Attitudes of Nursing Home Staff towards Influenza Vaccination: Opinions and Factors Influencing Hesitancy

 , ,
, ,
Abstract
:1. Introduction
- To describe adherence and attitudes of NH staff towards flu vaccination;
- To explore staff hesitancy and its relationship with the attitude towards flu vaccination.
2. Materials and Methods
2.1. Instrument: NH Staff Survey
2.2. Population and Data Collection
2.3. Data Assessment and Statistical Analysis
3. Results
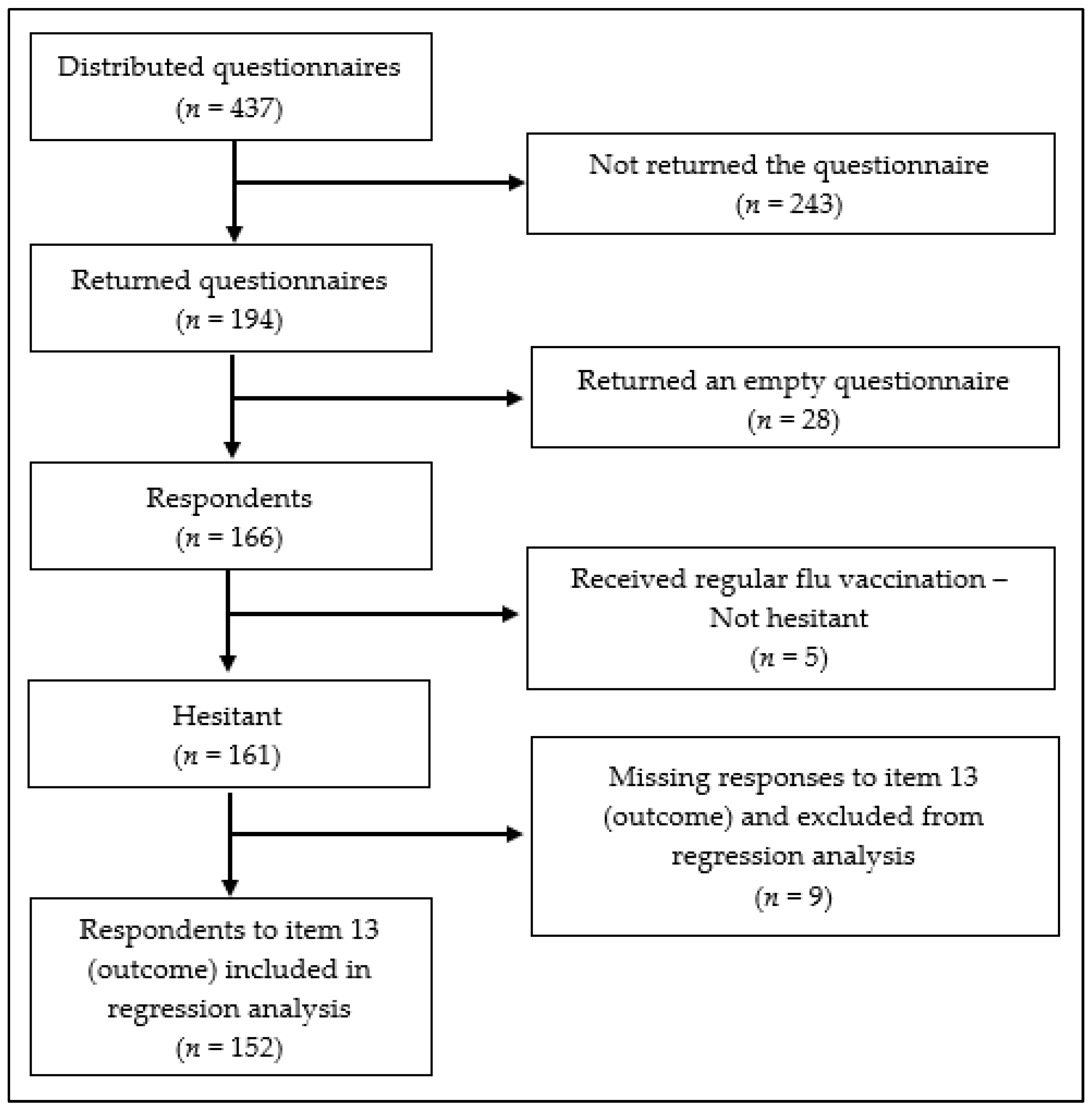
3.1. Survey Response Rate
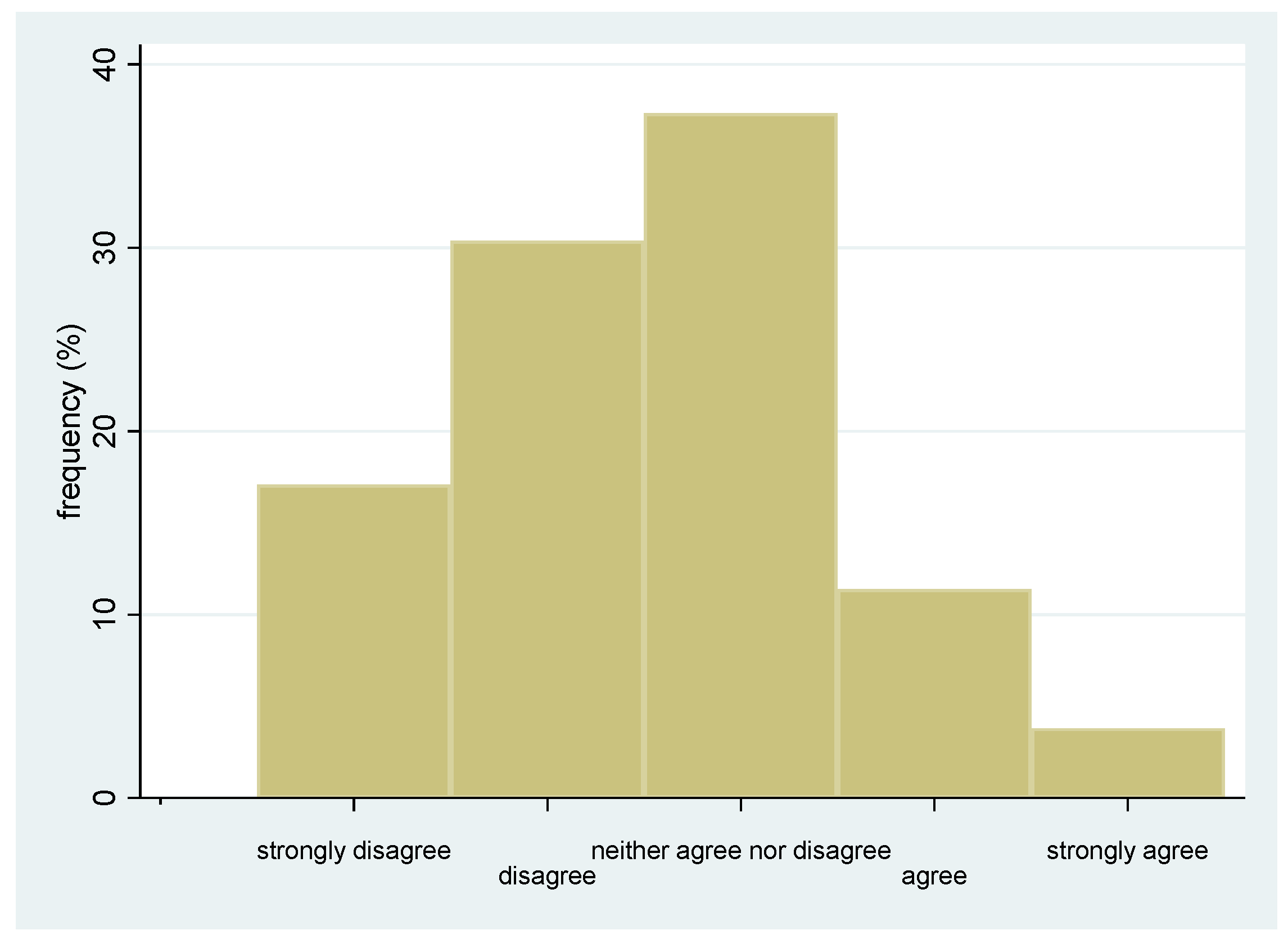
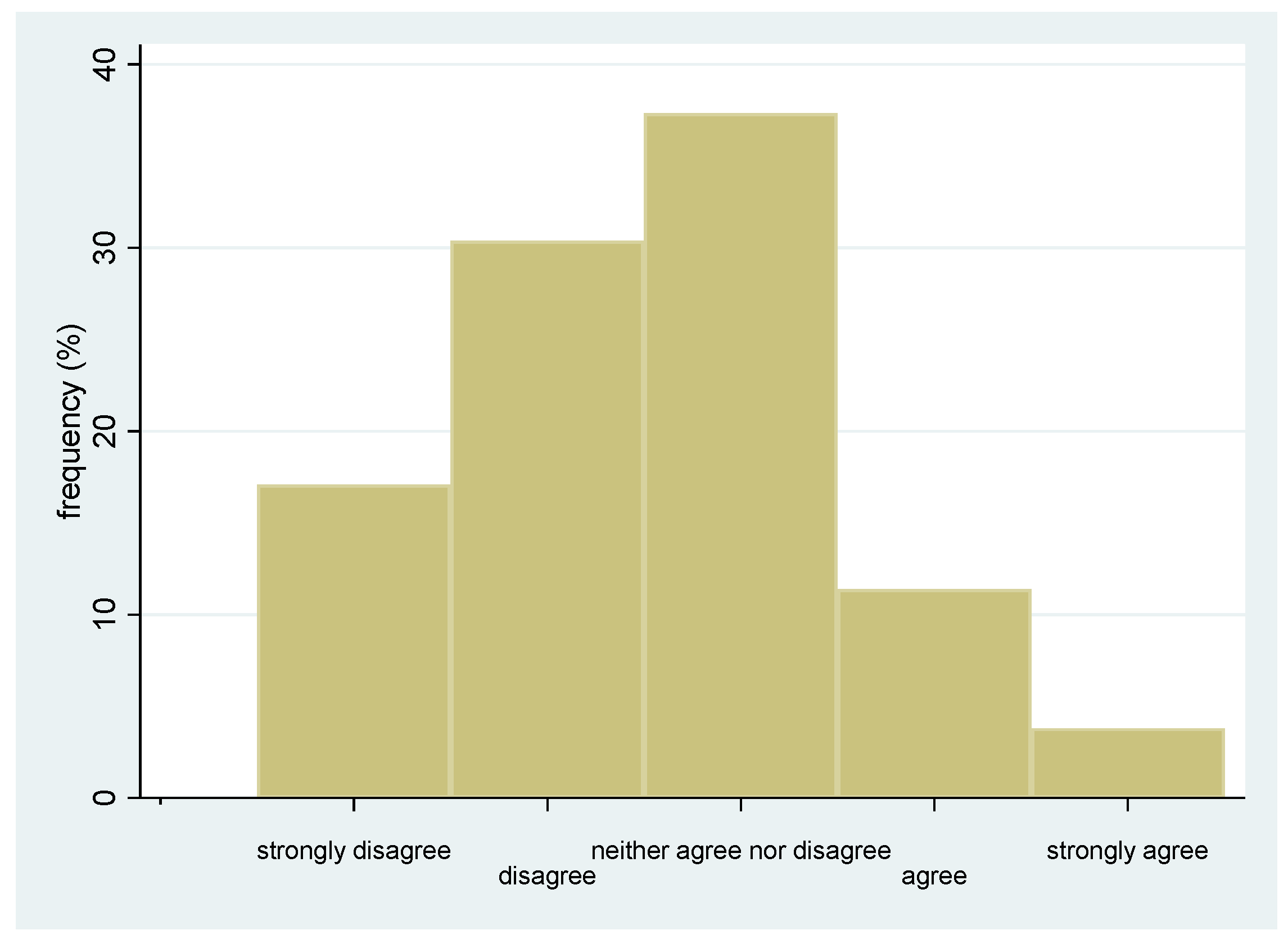
3.2. Adherence and Attitude towards Flu Vaccination
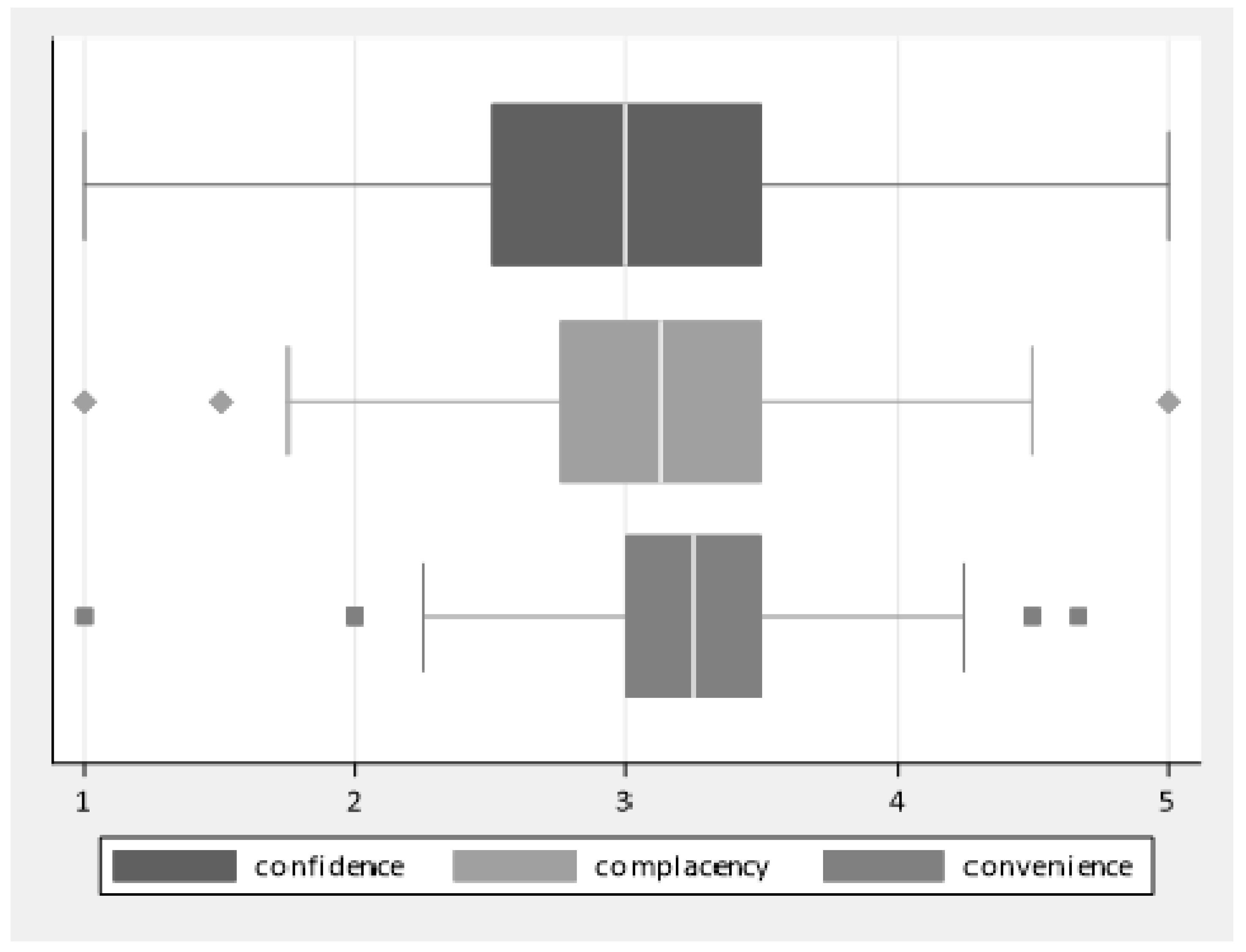
3.3. Distributions of Factors Influencing Hesitancy towards Flu Vaccination
3.4. Relationship between Potential Determinants of Hesitancy and Attitude towards Vaccination
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
| Strong Disagreement ▼ | Disagreement ▼ | Neither in Agreement, Nor in Disagreement ▼ | Agreement ▼ | Strong Agreement ▼ | |
| 1. Being vaccinated protects against influenza | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 2. The influenza vaccine is effective | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 3. It is important to protect my family against the flu by vaccinating myself | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 4. It is important to protect residents against the flu by vaccinating myself | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 5. The risk of getting influenza in NHs is very high. | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 6. Influenza is a potentially very dangerous/severe condition | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 7. I do not think that the influenza vaccination is useful | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 8. I am concerned about the adverse events of the influenza vaccine | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 9. I have been adequately informed by a doctor about the benefits of the influenza vaccination | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 10. I do not regularly get the influenza vaccination due to forgetfulness or lack of time | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 11. It would be useful to make the influenza vaccination mandatory for health professionals working in the NH | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 12. In the NH where I work, it is easy to get the influenza vaccination. | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
| 13. Staff working in the NH should get the flu vaccination each year | ☐1 | ☐2 | ☐3 | ☐4 | ☐5 |
Appendix B

{kind=link}
{kind=link}
{kind=link}
| Items | Never Vaccinated | Vaccinated at Least Once | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 1 | 2 | 3 | 4 | 5 | n | 1 | 2 | 3 | 4 | 5 | |
| Item 1. Being vaccinated protects against influenza | 129 | 13.2 | 24.8 | 45.0 | 11.6 | 5.4 | 16 | 0.0 | 0.0 | 37.5 | 43.8 | 18.8 |
| Item 2. The influenza vaccine is effective | 129 | 10.9 | 17.8 | 51.2 | 18.6 | 1.6 | 16 | 0.0 | 0.0 | 56.3 | 37.5 | 6.3 |
| Item 3. It is important to protect my family against the flu by vaccinating myself | 128 | 11.7 | 19.5 | 46.1 | 19.5 | 3.1 | 16 | 0.0 | 0.0 | 31.3 | 56.3 | 12.5 |
| Item 4. It is important to protect residents against the flu by vaccinating myself | 127 | 11.0 | 16.5 | 46.5 | 22.0 | 3.9 | 16 | 0.0 | 0.0 | 25.0 | 62.5 | 12.5 |
| Item 5. The risk of getting influenza in NHs is very high | 128 | 5.5 | 22.7 | 32.8 | 35.2 | 3.9 | 16 | 0.0 | 25.0 | 12.5 | 50.0 | 12.5 |
| Item 6. Influenza is a potentially very dangerous/severe condition | 128 | 3.9 | 14.8 | 37.5 | 39.1 | 4.7 | 16 | 0.0 | 0.0 | 56.3 | 37.5 | 6.3 |
| Item 7. I do not think that influenza vaccination is useful | 128 | 10.2 | 21.9 | 41.4 | 18.8 | 7.8 | 16 | 25.0 | 56.3 | 18.8 | 0.0 | 0.0 |
| Item 8. I am concerned about the adverse events of the influenza vaccine | 129 | 8.5 | 23.3 | 37.2 | 24.0 | 7.0 | 15 | 20.0 | 40.0 | 26.7 | 13.3 | 0.0 |
| Item 9. I have been adequately informed by a doctor about the benefits of the influenza vaccination | 129 | 8.5 | 22.5 | 27.1 | 38.0 | 3.9 | 15 | 6.7 | 6.7 | 20.0 | 60.0 | 6.7 |
| Item 10. I do not regularly get the influenza vaccination due to forgetfulness or lack of time | 124 | 33.1 | 37.1 | 20.2 | 4.8 | 4.8 | 15 | 33.3 | 33.3 | 26.7 | 6.7 | 0.0 |
| Item 11. It would be useful to make the influenza vaccination mandatory for health professionals working in the NH | 128 | 20.3 | 34.4 | 36.7 | 5.5 | 3.1 | 16 | 6.3 | 0.0 | 50.0 | 31.3 | 12.5 |
| Item 12. In the NH where I work, it is easy to get the influenza vaccination. | 129 | 40.3 | 34.9 | 18.6 | 3.1 | 3.1 | 16 | 12.5 | 12.5 | 37.5 | 31.3 | 6.3 |
| Item 13. Staff working in the NH should uptake flu vaccination each year | 129 | 3.1 | 1.6 | 17.8 | 48.8 | 28.7 | 16 | 0.0 | 0.0 | 18.8 | 43.8 | 37.5 |
References
- Czaja, C.A.; Miller, L.; Alden, N.; Wald, H.L.; Cummings, C.N.; Rolfes, M.A.; Anderson, E.J.; Bennett, N.M.; Billing, L.M.; Chai, S.J.; et al. Age-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance Network (FluSurv-NET). Open Forum Infect. Dis. 2019, 6. [Google Scholar] [CrossRef]
- Lansbury, L.E.; Brown, C.S.; Nguyen-Van-Tam, J.S. Influenza in long-term care facilities. Influenza Other Respir. Viruses 2017, 11, 356–366. [Google Scholar] [CrossRef]
- Gaillat, J.; Chidiac, C.; Fagnani, F.; Pecking, M.; Salom, M.; Veyssier, P.; Carrat, F. Morbidity and mortality associated with influenza exposure in long-term care facilities for dependant elderly people. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 1077–1086. [Google Scholar] [CrossRef]
- Jefferson, T.; Rivetti, D.; Rivetti, A.; Rudin, M.; Di Pietrantonj, C.; Demicheli, V. Efficacy and effectiveness of influenza vaccines in elderly people: A systematic review. Lancet Lond. Engl. 2005, 366, 1165–1174. [Google Scholar] [CrossRef]
- Dolan, G.P.; Harris, R.C.; Clarkson, M.; Sokal, R.; Morgan, G.; Mukaigawara, M.; Horiuchi, H.; Hale, R.; Stormont, L.; Béchard-Evans, L.; et al. Vaccination of healthcare workers to protect patients at increased risk of acute respiratory disease: Summary of a systematic review. Influenza Other Respir. Viruses 2013, 7, 93–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piano Nazionale di Prevenzione Vaccinale (Pnpv) 2017-2019. Available online: https://www.epicentro.iss.it/vaccini/PianoNazionaleVaccini (accessed on 6 February 2020).
- European Centre for Disease Prevention and Control. Seasonal Influenza Vaccination and Antiviral Use in EU/EEA Member States; Overview of vaccine recommendations for 2017–2018 and vaccination coverage rates for 2015–2016 and 2016–2017 influenza seasons; ECDC: Stockholm, Sweden, EU, 2018. [Google Scholar]
- Fortunato, F.; Tafuri, S.; Cozza, V.; Martinelli, D.; Prato, R. Low vaccination coverage among italian healthcare workers in 2013. Hum. Vaccines Immunother. 2014, 11, 133–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genovese, C.; Picerno, I.A.; Trimarchi, G.; Cannavò, G.; Egitto, G.; Cosenza, B.; Merlina, V.; Icardi, G.; Panatto, D.; Amicizia, D.; et al. Vaccination coverage in healthcare workers: A multicenter cross-sectional study in Italy. J. Prev. Med. Hyg. 2019, 60, E12–E17. [Google Scholar] [CrossRef]
- Squeri, R.; La Fauci, V.; Picerno, I.A.; Trimarchi, G.; Cannavò, G.; Egitto, G.; Cosenza, B.; Merlina, V.; Genovese, C. Evaluation of Vaccination Coverages in the Health Care Workers of a University Hospital in Southern Italy. Ann. Ig. Med. Prev. E Comunita 2019, 31, 13–24. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, M.; Valsecchi, M.; Speri, L.; Simeoni, L.; Campara, P.; Porchia, S.; Bolzonello, E.; Russo, F.; Bonavina, M.G.; Bovo, C. Increasing immunization coverage by intervening on determinants of refusal. Ann. Ig. Med. Prev. E Comunita 2012, 24, 15–20. [Google Scholar]
- Boey, L.; Bral, C.; Roelants, M.; De Schryver, A.; Godderis, L.; Hoppenbrouwers, K.; Vandermeulen, C. Attitudes, believes, determinants and organisational barriers behind the low seasonal influenza vaccination uptake in healthcare workers—A cross-sectional survey. Vaccine 2018, 36, 3351–3358. [Google Scholar] [CrossRef] [PubMed]
- Durando, P.; Alicino, C.; Dini, G.; Barberis, I.; Bagnasco, A.M.; Iudici, R.; Zanini, M.; Martini, M.; Toletone, A.; Paganino, C.; et al. Determinants of adherence to seasonal influenza vaccination among healthcare workers from an Italian region: Results from a cross-sectional study. BMJ Open 2016, 6, e010779. [Google Scholar] [CrossRef] [PubMed]
- Hauri, A.M.; Uphoff, H.; Gussmann, V.; Gawrich, S. Factors that affect influenza vaccine uptake among staff of long-term care facilities. Infect. Control Hosp. Epidemiol. 2006, 27, 638–641. [Google Scholar] [CrossRef] [PubMed]
- Kimura, A.C.; Nguyen, C.N.; Higa, J.I.; Hurwitz, E.L.; Vugia, D.J. The effectiveness of vaccine day and educational interventions on influenza vaccine coverage among health care workers at long-term care facilities. Am. J. Public Health 2007, 97, 684–690. [Google Scholar] [CrossRef] [PubMed]
- La Torre, G.; Mannocci, A.; Ursillo, P.; Bontempi, C.; Firenze, A.; Panico, M.G.; Sferrazza, A.; Ronga, C.; D’Anna, A.; Amodio, E.; et al. Prevalence of influenza vaccination among nurses and ancillary workers in Italy: Systematic review and meta analysis. Hum. Vaccin. 2011, 7, 728–733. [Google Scholar] [CrossRef] [PubMed]
- CDC. Barriers and Strategies to Improving Influenza Vaccination among Health Care Personnel|Seasonal Influenza (Flu)|CDC. 2019. Available online: https://www.cdc.gov/flu/toolkit/long-term-care/strategies.htm (accessed on 5 February 2020).
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors associated with uptake of vaccination against pandemic influenza: A systematic review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef]
- Lorenc, T.; Marshall, D.; Wright, K.; Sutcliffe, K.; Sowden, A. Seasonal influenza vaccination of healthcare workers: Systematic review of qualitative evidence. BMC Health Serv. Res. 2017, 17, 732. [Google Scholar] [CrossRef] [Green Version]
- Pless, A.; McLennan, S.R.; Nicca, D.; Shaw, D.M.; Elger, B.S. Reasons why nurses decline influenza vaccination: A qualitative study. BMC Nurs. 2017, 16, 20. [Google Scholar] [CrossRef] [Green Version]
- Prematunge, C.; Corace, K.; McCarthy, A.; Nair, R.C.; Pugsley, R.; Garber, G. Factors influencing pandemic influenza vaccination of healthcare workers—A systematic review. Vaccine 2012, 30, 4733–4743. [Google Scholar] [CrossRef]
- Desiante, F.; Caputi, G.; Cipriani, R. Assessment of coverage and analysis of the determinants of adherence to influenza vaccination in the general practitioners of Taranto. Ann. Ig. Med. Prev. E Comunita 2017, 29, 256–263. [Google Scholar] [CrossRef]
- Petek, D.; Kamnik-Jug, K. Motivators and barriers to vaccination of health professionals against seasonal influenza in primary healthcare. BMC Health Serv. Res. 2018, 18, 853. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.-L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. Cowling, B.J., Ed. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef] [PubMed]
- Darvishian, M.; Bijlsma, M.J.; Hak, E.; van den Heuvel, E.R. Effectiveness of seasonal influenza vaccine in community-dwelling elderly people: A meta-analysis of test-negative design case-control studies. Lancet Infect. Dis. 2014, 14, 1228–1239. [Google Scholar] [CrossRef]
- Haugh, M.; Gresset-Bourgeois, V.; Macabeo, B.; Woods, A.; Samson, S.I. A trivalent, inactivated influenza vaccine (Vaxigrip®): Summary of almost 50 years of experience and more than 1.8 billion doses distributed in over 120 countries. Expert Rev. Vaccines 2017, 16, 545–564. [Google Scholar] [CrossRef]
- AIFA Dispone il Divieto di Utilizzo per due Lotti del Vaccino Antinfluenzale FLUAD|AIFA Agenzia Italiana del Farmaco. Available online: http://www.agenziafarmaco.gov.it/content/aifa-dispone-il-divieto-di-utilizzo-due-lotti-del-vaccino-antinfluenzale-fluad-0 (accessed on 5 February 2020).
- European Medicines Agency. No Evidence that Fluad Vaccine Caused Deaths in Italy. Available online: http://www.ema.europa.eu/ema/index.jsp?curl=pages/news_and_events/news/2014/12/news_detail_002228.jsp&mid=WC0b01ac058004d5c1 (accessed on 3 January 2020).
- Dunning, J. Potential adverse effects of negative publicity surrounding antivirals for influenza. BMJ 2014, 348, g3015. [Google Scholar] [CrossRef] [Green Version]
- Signorelli, C.; Odone, A.; Conversano, M.; Bonanni, P. Deaths after Fluad flu vaccine and the epidemic of panic in Italy. BMJ 2015, 350, h116. [Google Scholar] [CrossRef]
- Al-Haddad, M.S.; Abdallah, Q.M.; Alhamyani, A.H.; Althomali, A.J.; Alshakhshir, S.M. General public knowledge and practices about the common cold. J. Taibah Univ. Med. Sci. 2016, 11, 104–109. [Google Scholar] [CrossRef] [Green Version]
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet Lond. Engl. 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- O’Connor, L.; Murphy, H.; Montague, E.; Boland, M. Epidemiology and Management of Seasonal Influenza Outbreaks in Long-term Care Facilities in the Health Service Executive East Area of Ireland during the 2013-2014 Influenza Season. J. Immun. 2017, 1, 22. [Google Scholar] [CrossRef] [Green Version]
- Strausbaugh, L.J.; Sukumar, S.R.; Joseph, C.L. Infectious disease outbreaks in nursing homes: An unappreciated hazard for frail elderly persons. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2003, 36, 870–876. [Google Scholar] [CrossRef]
- Thomas, R.E.; Jefferson, T.; Lasserson, T.J. Influenza vaccination for healthcare workers who care for people aged 60 or older living in long-term care institutions. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Lindley, M.C.; Allred, N.; Weinbaum, C.M.; Grohskopf, L. Effect of Influenza Vaccination of Healthcare Personnel on Morbidity and Mortality Among Patients: Systematic Review and Grading of Evidence. Clin. Infect. Dis. 2014, 58, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recommendations on Influenza Vaccination during the 2019–2020 Winter Season (2019). Available online: http://www.euro.who.int/en/health-topics/communicable-diseases/influenza/publications/2019/recommendations-on-influenza-vaccination-during-the-20192020-winter-season-2019 (accessed on 6 February 2020).
- Recommended Vaccines for Healthcare Workers|CDC. Available online: https://www.cdc.gov/vaccines/adults/rec-vac/hcw.html (accessed on 5 February 2020).
- Feemster, K.A.; Prasad, P.; Smith, M.J.; Feudtner, C.; Caplan, A.; Offit, P.; Coffin, S.E. Employee designation and health care worker support of an influenza vaccine mandate at a large pediatric tertiary care hospital. Vaccine 2011, 29, 1762–1769. [Google Scholar] [CrossRef] [PubMed]
- Chean, R.; Ferguson, J.K.; Stuart, R.L. Mandatory seasonal influenza vaccination of health care workers: A way forward to improving influenza vaccination rates. Healthc. Infect. 2014, 19, 42–44. [Google Scholar] [CrossRef]
- Pitts, S.I.; Maruthur, N.M.; Millar, K.R.; Perl, T.M.; Segal, J. A systematic review of mandatory influenza vaccination in healthcare personnel. Am. J. Prev. Med. 2014, 47, 330–340. [Google Scholar] [CrossRef]
- Rakita, R.M.; Hagar, B.A.; Crome, P.; Lammert, J.K. Mandatory influenza vaccination of healthcare workers: A 5-year study. Infect. Control Hosp. Epidemiol. 2010, 31, 881–888. [Google Scholar] [CrossRef]
- Betsch, C.; Böhm, R. Detrimental effects of introducing partial compulsory vaccination: Experimental evidence. Eur. J. Public Health 2016, 26, 378–381. [Google Scholar] [CrossRef] [Green Version]
- Finch, M. Point: Mandatory influenza vaccination for all heath care workers? Seven reasons to say “no.”. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2006, 42, 1141–1143. [Google Scholar] [CrossRef] [Green Version]


| Staff Position | Respondents | RR * |
|---|---|---|
| Staff managers/Leadership—Administrator, Medical Director, Director of Nursing | 5 (3.0%) | 33.3% (5/15) |
| Direct care staff—Physicians 1, Healthcare Assistants, Healthcare Technicians, physical therapists | 88 (53.0%) | 34.7% (88/254) |
| Nurses | 31 (18.7%) | 64.6% (32/48) |
| Other healthcare providers—Occupational/Speech/Respiratory therapists, dieticians/nutritionists, animators, Social Worker, Psychologist | 18 (10.8%) | 78.3% (18/23) |
| Administrative staff | 9 (5.4%) | 42.9% (9/21) |
| Support staff—Food Service/Dietary, Housekeeping, Laundry Service, Maintenance | 8 (4.8%) | 10.5% (8/76) |
| Missing | 7 (4.2%) |
| Latent Factors | Items | n | Score (%) 1 | ||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||
| Confidence | Being vaccinated protects against flu (Item 1) | 155 | 11.6 | 21.9 | 43.2 | 17.4 | 5.8 |
| The flu vaccine is effective (Item 2) | 155 | 9.7 | 15.5 | 50.3 | 22.6 | 1.9 | |
| I don’t think flu vaccination is useful (Item 7) | 153 | 12.4 | 24.8 | 37.9 | 18.3 | 6.5 | |
| I’m concerned about the adverse events of the influenza vaccine (Item 8) | 153 | 9.2 | 24.8 | 35.3 | 24.2 | 6.5 | |
| Complacency | It is important to protect my family against the flu by vaccinating myself (Item 3) | 153 | 10.5 | 17.6 | 44.4 | 23.5 | 3.9 |
| It is important to protect residents against the flu by vaccinating myself (Item 4) | 151 | 9.9 | 15.2 | 44.4 | 25.8 | 4.6 | |
| The risk of getting the flu is very high in the nursing home setting (Item 5) | 153 | 5.2 | 22.9 | 30.7 | 36.6 | 4.6 | |
| The flu disease is a potentially very severe/dangerous condition (Item 6) | 153 | 4.6 | 13.7 | 39.9 | 37.2 | 4.6 | |
| Convenience | I have been adequately informed by a physician about the benefits of the influenza vaccination (Item 9) | 153 | 7.8 | 21.6 | 26.8 | 39.9 | 3.9 |
| I do not regularly get the influenza vaccination due to forgetfulness or lack of time (Item 10) | 148 | 31.8 | 36.5 | 22.3 | 5.4 | 4.0 | |
| It would be useful to make the influenza vaccination mandatory for health professionals working in NHs (Item 11) | 153 | 35.9 | 31.4 | 21.6 | 7.8 | 3.3 | |
| In the NH where I work, it is easy to get the influenza vaccination (Item 12) | 154 | 2.6 | 1.9 | 18.8 | 48.7 | 27.9 | |
| Predictors | Simple Regressions | Multiple Regression | ||||
|---|---|---|---|---|---|---|
| Beta | p-Value | 95% CI | Beta | p-Value | 95% CI Beta | |
| Being advised by a physician (Q2) | −0.16 | 0.36 | −0.50; −0.18 | |||
| Working with residents (Q3) | −0.38 | 0.14 | −0.87; 0.12 | |||
| Complacency | 0.86 | <0.01 | 0.68; 1.04 | 0.60 | <0.01 | 0.36; 0.84 |
| Confidence | 0.67 | <0.01 | 0.49; 0.85 | 0.25 | 0.02 | 0.03; 0.46 |
| Convenience | 0.76 | <0.01 | 0.45; 1.06 | 0.38 | <0.01 | 0.11; 0.65 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moretti, F.; Visentin, D.; Bovolenta, E.; Rimondini, M.; Majori, S.; Mazzi, M.; Poli, A.; Tardivo, S.; Torri, E. Attitudes of Nursing Home Staff towards Influenza Vaccination: Opinions and Factors Influencing Hesitancy. Int. J. Environ. Res. Public Health 2020, 17, 1851. https://doi.org/10.3390/ijerph17061851
Moretti F, Visentin D, Bovolenta E, Rimondini M, Majori S, Mazzi M, Poli A, Tardivo S, Torri E. Attitudes of Nursing Home Staff towards Influenza Vaccination: Opinions and Factors Influencing Hesitancy. International Journal of Environmental Research and Public Health. 2020; 17(6):1851. https://doi.org/10.3390/ijerph17061851
Chicago/Turabian StyleMoretti, Francesca, Donatella Visentin, Elena Bovolenta, Michela Rimondini, Silvia Majori, Mariangela Mazzi, Albino Poli, Stefano Tardivo, and Emanuele Torri. 2020. "Attitudes of Nursing Home Staff towards Influenza Vaccination: Opinions and Factors Influencing Hesitancy" International Journal of Environmental Research and Public Health 17, no. 6: 1851. https://doi.org/10.3390/ijerph17061851
APA StyleMoretti, F., Visentin, D., Bovolenta, E., Rimondini, M., Majori, S., Mazzi, M., Poli, A., Tardivo, S., & Torri, E. (2020). Attitudes of Nursing Home Staff towards Influenza Vaccination: Opinions and Factors Influencing Hesitancy. International Journal of Environmental Research and Public Health, 17(6), 1851. https://doi.org/10.3390/ijerph17061851