Impact of 12-Month Smartphone Breathing Meditation Program upon Systolic Blood Pressure among Non-Medicated Stage 1 Hypertensive Adults

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
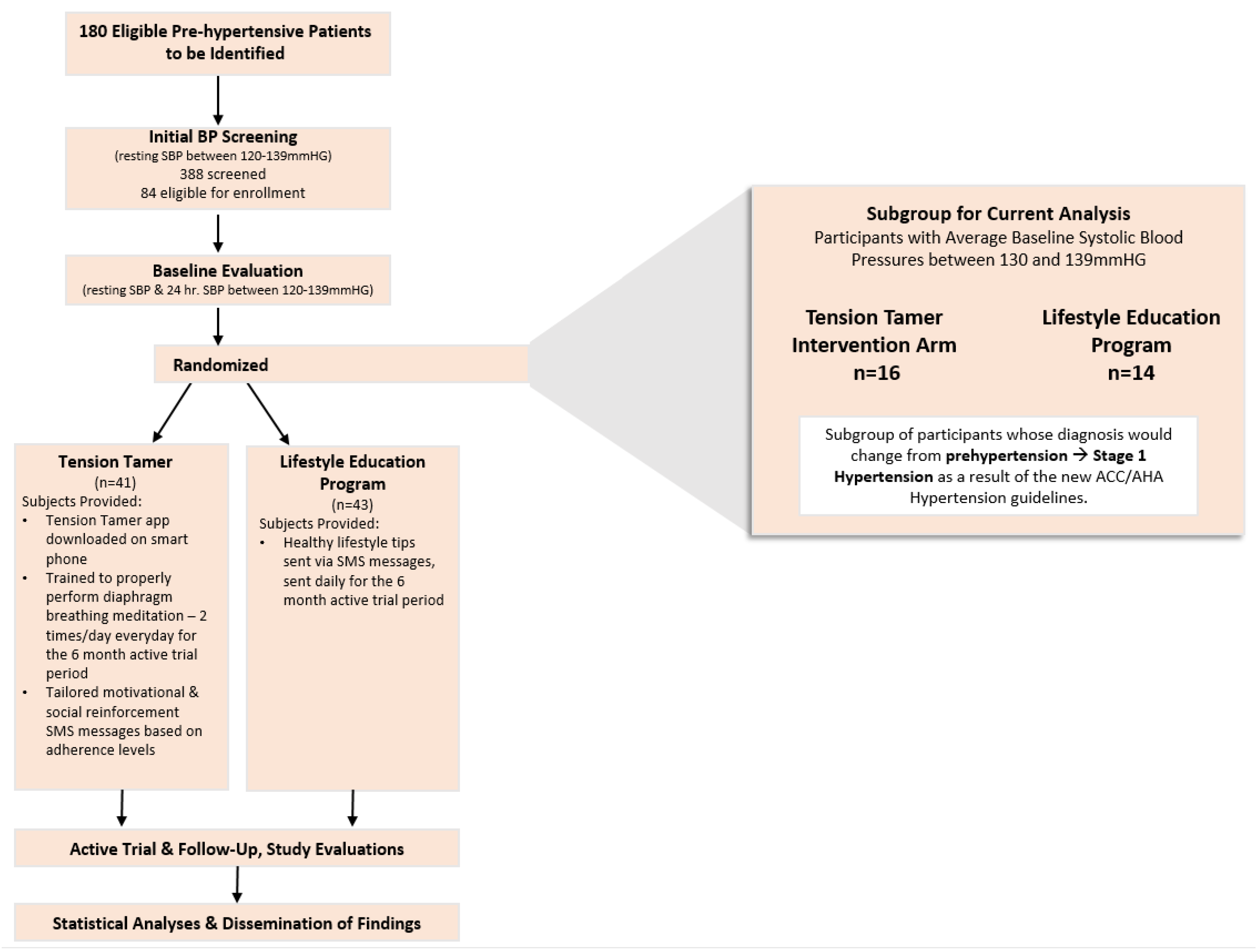
2.1. Research Design
2.2. Participants
2.3. Protocol, Intervention, and Groups
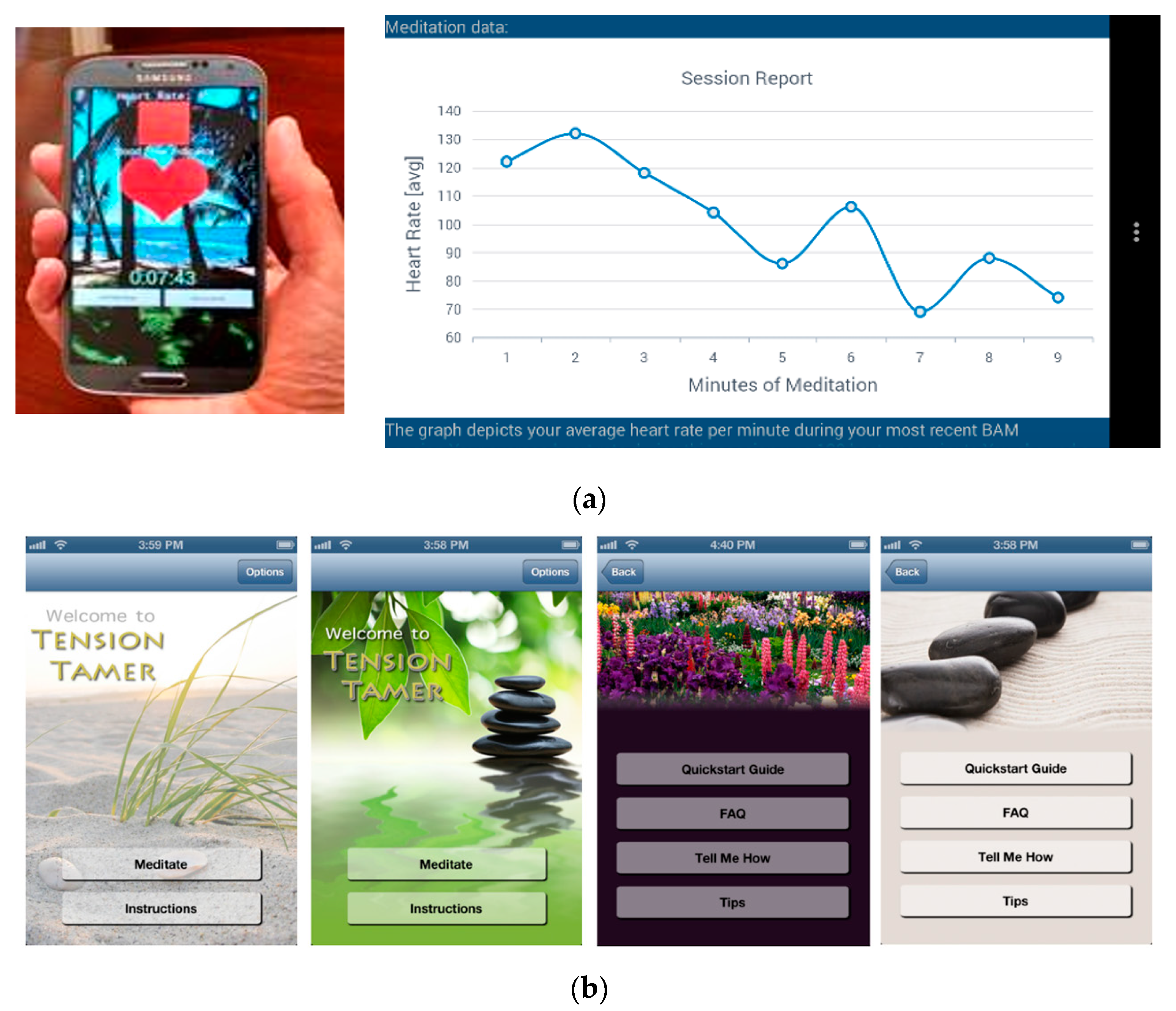
2.3.1. Tension Tamer (TT) Intervention Group
2.3.2. Lifestyle Education Program Delivered via Smartphone (SPCTL)
2.4. Outcome Measures
2.5. Statistical Analyses
3. Results
3.1. Recruitment and Retention Rates
3.2. Blood Pressure Control Changes
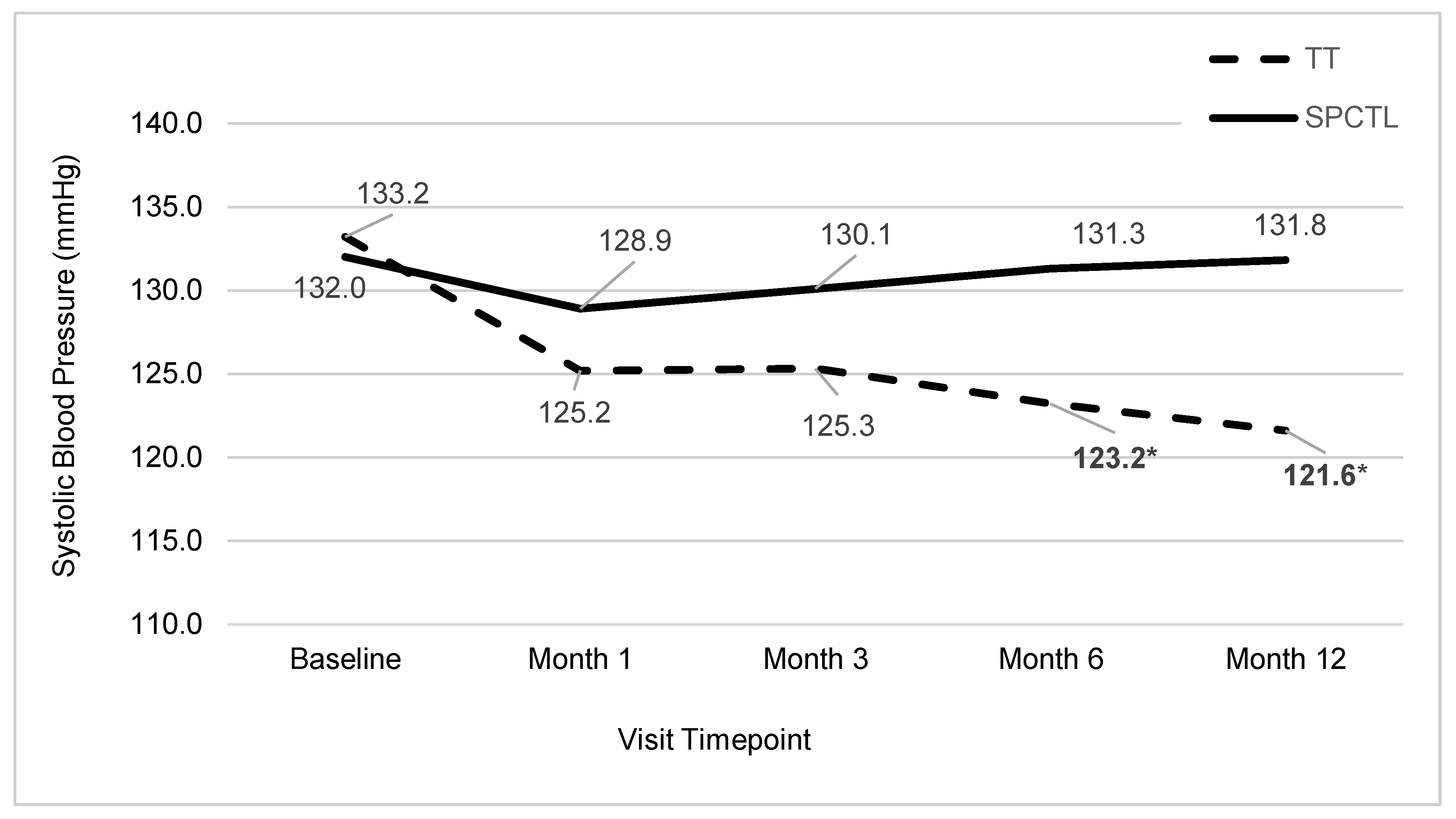
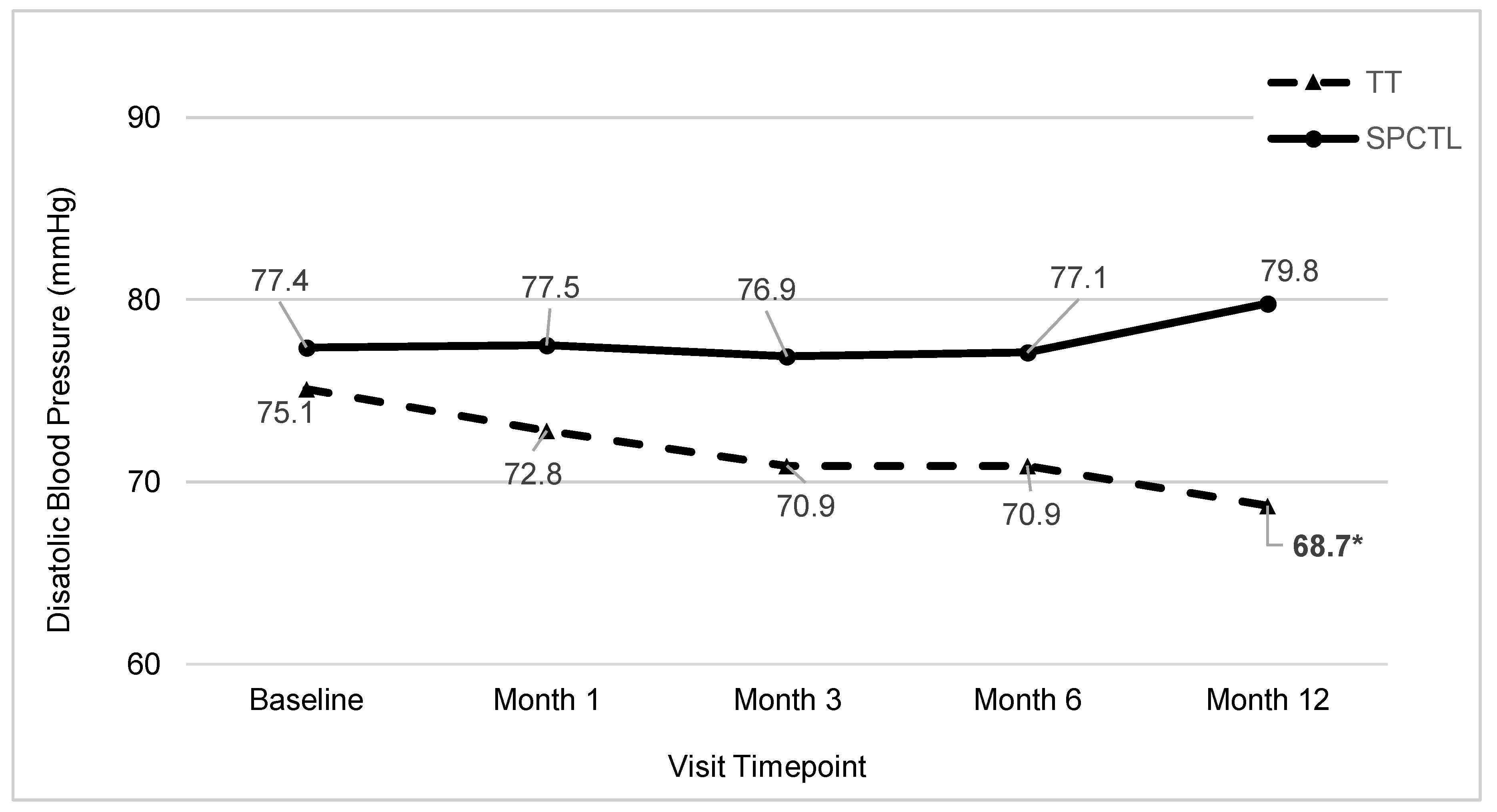
3.3. Resting Blood Pressure Level Changes
3.4. Adherence to TT and Runkeeper Dosage Rates
3.5. Perceived Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Muntner, P.; Carey, R.M.; Gidding, S.; Jones, D.W.; Taler, S.J.; Wright, J.T., Jr.; Whelton, P.K. Potential US Population Impact of the 2017 ACC/AHA High Blood Pressure Guideline. Circulation 2018, 137, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Khera, R.; Lu, Y.; Lu, J.; Saxena, A.; Nasir, K.; Jiang, L.; Krumholz, H.M. Impact of 2017 ACC/AHA guidelines on prevalence of hypertension and eligibility for antihypertensive treatment in United States and China: Nationally representative cross sectional study. BMJ 2018, 362, k2357. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 71, e127–e248. [Google Scholar] [PubMed]
- Nerenberg, K.A.; Zarnke, K.B.; Leung, A.A.; Dasgupta, K.; Butalia, S.; McBrien, K.; Harris, K.C.; Nakhla, M.; Cloutier, L.; Gelfer, M.; et al. Hypertension Canada’s 2018 Guidelines for Diagnosis, Risk Assessment, Prevention, and Treatment of Hypertension in Adults and Children. Can. J. Cardiol. 2018, 34, 506–525. [Google Scholar] [CrossRef]
- Levine, G.N.; Lange, R.A.; Bairey-Merz, C.N.; Davidson, R.J.; Jamerson, K.; Mehta, P.K.; Michos, E.D.; Norris, K.; Ray, I.B.; Saban, K.L.; et al. Meditation and Cardiovascular Risk Reduction: A Scientific Statement From the American Heart Association. J. Am. Heart Assoc. 2017, 6, e002218. [Google Scholar] [CrossRef]
- Esler, M.; Eikelis, N.; Schlaich, M.; Lambert, G.; Alvarenga, M.; Dawood, T.; Kaye, D.; Barton, D.; Pier, C.; Guo, L.; et al. Chronic mental stress is a cause of essential hypertension: Presence of biological markers of stress. Clin. Exp. Pharmacol. Physiol. 2008, 35, 498–502. [Google Scholar] [CrossRef]
- Rutledge, T.; Hogan, B.E. A quantitative review of prospective evidence linking psychological factors with hypertension development. Psychosom. Med. 2002, 64, 758–766. [Google Scholar]
- Spruill, T.M. Chronic psychosocial stress and hypertension. Curr. Hypertens. Rep. 2010, 12, 10–16. [Google Scholar] [CrossRef]
- Ospina, M.B.; Bond, K.; Karkhaneh, M.; Tjosvold, L.; Vandermeer, B.; Liang, Y.; Bialy, L.; Hooton, N.; Buscemi, N.; Dryden, D.M.; et al. Meditation practices for health: State of the research. Evid. Rep. Technol. Assess. (Full Rep.) 2007, 155, 1–263. [Google Scholar]
- Rainforth, M.V.; Schneider, R.H.; Nidich, S.I.; Gaylord-King, C.; Salerno, J.W.; Anderson, J.W. Stress reduction programs in patients with elevated blood pressure: A systematic review and meta-analysis. Curr. Hypertens. Rep. 2007, 9, 520–528. [Google Scholar] [CrossRef]
- Bussing, A.; Michalsen, A.; Khalsa, S.B.; Telles, S.; Sherman, K.J. Effects of yoga on mental and physical health: A short summary of reviews. Evid. Complement. Altern. Med. 2012, 2012, 165410. [Google Scholar] [CrossRef] [PubMed]
- Okonta, N.R. Does yoga therapy reduce blood pressure in patients with hypertension?: An integrative review. Holist. Nurs. Pract. 2012, 26, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.W.; Liu, C.; Kryscio, R.J. Blood pressure response to transcendental meditation: A meta-analysis. Am. J. Hypertens. 2008, 21, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Barnes, V.; Schneider, R.; Alexander, C.; Staggers, F. Stress, stress reduction, and hypertension in African Americans: An updated review. J. Natl. Med. Assoc. 1997, 89, 464. [Google Scholar] [PubMed]
- Goldstein, C.M.; Josephson, R.; Xie, S.; Hughes, J.W. Current perspectives on the use of meditation to reduce blood pressure. Int. J. Hypertens. 2012, 2012, 578397. [Google Scholar] [CrossRef] [PubMed]
- Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life; Hyperion Books: New York, NY, USA, 1994. [Google Scholar]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness; Revised and updated edition; Bantam Books: New York, NY, USA, 2013. [Google Scholar]
- Davidson, R.J.; Kaszniak, A.W. Conceptual and methodological issues in research on mindfulness and meditation. Am. Psychol. 2015, 70, 581–592. [Google Scholar] [CrossRef]
- Gregoski, M.J.; Mueller, M.; Vertegel, A.; Shaporev, A.; Jackson, B.B.; Frenzel, R.M.; Sprehn, S.M.; Treiber, F.A. Development and validation of a smartphone heart rate acquisition application for health promotion and wellness telehealth applications. Int. J. Telemed. Appl. 2012, 2012. [Google Scholar] [CrossRef]
- Gregoski, M.J.; Barnes, V.A.; Tingen, M.S.; Dong, Y.; Zhu, H.; Treiber, F.A. Differential Impact of Stress Reduction Programs upon Ambulatory Blood Pressure among African American Adolescents: Influences of Endothelin-1 Gene and Chronic Stress Exposure. Int. J. Hypertens. 2012, 2012, 510291. [Google Scholar] [CrossRef]
- Adams, Z.W.; Sieverdes, J.C.; Brunner-Jackson, B.; Mueller, M.; Chandler, J.; Diaz, V.; Patel, S.; Sox, L.R.; Wilder, S.; Treiber, F.A. Meditation smartphone application effects on prehypertensive adults’ blood pressure: Dose-response feasibility trial. Health Psychol. 2018, 37, 850. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Bandura, A. Social cognitive theory: An agentic perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Beynon-Davies, P.; Holmes, S. Design breakdowns, scenarios and rapid application development. Inf. Softw. Technol. 2002, 44, 579–592. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Nidich, S.I.; Rainforth, M.V.; Haaga, D.A.; Hagelin, J.; Salerno, J.W.; Travis, F.; Tanner, M.; Gaylord-King, C.; Grosswald, S.; Schneider, R.H. A randomized controlled trial on effects of the Transcendental Meditation program on blood pressure, psychological distress, and coping in young adults. Am. J. Hypertens. 2009, 22, 1326–1331. [Google Scholar] [CrossRef]
- Dickinson, H.; Campbell, F.; Beyer, F.; Nicolson, D.; Cook, J.; Ford, G.; Mason, J. Relaxation therapies for the management of primary hypertension in adults: A Cochrane review. J. Hum. Hypertens. 2008, 22, 809–820. [Google Scholar] [CrossRef]
- Wang, S.; Li, S.; Xu, X.; Lin, G.; Shao, L.; Zhao, Y.; Wang, T. Effect of slow abdominal breathing combined with biofeedback on blood pressure and heart rate variability in prehypertension. J. Altern. Complement. Med. 2010, 16, 1039–1045. [Google Scholar] [CrossRef]
- Mourya, M.; Mahajan, A.S.; Singh, N.P.; Jain, A.K. Effect of slow- and fast-breathing exercises on autonomic functions in patients with essential hypertension. J. Altern. Complement. Med. 2009, 15, 711–717. [Google Scholar] [CrossRef]
- Neter, J.E.; Stam, B.E.; Kok, F.J.; Grobbee, D.E.; Geleijnse, J.M. Influence of weight reduction on blood pressure: A meta-analysis of randomized controlled trials. Hypertension 2003, 42, 878–884. [Google Scholar] [CrossRef]
- Appel, L.J.; Champagne, C.M.; Harsha, D.W.; Cooper, L.S.; Obarzanek, E.; Elmer, P.J.; Stevens, V.J.; Vollmer, W.M.; Lin, P.H.; Svetkey, L.P.; et al. Effects of comprehensive lifestyle modification on blood pressure control: Main results of the PREMIER clinical trial. JAMA 2003, 289, 2083–2093. [Google Scholar]
- Appel, L.J.; Moore, T.J.; Obarzanek, E.; Vollmer, W.M.; Svetkey, L.P.; Sacks, F.M.; Bray, G.A.; Vogt, T.M.; Cutler, J.A.; Windhauser, M.M.; et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N. Engl. J. Med. 1997, 336, 1117–1124. [Google Scholar] [CrossRef]
- Goyal, M.; Singh, S.; Sibinga, E.M.; Gould, N.F.; Rowland-Seymour, A.; Sharma, R.; Berger, Z.; Sleicher, D.; Maron, D.D.; Shihab, H.M. Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Intern. Med. 2014, 174, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Julius, S.; Nesbitt, S. Sympathetic overactivity in hypertension: A moving target. Am. J. Hypertens. 1996, 9, 113S–120S. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic | Self-Reported Response | TT (n = 16) | SPCTL (n = 14) |
|---|---|---|---|
| Age (M+/− SD) | 46.5 ± 13.0 | 43.4 ± 14.2 | |
| Gender | Male | 48.7% | 49.3% |
| Female | 51.3% | 50.7% | |
| Race | African American | 51.3% | 42.1% |
| White | 48.7% | 57.9% | |
| Marital Status | Single | 6.7% | 20% |
| Married/Living with Significant Other | 73.3% | 66.7% | |
| Separated/Divorced | 13.3% | 6.7% | |
| Widowed | 6.7% | 6.7% | |
| Education | High School or less | 6.7% | 6.7% |
| Partial/College Grad | 93.3% | 93.3% | |
| Income | $0–25,000 | 20.0% | 33.3% |
| $25–50,000 | 13.3% | 13.3% | |
| >$50,000 | 53.3% | 53.3% | |
| Not Reported | 13.3% | 0% | |
| Employment | Full Time | 66.7% | 73.3% |
| Part-Time | 13.3% | 0% | |
| Retired/Disabled | 20.0% | 26.6% |
| Controlled SBP | TT | SPCTL | p-Value |
|---|---|---|---|
| Baseline | 0 | 0 | 0.481 |
| Month 1 | 68.8 | 35.7 | 0.074 |
| Month 3 | 73.3 | 57.1 | 0.377 |
| Month 6 | 78.6 | 35.7 | 0.021 |
| Month 12 | 91.7 | 50.0 | 0.029 |
| Controlled DBP | TT | SPCTL | p-Value |
|---|---|---|---|
| Baseline | Baseline | 75.0 | 0.771 |
| Month 1 | Month 1 | 87.5 | 0.642 |
| Month 3 | Month 3 | 86.7 | 0.642 |
| Month 6 | Month 6 | 85.7 | 0.571 |
| Month 9 | Month 12 | 83.3 | 0.600 |
| Time-Point | TT | SPCTL | p-Value |
|---|---|---|---|
| Month 1 | 77.3 | 68.2 | 0.288 |
| Month 3 | 77.1 | 67.1 | 0.408 |
| Month 6 | 78.0 | 61.5 | 0.189 |
| Month 12 | 69.8 | 65.2 | 0.760 |
| Timepoint | TT | HLAC | p-Value |
|---|---|---|---|
| Month 1 | 60.0 | 50.0 | 0.604 |
| Month 3 | 64.3 | 57.1 | 0.712 |
| Month 6 | 58.3 | 35.7 | 0.267 |
| Month 12 | 38.5 | 27.3 | 0.582 |
| Timepoint | TT | SPCTL | p-Value |
|---|---|---|---|
| Baseline | 56.3 | 64.2 | 0.667 |
| Month 1 | 56.3 | 60.8 | 0.182 |
| Month 3 | 50.0 | 42.9 | 0.717 |
| Month 6 | 23.1 | 46.2 | 0.233 |
| Month 12 | 38.5 | 50.0 | 0.600 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandler, J.; Sox, L.; Diaz, V.; Kellam, K.; Neely, A.; Nemeth, L.; Treiber, F. Impact of 12-Month Smartphone Breathing Meditation Program upon Systolic Blood Pressure among Non-Medicated Stage 1 Hypertensive Adults. Int. J. Environ. Res. Public Health 2020, 17, 1955. https://doi.org/10.3390/ijerph17061955
Chandler J, Sox L, Diaz V, Kellam K, Neely A, Nemeth L, Treiber F. Impact of 12-Month Smartphone Breathing Meditation Program upon Systolic Blood Pressure among Non-Medicated Stage 1 Hypertensive Adults. International Journal of Environmental Research and Public Health. 2020; 17(6):1955. https://doi.org/10.3390/ijerph17061955
Chicago/Turabian StyleChandler, Jessica, Luke Sox, Vanessa Diaz, Kinsey Kellam, Allison Neely, Lynne Nemeth, and Frank Treiber. 2020. "Impact of 12-Month Smartphone Breathing Meditation Program upon Systolic Blood Pressure among Non-Medicated Stage 1 Hypertensive Adults" International Journal of Environmental Research and Public Health 17, no. 6: 1955. https://doi.org/10.3390/ijerph17061955
APA StyleChandler, J., Sox, L., Diaz, V., Kellam, K., Neely, A., Nemeth, L., & Treiber, F. (2020). Impact of 12-Month Smartphone Breathing Meditation Program upon Systolic Blood Pressure among Non-Medicated Stage 1 Hypertensive Adults. International Journal of Environmental Research and Public Health, 17(6), 1955. https://doi.org/10.3390/ijerph17061955