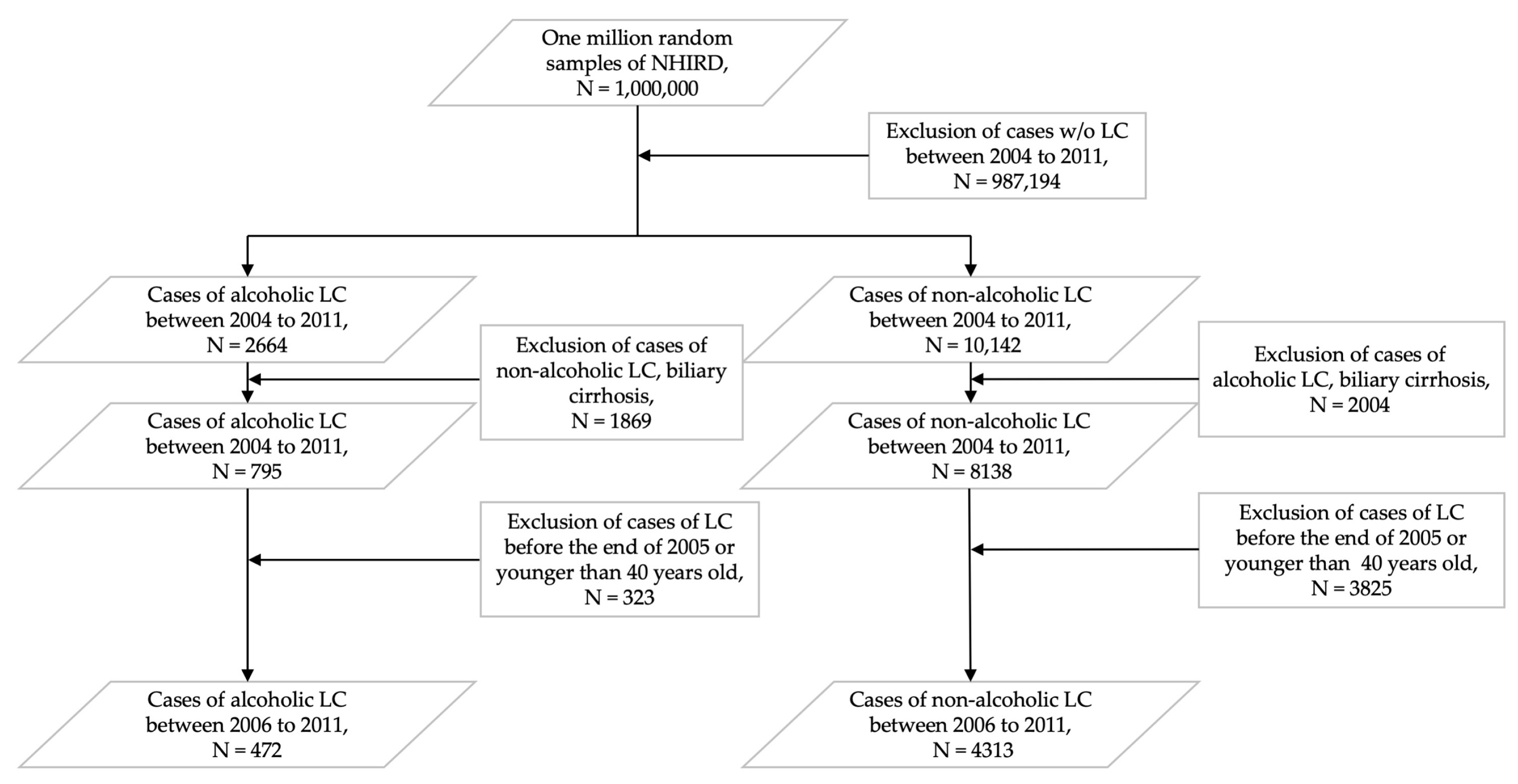
2.1. Study Population and Design
2.2. Comorbidities and Complications
2.3. Study Endpoint Measurement
2.4. Statistical and Data Analysis
2.5. Ethics
3. Results
3.1. Concomitant Comorbidities and Complications of Liver Cirrhosis
3.2. Hazard Ratios for Comorbidities, Complications of Liver Cirrhosis, and Survival
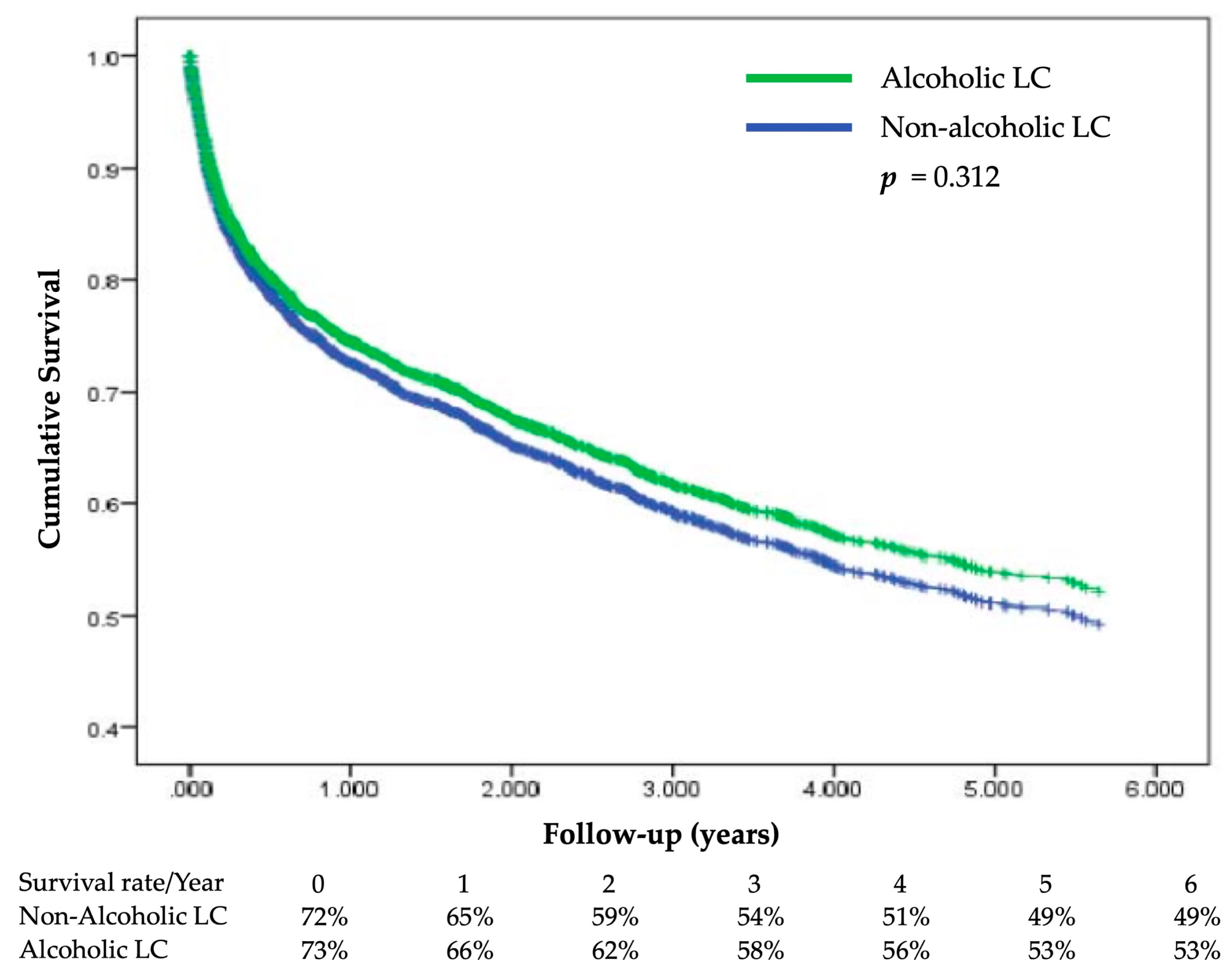
3.3. Survival Analysis Between the Two Study Groups
4. Discussion
4.1. Main Findings
4.2. Comparison with Other Studies
4.3. Clinical Implications
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of liver diseases in the world. J. Hepatol. 2019, 70, 151–171. [Google Scholar] [CrossRef]
- Tsochatzis, E.A.; Bosch, J.; Burroughs, A.K. Liver cirrhosis. Lancet 2014, 383, 1749–1761. [Google Scholar] [CrossRef]
- Rehm, J.; Samokhvalov, A.V.; Shield, K.D. Global burden of alcoholic liver diseases. J. Hepatol. 2013, 59, 160–168. [Google Scholar] [CrossRef]
- Ratib, S.; Fleming, K.M.; Crooks, C.J.; Walker, A.J.; West, J. Causes of death in people with liver cirrhosis in England compared with the general population: A population-based cohort study. Am. J. Gastroenterol. 2015, 110, 1149–1158. [Google Scholar] [CrossRef] [PubMed]
- Fleming, K.M.; Aithal, G.P.; Card, T.R.; West, J. All-cause mortality in people with cirrhosis compared with the general population: A population-based cohort study. Liver Int. 2012, 32, 79–84. [Google Scholar] [CrossRef] [PubMed]
- D′Amico, G.; Garcia-Tsao, G.; Pagliaro, L. Natural history and prognostic indicators of survival in cirrhosis: A systematic review of 118 studies. J. Hepatol. 2006, 44, 217–231. [Google Scholar]
- Jepsen, P.; Vilstrup, H.; Andersen, P.K.; Lash, T.L.; Sorensen, H.T. Comorbidity and survival of Danish cirrhosis patients: A nationwide population-based cohort study. Hepatology 2008, 48, 214–220. [Google Scholar] [CrossRef]
- Jepsen, P.; Vilstrup, H.; Lash, T.L. Development and validation of a comorbidity scoring system for patients with cirrhosis. Gastroenterology 2014, 146, 147–156. [Google Scholar] [CrossRef]
- Myers, R.P.; Tandon, P.; Ney, M.; Meeberg, G.; Faris, P.; Shaheen, A.A.; Aspinall, A.I.; Burak, K.W. Validation of the five-variable Model for End-stage Liver Disease (5vMELD) for prediction of mortality on the liver transplant waiting list. Liver Int. 2014, 34, 1176–1183. [Google Scholar] [CrossRef]
- Xu, Y.; Li, N.; Lu, M.; Dixon, E.; Myers, R.P.; Jolley, R.J.; Quan, H. Comparison of risk adjustment methods in patients with liver disease using electronic medical record data. BMC Gastroenterol. 2017, 17, 5. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Kim, W.R. The model for end-stage liver disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Polaris Observatory, C. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: A modelling study. Lancet Gastroenterol. Hepatol. 2018, 3, 383–403. [Google Scholar]
- Chen, C.H.; Yang, P.M.; Huang, G.T.; Lee, H.S.; Sung, J.L.; Sheu, J.C. Estimation of seroprevalence of hepatitis B virus and hepatitis C virus in Taiwan from a large-scale survey of free hepatitis screening participants. J. Formos. Med Assoc. Taiwan Yi Zhi 2007, 106, 148–155. [Google Scholar] [CrossRef]
- Su, S.Y.; Lee, W.C. Mortality Trends of Liver Diseases from 1981 to 2016 and the Projection to 2035 in Taiwan: An Age-Period-Cohort Analysis. Liver Int. 2019, 39, 770–776. [Google Scholar] [CrossRef]
- Jinjuvadia, R.; Liangpunsakul, S. Trends in Alcoholic Hepatitis-related Hospitalizations, Financial Burden, and Mortality in the United States. J. Clin. Gastroenterol. 2015, 49, 506–511. [Google Scholar]
- Liangpunsakul, S.; Haber, P.; McCaughan, G.W. Alcoholic Liver Disease in Asia, Europe, and North America. Gastroenterology 2016, 150, 1786–1797. [Google Scholar] [CrossRef]
- Fan, J.G. Epidemiology of alcoholic and nonalcoholic fatty liver disease in China. J. Gastroenterol. Hepatol. 2013, 28 Suppl 1, 11–17. [Google Scholar] [CrossRef]
- Wang, H.; Ma, L.; Yin, Q.; Zhang, X.; Zhang, C. Prevalence of alcoholic liver disease and its association with socioeconomic status in north-eastern China. Alcohol Clin. Exp. Res. 2014, 38, 1035–1041. [Google Scholar] [CrossRef]
- Eng, M.Y.; Luczak, S.E.; Wall, T.L. ALDH2, ADH1B, and ADH1C genotypes in Asians: A literature review. Alcohol Res. Health 2007, 30, 22–27. [Google Scholar]
- Li, T.K. Quantifying the risk for alcohol-use and alcohol-attributable health disorders: Present findings and future research needs. J. Gastroenterol. Hepatol. 2008, 23 (Suppl. 1), S2–S8. [Google Scholar] [CrossRef]
- Abe, H.; Aida, Y.; Seki, N.; Sugita, T.; Tomita, Y.; Nagano, T.; Itagaki, M.; Sutoh, S.; Nagatsuma, K.; Itoh, K.; et al. Aldehyde dehydrogenase 2 polymorphism for development to hepatocellular carcinoma in East Asian alcoholic liver cirrhosis. J. Gastroenterol. Hepatol. 2015, 30, 1376–1383. [Google Scholar] [CrossRef]
- Singh, G.K.; Hoyert, D.L. Social epidemiology of chronic liver disease and cirrhosis mortality in the United States, 1935–1997: Trends and differentials by ethnicity, socioeconomic status, and alcohol consumption. Hum. Biol. 2000, 72, 801–820. [Google Scholar] [PubMed]
- Henriksen, J.H.; Moller, S. Liver cirrhosis and arterial hypertension. World J. Gastroenterol. 2006, 12, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, I. Comparison of the relationships of alcohol intake with atherosclerotic risk factors in men with and without diabetes mellitus. Alcohol. Alcohol. 2011, 46, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Kim, K. Association of alcohol consumption with lipid profile in hypertensive men. Alcohol 2012, 47, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Vieira, B.A.; Luft, V.C.; Schmidt, M.I.; Chambless, L.E.; Chor, D.; Barreto, S.M.; Duncan, B.B. Timing and Type of Alcohol Consumption and the Metabolic Syndrome—ELSA-Brasil. PLoS ONE 2016, 11, e0163044. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Alcoholic Cirrhosis | Non-Alcoholic Cirrhosis | p-Value | ||
|---|---|---|---|---|---|
| N = 472 | N = 4313 | ||||
| N | % | N | % | ||
| Sex | <0.001 | ||||
| Male | 447 | 94.7 | 2699 | 62.6 | |
| Female | 25 | 5.3 | 1614 | 37.4 | |
| Age (years) | <0.001 | ||||
| 40–49 | 220 | 46.6 | 601 | 13.9 | |
| 50–59 | 152 | 32.2 | 1015 | 23.5 | |
| 60–69 | 68 | 14.4 | 974 | 22.6 | |
| >69 | 32 | 6.8 | 1723 | 39.9 | |
| Residence | <0.001 | ||||
| Metropolis | 246 | 52.1 | 2403 | 55.7 | |
| General area | 205 | 43.4 | 1837 | 42.6 | |
| Remote area | 20 | 4.2 | 68 | 1.6 | |
| Income (New Taiwan Dollar (NTD) per month) | <0.001 | ||||
| 0–14,009 | 201 | 42.6 | 2175 | 50.4 | |
| 14,010-42,030 | 248 | 52.5 | 1838 | 42.6 | |
| >42,939 | 22 | 4.7 | 295 | 6.8 | |
| Etiologies of non-alcoholic cirrhosis | |||||
| Hepatitis B | 1417 | 32.9 | |||
| Hepatitis C | 1377 | 31.9 | |||
| Non-alcoholic fatty liver disease | 428 | 9.9 | |||
| Others (biliary cirrhosis excluded) | 1091 | 25.3 | |||
| Comorbidity | <0.001 | ||||
| Yes | 324 | 68.6 | 3431 | 79.6 | |
| No | 148 | 31.4 | 882 | 20.4 | |
| Coronary heart disease (CAD) | 63 | 13.3 | 1091 | 25.3 | <0.001 |
| Cerebrovascular disease | |||||
| Hemorrhage | 15 | 3.2 | 578 | 13.4 | <0.001 |
| Ischemia | 24 | 5.1 | 684 | 15.9 | <0.001 |
| Hypertension | 197 | 41.7 | 2526 | 58.6 | <0.001 |
| Heart failure (HF) | 25 | 5.3 | 551 | 12.8 | <0.001 |
| Diabetes mellitus (DM) | 137 | 29.0 | 1584 | 36.7 | <0.001 |
| Chronic kidney disease (CKD) | 72 | 15.3 | 970 | 22.5 | <0.001 |
| Hyperlipidemia | 118 | 25.0 | 1035 | 24.0 | 0.629 |
| Chronic obstructive pulmonary disease (COPD) | 59 | 12.5 | 903 | 20.9 | <0.001 |
| Complication of cirrhosis | 0.007 | ||||
| Yes | 152 | 32.2 | 1663 | 38.6 | |
| No | 320 | 67.8 | 2650 | 61.4 | |
| Ascites or peritonitis | 79 | 16.7 | 1012 | 23.5 | <0.001 |
| Hepatic encephalopathy | 54 | 11.4 | 553 | 12.8 | 0.392 |
| Esophageal varices | 57 | 12.1 | 656 | 15.2 | 0.069 |
| Esophageal varices without bleeding | 25 | 5.3 | 396 | 9.2 | 0.005 |
| Esophageal varices with bleeding | 45 | 9.5 | 456 | 10.6 | 0.484 |
| Variable | Alcoholic Cirrhosis | Non-Alcoholic Cirrhosis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted Hazard Ratio | a Adjusted Hazard Ratio | Unadjusted Hazard Ratio | a Adjusted Hazard Ratio | |||||||||
| Risk Ratio | 95% CI | p-Value | Risk Ratio | 95% CI | p-Value | Risk Ratio | 95% CI | p-Value | Risk Ratio | 95% CI | p-Value | |
| Sex | ||||||||||||
| Male | 0.703 | 0.371–1.335 | 0.282 | 0.777 | 0.399–1.512 | 0.458 | 1.114 | 1.008–1.232 | 0.034 | 1.241 | 1.119-1.376 | <0.001 |
| Female (reference) | ||||||||||||
| Age (years) | ||||||||||||
| 40–49 (reference) | ||||||||||||
| 50–59 | 1.255 | 0.877–1.795 | 0.214 | 1.335 | 0.923–1.930 | 0.124 | 1.070 | 0.883–1.297 | 0.489 | 1.114 | 0.918–1.351 | 0.275 |
| 60–69 | 0.793 | 0.465–1.353 | 0.395 | 0.848 | 0.489–1.472 | 0.559 | 1.258 | 1.041–1.521 | 0.017 | 1.344 | 1.105–1.635 | 0.003 |
| >69 | 2.541 | 1.540–4.193 | <0.001 | 2.004 | 1.115–3.603 | 0.020 | 2.487 | 2.104–2.939 | <0.001 | 2.675 | 2.229–3.212 | <0.001 |
| Comorbidity | ||||||||||||
| Coronary heart disease | 1.098 | 0.700–1.723 | 0.685 | 1.170 | 0.703-1.948 | 0.546 | 1.129 | 1.014-1.257 | 0.027 | 0.886 | 0.785-1.000 | 0.050 |
| Cerebrovascular disease | ||||||||||||
| Hemorrhage | 1.799 | 0.883–3.666 | 0.106 | 1.578 | 0.732–3.400 | 0.244 | 1.356 | 1.077–1.706 | 0.01 | 1.377 | 1.090–1.738 | 0.007 |
| Ischemia | 1.279 | 0.692–2.361 | 0.432 | 0.879 | 0.439–1.758 | 0.715 | 1.221 | 1.071–1.393 | 0.003 | 0.950 | 0.827–1.092 | 0.470 |
| Hypertension | 0.845 | 0.614–1.162 | 0.300 | 0.684 | 0.471–0.994 | 0.046 | 1.059 | 0.960–1.167 | 0.253 | 0.783 | 0.698–0.878 | <0.001 |
| Heart failure | 1.393 | 0.754–2.571 | 0.290 | 0.981 | 0.477–2.016 | 0.958 | 1.510 | 1.328–1.715 | <0.001 | 1.136 | 0.987–1.308 | 0.076 |
| Diabetes mellitus | 0.958 | 0.683–1.343 | 0.802 | 1.056 | 0.732–1.524 | 0.771 | 1.047 | 0.949–1.156 | 0.360 | 1.090 | 0.981–1.212 | 0.110 |
| Chronic kidney disease | 2.137 | 1.488–3.070 | <0.001 | 2.276 | 1.520–3.409 | <0.001 | 1.881 | 1.698–2.084 | <0.001 | 1.751 | 1.571–1.951 | <0.001 |
| Hyperlipidemia | 0.452 | 0.293–0.699 | <0.001 | 0.447 | 0.282–0.708 | <0.001 | 0.574 | 0.505–0.653 | <0.001 | 0.571 | 0.499–0.652 | <0.001 |
| Chronic obstructive pulmonary disease | 1.227 | 0.800-1.883 | 0.348 | 1.240 | 0.789-1.951 | 0.351 | 1.346 | 1.205-1.502 | <0.001 | 0.994 | 0.883-1.119 | 0.920 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, T.-W.; Wang, C.-C.; Tsai, M.-C.; Wang, Y.-T.; Tseng, M.-H.; Lin, C.-C. Comorbidities and Outcome of Alcoholic and Non-Alcoholic Liver Cirrhosis in Taiwan: A Population-Based Study. Int. J. Environ. Res. Public Health 2020, 17, 2825. https://doi.org/10.3390/ijerph17082825
Yang T-W, Wang C-C, Tsai M-C, Wang Y-T, Tseng M-H, Lin C-C. Comorbidities and Outcome of Alcoholic and Non-Alcoholic Liver Cirrhosis in Taiwan: A Population-Based Study. International Journal of Environmental Research and Public Health. 2020; 17(8):2825. https://doi.org/10.3390/ijerph17082825
Chicago/Turabian StyleYang, Tzu-Wei, Chi-Chih Wang, Ming-Chang Tsai, Yao-Tung Wang, Ming-Hseng Tseng, and Chun-Che Lin. 2020. "Comorbidities and Outcome of Alcoholic and Non-Alcoholic Liver Cirrhosis in Taiwan: A Population-Based Study" International Journal of Environmental Research and Public Health 17, no. 8: 2825. https://doi.org/10.3390/ijerph17082825
APA StyleYang, T.-W., Wang, C.-C., Tsai, M.-C., Wang, Y.-T., Tseng, M.-H., & Lin, C.-C. (2020). Comorbidities and Outcome of Alcoholic and Non-Alcoholic Liver Cirrhosis in Taiwan: A Population-Based Study. International Journal of Environmental Research and Public Health, 17(8), 2825. https://doi.org/10.3390/ijerph17082825