Prediction of Frailty and Dementia Using Oral Health Impact Profile from a Population-Based Survey

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
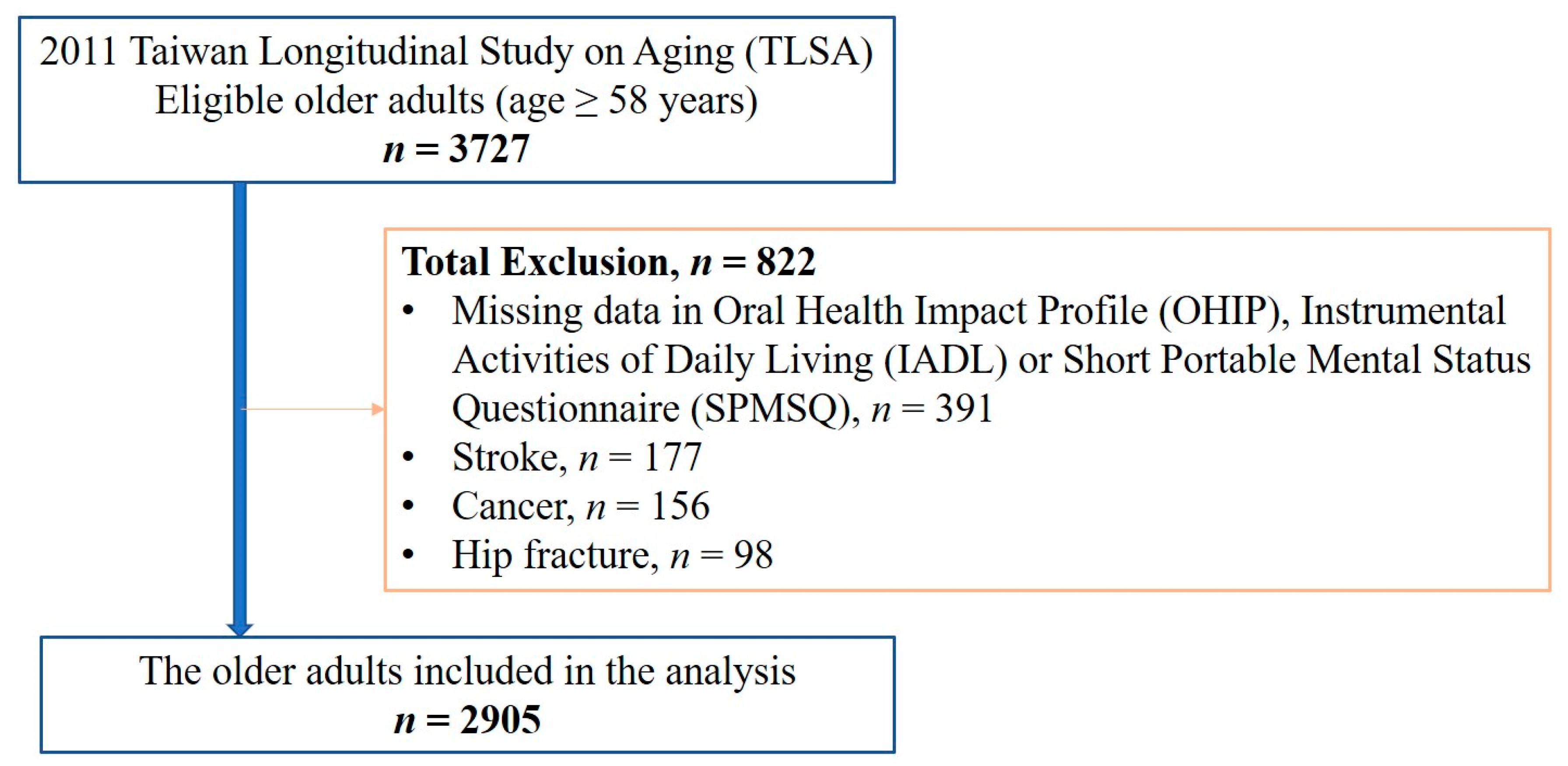
2.1. Data Source
2.2. Study Group Identification, Study Design and Ethical Approval
2.3. Research Variables
2.4. Definition of Frailty and Dementia
2.5. Statistical Analyses
3. Results
3.1. Characteristics of the Participants
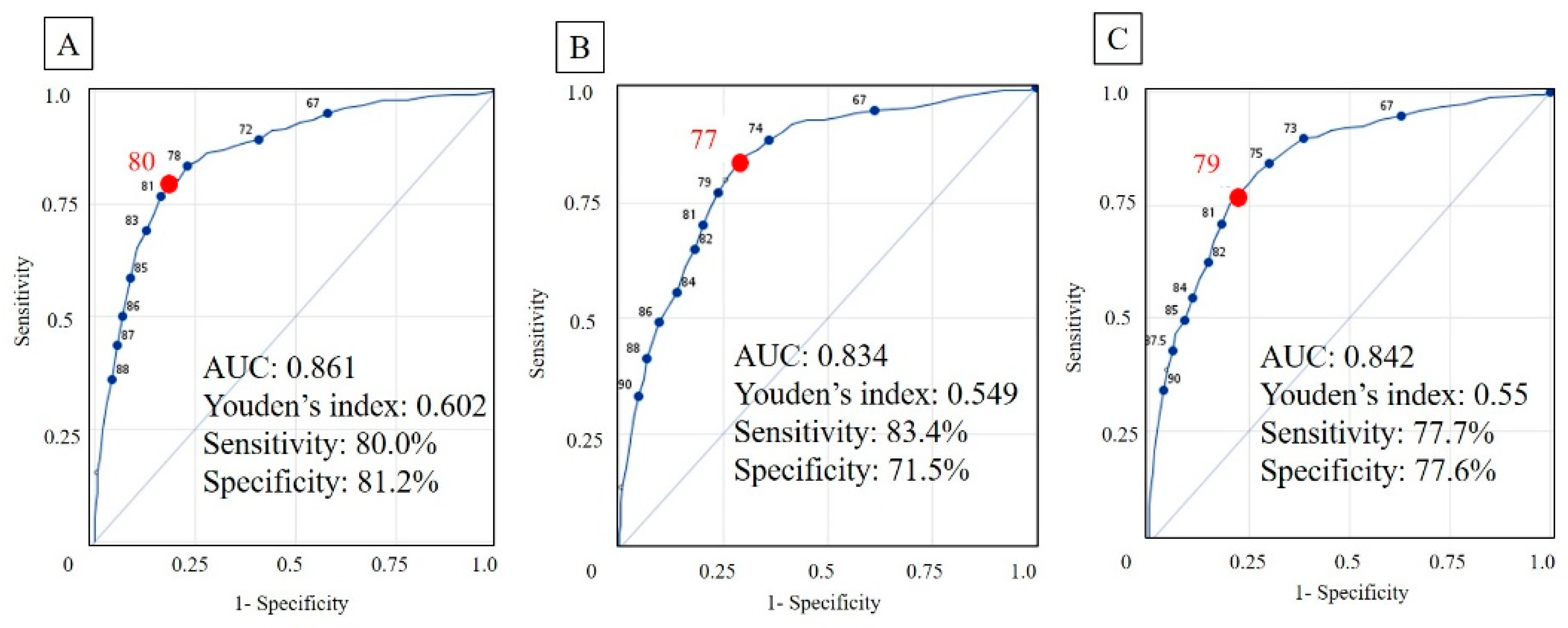
3.2. Development of Risk Models in the Prediction of Frailty and Dementia
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lamster, I.B.; Asadourian, L.; Del Carmen, T.; Friedman, P.K. The aging mouth: Differentiating normal aging from disease. Periodontol. 2000 2016, 72, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Germain, C.M.; Vasquez, E.; Batsis, J.A.; McQuoid, D.R. Sex, race and age differences in muscle strength and limitations in community dwelling older adults: Data from the Health and Retirement Survey (HRS). Arch. Gerontol. Geriatr. 2016, 65, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Theou, O.; Sluggett, J.K.; Bell, J.S.; Lalic, S.; Cooper, T.; Robson, L.; Morley, J.E.; Rockwood, K.; Visvanathan, R. Frailty, Hospitalization, and Mortality in Residential Aged Care. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 1090–1096. [Google Scholar] [CrossRef] [PubMed]
- Jayanama, K.; Theou, O.; Blodgett, J.M.; Cahill, L.; Rockwood, K. Frailty, nutrition-related parameters, and mortality across the adult age spectrum. BMC Med. 2018, 16, 188. [Google Scholar] [CrossRef]
- Merchant, R.A.; Chen, M.Z.; Tan, L.W.L.; Lim, M.Y.; Ho, H.K.; van Dam, R.M. Singapore Healthy Older People Everyday (HOPE) Study: Prevalence of Frailty and Associated Factors in Older Adults. J. Am. Med Dir. Assoc. 2017, 18, 734-e9. [Google Scholar] [CrossRef]
- Langa, K.M.; Larson, E.B.; Crimmins, E.M.; Faul, J.D.; Levine, D.A.; Kabeto, M.U.; Weir, D.R. A Comparison of the Prevalence of Dementia in the United States in 2000 and 2012. JAMA Intern. Med. 2017, 177, 51–58. [Google Scholar] [CrossRef]
- Ohara, T.; Hata, J.; Yoshida, D.; Mukai, N.; Nagata, M.; Iwaki, T.; Kitazono, T.; Kanba, S.; Kiyohara, Y.; Ninomiya, T. Trends in dementia prevalence, incidence, and survival rate in a Japanese community. Neurology 2017, 88, 1925–1932. [Google Scholar] [CrossRef]
- Hurd, M.D.; Martorell, P.; Delavande, A.; Mullen, K.J.; Langa, K.M. Monetary costs of dementia in the United States. N. Engl. J. Med. 2013, 368, 1326–1334. [Google Scholar] [CrossRef]
- Prince, M.; Ali, G.C.; Guerchet, M.; Prina, A.M.; Albanese, E.; Wu, Y.T. Recent global trends in the prevalence and incidence of dementia, and survival with dementia. Alzheimer’s Res. Ther. 2016, 8, 23. [Google Scholar] [CrossRef]
- Jia, J.; Wang, F.; Wei, C.; Zhou, A.; Jia, X.; Li, F.; Tang, M.; Chu, L.; Zhou, Y.; Zhou, C.; et al. The prevalence of dementia in urban and rural areas of China. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2014, 10, 1–9. [Google Scholar] [CrossRef]
- Dominguez, J.; Fe de Guzman, M.; Reandelar, M.; Thi Phung, T.K. Prevalence of Dementia and Associated Risk Factors: A Population-Based Study in the Philippines. J. Alzheimer’s Dis. JAD 2018, 63, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Han, J.W.; So, Y.S.; Seo, J.Y.; Kim, K.Y.; Kim, K.W. Prevalence and trends of dementia in Korea: A systematic review and meta-analysis. J. Korean Med. Sci. 2014, 29, 903–912. [Google Scholar] [CrossRef]
- Sado, M.; Ninomiya, A.; Shikimoto, R.; Ikeda, B.; Baba, T.; Yoshimura, K.; Mimura, M. The estimated cost of dementia in Japan, the most aged society in the world. PLoS ONE 2018, 13, e0206508. [Google Scholar] [CrossRef]
- Kuo, H.C.; Chen, J.H.; Wu, J.H.; Chou, T.M.; Yang, Y.H. Application of the Oral Health Impact Profile (OHIP) among Taiwanese elderly. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2011, 20, 1707–1713. [Google Scholar] [CrossRef] [PubMed]
- Slade, G.D.; Spencer, A.J. Development and evaluation of the Oral Health Impact Profile. Community Dent. Health 1994, 11, 3–11. [Google Scholar] [PubMed]
- Locker, D. Measuring oral health: A conceptual framework. Community Dent. Health 1988, 5, 3–18. [Google Scholar]
- Kushnir, D.; Zusman, S.P.; Robinson, P.G. Validation of a Hebrew version of the Oral Health Impact Profile 14. J. Public Health Dent. 2004, 64, 71–75. [Google Scholar] [CrossRef]
- Watanabe, Y.; Hirano, H.; Arai, H.; Morishita, S.; Ohara, Y.; Edahiro, A.; Murakami, M.; Shimada, H.; Kikutani, T.; Suzuki, T. Relationship Between Frailty and Oral Function in Community-Dwelling Elderly Adults. J. Am. Geriatr. Soc. 2017, 65, 66–76. [Google Scholar] [CrossRef]
- Ramsay, S.E.; Papachristou, E.; Watt, R.G.; Tsakos, G.; Lennon, L.T.; Papacosta, A.O.; Moynihan, P.; Sayer, A.A.; Whincup, P.H.; Wannamethee, S.G. Influence of Poor Oral Health on Physical Frailty: A Population-Based Cohort Study of Older British Men. J. Am. Geriatr. Soc. 2018, 66, 473–479. [Google Scholar] [CrossRef]
- Tada, A.; Miura, H. Association between mastication and cognitive status: A systematic review. Arch. Gerontol. Geriatr. 2017, 70, 44–53. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Sakuramoto, A.; Sugita, H.; Hasegawa, K.; Horii, N.; Sawada, T.; Shinmura, K.; Kishimoto, H. Relationship between oral environment and frailty among older adults dwelling in a rural Japanese community: A cross-sectional observational study. BMC Oral Health 2019, 19, 23. [Google Scholar] [CrossRef] [PubMed]
- Kamdem, B.; Seematter-Bagnoud, L.; Botrugno, F.; Santos-Eggimann, B. Relationship between oral health and Fried’s frailty criteria in community-dwelling older persons. BMC Geriatr. 2017, 17, 174. [Google Scholar] [CrossRef] [PubMed]
- Weijenberg, R.A.; Lobbezoo, F.; Visscher, C.M.; Scherder, E.J. Oral mixing ability and cognition in elderly persons with dementia: A cross-sectional study. J. Oral Rehabil. 2015, 42, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Administration, Ministry of Health and Welfare, Taiwan. Taiwan Longitudinal Study on Aging (TLSA). Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=1077&pid=6197 (accessed on 27 April 2019).
- Taiwan Provincial Institute of Family Planning; Population Studies Center and Institute of Gerontology, University of Michigan. 1989 Survey of Health and Living Status of the Elderly in Taiwan: Questionnaire and Survey Design; Population Studies Center, University of Michigan: Ann Arbor, MI, USA, 1989. [Google Scholar]
- Liang, J.; Wang, C.N.; Xu, X.; Hsu, H.C.; Lin, H.S.; Lin, Y.H. Trajectory of functional status among older Taiwanese: Gender and age variations. Soc. Sci. Med. (1982) 2010, 71, 1208–1217. [Google Scholar] [CrossRef] [PubMed]
- Mijajlović, M.D.; Pavlović, A.; Brainin, M.; Heiss, W.D.; Quinn, T.J.; Ihle-Hansen, H.B.; Hermann, D.M.; Assayag, E.B.; Richard, E.; Thiel, A.; et al. Post-stroke dementia - a comprehensive review. BMC Med. 2017, 15, 11. [Google Scholar] [CrossRef] [PubMed]
- Huisingh-Scheetz, M.; Walston, J. How should older adults with cancer be evaluated for frailty? J. Geriatr. Oncol. 2017, 8, 8–15. [Google Scholar] [CrossRef]
- Zaslavsky, O.; Li, W.; Going, S.; Datta, M.; Snetselaar, L.; Zelber-Sagi, S. Association between body composition and hip fractures in older women with physical frailty. Geriatr. Gerontol. Int. 2017, 17, 898–904. [Google Scholar] [CrossRef]
- Chang, H.T.; Hsu, N.W.; Chen, H.C.; Tsao, H.M.; Lo, S.S.; Chou, P. Associations between Body Mass Index and Subjective Health Outcomes among Older Adults: Findings from the Yilan Study, Taiwan. Int. J. Environ. Res. Public Health 2018, 15, 2645. [Google Scholar] [CrossRef]
- Wong, M.C.; Lo, E.C.; McMillan, A.S. Validation of a Chinese version of the Oral Health Impact Profile (OHIP). Community Dent. Oral Epidemiol. 2002, 30, 423–430. [Google Scholar] [CrossRef]
- Ekanayake, L.; Perera, I. Validation of a Sinhalese translation of the Oral Health Impact Profile-14 for use with older adults. Gerodontology 2003, 20, 95–99. [Google Scholar] [CrossRef]
- Kuo, H.C.; Chen, J.H.; Lai, S.K.; Shen, Y.C.; Wang, J.C.; Yang, Y.H. Development and validation of the Taiwanese short-form of the Oral Health Impact Profile (OHIP-7T). Taiwan J. Public Health 2013, 32, 393–402. [Google Scholar]
- Kuo, H.C.; Wang, R.H.; Wang, J.C.; Yang, Y.H. Assessing a conceptual model with both oral health and health related quality of life in community-dwelling elders. Arch. Gerontol. Geriatr. 2018, 79, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.J.; Wray, L.A.; Ofstedal, M.B. Diabetes-related change in physical disability from midlife to older adulthood: Evidence from 1996-2003 Survey of Health and Living Status of the Elderly in Taiwan. Diabetes Res. Clin. Pract. 2011, 91, 413–423. [Google Scholar] [CrossRef]
- Gobbens, R.J.; van Assen, M.A. The Prediction of ADL and IADL Disability Using Six Physical Indicators of Frailty: A Longitudinal Study in the Netherlands. Curr. Gerontol. Geriatr. Res. 2014, 2014, 358137. [Google Scholar] [CrossRef]
- Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- Yen, C.H.; Yeh, C.J.; Wang, C.C.; Liao, W.C.; Chen, S.C.; Chen, C.C.; Liang, J.; Lai, T.J.; Lin, H.S.; Lee, S.H.; et al. Determinants of cognitive impairment over time among the elderly in Taiwan: Results of the national longitudinal study. Arch. Gerontol. Geriatr. 2010, 50 (Suppl. 1), S53–S57. [Google Scholar] [CrossRef]
- Euser, S.M.; Schram, M.T.; Hofman, A.; Westendorp, R.G.; Breteler, M.M. Measuring cognitive function with age: The influence of selection by health and survival. Epidemiology 2008, 19, 440–447. [Google Scholar] [CrossRef]
- Lemon, S.C.; Roy, J.; Clark, M.A.; Friedmann, P.D.; Rakowski, W. Classification and regression tree analysis in public health: Methodological review and comparison with logistic regression. Ann. Behav. Med. 2003, 26, 172–181. [Google Scholar] [CrossRef]
- Ruopp, M.D.; Perkins, N.J.; Whitcomb, B.W.; Schisterman, E.F. Youden Index and optimal cut-point estimated from observations affected by a lower limit of detection. Biom. J. Biom. Z. 2008, 50, 419–430. [Google Scholar] [CrossRef]
- Gil-Montoya, J.A.; Ponce, G.; Sanchez Lara, I.; Barrios, R.; Llodra, J.C.; Bravo, M. Association of the oral health impact profile with malnutrition risk in Spanish elders. Arch. Gerontol. Geriatr. 2013, 57, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Bakker, M.H.; Vissink, A.; Spoorenberg, S.L.W.; Jager-Wittenaar, H.; Wynia, K.; Visser, A. Are Edentulousness, Oral Health Problems and Poor Health-Related Quality of Life Associated with Malnutrition in Community-Dwelling Elderly (Aged 75 Years and Over)? A Cross-Sectional Study. Nutrients 2018, 10, 1965. [Google Scholar] [CrossRef] [PubMed]
- Castrejon-Perez, R.C.; Borges-Yanez, S.A.; Gutierrez-Robledo, L.M.; Avila-Funes, J.A. Oral health conditions and frailty in Mexican community-dwelling elderly: A cross sectional analysis. BMC Public Health 2012, 12, 773. [Google Scholar] [CrossRef] [PubMed]
- Semba, R.D.; Blaum, C.S.; Bartali, B.; Xue, Q.L.; Ricks, M.O.; Guralnik, J.M.; Fried, L.P. Denture use, malnutrition, frailty, and mortality among older women living in the community. J. Nutr. Health Aging 2006, 10, 161–167. [Google Scholar] [PubMed]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tetsuo, T.; Akishita, M.; Iijima, K. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 1661–1667. [Google Scholar] [CrossRef]
- Hakeem, F.F.; Bernabe, E.; Sabbah, W. Association between oral health and frailty: A systematic review of longitudinal studies. Gerodontology 2019. [Google Scholar] [CrossRef]
- Stein, P.S.; Desrosiers, M.; Donegan, S.J.; Yepes, J.F.; Kryscio, R.J. Tooth loss, dementia and neuropathology in the Nun study. J. Am. Dent. Assoc. 2007, 138, 1314–1322. [Google Scholar] [CrossRef]
- Lin, C.S. Revisiting the link between cognitive decline and masticatory dysfunction. BMC Geriatr. 2018, 18, 5. [Google Scholar] [CrossRef]
- Cerutti-Kopplin, D.; Feine, J.; Padilha, D.M.; de Souza, R.F.; Ahmadi, M.; Rompre, P.; Booij, L.; Emami, E. Tooth Loss Increases the Risk of Diminished Cognitive Function: A Systematic Review and Meta-analysis. JDR Clin. Transl. Res. 2016, 1, 10–19. [Google Scholar] [CrossRef]
- Aliani, M.; Udenigwe, C.C.; Girgih, A.T.; Pownall, T.L.; Bugera, J.L.; Eskin, M.N. Aroma and taste perceptions with Alzheimer disease and stroke. Crit. Rev. Food Sci. Nutr. 2013, 53, 760–769. [Google Scholar] [CrossRef]
- Wu, B.; Fillenbaum, G.G.; Plassman, B.L.; Guo, L. Association Between Oral Health and Cognitive Status: A Systematic Review. J. Am. Geriatr. Soc. 2016, 64, 739–751. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age (Mean ± SD) | 69.46 ± 9.26 |
|---|---|
| Sex, n (%) | |
| Male | 1426 (49.1) |
| Female | 1479 (50.1) |
| Height (cm) (mean ± SD) (n = 2337) | 160.28 ± 7.81 |
| Weight (kg) (mean ± SD) (n = 2617) | 62.66 ± 10.64 |
| BMI (kg/m2) (mean ± SD) (n = 2289) | 24.34 ± 3.43 |
| Underweight (BMI < 18.5 kg/m2), n (%) | 72 (2.5) |
| Normal weight (18.5 ≤ BMI < 24 kg/m2), n (%) | 1027 (35.4) |
| Overweight (24 ≤ BMI < 27 kg/m2), n (%) | 737 (25.4) |
| Obese (BMI ≥ 27 kg/m2), n (%) | 453 (15.6) |
| No self-reported height or weight, n (%) | 616 (21.2) |
| Alcohol | 909 (31.3) |
| Smoking | 410 (14.1) |
| Marital status, n (%) | |
| Married and Cohabitant | 1977 (68.1) |
| Single and Divorced and Widowed | 928 (31.9) |
| Education, n (%) | |
| Uneducated | 578 (19.9) |
| Elementary school | 1299 (44.7) |
| Junior high school | 352 (12.1) |
| Senior high school | 365 (12.6) |
| College or above | 311 (10.7) |
| Comorbidities, n (%) | |
| Hypertension | 1249 (43.0) |
| Diabetes mellitus | 490 (16.9) |
| Cardiovascular disease | 476 (16.4) |
| Hyperlipidemia | 360 (12.4) |
| Chronic obstructive pulmonary disease | 105 (3.6) |
| Arthritis | 415 (14.3) |
| Chronic liver disease | 261 (9.0) |
| Chronic kidney disease | 246 (8.5) |
| Dental prosthesis, n (%) | 2261 (77.8) |
| Fixed dental prosthesis, n (%) | 1324 (45.6) |
| Removable dental prosthesis, n (%) | 1112 (38.3) |
| 0-Never | 1-Hardly Never | 2-Occasionally | 3-Fairly Often | 4-Very Often | Mean ± SD | |
|---|---|---|---|---|---|---|
| OHIP-7T Q1: self-conscious? (Q20) | 1423 (49.0%) | 387 (13.3%) | 524 (18.0%) | 396 (13.6%) | 175 (6.0%) | 1.14 ± 1.32 |
| OHIP-7T Q2: interrupt meal? (Q32) | 2034 (70.0%) | 339 (11.7%) | 272 (9.4%) | 195 (6.7%) | 65 (2.2%) | 0.59 ± 1.05 |
| OHIP-7T Q3: uncomfortable to eat? (Q16) | 1668 (57.4%) | 331 (11.4%) | 473 (16.3%) | 324 (11.2%) | 109 (3.8%) | 0.92 ± 1.23 |
| OHIP-7T Q4: concentration affected? (Q37) | 2456 (84.5%) | 207 (7.1%) | 160 (5.5%) | 60 (2.1%) | 22 (0.8%) | 0.27 ± 0.72 |
| OHIP-7T Q5: trouble pronouncing words? (Q2) | 2483 (85.5%) | 181 (6.2%) | 139 (4.8%) | 78 (2.7%) | 24 (0.8%) | 0.27 ± 0.74 |
| OHIP-7T Q6: difficult doing jobs? (Q43) | 2645 (91.0%) | 134 (4.6%) | 72 (2.5%) | 37 (1.3%) | 17 (0.6%) | 0.16 ± 0.57 |
| OHIP-7T Q7: taste worse? (Q6) | 2288 (78.8%) | 239 (8.2%) | 174 (6.0%) | 155 (5.3%) | 49 (1.7%) | 0.43 ± 0.94 |
| Model 1: Prediction of Frailty | ||||
| Risk Score Items | Odds Ratio | 95% CI | p Value | Risk Score Weights 1 |
| Age | 1.17 | 1.15–1.20 | <0.001 | 1 |
| Female | 1.67 | 1.22–2.29 | 0.001 | 1 |
| OHIP-7T Q3 score 2 | 1.33 | 1.19–1.49 | <0.001 | 1 |
| No dental prosthesis | 1.61 | 1.11–2.35 | 0.01 | 1 |
| Diabetes mellitus | 2.39 | 1.68–3.40 | <0.001 | 2 |
| Chronic kidney disease | 2.59 | 1.61–4.17 | <0.001 | 2 |
| Model 2: Prediction of Dementia | ||||
| Risk Score Items | Odds Ratio | 95% CI | p Value | Risk Score Weights 1 |
| Age | 1.12 | 1.10–1.13 | <0.001 | 1 |
| Female | 2.84 | 2.17–3.72 | <0.001 | 3 |
| OHIP-7T Q3 score 2 | 1.17 | 1.01–1.37 | 0.04 | 1 |
| OHIP-7T Q7 score 3 | 1.21 | 1.06–1.37 | 0.005 | 1 |
| No dental prosthesis | 1.45 | 1.07–1.97 | 0.02 | 1 |
| Inability to self-report height or weight | 4.52 | 3.52–5.81 | <0.001 | 4 |
| Model 3: Prediction of Frailty or Dementia | ||||
| Risk Score Items | Odds Ratio | 95% CI | p Value | Risk Score Weights 1 |
| Age | 1.14 | 1.12–1.15 | <0.001 | 1 |
| Female | 2.50 | 1.95–3.19 | <0.001 | 2 |
| OHIP-7T Q3 score 2 | 1.12 | 1.02–1.24 | 0.02 | 1 |
| OHIP-7T Q7 score 3 | 1.22 | 1.08–1.38 | 0.001 | 1 |
| No dental prosthesis | 1.51 | 1.13–2.01 | 0.005 | 1 |
| Inability to self-report height or weight | 3.68 | 2.89–4.69 | <0.001 | 3 |
| Diabetes mellitus | 1.42 | 1.07–1.89 | 0.02 | 1 |
| Chronic kidney disease | 1.56 | 1.04–2.33 | 0.03 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tai, C.-J.; Chen, J.-H.; Tseng, T.-G.; Lin, Y.-T.; Hsiao, Y.-H.; Lee, M.-C.; Yang, Y.-H. Prediction of Frailty and Dementia Using Oral Health Impact Profile from a Population-Based Survey. Int. J. Environ. Res. Public Health 2020, 17, 1997. https://doi.org/10.3390/ijerph17061997
Tai C-J, Chen J-H, Tseng T-G, Lin Y-T, Hsiao Y-H, Lee M-C, Yang Y-H. Prediction of Frailty and Dementia Using Oral Health Impact Profile from a Population-Based Survey. International Journal of Environmental Research and Public Health. 2020; 17(6):1997. https://doi.org/10.3390/ijerph17061997
Chicago/Turabian StyleTai, Chi-Jung, Jen-Hao Chen, Tzyy-Guey Tseng, Yi-Ting Lin, Yu-Han Hsiao, Meng-Chih Lee, and Yi-Hsin Yang. 2020. "Prediction of Frailty and Dementia Using Oral Health Impact Profile from a Population-Based Survey" International Journal of Environmental Research and Public Health 17, no. 6: 1997. https://doi.org/10.3390/ijerph17061997
APA StyleTai, C.-J., Chen, J.-H., Tseng, T.-G., Lin, Y.-T., Hsiao, Y.-H., Lee, M.-C., & Yang, Y.-H. (2020). Prediction of Frailty and Dementia Using Oral Health Impact Profile from a Population-Based Survey. International Journal of Environmental Research and Public Health, 17(6), 1997. https://doi.org/10.3390/ijerph17061997