Prevalence and Characterization of Specific Phobia Disorder in People over 65 Years Old in a Madrid Community Sample (Spain) and its Relationship to Quality of Life


Abstract

1. Introduction
2. Materials and Methods
2.1. Sample and Procedure
- -
- Living in Madrid;
- -
- Between 65 and 84 years of age;
- -
- Able to provide informed consent to participate in the study.
- -
- Presenting with a severe cognitive impairment as evaluated using a Mini-Mental State Examination [44] cut-off point of > 18;
- -
- Having a language barrier that prevented an interview.
2.2. Instruments
2.2.1. Evaluation of Specific Phobia Disorder
2.2.2. Level of Performance Evaluation
2.2.3. Evaluation of Quality of Life
2.3. Statistical Analyses
3. Results
3.1. Twelve-month Prevalence of Specific Phobia Disorder
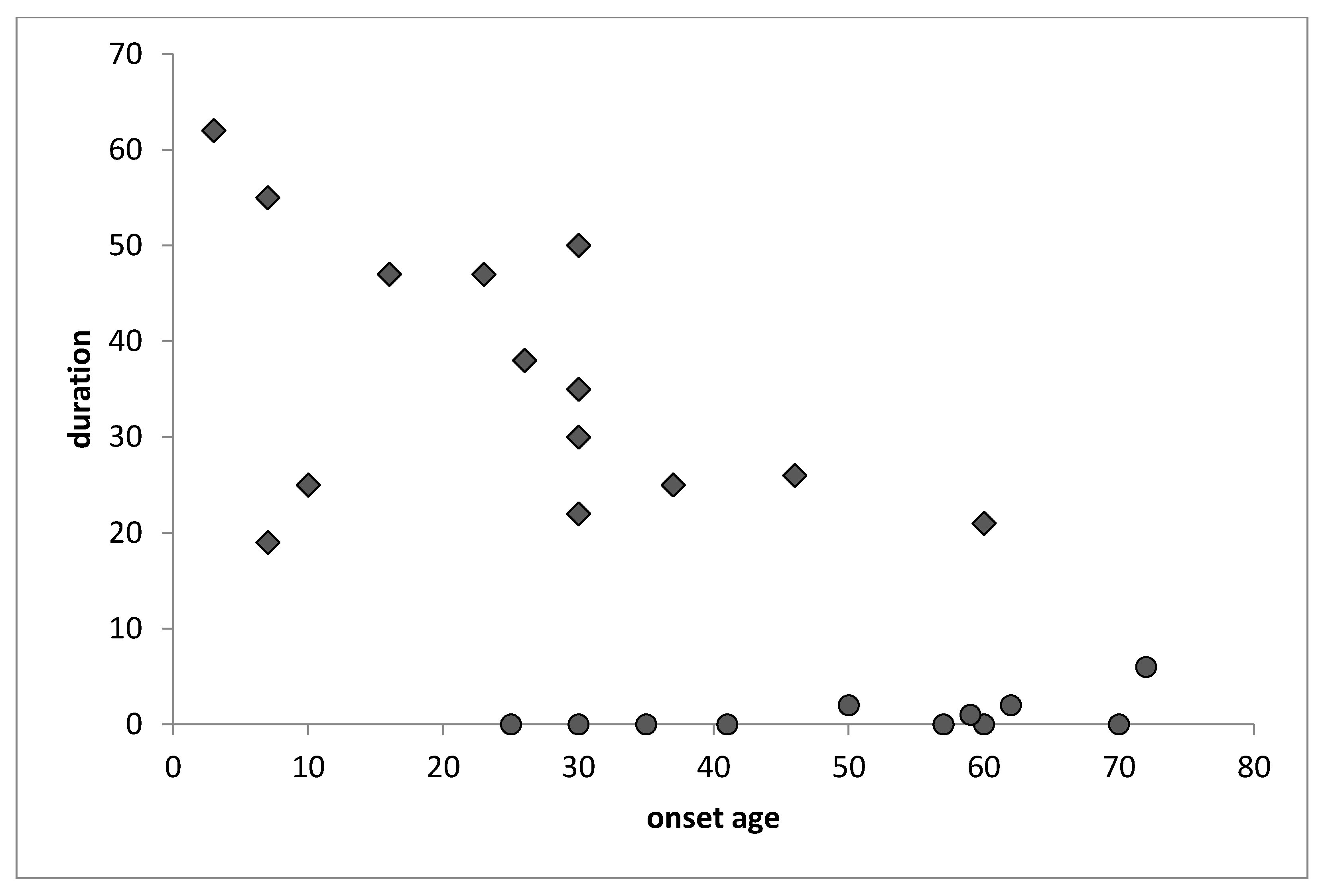
3.2. Age of Onset and Duration of Specific Phobia Disorder
3.3. Description of the Symptomatology of the Specific Phobia Disorder
3.3.1. Description of Problematic Situations
3.3.2. Description of Phobic Stimuli
3.3.3. Description of the Symptoms of Specific Phobia Disorder
3.4. Level of Functioning and Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Eurostat. European Health Interview Survey (EHIS); European Union: Luxembourg, 2014. [Google Scholar]
- Kessler, R.C.; Üstün, T.B. (Eds.) The WHO World Mental Health Surveys: Global Perspectives on the Epidemiology of Mental Disorders (Volume 6); Cambridge University Press: New York, NY, USA, 2008. [Google Scholar]
- Alonso, J.; Angermeyer, M.; Bernert, S.; Bruffaerts, R.; Brugha, T.; Bryson, H.; Vollebergh, W. Prevalence of mental disorders in Europe: Results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr. Scand. 2004, 109, 21–27. [Google Scholar] [CrossRef]
- Prince, M.J.; Wu, F.; Guo, Y.; Robledo, L.M.G.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Segal, D.L.; Qualls, S.H.; Smyer, M.A. Aging and Mental Health; John Wiley & Sons: Hoboken, NJ, USA, 2018. [Google Scholar]
- World Health Organization. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization world mental health surveys. J. Am. Med. Assoc. 2004, 291, 2581–2590. [Google Scholar] [CrossRef] [PubMed]
- Volkert, J.; Schulz, H.; Härter, M.; Wlodarcyzk, O.; Andreas, S. The prevalence of mental disorders in older people in Western countries- a meta analysis. Ageing Res. Rev. 2013, 12, 339–353. [Google Scholar] [CrossRef] [PubMed]
- Jeste, D.V.; Blazer, D.G.; First, M.A. Aging-related diagnostic variations: Need for diagnostic criteria appropriate for elderly psychiatric patients. Biol. Psychiatry 2005, 58, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Lenze, E.J.; Loebach-Wetherell, J. A lifespan view of anxiety disorders. Dialogues Clin. Neurosci. 2011, 13, 381–399. [Google Scholar] [PubMed]
- Mohlman, J.; Bryant, C.; Lenze, E.J.; Stanley, M.A.; Gum, A.; Flint, A.; Craske, M.G. Improving recognition of late life anxiety disorders in Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition: Observations and recommendations of the Advisory Committee to the Lifespan Disorders Work Group. Int. J. Geriatr. Psychiatry 2012, 27, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Wolitzky-Taylor, K.B.; Castriotta, N.; Lenze, E.J.; Stanley, M.A.; Craske, M.G. Anxiety disorders in older adults: A comprehensive review. Depress. Anxiety 2010, 27, 190–211. [Google Scholar] [CrossRef]
- Cisneros, G.A.; Ausín, B. Prevalencia de los trastornos de ansiedad en las personas mayores de 65 años: Una revisión sistemática. Revista Española de Geriatría y Gerontología 2018, 54, 34–48. [Google Scholar] [CrossRef]
- Andreas, S.; Schulz, H.; Volkert, J.; Dehoust, M.; Sehner, S.; Suling, A.; Härter, M. Prevalence of mental disorders in elderly people: The European MentDis_ICF65+ study. Br. J. Psychiatry 2017, 210, 125–131. [Google Scholar] [CrossRef]
- Beekman, A.; Bremmer, M.; Deeg, D.; van Balkom, A.; Smit, J.; Van Tilburg, W. Anxiety disorders in later life: A report from the longitudinal aging study Amsterdam. Int. J. Geriatr. Psychiatry 1998, 13, 717–726. [Google Scholar] [CrossRef]
- Canuto, A.; Weber, K.; Baertschi, M.; Andreas, S.; Volkert, J.; Dehoust, M.; Härter, M. Anxiety disorders in old age: Psychiatric comorbidities, quality of life, and prevalence according to age, gender, and country. Am. J. Geriatr. Psychiatry 2018, 26, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Grenier, S.; Schuurmans, J.; Goldfarb, M.; Préville, M.; Boyer, R.; O’Connor, K.; Hudon, C. The epidemiology of specific phobia and subthreshold fear subtypes in a community-based sample of older adults. Depress. Anxiety 2011, 28, 456–463. [Google Scholar] [CrossRef] [PubMed]
- Gum, A.M.; King-Kallimanis, B.; Kohn, R. Prevalence of mood, anxiety, and substance-abuse disorders for older Americans in the national comorbidity survey-replication. Am. J. Geriatr. Psychiatry 2009, 17, 769–781. [Google Scholar] [CrossRef] [PubMed]
- Trollor, J.; Anderson, T.; Sachdev, P.; Brodaty, H.; Andrews, G. Prevalence of mental disorders in the elderly: The Australian National Mental Health and Well-Being Survey. Am. J. Geriatr. Psychiatry 2007, 15, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Byers, A.; Yaffe, K.; Covinsky, K.; Friedman, M.; Bruce, M. High occurrence of mood and anxiety disorders among older adults. Arch. Gen. Psychiatry 2010, 67, 489–496. [Google Scholar] [CrossRef]
- Streiner, D.; Cairney, J.; Veldhuizen, S. The epidemiology of psychological problems in the elderly. Can. J. Psychiatry 2006, 51, 185–191. [Google Scholar] [CrossRef]
- Kirmizioglu, Y.; Doğan, O.; Kuğu, N.; Akyüz, G. Prevalence of anxiety disorders among elderly people. Int. J. Geriatr. Psychiatry 2009, 24, 1026–1033. [Google Scholar] [CrossRef]
- McCabe, L.; Cairney, J.; Veldhuizen, S.; Herrmann, N.; Streiner, D. Prevalence and correlates of agoraphobia in older adults. Am. J. Geriatr. Psychiatry 2006, 14, 515–522. [Google Scholar] [CrossRef]
- Corna, L.; Cairney, J.; Herrmann, N.; Veldhuizen, S.; McCabe, L.; Streiner, D. Panic disorder in later life: Results from a national survey of Canadians. Int. Psychogeriatr. 2007, 19, 1084–1096. [Google Scholar] [CrossRef]
- Zhang, X.; Norton, J.; Carrière, I.; Ritchie, K.; Chaudieu, I.; Ancelin, M. Generalized anxiety in community-dwelling elderly: Prevalence and clinical characteristics. J. Affect. Disord. 2015, 172, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Üstün, T.B. The world mental health (WMH) survey initiative version of the world health organization (WHO) composite international diagnostic interview (CIDI). Int. J. Methods Psychiatr. Res. 2004, 13, 93–121. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.; Lecrubier, Y.; Harnett-Sheehan, K.; Janavs, J.; Weiller, E.; Bonora, L.; Dunbar, G. The validity of the Mini International Neuropsychiatric Interview (MINI) according to the SCID-P and its reliability. Eur. Psychiatry 1997, 12, 232–241. [Google Scholar] [CrossRef]
- Grenier, S.; Desjardins, F.; Raymond, B.; Payette, M.C.; Rioux, M.È.; Landreville, P.; Vasiliadis, H.M. Six-month prevalence and correlates of Generalized Anxiety Disorder among primary care patients aged 70 years and over: Results from the ESA-services study. Int. J. Geriatr. Psychiatry 2018, 34, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Andreas, S.; Härter, M.; Volkert, J.; Hausberg, M.; Sehner, S.; Wegscheider, K.; Schulz, H. The MentDis_ICF65+ study protocol: Prevalence, 1-year incidence and symptom severity of mental disorders in the elderly and their relationship to functioning (ICF) and service utilisation. BMC Psychiatry 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Wittchen, H.U.; Strehle, J.; Gerschler, A.; Volkert, J.; Dehoust, M.; Sehner, S.; Andreas, S. Measuring symptoms and diagnosing mental disorders in the elderly community: The test-retest reliability of the CIDI65+. Int. J. Methods Psychiatr. Res. 2015, 24, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Becker, E.S.; Rinck, M.; Türke, V.; Kause, P.; Goodwin, R.; Neumer, S.; Margraf, J. Epidemiology of specific phobia subtypes: Findings from the Dresden Mental Health Study. Eur. Psychiatry 2007, 22, 69–74. [Google Scholar] [CrossRef]
- Wardenaar, K.J.; Lim, C.C.; Al-Hamzawi, A.O.; Alonso, J.; Andrade, L.H.; Benjet, C.; Gureje, O. The cross-national epidemiology of specific phobia in the World Mental Health Surveys. Psychol. Med. 2017, 47, 1744–1760. [Google Scholar] [CrossRef]
- Sancassiani, F.; Romano, F.; Balestrieri, M.; Caraci, F.; Di Sciascio, G.; Drago, F.; Preti, A. The prevalence of Specific Phobia by age in an Italian nationawide survey: How much does it affect the quality of life? Clin. Pract. Epidemiol. Ment. Health 2019, 15, 30. [Google Scholar] [CrossRef]
- Bijl, R.V.; Ravelli, A.; van Zessen, G. Prevalence of psychiatric disorder in the general population: Results of the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Soc. Psychiatry Psychiatr. Epidemiol. 1998, 33, 587–595. [Google Scholar] [CrossRef]
- Bourdon, K.H.; Boyd, J.H.; Rae, D.S.; Burns, B.J.; Thompson, J.W.; Locke, B.Z. Gender differences in phobias: Results of the ECA community survey. J. Anxiety Disord. 1988, 2, 227–241. [Google Scholar] [CrossRef]
- Fredrikson, M.; Annas, P.; Fischer, H.; Wik, G. Gender and age differences in the prevalence of specific fears and phobias. Behav. Res. Ther. 1996, 34, 33–39. [Google Scholar] [CrossRef]
- Kessler, R.C.; McGonagle, K.A.; Zhao, S.; Nelson, C.B.; Hughes, M.; Eshleman, S.; Wittchen, H.-U.; Kendler, K.S. Lifetime and 12 month prevalence of DSM-III-R psychiatric disorders in the United States: Results from the National Comorbidity Survey. Arch. Gen. Psychiatry 1994, 51, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Stinson, F.S.; Dawson, D.A.; Chou, S.P.; Smith, S.; Goldstein, R.B.; Ruan, W.J.; Grant, B.F. The epidemiology of DSM-IV specific phobia in the USA: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Psychol. Med. 2007, 37, 1047–1059. [Google Scholar] [CrossRef] [PubMed]
- Depla, M.F.; ten Have, M.L.; van Balkom, A.J.; de Graaf, R. Specific fears and phobias in the general population: Results from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 200–208. [Google Scholar] [CrossRef]
- Goisman, R.M.; Allsworth, J.; Rogers, M.P.; Warshaw, M.G.; Goldenberg, I.; Vasile, R.G.; Rodriguez-Villa, F.; Mallya, G.; Keller, M.B. Simple phobia as a comorbid anxiety disorder. Depress. Anxiety 1998, 7, 105–112. [Google Scholar] [CrossRef]
- Magee, W.J.; Eaton, W.W.; Wittchen, H.U.; McGonagle, K.A.; Kessler, R.C. Agoraphobia, simple phobia, and social phobia in the national comorbidity survey. Arch. Gen. Psychiatry 1996, 53, 159–168. [Google Scholar] [CrossRef]
- Mackenzie, C.S.; Reynolds, K.; Chou, B.A.K.-L.; Pagura, J.; Sareen, J. Prevalence and correlates of Generalized Anxiety Disorder in a national sample of older adults. Am. J. Psychiatry 2011, 19, 305–315. [Google Scholar] [CrossRef]
- Porensky, E.K.; Dew, M.A.; Karp, J.F.; Skidmore, E.; Rollman, B.L.; Shear, M.K.; Lenze, E.J. The burden of late-life generalized anxiety disorder: Effects on disability, health-related quality of life, and healthcare utilization. Am. J. Geriatr. Psychiatry 2009, 17, 473–482. [Google Scholar] [CrossRef]
- Sarma, S.I.; Byrne, G.J. Relationship between anxiety and quality of life in older mental health patients. Australas. J. Ageing 2014, 33, 201–204. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- American Psychatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; Text Revision; American Psychiatric Publishing: Washington, DC, USA, 2000. [Google Scholar]
- American Psychiatric Association. DSM-5: Manual Diagnóstico e Estatístico de Transtornos Mentais; Artmed Editora: Rio, Brazil, 2014. [Google Scholar]
- Üstün, T.B.; Kostanjsek, N.; Chatterji, S.; Rehm, J. (Eds.) Measuring Health and Disability: Manual for WHO Disability Assessment Schedule WHODAS 2.0; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Burns, A.; Beevor, A.; Lelliott, P.; Wing, J.; Blakey, A.; Orrell, M.; Hadden, S. Health of the Nation Outcome Scales for elderly people (HoNOS 65+). Br. J. Psychiatry 1999, 174, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Ausín, B.; Muñoz, M.; Quiroga, M.Á. Adaptación española de las escalas de resultados para personas mayores HoNOS65+ (Health of the Nation Outcome Scales for Older Adults). Revista Española de Geriatría y Gerontología 2007, 42, 88–95. [Google Scholar] [CrossRef]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadística. Censo de Poblaciones y Viviendas [Census of Population and Housing]. Catalogue Number 30243. 2011. Available online: http://www.ine.es/censos2011_datos/cen11_datos_inicio.htm (accessed on 13 February 2012).
- R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing; Vienna, Austria, 2015. Available online: https://www.R-project.org/ (accessed on 15 March 2020).
- Aragon, T.J. Epitools: Epidemiology Tools. R Package Version 0.5-10. 2017. Available online: https://CRAN.R-project.org/package=epitools (accessed on 15 March 2020).
- Volkert, J.; Andreas, S.; Härter, M.; Dehoust, M.; Sehner, S.; Suling, A.; Schulz, H. Predisposing, enabling and need factors of service utilization in the elderly with mental health problems. Int. Psychogeriatr. 2018, 30, 1027–1037. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Reducing stigma and discrimination against older people with mental disorders. In A Technical Consensus Statement; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Wetherell, J.L.; Thorp, S.R.; Patterson, T.L.; Golshan, S.; Jeste, D.V.; Gatz, M. Quality of life in geriatric generalized anxiety disorder: A preliminary investigation. J. Psychiatr. Res. 2004, 38, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Comer, J.S.; Blanco, C.; Hasin, D.S.; Liu, S.M.; Grant, B.F.; Turner, J.B.; Olfson, M. Health-related quality of life across the anxiety disorders: Results from the national epidemiologic survey on alcohol and related conditions (NESARC). J. Clin. Psychiatry 2011, 72, 43–50. [Google Scholar] [CrossRef]
- Moffitt, T.E.; Caspi, A.; Taylor, A.; Kokaua, J.; Milne, B.J.; Polanczyk, G.; Poulton, R. How common are common mental disorders? Evidence that lifetime prevalence rates are doubled by prospective versus retrospective ascertainment. Psychol. Med. 2010, 40, 899–909. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Socio-demographic Characteristics | Nº | Prevalence (%) |
|---|---|---|
| Gender | ||
| Men | 267 | 48.1 |
| Women | 288 | 51.9 |
| Age (Average) | ||
| 65–74 | 296 | 53.3 |
| 75–84 | 259 | 46.7 |
| Country born | ||
| Spain | 547 | 98.6 |
| Other | 8 | 1.4 |
| Parents born in the same country | ||
| No | 11 | 2 |
| Yes | 544 | 98 |
| Marital Status | ||
| Married | 336 | 60.5 |
| Separated | 13 | 2.3 |
| Divorced | 28 | 5 |
| Widower | 151 | 27.2 |
| Never been married | 26 | 4.7 |
| Other | 1 | 0.2 |
| Widower since (nº ages) | 13.09 (0–50) | |
| School/education | ||
| No | 258 | 46.5 |
| Yes | 297 | 53.5 |
| Years of schooling | ||
| 0–3 | 88 | 15.9 |
| 4–12 | 338 | 61.1 |
| 13+ | 127 | 23 |
| Work status | ||
| Retired | 400 | 72.1 |
| Homemaker/housewife | 137 | 24.7 |
| Working/employed | 13 | 2.3 |
| Unemployed | 4 | 0.7 |
| Other | 1 | 0.2 |
| Prevalence Rate | Odds Ratio | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Disorder | N(555) | INE 2011 | Total | Men | Woman | 65–74 | 75–84 | Men/woman | 65–74/75–84 |
| Specific phobia (12 months) | 67 | 111438 | 0.13 | 0.07 | 0.17 | 0.16 | 0.08 | 0.38 *** (0.21–0.69) | 2.08 ** (1.18–3.79) |
| Type of specific phobia | |||||||||
| Animals (vital) | 43 | 73922 | 0.08 | 0.02 | 0.13 | 0.10 | 0.05 | 0.13 *** (0.04–0.33) | 1.9 (0.95–3.98) |
| Animals (12 months) | 23 | 39701 | 0.05 | 0.01 | 0.07 | 0.05 | 0.03 | 0.1 *** (0.01–0.4) | 1.38 (0.54–3.68) |
| Animals (month) | 14 | 24163 | 0.03 | 0.00 | 0.05 | 0.03 | 0.02 | 0.08 ** (0–0.54) | 1.59 (0.47–6.13) |
| Natural environment (vital) | 45 | 75145 | 0.09 | 0.06 | 0.10 | 0.11 | 0.05 | 0.51 * (0.25–1.01) | 2.29 * (1.14–4.87) |
| Natural environment (12 months) | 27 | 45381 | 0.05 | 0.03 | 0.07 | 0.07 | 0.03 | 0.36 * (0.13–0.91) | 2.6 * (1.04–7.42) |
| Natural environment (month) | 15 | 24880 | 0.03 | 0.02 | 0.03 | 0.04 | 0.02 | 0.53 (0.14–1.73) | 2.46 (0.72–10.71) |
| Blood-injections-injuries (vital) | 31 | 49672 | 0.06 | 0.06 | 0.06 | 0.06 | 0.05 | 1.01 (0.46–2.24) | 1.41 (0.64–3.26) |
| Blood-injections-injuries (12 months) | 19 | 30778 | 0.04 | 0.03 | 0.04 | 0.04 | 0.03 | 0.62 (0.2–1.74) | 1.21 (0.44–3.53) |
| Blood-injections-injuries (month) | 7 | 10216 | 0.01 | 0.02 | 0.01 | 0.01 | 0.02 | 2.72 (0.44–28.84) | 0.65 (0.09–3.9) |
| Situational (vital) | 33 | 54871 | 0.06 | 0.04 | 0.07 | 0.07 | 0.05 | 0.6 (0.26–1.31) | 1.57 (0.72–3.58) |
| Situational (12 months) | 14 | 23490 | 0.03 | 0.01 | 0.03 | 0.02 | 0.03 | 0.42 (0.1–1.49) | 0.65 (0.18–2.17) |
| Situational (month) | 6 | 10207 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.54 (0.05–3.78) | 0.87 (0.12–6.58) |
| Psychosocial Factors | Coefficient | std. Error | OR | CI (95%) of OR |
|---|---|---|---|---|
| Age | −0.07 | 0.02 | 0.93 | (0.89–0.97) |
| Gender (men/women) | −0.93 | 0.29 | 0.40 | (0.22–0.69) |
| Number of significant people | −0.05 | 0.02 | 0.95 | (0.91–0.98) |
| Prevalence Rate | Odds Ratio | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | N (555) | Statistics National Institute (INE) 2011 | Total | Hombres | Women | 65–74 | 75–84 | Men/Women | 65–74/75–84 |
| Problematic situations | |||||||||
| Being outside home alone | 24 | 39690 | 0.27 | 0.21 | 0.30 | 0.21 | 0.35 | 0.63 (0.18–1.95) | 0.5 (0.17–1.45) |
| Travelling on a bus. train. underground/subway or using other public transport | 24 | 40287 | 0.27 | 0.24 | 0.28 | 0.29 | 0.24 | 0.83 (0.25–2.49) | 1.3 (0.44–4.03) |
| Being in a crowd or standing in line | 43 | 69131 | 0.47 | 0.52 | 0.46 | 0.46 | 0.50 | 1.26 (0.47–3.37) | 0.87 (0.34–2.22) |
| Being in a public place. such as shops. markets. department store. a theatre. or car park | 7 | 12171 | 0.08 | 0.00 | 0.11 | 0.07 | 0.09 | 0 (0–1.4) | 0.8 (0.13–5.8) |
| Travelling alone or going on a long trip | 17 | 28939 | 0.20 | 0.07 | 0.25 | 0.14 | 0.26 | 0.23 * (0.02–1.11) | 0.47 (0.14–1.55) |
| Crossing a bridge | 29 | 48386 | 0.33 | 0.28 | 0.34 | 0.34 | 0.29 | 0.73 (0.24–2.09) | 1.23 (0.45–3.5) |
| Stimuli | |||||||||
| Living things like insects. snakes. birds. or other animals | 143 | 240091 | 0.27 | 0.13 | 0.38 | 0.31 | 0.20 | 0.25 *** (0.16–0.39) | 1.84 ** (1.22–2.79) |
| The sight of blood | 50 | 80904 | 0.09 | 0.09 | 0.09 | 0.11 | 0.07 | 1.09 (0.58–2.03) | 1.62 (0.86–3.15) |
| Getting an injection | 22 | 35917 | 0.04 | 0.04 | 0.04 | 0.05 | 0.02 | 0.9 (0.34–2.3) | 2.41 (0.88–7.63) |
| Going to the dentist or hospital | 61 | 99273 | 0.11 | 0.09 | 0.13 | 0.12 | 0.10 | 0.72 (0.4–1.28) | 1.2 (0.68–2.15) |
| Heights | 104 | 167760 | 0.19 | 0.19 | 0.19 | 0.20 | 0.17 | 1 (0.64–1.56) | 1.18 (0.75–1.87) |
| Storms. thunder. or lightning | 53 | 89110 | 0.10 | 0.04 | 0.15 | 0.12 | 0.07 | 0.25 *** (0.11–0.51) | 1.97 * (1.05–3.84) |
| Being in water. such as a lake or swimming pool | 21 | 35095 | 0.04 | 0.01 | 0.06 | 0.04 | 0.03 | 0.24 ** (0.06–0.76) | 1.17 (0.45–3.21) |
| Flying in an airplane | 51 | 82993 | 0.09 | 0.08 | 0.10 | 0.11 | 0.07 | 0.8 (0.43–1.49) | 1.68 (0.89–3.25) |
| Being in a closed space like a basement. tunnel. or elevator | 86 | 144121 | 0.16 | 0.09 | 0.22 | 0.18 | 0.13 | 0.36 *** (0.21–0.61) | 1.41 (0.86–2.33) |
| Any other situations | 8 | 13353 | 0.02 | 0.00 | 0.02 | 0.01 | 0.02 | 0.15 * (0–1.19) | 0.87 (0.16–4.74) |
| Without fear | 285 | 433604 | 0.50 | 0.61 | 0.43 | 0.45 | 0.59 | 2.07 *** (1.45–2.95) | 0.56 *** (0.39–0.79) |
| General Symptomatology | |||||||||
| Pounding or racing heart | 38 | 62499 | 0.42 | 0.45 | 0.41 | 0.43 | 0.41 | 1.17 (0.43–3.12) | 1.07 (0.42–2.8) |
| Sweating | 24 | 39059 | 0.26 | 0.31 | 0.25 | 0.30 | 0.21 | 1.37 (0.45–4.04) | 1.67 (0.56–5.45) |
| Trembling or shaking | 16 | 25575 | 0.17 | 0.24 | 0.15 | 0.16 | 0.21 | 1.83 (0.51–6.33) | 0.74 (0.22–2.63) |
| Dry mouth | 29 | 47157 | 0.32 | 0.34 | 0.31 | 0.36 | 0.26 | 1.16 (0.4–3.25) | 1.54 (0.56–4.5) |
| Difficulty breathing or shortness of breath | 28 | 45547 | 0.31 | 0.34 | 0.30 | 0.30 | 0.32 | 1.25 (0.43–3.53) | 0.91 (0.33–2.56) |
| Sensation of choking | 26 | 42178 | 0.29 | 0.41 | 0.23 | 0.32 | 0.24 | 2.35 (0.82–6.77) | 1.53 (0.53–4.71) |
| Pain or discomfort in chest | 5 | 8044 | 0.05 | 0.03 | 0.07 | 0.07 | 0.03 | 0.51 (0.01–5.5) | 2.52 (0.24–128.66) |
| Stomach pains or discomfort in stomach | 9 | 15305 | 0.10 | 0.07 | 0.11 | 0.13 | 0.06 | 0.57 (0.05–3.3) | 2.27 (0.4–23.71) |
| Feeling dizzy or lightheaded | 14 | 23452 | 0.16 | 0.21 | 0.13 | 0.20 | 0.09 | 1.72 (0.44–6.4) | 2.5 (0.59–15.11) |
| Things around you seemed unreal | 9 | 14474 | 0.10 | 0.17 | 0.07 | 0.13 | 0.06 | 2.93 (0.58–16.12) | 2.27 (0.4–23.71) |
| Afraid of losing control or acting crazy | 10 | 16015 | 0.11 | 0.21 | 0.07 | 0.16 | 0.03 | 3.66 (0.78–19.33) | 6.22 (0.8–284.83) |
| Afraid of dying | 15 | 23579 | 0.16 | 0.28 | 0.11 | 0.20 | 0.12 | 2.9 (0.81–10.73) | 1.82 (0.48–8.59) |
| Hot flushes or chills | 18 | 29367 | 0.20 | 0.24 | 0.18 | 0.23 | 0.15 | 1.44 (0.41–4.73) | 1.74 (0.51–6.94) |
| Tingling or numbness in hands. arms. or legs | 13 | 21205 | 0.14 | 0.14 | 0.15 | 0.13 | 0.18 | 0.93 (0.19–3.73) | 0.67 (0.17–2.67) |
| No symptoms | 23 | 37042 | 0.25 | 0.21 | 0.28 | 0.20 | 0.35 | 0.68 (0.19–2.12) | 0.45 (0.15–1.32) |
| Disorder | R | p-Value | R2 | |
|---|---|---|---|---|
| Specific phobia | Global WHODAS II | 0.12 | 0.004 | 0.01 |
| Specific phobia | Total HoNOS65+ | 0.19 | 0.000 | 0.03 |
| Specific phobia | Total WHOQOL-BREF | −0.08 | 0.048 | 0.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ausín, B.; Muñoz, M.; Castellanos, M.Á.; García, S. Prevalence and Characterization of Specific Phobia Disorder in People over 65 Years Old in a Madrid Community Sample (Spain) and its Relationship to Quality of Life. Int. J. Environ. Res. Public Health 2020, 17, 1915. https://doi.org/10.3390/ijerph17061915
Ausín B, Muñoz M, Castellanos MÁ, García S. Prevalence and Characterization of Specific Phobia Disorder in People over 65 Years Old in a Madrid Community Sample (Spain) and its Relationship to Quality of Life. International Journal of Environmental Research and Public Health. 2020; 17(6):1915. https://doi.org/10.3390/ijerph17061915
Chicago/Turabian StyleAusín, Berta, Manuel Muñoz, Miguel Ángel Castellanos, and Sara García. 2020. "Prevalence and Characterization of Specific Phobia Disorder in People over 65 Years Old in a Madrid Community Sample (Spain) and its Relationship to Quality of Life" International Journal of Environmental Research and Public Health 17, no. 6: 1915. https://doi.org/10.3390/ijerph17061915
APA StyleAusín, B., Muñoz, M., Castellanos, M. Á., & García, S. (2020). Prevalence and Characterization of Specific Phobia Disorder in People over 65 Years Old in a Madrid Community Sample (Spain) and its Relationship to Quality of Life. International Journal of Environmental Research and Public Health, 17(6), 1915. https://doi.org/10.3390/ijerph17061915