Global Incidence and Mortality Patterns of Pedestrian Road Traffic Injuries by Sociodemographic Index, with Forecasting: Findings from the Global Burden of Diseases, Injuries, and Risk Factors 2017 Study

 ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Data Source and Data Extraction
2.2. Sociodemographic Index
2.3. Outcome Metrics
2.4. Uncertainty Intervals
2.5. Statistical Analysis
3. Results
3.1. Incidence and Trends
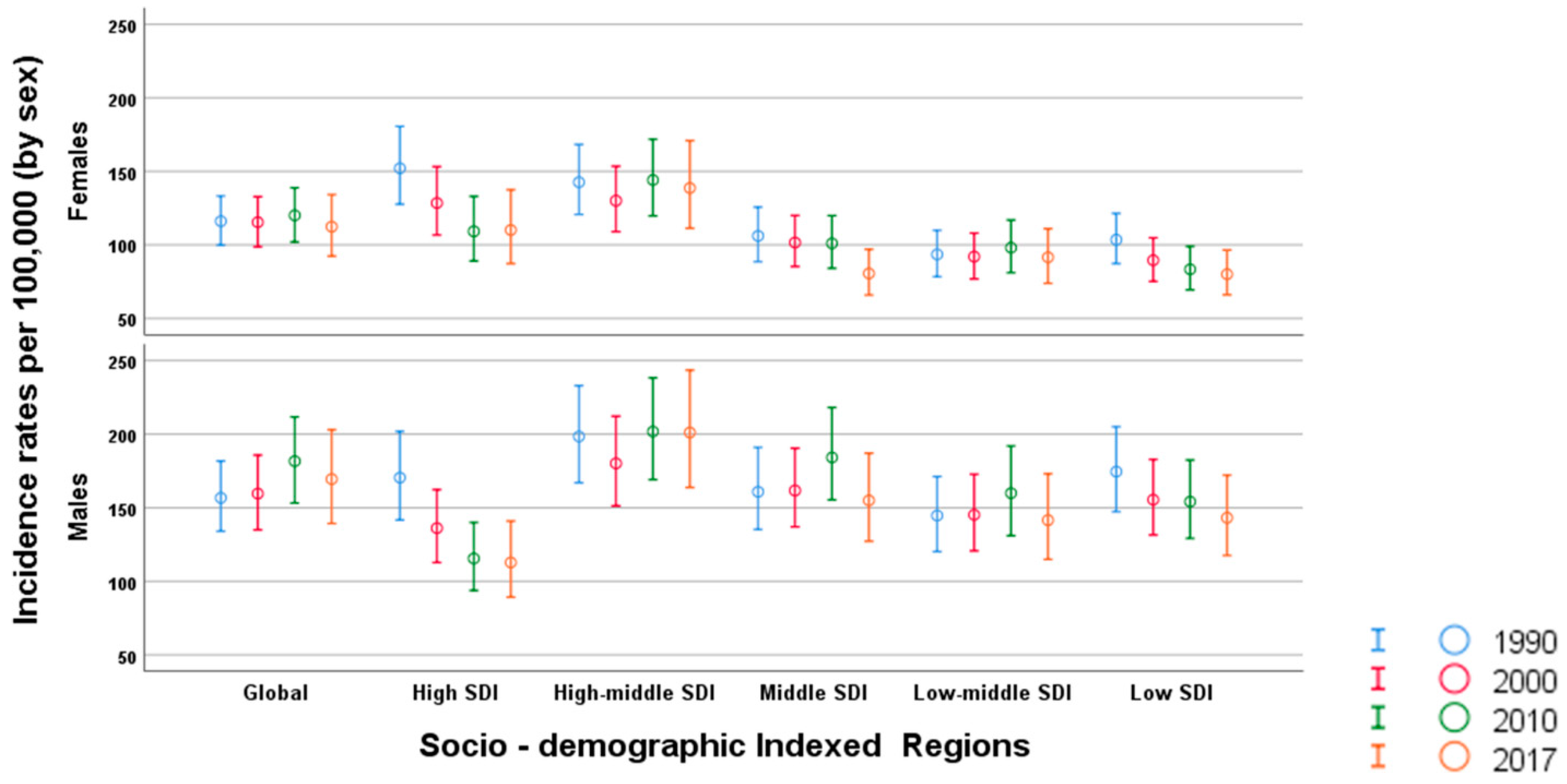
3.2. Incidence and Trends by Age and Sex
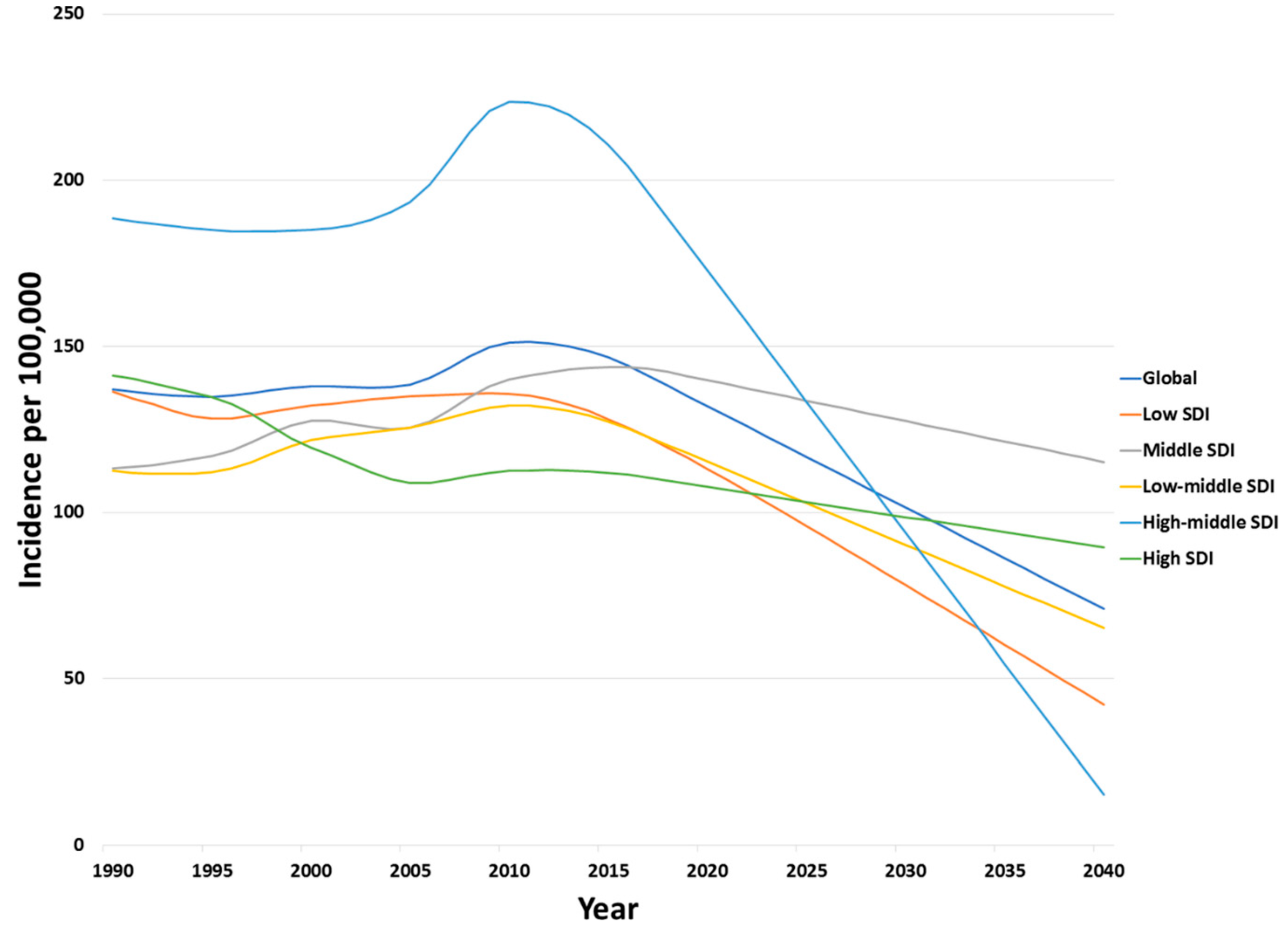
3.3. Forecasted Incidence Trends
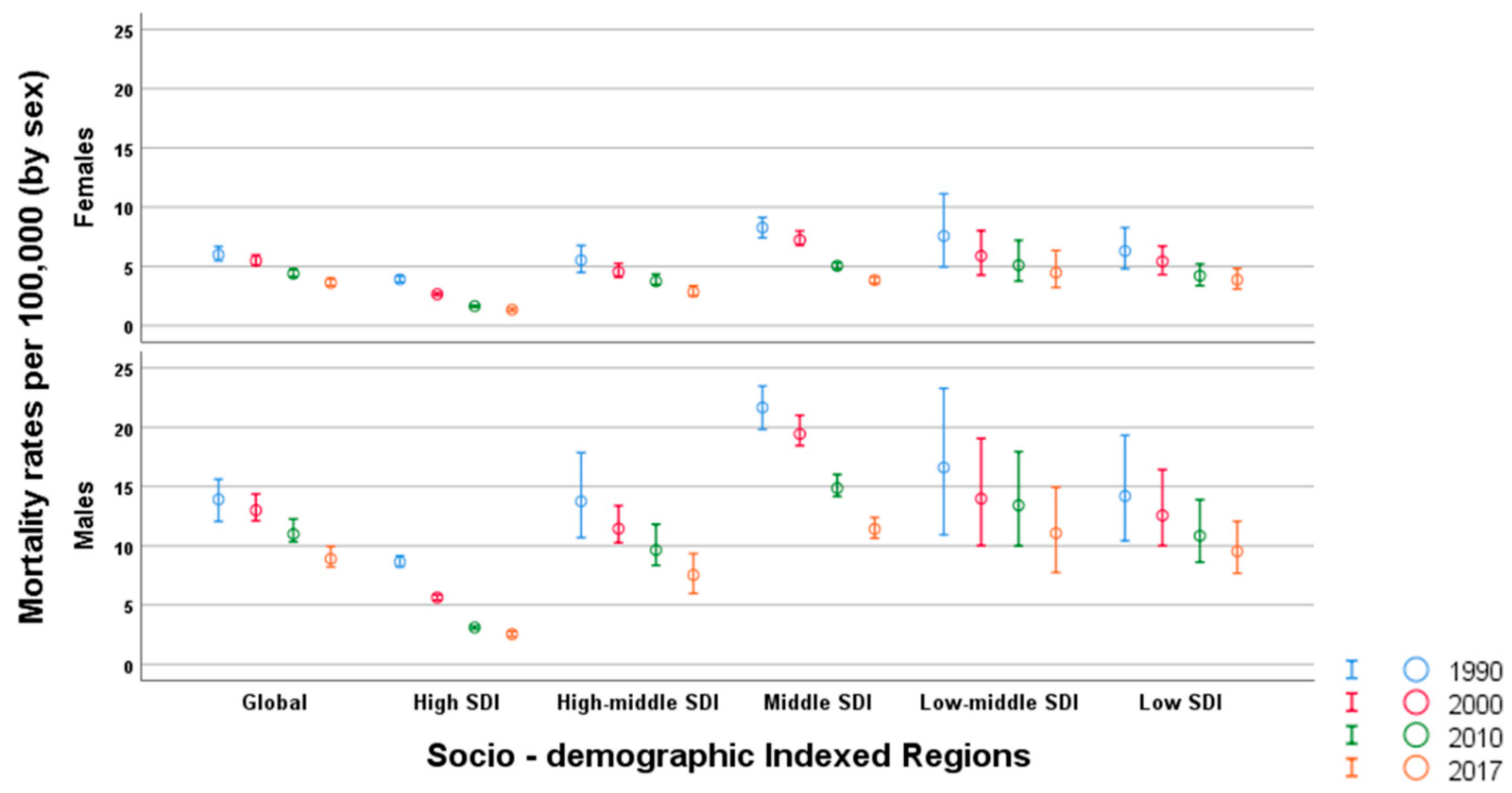
3.4. Mortality and Trends
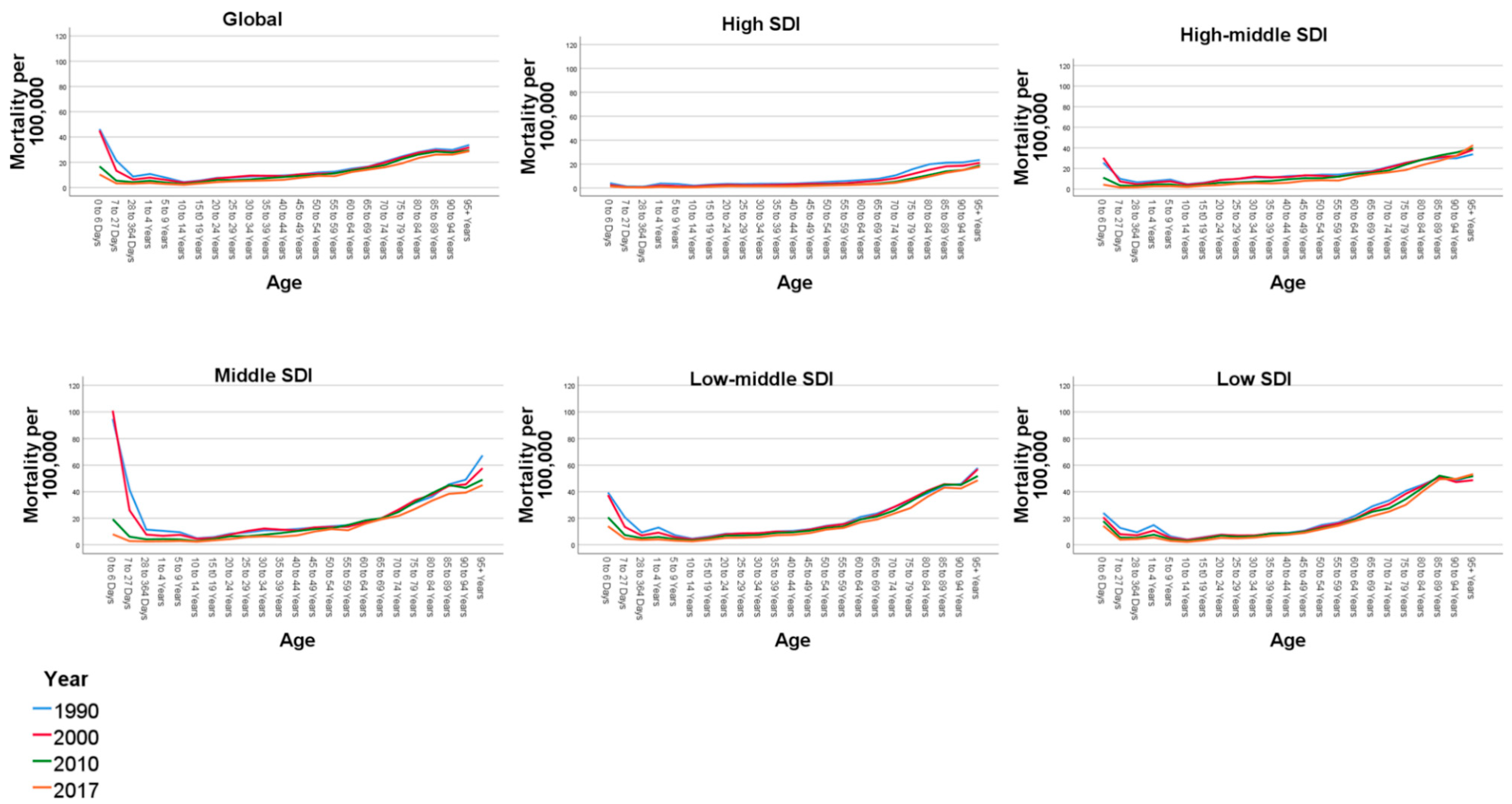
3.5. Mortality Trends by Age and Sex
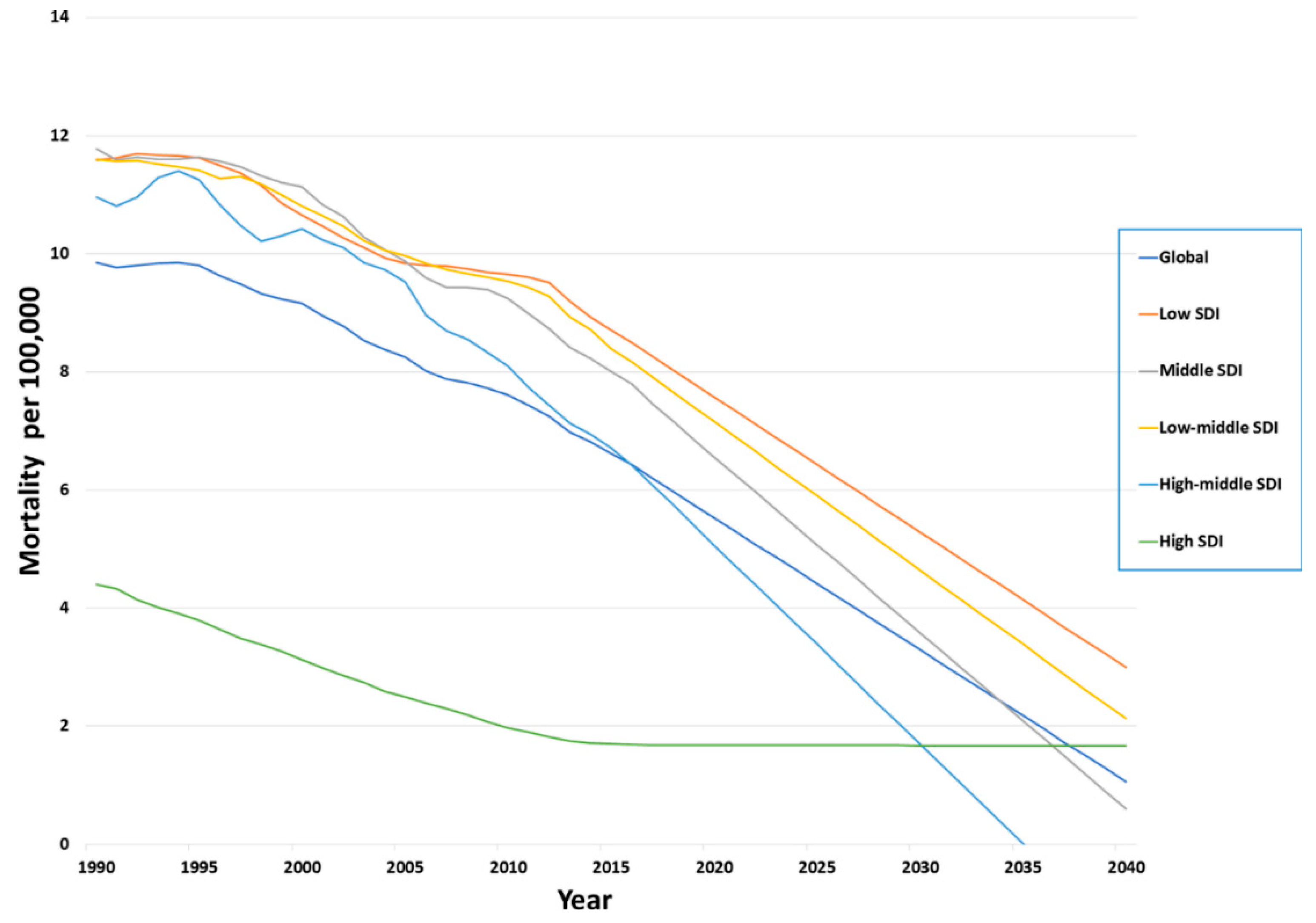
3.6. Forecasted Trends of Mortality
4. Discussion
5. Limitations
Future Work
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Status Report on Road Safety 2018: Summary; (WHO/NMH/NVI/1820) Licence: CC BY-NC-SA 30 IGO; World Health Organization: Geneva, Switzerland, 2018; Available online: https://apps.who.int/iris/bitstream/handle/10665/277370/WHO-NMH-NVI-18.20-eng.pdf?ua=1 (accessed on 29 January 2020).
- Bartolomeos, K.; Croft, P.; Job, S.; Khayes, M.; Kobusingye, O.; Peden, M.; Schwebel, D.; Sleet, D.; Tiwari, G.; Turner, B.; et al. Pedestrian Safety: A Road Safety Manual for Decision-Makers and Practitioners; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Kim, J.-K.; Ulfarsson, G.-F.; Shankar, V.N.; Kim, S. Age and pedestrian injury severity in motor-vehicle crashes: A heteroskedastic logit analysis. Accid. Anal. Prev. 2008, 40, 1695–1702. [Google Scholar] [CrossRef] [PubMed]
- Mayou, R.; Bryant, B. Consequences of road traffic accidents for different types of road user. Injury 2003, 34, 197–202. [Google Scholar] [CrossRef]
- Mohan, D.; Khayesi, M.; Tiwari, G.; Nafukho, F.M. Road Traffic Injury Prevention Training Manual; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Toroyan, T.; Khayesi, M.; Peden, M. Time to prioritise safe walking. Int. J. Inj. Control Saf. Promot. 2013, 20, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, G.; Hill, R.; Lewis, V. Children’s attentional skills and road behaviour. J. Exp. Psychol. Appl. 2001, 7, 227–234. [Google Scholar] [CrossRef]
- Arnett, J. Developmental sources of crash risk in young drivers. Inj. Prev. 2002, 8, ii17–ii23. [Google Scholar]
- Converso, D.; Sottimano, I.; Guidetti, G.; Loera, B.; Cortini, M.; Viotti, S. Aging and Work Ability: The Moderating Role of Job and Personal Resources. Front. Psychol. 2018, 8, 2262. [Google Scholar] [CrossRef]
- UN. The Sustainable Development Goals. Goal 3: Ensure Healthy Lives and Promote Well-Being for All at All Ages. Available online: https://www.un.org/sustainabledevelopment/health/ (accessed on 24 January 2020).
- Trafikverket, Swedish Transport Administration. Saving Lives Beyond 2020: The Next Steps—Recommendations of the Academic Expert Group for the Third Ministerial Conference on Global Road Safety; Swedish Transport Administration: Stockholm, Sweden, 2019.
- James, S.L.; Lucchesi, L.R.; Bisignano, C.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Liu, Z.; McCracken, D.; Nixon, M.R.; et al. Morbidity and mortality from road injuries: Results from the Global Burden of Disease Study 2017. Inj. Prev. 2020. [Google Scholar] [CrossRef]
- Leach-Kemon, K.; Gall, J. Why Estimate? Institute for Health Metrics and Evaluation. 2018. Available online: http://www.healthdata.org/acting-data/why-estimate (accessed on 28 December 2019).
- Naghavi, M.; Aajobir, A.A.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abera, S.F.; Agrawal, A. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- Global Burden of Diseases. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- McKee, S. Rethinking Development and Health: Findings from the GLOBAL Burden of Disease Study; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2016; p. 14. [Google Scholar]
- IHME. Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2017 (GBD 2017) Socio-Demographic Index (SDI) 1950–2017. Available online: http://ghdx.healthdata.org/record/ihme-data/gbd-2017-socio-demographic-index-sdi-1950%E2%80%932017 (accessed on 29 January 2020).
- Mathers, C.D.; Salomon, J.A.; Ezzati, M.; Begg, S.; Vander Hoorn, S.; Lopez, A.D. Sensitivity and uncertainty analyses for burden of disease and risk factor estimates. In Global Burden of Disease and Risk Factors; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2006. [Google Scholar]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef]
- National Center for Statistics and Analysis. (2015, July) Overview: 2013 Data. Available online: https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/812196 (accessed on 29 January 2020).
- Bazargan-Hejazi, S.; Ahmadi, A.; Shirazi, A.; Ainy, E.; Djalalinia, S.; Fereshtehnejad, S.M.; Jahanmehr, N.; Kiadaliri, A.; Moradi-Lakeh, M.; Parsaeian, M.; et al. The Burden of Road Traffic Injuries in Iran and 15 Surrounding Countries: 1990–2016. Arch. Iran. Med. 2018, 21, 556–565. [Google Scholar] [PubMed]
- Juillard, C.; Etoundi Mballa, G.A.; Bilounga Ndongo, C.; Stevens, K.A.; Hyder, A.A. Patterns of injury and violence in Yaoundé Cameroon: An analysis of hospital data. World J. Surg. 2011, 35, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Charters, K.E.; Gabbe, B.J.; Mitra, B. Population incidence of pedestrian traffic injury in high-income countries: A systematic review. Injury 2017, 48, 1331–1338. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Al-Habib, A.; Alaqeel, A.; Marwa, I.; Almohammadi, M.; Al Shalaan, H.; AlEissa, S.; Zamakhshary, M.; Al-Bedah, K.; Al-Enazi, S.; Mukhtar, F. Causes and patterns of spine trauma in children and adolescents in Saudi Arabia: Implications for injury prevention. Ann. Saudi Med. 2014, 34, 31–37. [Google Scholar] [CrossRef]
- Hobday, M.B.; Knight, S. Motor vehicle collisions involving adult pedestrians in eThekwini in 2007. Int. J. Inj Control. Saf. Promot. 2010, 17, 61–68. [Google Scholar] [CrossRef]
- Da Costa, J.P.; Laing, J.; Kong, V.Y.; Bruce, J.L.; Laing, G.L.; Clarke, D.L. A review of geriatric injuries at a major trauma centre in South Africa. South Afr. Med. J. 2019, 110, 44–48. [Google Scholar] [CrossRef]
- Patel, D.C.; Dhillon, N.K.; Linaval, N.; Patel, K.; Margulies, D.R.; Ley, E.J.; Barmparas, G. Data-Driven Opportunity to Reduce Elderly Pedestrian Trauma. Am. Surg. 2019, 85, 466–470. [Google Scholar]
- Seah, R.; Lystad, R.P.; Curtis, K.; Mitchell, R. Socioeconomic variation in injury hospitalisations in Australian children ≤ 16 years: A 10-year population-based cohort study. BMC Public Health 2018, 18, 1336. [Google Scholar] [CrossRef]
- Desapriya, E.; Sones, M.; Ramanzin, T.; Weinstein, S.; Scime, G.; Pike, I. Injury prevention in child death review: Child pedestrian fatalities. Inj. Prev. 2011, 17, i4–i9. [Google Scholar] [CrossRef] [PubMed]
- Laflamme, L.; Diderichsen, F. Social differences in traffic injury risks in childhood and youth—A literature review and a research agenda. Inj. Prev. 2000, 6, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Strukcinskiene, B.; Uğur-Baysal, S.; Raistenskis, J. Traffic injury mortality trends in children and adolescents in Lithuania among road users. Turk. J. Pediatr. 2014, 56, 285–290. [Google Scholar] [PubMed]
- Griffin, B.; Watt, K.; Kimble, R.; Wallis, B.; Shields, L. Systematic literature review of incidence rates of low-speed vehicle run-over incidents in children. Worldviews Evid. Based Nurs. 2014, 11, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.L.; Christou, E.; Rosengren, K.S. Children achieve adult-like sensory integration during stance at 12-years-old. Gait Posture 2006, 23, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Bartels, D.; Bhalla, K.; Shahraz, S.; Abraham, J.; Lozano, R.; Murray, C.J. Incidence of road injuries in Mexico: Country report. Int. J. Inj. Control Saf. Promot. 2010, 17, 169–176. [Google Scholar] [CrossRef]
- Munivenkatappa, A.; Pruthi, N.; Philip, M.; Devi, B.I.; Somanna, S. Elderly pedestrian neurotrauma: A descriptive study from a premier neurotrauma center in India. J. Neurosci. Rural. Pract. 2013, 4, 29–32. [Google Scholar] [CrossRef]
- Sze, N.N.; Su, J.; Bai, L. Exposure to pedestrian crash based on household survey data: Effect of trip purpose. Accid. Anal. Prev. 2019, 128, 17–24. [Google Scholar] [CrossRef]
- Azami-Aghdash, S.; Aghaei, M.H.; Sadeghi-Bazarghani, H. Epidemiology of Road Traffic Injuries among Elderly People; A Systematic Review and Meta-Analysis. Bull. Emerg. Trauma 2018, 6, 279–291. [Google Scholar] [CrossRef]
- Sadeghi-Bazargani, H.; Samadirad, B.; Moslemi, F. A decade of road traffic fatalities among the elderly in north-West Iran. BMC Public Health 2018, 18, 111. [Google Scholar] [CrossRef]
- Demetriades, D.; Murray, J.; Martin, M.; Velmahos, G.; Salim, A.; Alo, K.; Rhee, P. Pedestrians injured by automobiles: Relationship of age to injury type andseverity. J. Am. Coll. Surg. 2004, 199, 382–387. [Google Scholar] [CrossRef]
- Rebollo-Soria, M.C.; Arregui-Dalmases, C.; Sánchez-Molina, D.; Velázquez-Ameijide, J.; Galtés, I. Injury pattern in lethal motorbikes-pedestrian collisions, in the area of Barcelona, Spain. J. Forensic Leg. Med. 2016, 43, 80–84. [Google Scholar] [CrossRef]
- Solagberu, B.A.; Balogun, R.A.; Mustafa, I.A.; Ibrahim, N.A.; Oludara, M.A.; Ajani, A.O.; Idowu, O.E.; Osuoji, R.I. Pedestrian injuries in the most densely populated city in Nigeria-an epidemic calling for control. Traffic Inj. Prev. 2015, 16, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Matsui, Y.; Oikawa, S.; Ando, K. Risks of pedestrian serious injuries and fatalities associated with impact velocities of cars in car-versus-pedestrian accidents in Japan. Stapp Car Crash J. 2013, 57, 201–217. [Google Scholar] [PubMed]
- Moran, D.; Bose, D.; Bhalla, K. Impact of improving vehicle crashworthiness design on the burden of injuries to pedestrians in USA, Germany and India. Traffic Inj. Prev. 2017, 18, 832–838. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, C.M.; Barry, W.E.; Barin, E.N.; Mert, M.; Lowery, C.; Upperman, J.S.; Jensen, A.R.; Arbogast, H. Interactive Education is Associated With Lower Incidence of Pedestrian-Related Injury in Children. J. Surg. Res. 2019, 244, 57–62. [Google Scholar] [CrossRef]
- Morrongiello, B.A.; Corbett, M.; Beer, J.; Koutsoulianos, S. A Pilot Randomized Controlled Trial Testing the Effectiveness of a Pedestrian Training Program That Teaches Children Where and How to Cross the Street Safely. J. Pediatr. Psychol. 2018, 43, 1147–1159. [Google Scholar] [CrossRef]
- Duperrex, O.; Roberts, I.; Bunn, F. Safety education of pedestrians for injury prevention. Cochrane Database Syst. Rev. 2002. [Google Scholar] [CrossRef]
- Lunevicius, R.; Herbert, H.K.; Hyder, A.A. The epidemiology of road traffic injuries in the Republic of Lithuania, 1998–2007. Eur. J. Public Health 2010, 20, 702–706. [Google Scholar] [CrossRef]
- Thomas, M.; Riemann, B.; Jones, J. Epidemiology of alcohol and drug screening among pedestrian fatalities in the United States, 2014–2016. Traffic Inj. Prev. 2019, 20, 557–562. [Google Scholar] [CrossRef]
- Fox, L.; Serre, M.L.; Lippmann, S.J.; Rodríguez, D.A.; Bangdiwala, S.I.; Gutiérrez, M.I.; Escobar, G.; Villaveces, A. Spatiotemporal approaches to analyzing pedestrian fatalities: The case of Cali, Colombia. Traffic Inj. Prev. 2015, 16, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Retting, R.A.; Ferguson, S.A.; McCartt, A.T. A review of evidence-based traffic engineering measures designed to reduce pedestrian-motor vehicle crashes. Am. J. Public Health 2003, 93, 1456–1463. [Google Scholar] [CrossRef] [PubMed]
- Chalabi, Z.; Roberts, I.; Edwards, P.; Dowie, J. Traffic and the risk of vehicle-related pedestrian injury: A decision analytic support tool. Inj. Prev. 2008, 14, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Kudryavtsev, A.V.; Nilssen, O.; Lund, J.; Grjibovski, A.M.; Ytterstad, B. Road traffic crashes with fatal and non-fatal injuries in Arkhangelsk, Russia in 2005–2010. Int. J. Inj. Control Saf. Promot. 2013, 20, 349–357. [Google Scholar] [CrossRef][Green Version]
- Loewe, M.; Rippin, N. Translating an Ambitious Vision into Global Transformation: The 2030 Agenda for Sustainable Development; DIE Discussion Paper 2015/7. Available online: https://www.die-gdi.de/discussion-paper/article/translating-an-ambitious-vision-into-globaltransformation-the-2030-agenda-for-sustainable-development/ (accessed on 2 February 2020).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category |
| |||
|---|---|---|---|---|
| 1990 | 2000 | 2010 | 2017 | |
| Global | 136.4 (116.91–157.46) | 137.49 (116.86–159.26) | 150.85 (127.55–175.26) | 140.92 (115.81–168.53) |
| High SDI | 140 (118.69–163.47) | 118.63 (100.3–138.74) | 112.06 (93.04–133.03) | 110.05 (88.33–135.33) |
| High–middle SDI | 187.46 (159.72–216.89) | 184.39 (156.05–213.86) | 223.15 (188.96–259.89) | 195.52 (160.55–234.45) |
| Middle SDI | 113.08 (96.17–131.72) | 127.27 (108.04–147.98) | 140.04 (118.79–162.58) | 143.19 (118–171.35) |
| Low–middle SDI | 112.34 (95.31–131.22) | 121.58 (103.23–142.46) | 132.21 (110.98–155.84) | 122.9 (100.75–147.7) |
| Low SDI | 136.25 (116.2–158.91) | 132.01 (112.5–153.71) | 135.76 (114.39–160.5) | 122.81 (101.48–147.67) |
| ||||
| Global | 9.94 (8.75–11.14) | 9.23 (8.59–10.16) | 7.68 (7.21–8.5) | 6.25 (5.77–6.94) |
| High SDI | 4.47 (4.37–4.61) | 3.16 (3.11–3.22) | 1.99 (1.95–2.03) | 1.69 (1.64–1.76) |
| High–middle SDI | 11.1 (9.56–12.64) | 10.54 (10–11.25) | 8.2 (7.89–8.97) | 6.14 (5.72–6.67) |
| Middle SDI | 11.8 (10.35–13.23) | 11.17 (10.47–12.22) | 9.32 (8.84–10.06) | 7.52 (6.98–8.18) |
| Low–middle SDI | 11.57 (9.92–13.87) | 10.82 (9.6–12.69) | 9.59 (8.41–11.3) | 7.99 (6.8–9.58) |
| Low SDI | 11.48 (9.27–14.01) | 10.6 (9.06–12.54) | 9.64 (8.48–11.26) | 8.29 (7.24–9.64) |
| Category |
| ||
|---|---|---|---|
| 1990 to 2017 | 2000 to 2017 | 2010 to 2017 | |
| Global | 3.31 (−9.94 to 16.56) | 2.49 (−9.99 to 14.97) | −6.58 (−14.25 to 1.09) |
| High SDI | −21.39 (−35.03 to −7.74) | −7.23 (−20.16 to 5.7) | −1.79 (−9.75 to 6.17) |
| High–middle SDI | 4.29 (−9.81 to 18.39) | 6.03 (−7.41 to 19.47) | −12.38 (−20.64 to −4.11) |
| Middle SDI | 26.62 (8.87 to 44.36) | 12.5 (−4.28 to 29.28) | 2.24 (−8.25 to 12.73) |
| Low–middle SDI | 9.4 (−6.93 to 25.73) | 1.08 (−15.27 to 17.43) | −7.04 (−16.63 to 2.55) |
| Low SDI | −9.86 (−25.26 to 5.54) | −6.96 (−22.39 to 8.47) | −9.53 (−18.58 to −0.47) |
| |||
| Global | −37.12 (−45.19 to −29.04) | −32.28 (−40.31 to −24.24) | −18.61 (−23.32 to −13.89) |
| High SDI | −62.19 (−70.48 to −53.89) | −46.51 (−54.84 to −38.17) | −15.07 (−19.95 to −10.18) |
| High–middle SDI | −44.68 (−52.97 to −36.38) | −41.74 (−50.21 to −33.26) | −25.12 (−30.19 to −20.04) |
| Middle SDI | −36.27 (−43.23 to −29.3) | −32.67 (−42.32 to −23.01) | −19.31 (−25.92 to −12.69) |
| Low–middle SDI | −30.94 (−37.56 to −24.31) | −26.15 (−34.6 to −17.69) | −16.68 (−22.41 to −10.94) |
| Low SDI | −27.78 (−34.61 to −20.94) | −21.79 (−29.91 to −13.66) | −14 (−19.41 to −8.58) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, M.A.B.; Grivna, M.; Nauman, J.; Soteriades, E.S.; Cevik, A.A.; Hashim, M.J.; Govender, R.; Al Azeezi, S.R. Global Incidence and Mortality Patterns of Pedestrian Road Traffic Injuries by Sociodemographic Index, with Forecasting: Findings from the Global Burden of Diseases, Injuries, and Risk Factors 2017 Study. Int. J. Environ. Res. Public Health 2020, 17, 2135. https://doi.org/10.3390/ijerph17062135
Khan MAB, Grivna M, Nauman J, Soteriades ES, Cevik AA, Hashim MJ, Govender R, Al Azeezi SR. Global Incidence and Mortality Patterns of Pedestrian Road Traffic Injuries by Sociodemographic Index, with Forecasting: Findings from the Global Burden of Diseases, Injuries, and Risk Factors 2017 Study. International Journal of Environmental Research and Public Health. 2020; 17(6):2135. https://doi.org/10.3390/ijerph17062135
Chicago/Turabian StyleKhan, Moien A. B., Michal Grivna, Javaid Nauman, Elpidoforos S. Soteriades, Arif Alper Cevik, Muhammad Jawad Hashim, Romona Govender, and Salma Rashid Al Azeezi. 2020. "Global Incidence and Mortality Patterns of Pedestrian Road Traffic Injuries by Sociodemographic Index, with Forecasting: Findings from the Global Burden of Diseases, Injuries, and Risk Factors 2017 Study" International Journal of Environmental Research and Public Health 17, no. 6: 2135. https://doi.org/10.3390/ijerph17062135
APA StyleKhan, M. A. B., Grivna, M., Nauman, J., Soteriades, E. S., Cevik, A. A., Hashim, M. J., Govender, R., & Al Azeezi, S. R. (2020). Global Incidence and Mortality Patterns of Pedestrian Road Traffic Injuries by Sociodemographic Index, with Forecasting: Findings from the Global Burden of Diseases, Injuries, and Risk Factors 2017 Study. International Journal of Environmental Research and Public Health, 17(6), 2135. https://doi.org/10.3390/ijerph17062135