A Cost-Minimization Analysis of a Medical Record-based, Store and Forward and Provider-to-provider Telemedicine Compared to Usual Care in Catalonia: More Agile and Efficient, Especially for Users

 , ,
, , 
Abstract
1. Introduction
2. Methodology
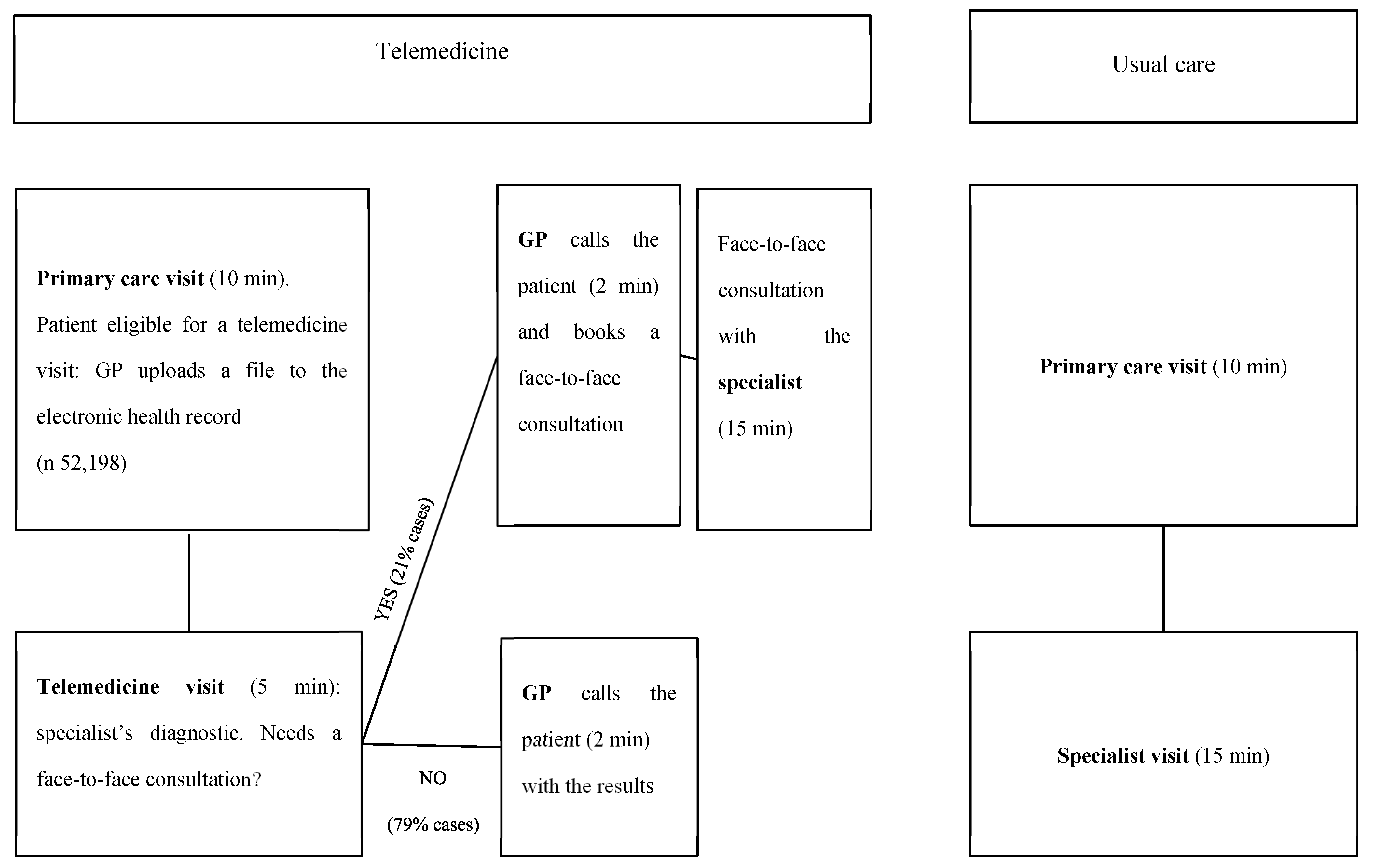
2.1. Service Description
2.2. Study Type
2.3. Direct Costs
2.4. Indirect Costs
3. Results
Sensitivity Analysis: An Even More Favorable Scenario for Telemedicine
4. Discussion
4.1. In Relation to the Study with 2016 Data
4.2. Sensitive Variables
4.3. Factors not Included in the Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bashshur, R.; Shannon, G.; Krupinski, E. The taxonomy of telemedicine. Telemed J. E Health 2011, 17, 484–494. [Google Scholar] [CrossRef] [PubMed]
- NICE. Evidence Standards Framework for Digital Health Technologies; NICE: London, UK, 2019. [Google Scholar]
- WHO. Guideline: Recommendations on Digital Interventions for Health System Strengthening; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Kruse, C.S.; Soma, M.; Pulluri, D.; Nemali, N.T.; Brooks, M. The effectiveness of telemedicine in the management of chronic heart disease—A systematic review. JRSM Open 2017, 8, 2054270416681747. [Google Scholar] [CrossRef] [PubMed]
- Delgoshaei, B.; Mobinizadeh, M.; Mojdekar, R.; Afzal, E.; Arabloo, J.; Mohamadi, E. Telemedicine: A systematic review of economic evaluations. Med. J. Islam. Repub. Iran 2017, 31, 113. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Lee, S.W.H. Telemedicine cost-effectiveness for diabetes management: A systematic review. Diabetes Technol. Ther. 2018, 20, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Warren, R.; Carlisle, K.; Mihala, G.; Scuffham, P.A. Effects of telemonitoring on glycaemic control and healthcare costs in type 2 diabetes: A randomized controlled trial. J. Telemed. Telecare 2018, 24, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; English, J.C., 3rd. Teledermatology: A review and update. Am. J. Clin. Dermatol. 2018, 19, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Natafgi, N.; Shane, D.M.; Ullrich, F.; MacKinney, A.C.; Bell, A.; Ward, M.M. Using tele-emergency to avoid patient transfers in rural emergency departments: An assessment of costs and benefits. J. Telemed. Telecare 2018, 24, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Langabeer, J.R., 2nd; Champagne-Langabeer, T.; Alqusairi, D.; Kim, J.; Jackson, A.; Persse, D. Cost-benefit analysis of telehealth in pre-hospital care. J. Telemed. Telecare 2017, 23, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, A.S.; Hansen, L.; Sørensen, S.S.; Jensen, M.B.; Ehlers, L.H. Is telehealthcare for heart failure patients cost-effective? An economic evaluation alongside the Danish TeleCare North heart failure trial. BMJ Open 2020, 10, e031670. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Alaball, J.; Garcia Domingo, J.L.; Garcia Cuyàs, F.; Peña, J.M.; Mateo, G.F.; Rosanas, J.D.; Valmaña, G.S. A cost savings analysis of asynchronous teledermatology compared to face-to-face dermatology in Catalonia. BMC Health Serv. Res. 2018, 18, 650. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Alaball, J.; Franch-Parella, J.; Seguí, F.L.; Cuyàs, F.G.; Peña, J.M. Impact of a Telemedicine Program on the Reduction in the Emission of Atmospheric Pollutants and Journeys by Road. Int. J. Environ. Res. Public Health 2019, 16, 4366. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Alaball, J.; Álamo-Junquera, D.; López-Aguilá, S.; García-Altés, A. Evaluation of the impact of teledermatology in decreasing the waiting list in the Bages region (2009–2012). Aten. Primaria 2015, 47, 320. [Google Scholar] [CrossRef] [PubMed]
- Institut Català de la Salut. Llibre de Retribucions 2019. Available online: http://ics.gencat.cat/web/.content/documents/transparencia/personal/2019-Taules-retributives-estatutaris-gener-juny.pdf (accessed on 18 March 2020).
- Unió Catalana d’Hospitals. Xè Conveni Col·Lectiu de Treball D’establiments Sanitaris D’hospitalització, Assistència, Consulta i Laboratoris D’anàlisis Clíniques. Available online: https://www.uch.cat/negociacio-collectiva-/convenis-collectius-del-sector-sanitari-100/xe-conveni-collectiu-de-treball-destabliments-sanitaris-dhospitalitzacio-assistencia-consulta-i-laboratoris-danalisis-cliniques.html (accessed on 18 March 2020).
- Sistema d’Avaluació d’Inversions en Transport (SAIT). Available online: http://territori.gencat.cat/ca/03_infraestructures_i_mobilitat/carreteres/SAIT (accessed on 18 March 2020).



{kind=link}
{kind=link}
| Type of Telemedicine | Number of Visits | Face-to-Face Visits Saved (%) |
|---|---|---|
| Teledermatology | 40,658 | 77.7 |
| Teleophthalmology | 1180 | 72.1 |
| Teleaudiometries | 9823 | 86.2 |
| Teleulcers | 537 | 88.5 |
| Total (weighted average) | 52,198 | (79.3) |
| Direct Costs | Indirect Costs | |
|---|---|---|
| Users | Travel costs | Time spent by caregiversTravel time |
| Healthcare system | GP’s timeNurse’s time |
| Concept | Amount | Source | |
|---|---|---|---|
| Costs (€) | Wage/h primary care doctor | 24.60 | ICS [15] |
| Wage/h primary care nurse | 17.68 | ||
| Wage/h hospital doctor | 22.46 | UCH [16] | |
| Wage/h hospital nurse | 16.53 | ||
| Travel cost per km | 0.25 * | Own | |
| Average time value (patient and caregiver) | 13.36 | SAIT [17] | |
| Variables observed | Total number of visits | 52,198 | Own |
| Number of visits saved | 41,402 | ||
| Teleulcers number of visits | 537 | ||
| Teleulcers number of visits saved | 472 | ||
| Not teleulcers number of visits | 51,661 | ||
| Not teleulcers number of visits saved | 40,930 | ||
| Minutes with specialist in face-to-face visit | 15 * | ||
| Minutes with specialist in teleconsultation | 5 * | ||
| Minutes in primary care visit | 2 * | ||
| Average travel distance km | 21.58 | R + Google API | |
| Average travel time | 0.4 | R + Google API |
| Concept | Telemedicine | Usual Care | Difference | |
|---|---|---|---|---|
| Healthcare system’s costs | Primary care staff phone call | 42,675 | 42,675 | |
| Hospital staff | 137,805 | 292,347 | −154,542 | |
| Users’ costs(patient and caregiver) | Consultation time | 62,240 | 247,565 | −185,325 |
| Travel time | 962 | 318,957 | −317,995 | |
| Travel cost (private car) | 58,244 | 223,455 | −165,211 | |
| Total | 301,926 | 1082,324 | −780,397 | |
| Total per patient | 5.78 | 20.73 | −14.95 |
| Concept | Telemedicine | Usual Care | Difference | |
|---|---|---|---|---|
| Healthcare system costs | Primary care staff phone call | 51,210 | 51,210 | |
| Hospital staff | 165,366 | 350,816 | −185,451 | |
| User’s costs | Patient: consultation time | 50,221 | 247,565 | −197,344 |
| Patient: travel time | 1154 | 382,748 | −381,594 | |
| Travel cost (private car) | 69,893 | 268,146 | −198,253 | |
| Total | 337,844 | 1249,275 | −911,431 | |
| Total per patient | 6.47 | 23,93 | −17.46 |
| Type of Costs | Previous Study [12] (€) | Baseline Scenario (€) | Previous Study [12] (% of total) | Baseline Scenario(% of total) | |
|---|---|---|---|---|---|
| Healthcare system costs | Primary care staff | 0.77 | 0.82 | 22.60 | 14.33 |
| Hospital staff | −3.42 | −2.96 | |||
| User’s costs | Time | −6.31 | −9.64 | 77.40 | 85.67 |
| Travel cost | −2.76 | −3.17 | |||
| Total | −11.71 | −14.95 | 100 | 100 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López Seguí, F.; Franch Parella, J.; Gironès García, X.; Mendioroz Peña, J.; García Cuyàs, F.; Adroher Mas, C.; García-Altés, A.; Vidal-Alaball, J. A Cost-Minimization Analysis of a Medical Record-based, Store and Forward and Provider-to-provider Telemedicine Compared to Usual Care in Catalonia: More Agile and Efficient, Especially for Users. Int. J. Environ. Res. Public Health 2020, 17, 2008. https://doi.org/10.3390/ijerph17062008
López Seguí F, Franch Parella J, Gironès García X, Mendioroz Peña J, García Cuyàs F, Adroher Mas C, García-Altés A, Vidal-Alaball J. A Cost-Minimization Analysis of a Medical Record-based, Store and Forward and Provider-to-provider Telemedicine Compared to Usual Care in Catalonia: More Agile and Efficient, Especially for Users. International Journal of Environmental Research and Public Health. 2020; 17(6):2008. https://doi.org/10.3390/ijerph17062008
Chicago/Turabian StyleLópez Seguí, Francesc, Jordi Franch Parella, Xavier Gironès García, Jacobo Mendioroz Peña, Francesc García Cuyàs, Cristina Adroher Mas, Anna García-Altés, and Josep Vidal-Alaball. 2020. "A Cost-Minimization Analysis of a Medical Record-based, Store and Forward and Provider-to-provider Telemedicine Compared to Usual Care in Catalonia: More Agile and Efficient, Especially for Users" International Journal of Environmental Research and Public Health 17, no. 6: 2008. https://doi.org/10.3390/ijerph17062008
APA StyleLópez Seguí, F., Franch Parella, J., Gironès García, X., Mendioroz Peña, J., García Cuyàs, F., Adroher Mas, C., García-Altés, A., & Vidal-Alaball, J. (2020). A Cost-Minimization Analysis of a Medical Record-based, Store and Forward and Provider-to-provider Telemedicine Compared to Usual Care in Catalonia: More Agile and Efficient, Especially for Users. International Journal of Environmental Research and Public Health, 17(6), 2008. https://doi.org/10.3390/ijerph17062008