Affordability and Availability of Child Restraints in an Under-Served Population in South Africa

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Observational Study
2.3. Survey
3. Results
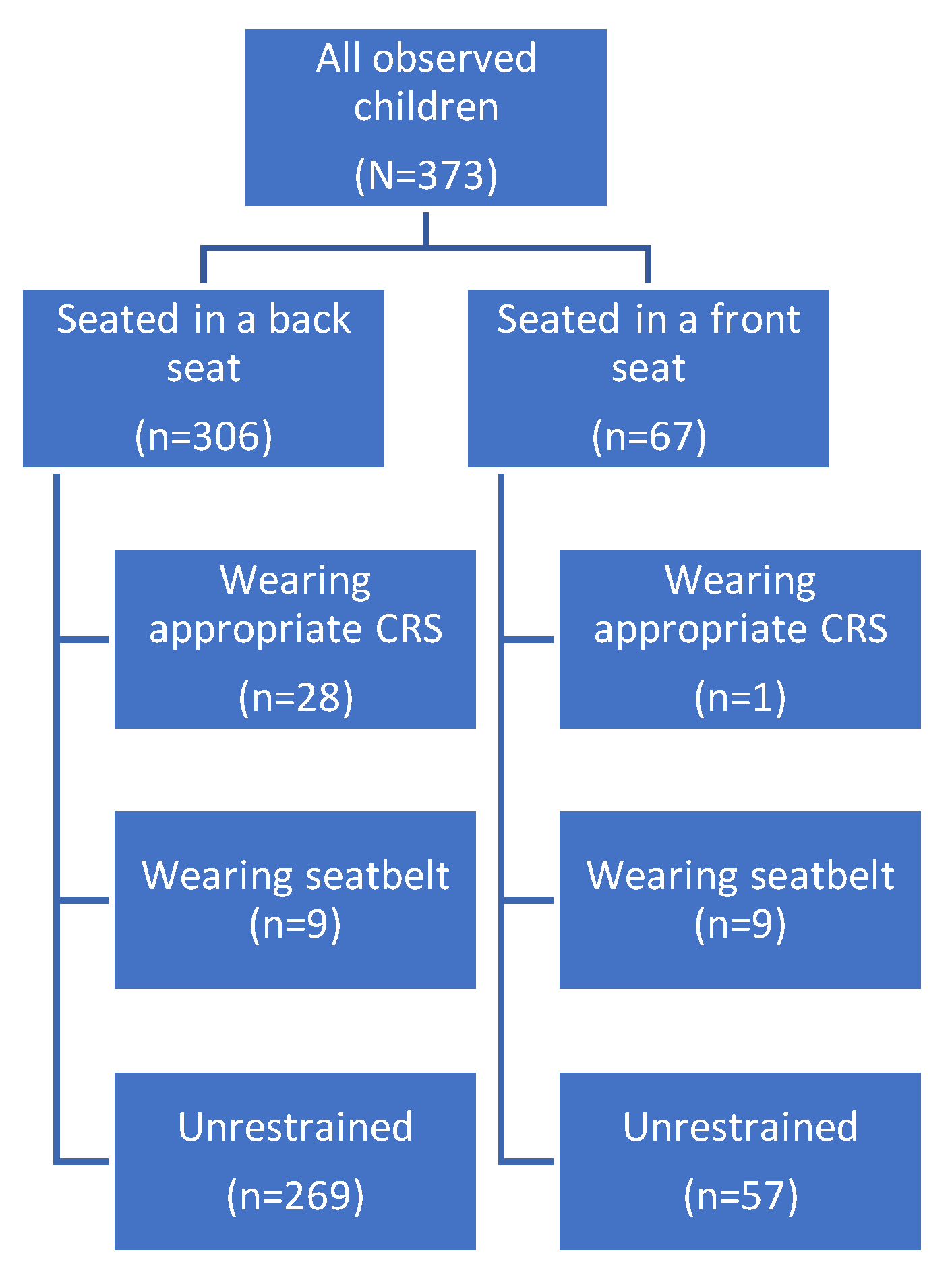
3.1. Observational Survey Results
3.2. Survey Results
3.2.1. Demographics
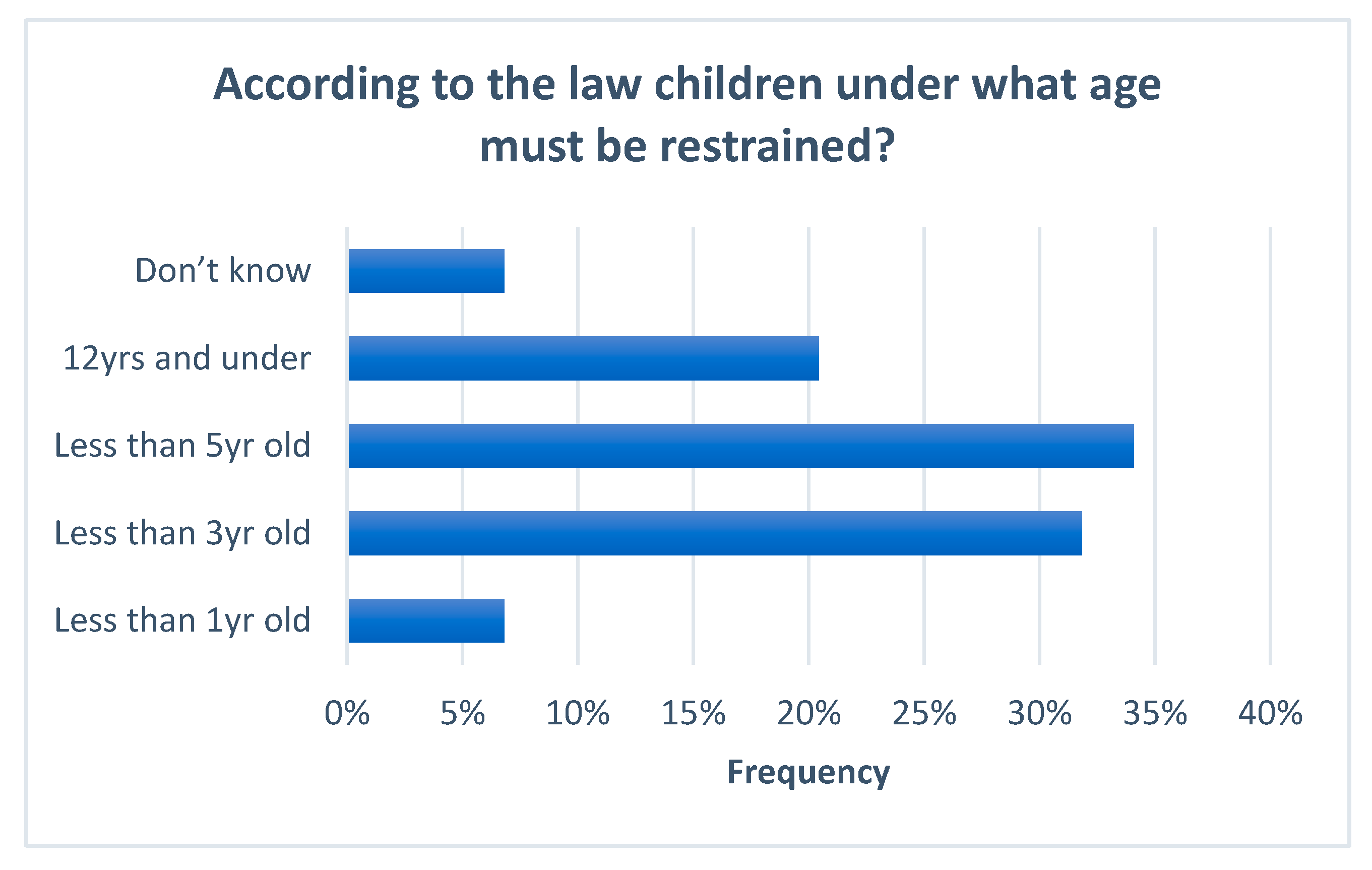
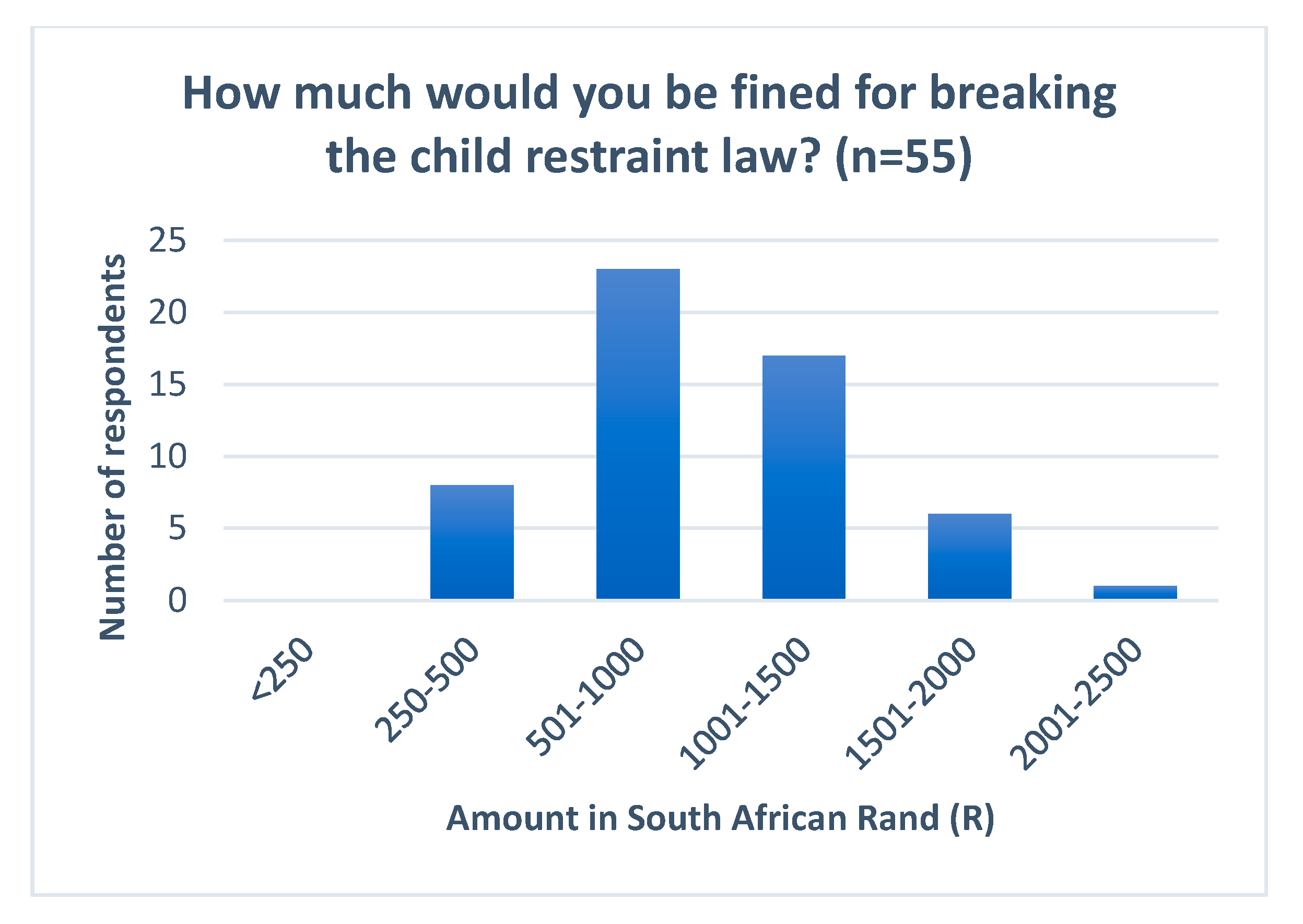
3.2.2. Knowledge of the Current Law
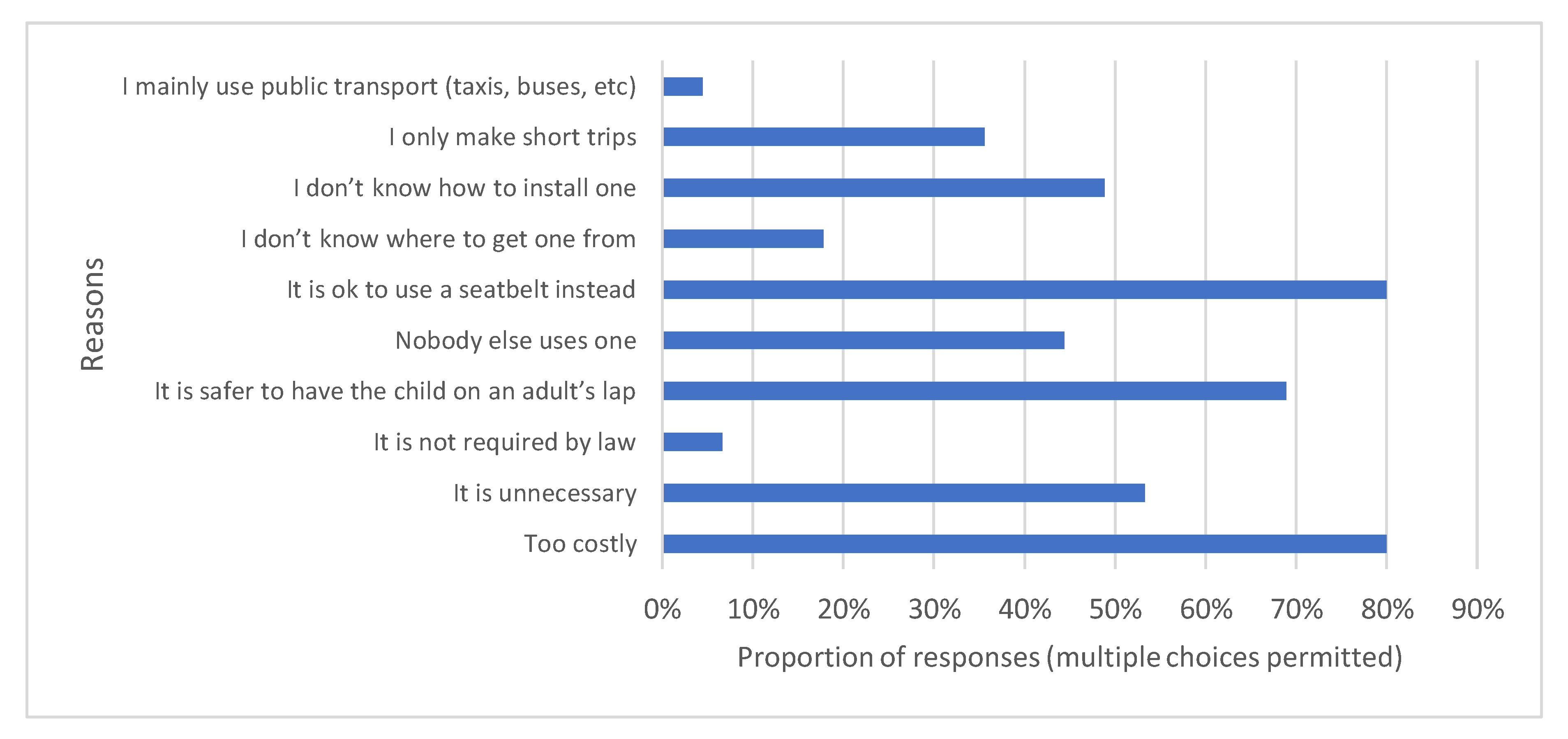
3.2.3. Importance of Child Restraints
3.2.4. Child Restraint Ownership
3.2.5. Information on and Cost of Child Restraints
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Peden, M.; Oyegbite, K.; Ozanne-Smith, J.; Hyder, A.A.; Branche, C.; Rahman, A.; Rivara, F.; Bartolomeos, K. World Report on Child Injury Prevention; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Alonge, O.; Hyder, A.A. Reducing the Global Burden of Childhood Unintentional Injuries. Arch. Dis. Child. 2014, 99, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Wyk, V.P.-V.; Msemburi, W.; Laubscher, R.; Dorrington, R.E.; Groenewald, P.; Glass, T.; Nojilana, B.; Joubert, J.D.; Matzopoulos, R.; Prinsloo, M.; et al. Mortality trends and differentials in South Africa from 1997 to 2012: Second National Burden of Disease Study. Lancet Glob. Health 2016, 4, e642–e653. [Google Scholar]
- Matzopoulos, R.; Prinsloo, M.; Wyk, V.P.-V.; Gwebushe, N.; Mathews, S.; Martin, L.; Laubscher, R.; Abrahams, N.; Msemburi, W.; Lombard, C.; et al. Injury-related mortality in South Africa: A retrospective descriptive study of postmortem investigations. Bull. World Health Organ. 2015, 93, 303–313. [Google Scholar] [CrossRef] [PubMed]
- Prinsloo, M. Estimating Injury Mortality in South Africa and Identifying Urban-Rural Differences, in Public Health and Family Medicine. Ph.D. Thesis, University of Cape Town, Cape Town, South Africa, 2019; p. 191. [Google Scholar]
- Elliott, M.R.; Kallan, M.J.; Durbin, D.R.; Winston, F.K. Effectiveness of Child Safety Seats vs Seat Belts in Reducing Risk for Death in Children in Passenger Vehicle Crashes. Arch. Pediatr. Adolesc. Med. 2006, 160, 617–621. [Google Scholar] [CrossRef] [PubMed]
- Zaloshnja, E.; Miller, T.R.; Hendrie, D. Effectiveness of Child Safety Seats vs Safety Belts for Children Aged 2 to 3 Years. Arch. Pediatr. Adolesc. Med. 2007, 161, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Arbogast, K.; Jermakian, J.S.; Kallan, M.J.; Durbin, D.R. Effectiveness of Belt Positioning Booster Seats: An Updated Assessment. Pediatrics 2009, 124, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Keay, L.; Brown, J.; Hunter, K.; Ivers, R. Adopting child restraint laws to address child passenger injuries: Experience from high income countries and new initiatives in low and middle income countries. Injury 2015, 46, 933–934. [Google Scholar] [CrossRef]
- Zaza, S.; Sleet, D.A.; Thompson, R.S.; Sosin, D.M.; Bolen, J.C. Reviews of evidence regarding interventions to increase use of child safety seats. Am. J. Prev. Med. 2001, 21, 31–47. [Google Scholar] [CrossRef]
- Elvik, R.; Vaa, T.; Hoye, A.; Sorensen, M. The Handbook of Road Safety Measures; Elsevier: Amsterdam, The Netherlands, 2004. [Google Scholar]
- Pérez-Núñez, R.; Chandran, A.; Híjar, M.; Celis, A.; Carmona-Lozano, M.S.; Lunnen, J.C.; Hyder, A.A. The use of seatbelts and child restraints in three Mexican cities. Int. J. Inj. Control. Saf. Promot. 2013, 20, 385–393. [Google Scholar] [CrossRef]
- Ojo, T.K. Seat belt and child restraint use in a developing country metropolitan city. Accid. Anal. Prev. 2018, 113, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.; Ho, C.; Keay, L.; McCaffery, K.; Hunter, K.; Charlton, J.L.; Hayen, A.; Bilston, L.E.; Brown, J. Barriers to correct child restraint use: A qualitative study of child restraint users and their needs. Saf. Sci. 2018, 109, 186–194. [Google Scholar] [CrossRef]
- Van Hoving, D.J.; Sinclair, M.; Wallis, L. Patterns of seatbelt use in different socioeconomic communities in the Cape Town Metropole, South Africa. S. Afr. Med. J. 2013, 103, 628. [Google Scholar] [CrossRef] [PubMed]
- Child Accident Prevention Foundation of South Africa. BUCKLE UP 2013; Child Accident Prevention Foundation of South Africa: Cape Town, South Africa, 2013. [Google Scholar]
- Kling, J.; Nicholls, T.; Ntambeka, P.; Van As, A. Restraint use for child passengers in South Africa. South Afr. Med. J. 2011, 101, 146. [Google Scholar] [CrossRef][Green Version]
- WHO. Global Status Report on Road Safety 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Janmohammed, A.; Attwood, P.; Mtambeka, P.; Prinsloo, M.; Peden, M. The need for stronger child restraint laws. S. Afr. Med. J. 2019, 109, 12672. [Google Scholar] [CrossRef]
- Chen, X.; Yang, J.; Peek-Asa, C.; Li, L. Parents’ experience with child safety restraint in China. BMC Public Health 2014, 14, 318. [Google Scholar] [CrossRef]
- Keay, L.; Hunter, K.; Brown, J.; Simpson, J.M.; Bilston, L.E.; Elliott, M.; Stevenson, M.; Ivers, R. Evaluation of an Education, Restraint Distribution, and Fitting Program to Promote Correct Use of Age-Appropriate Child Restraints for Children Aged 3 to 5 Years: A Cluster Randomized Trial. Am. J. Public Health 2012, 102, e96–e102. [Google Scholar] [CrossRef]
- Otieno, G.; Marinda, E.; Bärnighausen, T.; Tanser, F. High rates of homicide in a rural South African population (2000–2008): Findings from a population-based cohort study. Popul. Health Metrics 2015, 13, 20. [Google Scholar] [CrossRef]
- Seedat, M.; Van Niekerk, A.; Jewkes, R.; Suffla, S.; Ratele, K. Violence and injuries in South Africa: Prioritising an agenda for prevention. Lancet 2009, 374, 1011–1022. [Google Scholar] [CrossRef]
- Clay, C.; Van As, A.B.; Hunter, K.; Peden, M. Latest results show urgent need to address child restraint use. S. Afr. Med. J. 2019, 109, 12544. [Google Scholar] [CrossRef]
- Peden, M.; Scurfield, R.; Sleet, D.; Mohan, D.; Hyder, A.A.; Jarawan, E.; Mathers, C. World Report on Road Traffic Injury Prevention; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Chen, X.; Yang, J.; Peek-Asa, C.; McGehee, D.V.; Li, L. Parents’ Knowledge, Attitude, and Use of Child Restraints, Shantou, China. Am. J. Prev. Med. 2014, 46, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Mc Ilvenny, S.; Al Mahrouqi, F.; Al Busaidi, T.; Al Nabhani, A.; Al Hikmani, F.; Al Kharousi, Z.; Al Mammari, S.; Al Hoti, A.; Al Shihi, A.; Al Lawati, A.; et al. Rear seat belt use as an indicator of safe road behaviour in a rapidly developing country. J. R. Soc. Promot. Health 2004, 124, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Lei, H.; Yang, J.; Liu, X.; Chen, X.; Li, L. Has Child Restraint System Use Increased among Parents of Children in Shantou, China? Int. J. Environ. Res. Public Health 2016, 13, 964. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.R.; Korošec, A.; Bilban, M. The influence of parental education and other socio-economic factors on child car seat use. Slov. J. Public Health 2017, 56, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Braver, E.R.; Whitfield, R.; Ferguson, S.A. Seating positions and children’s risk of dying in motor vehicle crashes. Inj. Prev. 1998, 4, 181–187. [Google Scholar] [CrossRef]
- Arbogast, K.; Kallan, M.J.; Durbin, D.R. Front versus Rear Seat Injury Risk for Child Passengers: Evaluation of Newer Model Year Vehicles. Traffic Inj. Prev. 2009, 10, 297–301. [Google Scholar] [CrossRef]
- Rus, D.; Jurchis, F.; Baragan, E.; Chereches, R.; Peek-Asa, C.; Mocean, F. Child safety restraint usage in Romania—An observational study designDiana Rus. Eur. J. Public Health 2015, 25 (Suppl. 3), 209. [Google Scholar] [CrossRef]
- Sam, E.F. Don’t learn safety by accident: A survey of child safety restraint usage among drivers in Dansoman, Accra. J. Transp. Health 2015, 2, 160–165. [Google Scholar] [CrossRef]
- Urie, Y.; Velaga, N.R.; Maji, A. Cross-Sectional Study of Road Accidents and Related Law Enforcement Efficiency for Ten Countries: A Gap Coherence Analysis. Traffic Inj. Prev. 2016, 17, 686–691. [Google Scholar] [CrossRef]
- Eby, D.W.; Kostyniuk, L.P. A statewide analysis of child safety seat use and misuse in Michigan. Accid. Anal. Prev. 1999, 31, 555–566. [Google Scholar] [CrossRef]
- De Oliveira, S.R.L.; Carvalho, M.D.D.B.; Santana, R.G.; Camargo, G.C.S.; Lüders, L.; Franzin, S. Child safety restraint use among children attending day care centers. Revista de Saúde Pública 2009, 43, 761–767. [Google Scholar]
- Sangowawa, A.; Ekanem, S.; Alagh, B.; Ebong, I.; Faseru, B.; Uchendu, O.; Adekunle, B.; Shaahu, V.; Fajola, A. Child seating position and restraint use in the Ibadan Metropolis, South Western Nigeria: Original contribution. Afr. Saf. Promot. 2006, 4, 37–49. [Google Scholar]
- Şevketoğlu, E.; Hatipoğlu, S.; Esin, G.; Oztora, S. Knowledge and attitude of Turkish parents regarding car safety seats for children. Ulusal Travma ve Acil Cerrahi Dergisi = Turk. J. Trauma Emerg. Surg. TJTES 2009, 15, 482–486. [Google Scholar]
- Raman, S.R.; Landry, M.D.; Ottensmeyer, C.A.; Jacob, S.; Hamdan, E.; Bouhaimed, M. Keeping our children safe in motor vehicles: Knowledge, attitudes and practice among parents in Kuwait regarding child car safety. Int. J. Inj. Control. Saf. Promot. 2013, 20, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Zonfrillo, M.R.; Ferguson, R.W.; Walker, L. Reasons for Child Passenger Nonrestraint in Motor Vehicles. Traffic Inj. Prev. 2015, 16 (Suppl. 2), S41–S45. [Google Scholar] [CrossRef]
- Tavakoli, Z.; Davoodi, S.R.; Azimmohseni, M. Factors affecting use and nonuse of child safety car seats in Gorgan, Iran. Traffic Inj. Prev. 2019, 20, 661–666. [Google Scholar] [CrossRef]
- ChildSafe. ChildSafe: Keep Kids Safe from Harm. Available online: https://www.childsafe.org.za/index.html (accessed on 1 January 2020).
- Gupta, S.; Paichadze, N.; Gritsenko, E.; Klyavin, V.; Yurasova, E.; Hyder, A.A. Evaluation of the five-year Bloomberg Philanthropies Global Road Safety Program in the Russian Federation. Public Health 2017, 144, S5–S14. [Google Scholar] [CrossRef]
- Jarahi, L.; Karbakhsh, M.; Rashidian, A. Parental willingness to pay for child safety seats in Mashad, Iran. BMC Public Health 2011, 11, 281. [Google Scholar] [CrossRef] [PubMed]
- Wheel Well. Wheel Well: For Children in Road Safety. 2008. Available online: https://www.wheelwell.org.za (accessed on 1 January 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site. | Suburb | Survey Responses | Observational Study | ||
|---|---|---|---|---|---|
| Yes | No | Total | |||
| Daycares: | |||||
| Site 1 | Seapoint | 22 | 25 | 47 | 56 |
| Site 2 | Gugulethu | 4 | 3 | 7 | 20 |
| Site 3 | Athlone | 2 | 8 | 10 | 21 |
| Hospitals: | |||||
| Site 4 | Khayelitsha | 17 | 9 | 26 | 33 |
| Site 5 | Mitchells Plain | 23 | 15 | 38 | 83 |
| Site 6 | Athlone | 17 | 4 | 21 | 44 |
| Site 7 | Wynberg | 13 | 6 | 19 | 22 |
| TOTAL | 98 (58.3%) | 70(41.7%) | 168 | 279 | |
| Age | Total | |||
|---|---|---|---|---|
| <1 Year | 1–3 Years | >3 Years | ||
| Front Seat | ||||
| Unrestrained | 3 | 30 | 24 | 57 (85.1%) |
| Restrained in CRS | 0 | 1 | 0 | 1 (1.5%) |
| Restrained by seatbelt | 0 | 2 | 7 | 9 (13.4%) |
| Total | 3 | 33 | 31 | 67 (100%) |
| Back Seat | ||||
| Unrestrained | 49 | 99 | 121 | 269 (87.9%) |
| Restrained in CRS | 7 | 21 | 0 | 28 (9.2%) |
| Restrained by seatbelt | 0 | 1 | 8 | 9 (2.9%) |
| Total | 56 | 121 | 129 | 306 (100%) |
| Child in Restraint? | Total | ||
|---|---|---|---|
| Driver Wearing Seatbelt? | n | Y | |
| n | 250 (73%) | 7 | 257 |
| Y | 94 (27%) | 22 | 116 |
| Total | 344 | 29 | 373 |
| Characteristic | n | % | |
|---|---|---|---|
| Relationship to the children) in car (n = 98) | Mother | 38 | 39% |
| Father | 49 | 50% | |
| Other Relative | 6 | 6% | |
| Friend of child’s parents | 3 | 3% | |
| Taxi driver/Hired Driver | 2 | 2% | |
| Other | 0 | 0% | |
| Sex of respondent (n = 78) | Male | 47 | 60% |
| Female | 31 | 40% | |
| Age of respondent (n = 94) | <30 years old | 14 | 15% |
| 30–39 years old | 42 | 45% | |
| 40–49 years old | 30 | 32% | |
| 50–59 years old | 6 | 6% | |
| ≥60 years old | 2 | 2% | |
| Age of child(ren) in car (n = 133) | 0–2 years | 36 | 27% |
| 3–8 years | 83 | 62% | |
| 9–14 years | 12 | 9% | |
| Highest level of education of respondent (n = 90) | No schooling | 1 | 1% |
| Primary school | 0 | 0% | |
| Secondary or high school | 48 | 53% | |
| Post school education (such as college or university) | 41 | 46% | |
| Number of years that respondent has been driving (n = 94) | <10 years | 33 | 35% |
| 10–14 years | 37 | 39% | |
| 15–19 years | 12 | 13% | |
| ≥ 20 years | 12 | 13% | |
| Does respondent own the car? (n = 88) | Yes | 85 | 97% |
| No | 3 | 3% | |
| Total Monthly Family Income in South African Rand * (n = 97) | < R1 600 | 0 | 0% |
| R1 600–R3 200 | 1 | 1% | |
| R3 201–R6 400 | 4 | 4% | |
| R6 401–R12 800 | 10 | 10% | |
| R12 801–R25 600 | 16 | 16% | |
| R25 601–R50,000 | 5 | 5% | |
| > R50,000 | 3 | 3% | |
| I don’t know | 20 | 21% | |
| Do not wish to answer | 38 | 39% |
| n | % | |
|---|---|---|
| Where was car seat purchased? | ||
| Hand me down from relative or previous child | 11 | 23% |
| Garage sale | 1 | 2% |
| Bought online | 8 | 17% |
| New from store | 26 | 54% |
| Car seat exchange program | 0 | 0% |
| Gift, Brand new | 2 | 4% |
| How much did the car seat cost? | ||
| It was free (e.g., a gift or handed down) | 11 | 22% |
| R1–R999.99 | 7 | 14% |
| R1000.00–R2999.99 | 27 | 53% |
| R3000.00–R4999.99 | 3 | 6% |
| R5000.00–R6999.99 | 1 | 2% |
| R7000.00 and above | 0 | 0% |
| I Don’t know | 2 | 4% |
| What factors were important when purchasing the car seat? | ||
| Colour | 23 | 14% |
| Price | 19 | 12% |
| Style/look | 24 | 15% |
| Quality | 35 | 22% |
| Brand/company name | 8 | 5% |
| Easy to install | 23 | 14% |
| Age appropriate seat | 21 | 13% |
| Recommended to me by somebody | 8 | 5% |
| Other (please specify) | 1 | 1% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Puvanachandra, P.; Janmohammed, A.; Mtambeka, P.; Prinsloo, M.; Van As, S.; Peden, M.M. Affordability and Availability of Child Restraints in an Under-Served Population in South Africa. Int. J. Environ. Res. Public Health 2020, 17, 1979. https://doi.org/10.3390/ijerph17061979
Puvanachandra P, Janmohammed A, Mtambeka P, Prinsloo M, Van As S, Peden MM. Affordability and Availability of Child Restraints in an Under-Served Population in South Africa. International Journal of Environmental Research and Public Health. 2020; 17(6):1979. https://doi.org/10.3390/ijerph17061979
Chicago/Turabian StylePuvanachandra, Prasanthi, Aliasgher Janmohammed, Pumla Mtambeka, Megan Prinsloo, Sebastian Van As, and Margaret M. Peden. 2020. "Affordability and Availability of Child Restraints in an Under-Served Population in South Africa" International Journal of Environmental Research and Public Health 17, no. 6: 1979. https://doi.org/10.3390/ijerph17061979
APA StylePuvanachandra, P., Janmohammed, A., Mtambeka, P., Prinsloo, M., Van As, S., & Peden, M. M. (2020). Affordability and Availability of Child Restraints in an Under-Served Population in South Africa. International Journal of Environmental Research and Public Health, 17(6), 1979. https://doi.org/10.3390/ijerph17061979