Incidence and Predictors of Cognitive Frailty Among Older Adults: A Community-based Longitudinal Study

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
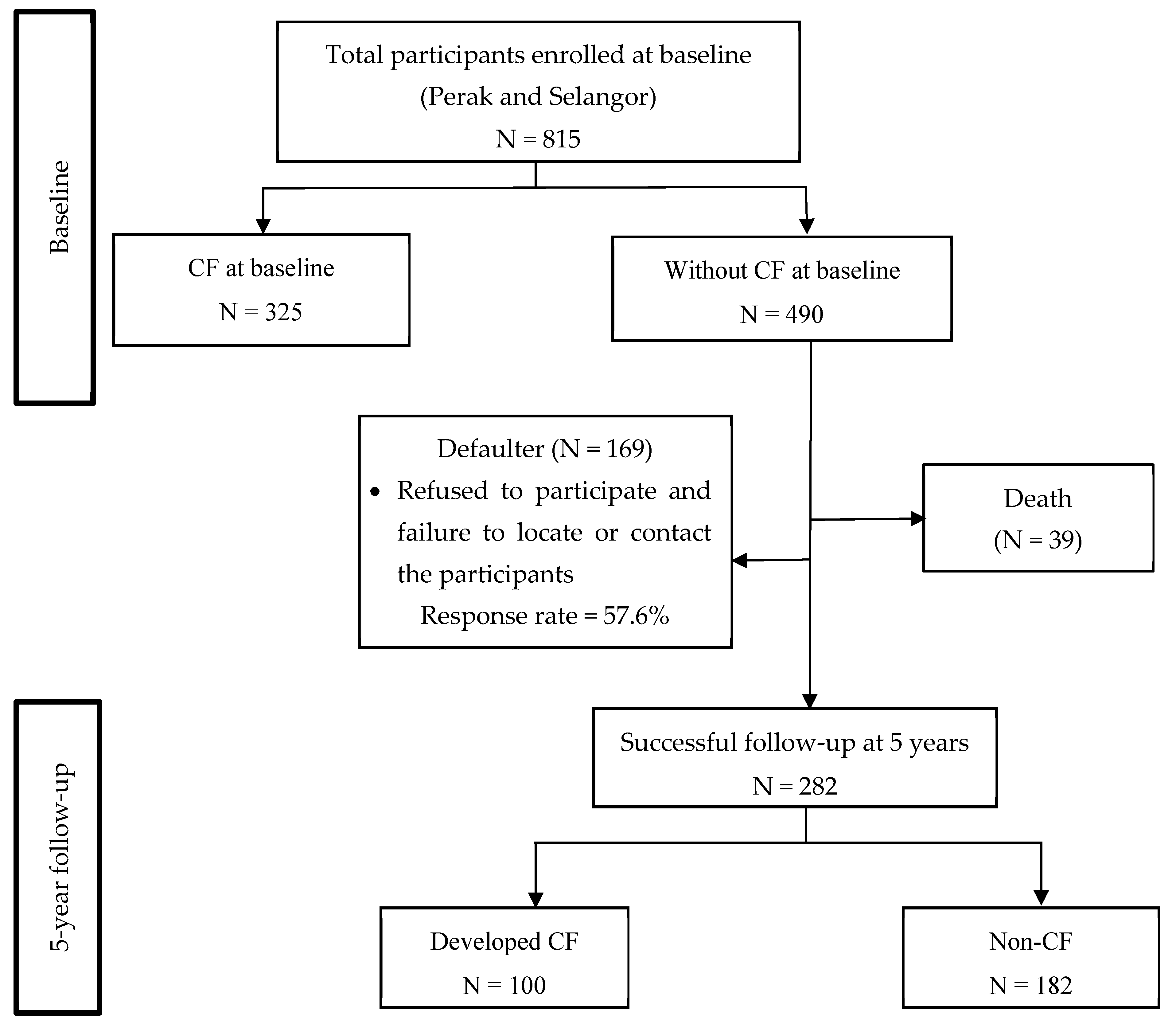
3.1. Data Collection
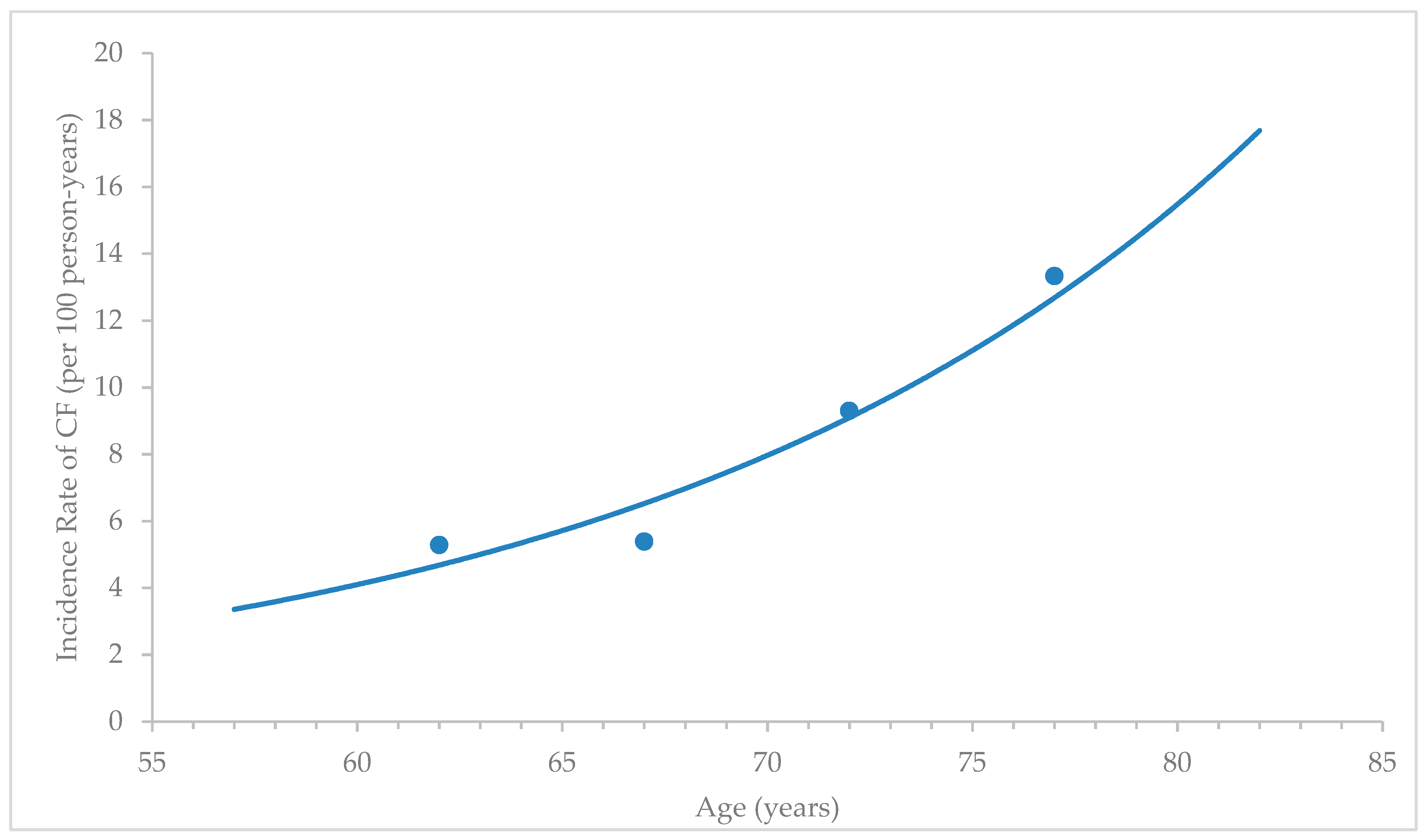
3.2. Incidence and Operational Definition of Cognitive Frailty
- Shrinking, subjective report of unintentional loss of weight around 5 kg in the prior year (i.e., not due to diet or exercise).
- Self-report of exhaustion and poor endurance and energy, defined by using two items of the Center for Epidemiologic Studies Depression scale (CES-D): (a) I felt that everything I did was an effort; and (b) I could not get going; (the question was how often in the last week did you feel like this (rare = 0, some or little time (1–2 days) = 1, moderate (3–4 days) = 2, and most of the times = 3). Participants who scored two and above were categorised as frail based on this exhaustion criteria.
- For the low physical activity, a low physical activity was assessed using the Physical Activity Scale for Elderly (PASE), and a low physical activity was identified by low scores (in the lowest tertile) of the PASE score.
- Slowness was defined using the five-meter gait speed test with the cut-off points stated in the original reference adjusted for the gender and height.
- The last criterion was weakness. It was defined using a hand grip strength test with the cut-off points stated in the original reference adjusted for the gender and body mass index.
3.3. Possible Predictors of Cognitive Frailty:
3.3.1. Socio-demographic Data and Health Condition
3.3.2. Nutritional Status, Body Composition, and Blood Pressure
3.3.3. Cognitive Function Test
3.3.4. Physical Fitness and Functional Status
3.3.5. Psychosocial
3.3.6. Dietary Intake
3.3.7. Biochemical Analysis
3.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Öhman, H.; Savikko, N.; Strandberg, T.E.; Pitkälä, K.H. Effect of Physical Exercise on Cognitive Performance in Older Adults with Mild Cognitive Impairment or Dementia: A Systematic Review. Dement. Geriatr. Cogn. Disord. 2014, 38, 347–365. [Google Scholar] [CrossRef]
- Mehta, D.; Jackson, R.; Paul, G.; Shi, J.; Sabbagh, M. Why do trials for Alzheimer’s disease drugs keep failing? A discontinued drug perspective for 2010-2015. Expert Opin. Investig. Drugs 2017, 26, 735–739. [Google Scholar] [CrossRef]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; van Kan, G.A.; Ousset, P.J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (I.A.N.A./I.A.G.G.) International consensus group. J. Nutr. Health Aging 2013, 17, 1–9. [Google Scholar] [CrossRef]
- Shimada, H.; Doi, T.; Lee, S.; Makizako, H.; Chen, L.; Id, H.A. Cognitive Frailty Predicts Incident Dementia among Community-Dwelling Older People. J. Clin. Med. 2018, 7, 250. [Google Scholar] [CrossRef] [Green Version]
- Ng, P.T.; Feng, L.; Shwe, M.; Nyunt, Z.; Larbi, A. Frailty in Older Persons: Multisystem Risk Factors and the Frailty Risk Index (FRI). J. Am. Med. Dir. Assoc. 2014, 15, 635–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteban-cornejo, I.; Cabanas-sánchez, V.; Rodriguez-artalejo, F.; Martinez-gomez, D. Cognitive Frailty and Mortality in a National Cohort of Older Adults: The Role of Physical Activity. Mayo Clin. Proc. 2019, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Grande, G.; Haaksma, M.L.; Rizzuto, D.; Melis, R.J.F.; Marengoni, A.; Onder, G.; Vetrano, D.L. Co-occurrence of cognitive impairment and physical frailty, and incidence of dementia: Systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2019, 107, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Shwe, M.; Nyunt, Z.; Gao, Q.; Feng, L.; Lee, T.S.; Tsoi, T.; Chong, M.S.; Lim, W.S.; Collinson, S.; et al. Physical Frailty, Cognitive Impairment, and the Risk of Neurocognitive Disorder in the Singapore Longitudinal Ageing Studies. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 369–375. [Google Scholar] [CrossRef] [Green Version]
- Rosano, C.; Studenski, S.A.; Aizenstein, H.J.; Boudreau, R.M.; Longstreth, W.T., Jr.; Newman, A.B. Slower gait, slower information processing and smaller prefrontal area in older adults. Age Ageing 2012, 41, 58–64. [Google Scholar] [CrossRef] [Green Version]
- Welmer, A.K.; Rizzuto, D.; Qiu, C.; Caracciolo, B.; Laukka, E.J. Walking Speed, Processing Speed, and Dementia: A Population-Based Longitudinal Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, 1503–1510. [Google Scholar] [CrossRef] [Green Version]
- Franceschi, C.; Campisi, J. Chronic Inflammation (Inflammaging) and Its Potential Contribution to Age-Associated Diseases. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69 (Suppl. 1), S4–S9. [Google Scholar] [CrossRef]
- Ferrucci, L.; Fabbri, E. Inflammageing: Chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 2018, 15, 505–522. [Google Scholar] [CrossRef] [PubMed]
- Qiu, C.; Fratiglioni, L. A major role for cardiovascular burden in age-related cognitive decline. Nat. Rev. Cardiol. 2015, 12, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Haaksma, M.L.; Vilela, L.R.; Marengoni, A.; Calderón-Larrañaga, A.; Leoutsakos, J.-M.S.; Olde Rikkert, M.G.M.; Melis, R.J.F. Comorbidity and progression of late onset Alzheimer’s disease: A systematic review. PLoS ONE 2017, 12, e0177044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sargent, L.; Nalls, M.; Starkweather, A.; Hobgood, S.; Thompson, H.; Amella, E.J.; Singleton, A. Shared biological pathways for frailty and cognitive impairment: A systematic review. Ageing Res. Rev. 2018, 47, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Ruan, Q.; D’Onofrio, G.; Greco, A. From Sarcopenia to Frailty: The Pathophysiological Basis and Potential Target Molecules of Intervention. Frailty Sarcopenia Onset Dev. Clin. Chall. 2017, 3, 55–69. [Google Scholar] [CrossRef] [Green Version]
- Davies, B.; García, F.; Ara, I.; Artalejo, F.R.; Rodriguez-Mañas, L.; Walter, S. Relationship Between Sarcopenia and Frailty in the Toledo Study of Healthy Aging: A Population Based Cross-Sectional Study. J. Am. Med. Dir. Assoc. 2018, 19, 282–286. [Google Scholar] [CrossRef]
- Rivan, N.F.M.; Shahar, S.; Rajab, N.F.; Kaur, D.; Singh, A.; Din, N.C.; Hazlina, M.; Aizan, T.; Abdul, T. Cognitive Frailty among Malaysian Older Adults: Baseline Findings from the LRGS TUA Cohort Study. Clin. Interv. Aging 2019, 14, 1343–1352. [Google Scholar] [CrossRef] [Green Version]
- Roppolo, M.; Mulasso, A.; Rabaglietti, E. Cognitive frailty in Italian community-dwelling older adults: Prevalence rate and its association with disability. J. Nutr. Health Aging 2016, 5, 1–6. [Google Scholar] [CrossRef]
- Noordzij, M.; Dekker, W.; Zoccali, C.; Jager, J. Measures of Disease Frequency: Prevalence and incidence. Nephron Clin. Pract. 2010, 115, 17–20. [Google Scholar] [CrossRef]
- Shahar, S.; Omar, A.; Vanoh, D.; Aizan, T. Approaches in Methodology for Population-Based Longitudinal Study on Neuroprotective Model for Healthy Longevity (TUA) among Malaysian Older Adults. Aging Clin. Exp. Res. 2015, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Caracciolo, B.; Brayne, C.; Gauthier, S.; Jelic, V.; Fratiglioni, L. Mild Cognitive Impairment: A Concept in Evolution. J. Intern. Med. 2014, 275, 214–228. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.K.; Shahar, S.; Chin, A.; Aini, N.; Yusoff, M.; Rajab, N.; Abdul, S. Prevalence of Gender Disparities and Predictors Affecting the Occurrence of Mild Cognitive Impairment (MCI). Arch. Gerontol. Geriatr. 2012, 54, 185–191. [Google Scholar] [CrossRef]
- Ibrahim, N.M.; Shohaimi, S.; Chong, H.T.; Abdul Rahman, A.H.; Razali, R.; Esther, E.; Basri, H.B. Validation Study of the Mini-Mental State Examination in a Malay-Speaking Elderly Population in Malaysia. Dement. Geriatr. Cogn. Disord. 2009, 247–253. [Google Scholar] [CrossRef]
- Parkinson, C. Smoking Beliefs and Behavior Among Youth in Malaysia and Thailand. Am. J. Health Behav. 2009, 33, 366–375. [Google Scholar] [CrossRef] [Green Version]
- Mutalip, M.H.B.A.; Kamarudin, R.B.; Manickam, M.; Abd Hamid, H.A.B.; Saari, R.B. Alcohol Consumption and Risky Drinking Patterns in Malaysia: Findings from NHMS 2011. Alcohol Alcohol. 2014, 49, 593–599. [Google Scholar] [CrossRef] [Green Version]
- Simpson, C.F.; Boyd, C.M.; Carlson, M.C.; Griswold, M.E.; Guralnik, J.M.; Fried, L.P. Agreement between self-report of disease diagnoses and medical record validation in disabled older women: Factors that modify agreement. J. Am. Geriat. Soc. 2004, 53, 123–127. [Google Scholar] [CrossRef]
- Razali, R.; Jean-li, L.; Jaffar, A.; Ahmad, M.; Azhar, S.; Midin, M.; Sidi, H.; Ahmad, S. ScienceDirect Is the Bahasa Malaysia Version of the Montreal Cognitive Assessment (MoCA-BM) a Better Instrument than the Malay Version of the Mini Mental State Examination (M-MMSE) in Screening for Mild Cognitive Impairment (MCI) in the Elderly? Compr. Psychiatry 2014, 55, S70–S75. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Adult Intelligence Scale-III; The Psychological Corporation: San Antonio, TX, USA, 1994. [Google Scholar]
- Strauss, E.; Sherman, E.M.; Spreen, O. A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary; Ocford University: New York, NY, USA, 2006; pp. 1–3. [Google Scholar]
- Jones, C.J.; Rikli, R.E. Measuring Functional Fitness in Older Adults. J. Act. Aging 2002, 1, 24–30. [Google Scholar]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged, the index of ADL: A standardized measure of biological and psychosocial function. J. Am. Geriatr. Soc. 1963, 37, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Graf, C. The Lawton instrumental activities of daily living scale. Am. J. Nurs. 2008, 108, 52–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teh, E.E.; Hasanah, C.I. Validation of Malay Version of Geriatric Depression Scale among Elderly Inpatients. Penang Hospital and School of Medical Sciences, Universiti Sains Malaysia. September 2004. Available online: http://priory.com/psych/MalayGDS.html (accessed on 20 November 2019).
- Andrews, G.; Kemp, A.; Sunderland, M.; Korff, M.; Von Ustun, T.B. Normative Data for the 12 Item WHO Disability Assessment Schedule 2.0. PLoS ONE 2009, 4, e8343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahar, S.; Earland, J.; Rahman, S.A. Validation of a Dietary History Questionnaire against a 7-D Weighed Record for Estimating Nutrient Intake among Rural Elderly Malays. Mal. J. Nutr. 2000, 6, 33–44. [Google Scholar]
- Hussin, N.M.; Shahar, S.; Yahya, H.M.; Din, N.C.; Kaur, D.; Singh, A. Incidence and predictors of mild cognitive impairment (MCI) within a multi-ethnic Asian populace: A community-based longitudinal study. BMC Public Health 2019, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Serra-Prat, M.; Papiol, M.; Vico, J.; Palomera, E.; Arús, M.; Cabré, M. Incidence and Risk Factors for Frailty in the Community-Dwelling Elderly Population. A Two-year Follow-Up Cohort Study. J. Gerontol. Geriatr. Res 2017, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Corrada, M.M.; Brookmeyer, R.; Paganini-Hill, A.; Berlau, D.; Kawas, C.H. Dementia incidence continues to increase with age in the oldest old: The 90+ study. Ann. Neurol. 2010, 67, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Shimada, H.; Makizako, H.; Tsutsumimoto, K.; Doi, T.; Lee, S.; Suzuki, T. Cognitive Frailty and Incidence of Dementia in Older Persons. Alzheimer’s Dement. 2017, 13, P1182. [Google Scholar] [CrossRef]
- Shankar, A.; Mcmunn, A.; Demakakos, P.; Hamer, M.; Steptoe, A.; Shankar, A.; Hamer, M.; Steptoe, A. Health Psychology Social Isolation and Loneliness: Prospective Associations with Functional Status in Older Adults. Health Psychol. 2016, 36, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Boulos, C.; Salameh, P.; Barberger-gateau, P. Social Isolation and Risk for Malnutrition among Older People. Geriatr. Gerontol. Int. 2016, 1–9. [Google Scholar] [CrossRef]
- Shimada, H.; Makizako, H.; Lee, S.; Doi, T.; Lee, S.; Tsutsumimoto, K.; Suzuki, T. Impact of cognitive frailty on daily activities in older persons. J. Nutr. Health Aging 2016, 20, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Lozupone, M.; Solfrizzi, V.; Sardone, R.; Dibello, V.; Di Lena, L.; Logroscino, G. Different Cognitive Frailty Models and Health- and Cognitive-related Outcomes in Older Age: From Epidemiology to Prevention. J. Alzheimer’s Dis. 2018, 62, 993–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, M.Y.; Levine, D.A.; Zahodne, L.B.; Kabeto, M.U.; Langa, K.M. Multimorbidity and Cognitive Decline Over 14 Years in Older Americans. J. Gerontol. Ser. A. 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Weiss, C.O. Frailty and Chronic Diseases in Older Adults. Clin. Geriatr. Med. 2011, 27, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Cognitive Impairment. Available online: https://www.cdc.gov/aging/pdf/cognitive_impairment/cogimp_poilicy_final.pdf (accessed on 27 December 2019).
- Fougère, B.; Daumas, M.; Lilamand, M.; Sourdet, S.; Delrieu, J.; Vellas, B. Association Between Frailty and Cognitive Impairment: Cross-Sectional Data From Toulouse Frailty Day Hospital. J. Am. Med. Dir. Assoc. 2017, 1–5. [Google Scholar] [CrossRef]
- Robertson, D.A.; Savva, G.M.; Anne, R. Frailty and Cognitive Impairment—A Review of the Evidence and Causal Mechanisms. Ageing Res. Rev. 2013, 12, 840–851. [Google Scholar] [CrossRef]
- Thein, F.S.; Li, Y.; Shwe, M.; Nyunt, Z.; Gao, Q.; Wee, S.L. Physical Frailty and Cognitive Impairment Is Associated with Diabetes and Adversely Impact Functional Status and Mortality. Postgrad. Med. 2018, 130, 561–567. [Google Scholar] [CrossRef]
- Arts, M.H.L.; Collard, R.M.; Comijs, H.C.; Zuidersma, M.; Rooij, S.E.; De Naarding, P.; Voshaar, R.C.O. Physical Frailty and Cognitive Functioning in Depressed Older Adults: Findings from the NESDO Study. J. Am. Med. Dir. Assoc. 2015. [Google Scholar] [CrossRef]
- Zivin, K.; Wharton, T.; Rostant, O. The economic, public health, and caregiver burden of late-life depression. Psychiatr. Clin. Na 2013, 36, 631–649. [Google Scholar] [CrossRef] [Green Version]
- Soysal, A.P.; Veronese, N.; Thompson, T.; Kahl, K.G.; Fernandes, B.S.; Prina, A.M.; Scho, P.; Koyanagi, A.; Tseng, P.; Lin, P.; et al. Relationship between Depression and Frailty in Older Adults: A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2017, 1–34. [Google Scholar] [CrossRef]
- Savva, G.M.; Donoghue, O.A.; Horgan, F.; Regan, C.O.; Cronin, H.; Kenny, R.A. Using Timed Up-and-Go to Identify Frail Members of the Older Population. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Kaur, D.; Singh, A.; Shahar, S. “Timed Up and Go” Test: Age, Gender and Cognitive Impairment Stratified Normative Values of Older Adults. PLoS ONE 2017, 12, e0185641. [Google Scholar] [CrossRef]
- Lee, J.E.; Shin, D.W.; Jeong, S.; Son, K.Y.; Cho, B.; Yoon, J.L.; Park, B.J.; Kwon, I.S.; Lee, J.; Kim, S. Association Between Timed Up and Go Test and Future Dementia Onset. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1238–1243. [Google Scholar] [CrossRef] [PubMed]
- Sunderaraman, P.; Maidan, I.; Kozlovski, T.; Apa, Z.; Mirelman, A. Differential Associations Between Distinct Components of Cognitive Function and Mobility: Implications for Understanding Aging, Turning and Dual-Task Walking. Front. Aging Neurosci. 2019, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.L.; Blizzard, L.; Wood, A.G.; Srikanth, V.; Thomson, R.; Sanders, L.M.; Callisaya, M.L. Cognitive Function, Gait, and Gait Variability in Older People: A Population-Based Study. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Jie, Z.; Socsci, K.B.; Yin, E.; Khoo, H.; Koo, E.H.; Merchant, R.A. The Utility of Brief Cognitive Tests for Patients With Type 2 Diabetes Mellitus: A Systematic Review. J. Am. Med. Dir. Assoc. 2016. [Google Scholar] [CrossRef]
- Jaeger, J. Digit Symbol Substitution Test The Case for Sensitivity Over Specificity in Neuropsychological Testing. J. Clin. Psychopharmacol. 2018, 38, 513–519. [Google Scholar] [CrossRef]
- Robertson, D.A.; Savva, G.M.; Coen, R.F.; Kenny, R.-A. Cognitive Function in the Prefrailty and Frailty Syndrome. J. Am. Geriatr. Soc. 2014, 62, 2118–2124. [Google Scholar] [CrossRef]
- Recommended Nutrient Intake. A Report of the Technical Working Group on Nutritional Guidelines; Ministry of Health Malaysia: Putrajaya, Malaysia, 2017.
- Lapid, M.; Takahashi, P.; Cha, S. Vitamin D and depression in geriatric primary care patients. Clin. Interv. Aging 2013, 8, 509–514. [Google Scholar] [CrossRef] [Green Version]
- Gunton, J.E.; Girgis, C.M.; Baldock, P.A.; Lips, P. Bone Muscle Interactions and Vitamin, D. Bone 2015, 1–6. [Google Scholar] [CrossRef]
- Halil, M.; Kizilarslanoglu, M.C.; Kuyumcu, M.E.; Yesil, Y.; Jentoft, A.J.C. Cognitive Aspects of Frailty: Mechanisms Behind The Link Between Frailty and Cognitive Impairment. J. Nutr. Health Aging 2014, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mason, C.; Xiao, L.; Imayama, I.; Duggan, C.R.; Foster-schubert, K.E.; Kong, A.; Campbell, K.L.; Wang, C.; Villasenor, A.; Neuhouser, M.L.; et al. On Sarcopenia in Postmenopausal Women. Clin. Sci. 2013, 607–614. [Google Scholar] [CrossRef] [Green Version]
- Lau, H.; Fitri, A.; Ludin, M.; Rajab, N.F.; Shahar, S. Identification of Neuroprotective Factors Associated with Successful Ageing and Risk of Cognitive Impairment among Malaysia Older Adults. Curr. Gerontol. Geriatr. Res. 2017, 2017, 4218756. [Google Scholar] [CrossRef] [Green Version]
- Brouwer-brolsma, E.M.; Rest, O.; Van De Tieland, M.; Zwaluw, N.L.; Van Der Steegenga, W.T.; Adam, J.J.; Loon, L.J.C.; Van Feskens, E.J.M.; Groot, L.C. Serum 25-Hydroxyvitamin D Is Associated With Cognitive Executive Function in Dutch Prefrail and Frail Elderly: A Cross-Sectional Study Exploring the Associations of 25-Hydroxyvitamin D With Glucose Metabolism, Cognitive Performance and Depression. J. Am. Med. Dir. Assoc. 2013, 14, e9–e17. [Google Scholar] [CrossRef] [PubMed]
- Borges, M.K.; Canevelli, M.; Cesari, M.; Aprahamian, I. Frailty as a Predictor of Cognitive Disorders: A Systematic Review and Data Source and Search Strategy. Front. Med. 2019, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkins, C.H.; Roe, C.M.; Morris, J.C.; Galvin, J.E. Of Dementia of the Alzheimer’S Type. Clin. Investig. 2013, 1055–1059. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliff, S.; Rikkert, M.O.; Rockwood, K. Frailty in Elderly People. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Haslbeck, J.W.; McCorkle, R.; Schaeffer, D. Chronic Illness Self-Management While Living Alone in Later Life. Res. Aging 2012, 34, 507–547. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Parameters | N = 694 | p-Value | |
|---|---|---|---|
| Dropout (n = 169) | Non-Dropout (n = 282) | ||
| Age, mean ± sd | 68.19 ± 5.79 | 67.00 ± 4.98 | 0.020 |
| Gender: | |||
| Male | 77 (45.8%) | 126 (44.7%) | 0.707 |
| Female | 92 (54.2%) | 156 (55.3%) | |
| Ethnic: | |||
| Malay | 60 (35.5%) | 120 (43.3%) | 0.056 |
| Chinese & Indian | 109 (64.5%) | 162 (56.7%) | |
| Education years, mean ± sd | 6.51 ± 4.51 | 6.98 ± 4.64 | 0.284 |
| Household income, mean ± sd | 1806.39 ± 2579.66 | 1945.88 ± 2814.25 | 0.585 |
| Social support, mean ± sd | 40.29 ± 13.45 | 39.07 ± 14.54 | 0.363 |
| Living alone | 38 (22.4%) | 18 (6.4%) | 0.001 * |
| Smoking | 46 (27.2%) | 50 (17.7%) | 0.655 |
| Alcohol drinking | 16 (9.5%) | 16 (5.7%) | 0.855 |
| Diseases: | |||
| Diabetes | 64 (37.9%) | 53 (18.8%) | 0.067 |
| Hypertension | 111 (65.7%) | 110 (39.0%) | 0.190 |
| Hypercholesterolemia | 62 (36.7%) | 68 (24.1%) | 0.917 |
| Heart disease | 17 (10.1%) | 12 (4.26%) | 0.249 |
| Mild Cognitive Impairment (MCI) | 44 (26.0%) | 53 (20.6%) | 0.337 |
| Frailty status (pre-frailty & frailty) | 134 (79.3%) | 139 (49.3%) | 0.293 |
| Baseline Parameters | CF Status at 5 Years | ||
|---|---|---|---|
| N = 282 | p-Value | ||
| CF (n = 100) | Non-CF (n = 182) | ||
| Age, mean ± sd: | 69.09 ± 5.70 | 66.25 ± 4.54 | <0.001 * |
| Sex | |||
| Men | 37 (37.0%) | 89 (48.9%) | 0.061 |
| Women | 63 (60.3%) | 93 (51.1%) | |
| Ethnic | |||
| Malay | 47 (47.0%) | 74 (40.7%) | 0.317 |
| Chinese & Indian | 53 (53.0%) | 108 (59.3%) | |
| Education (years), mean (sd): | 3.67 ± 3.33 | 8.08 ± 4.50 | <0.001 * |
| Living alone | 14 (14.0%) | 10 (5.5%) | 0.024 |
| Smoker | 18 (18.0%) | 38 (20.9%) | 0.641 |
| Alcohol drinking | 4 (4.0%) | 13 (7.1%) | 0.433 |
| Household income, mean ± sd | 1172.73 ± 1511.22 | 2108.97 ± 305.90 | 0.001 * |
| Diseases | |||
| Diabetes | 29 (29.0%) | 34 (18.7%) | 0.053 |
| Hypertension | 53 (53.0%) | 75 (41.2%) | 0.062 |
| Hypercholesterolemia | 31 (31.0%) | 48 (26.4%) | 0.410 |
| Heart Disease | 9 (9.0%) | 7 (3.8%) | 0.104 |
| Body Mass Index, mean ± sd | 25.88 ± 4.19 | 25.24 ± 3.98 | 0.210 |
| % Body Fat, mean ± sd | 40.69 ± 10.70 | 37.15 ± 9.78 | 0.005 * |
| Fat mass (kg), mean ± sd | 25.33 ± 8.58 | 24.25 ± 8.71 | 0.316 |
| Fat free mass (kg), mean ± sd | 36.34 ± 7.85 | 39.95 ± 8.10 | <0.001 * |
| Skeletal muscle mass (kg), mean ± sd | 19.26 ± 4.68 | 21.48 ± 4.85 | <0.001 * |
| Fasting blood sugar (mmol/l), mean ± sd | 6.28 ± 2.64 | 5.95 ± 2.01 | 0.287 |
| HbA1c (%), mean ± sd | 15.01 ± 2.85 | 14.45 ± 2.55 | 0.124 |
| Total cholesterol (mmol/l), mean ± sd | 5.35 ± 1.08 | 5.11 ± 0.99 | 0.091 |
| High density lipoprotein (mmol/l), mean ± sd | 1.46 ± 0.37 | 1.44 ± 0.38 | 0.740 |
| Low density lipoprotein (mmol/l), mean ± sd | 3.18 ± 0.97 | 3.06 ± 0.93 | 0.338 |
| Triglyceride (mmol/l), mean ± sd | 1.60 ± 0.73 | 1.39 ± 0.75 | 0.032 |
| Albumin (g/l), mean ± sd | 43.21 ± 2.93 | 42.91 ± 2.86 | 0.452 |
| Blood Pressure: | |||
| Diastolic (mmHg), mean ± sd | 77.31 ± 10.39 | 76.32 ± 19.40 | 0.542 |
| Systolic (mmHg), mean ± sd | 143.09 ± 17.73 | 136.02 ± 19.40 | 0.003 * |
| Calf Circumference (cm), mean ± sd | 33.88 ± 3.16 | 34.67 ± 3.53 | 0.062 |
| Waist Circumference (cm), mean ± sd | 89.67 ± 10.27 | 88.81 ± 10.55 | 0.512 |
| Hip Circumference (cm), mean ± sd | 97.94 ± 8.88 | 98.39 ± 8.61 | 0.677 |
| MUAC (cm), mean ± sd | 29.10 ± 3.25 | 29.08 ± 3.05 | 0.965 |
| Psychosocial and functional status: | |||
| GDS, mean ± sd | 2.57 ± 2.05 | 1.92 ± 2.06 | <0.001 * |
| ADL, mean ± sd | 37.16 ± 9.31 | 43.91 ± 10.11 | <0.001 * |
| IADL, mean ± sd | 12.61 ± 2.08 | 13.48 ± 1.10 | <0.001 * |
| WHODAS, mean ± sd | 7.49 ± 7.86 | 3.55 ± 6.17 | <0.001 * |
| Neurocognitive | |||
| Mild Cognitive Impairment (MCI) | 42 (42.4%) | 51 (28.0%) | 0.017 |
| PCA of cognitive test | -0.31 ± 0.90 | 0.78 ± 0.94 | <0.001 * |
| MMSE, mean ± sd | 21.90 ± 4.99 | 25.79 ± 3.47 | <0.001 * |
| MoCA, mean ± sd | 17.88 ± 5.03 | 22.25 ± 4.77 | <0.001 * |
| Span Digit, mean ± sd | 7.29 ± 2.50 | 8.51 ± 2.28 | <0.001 * |
| RAVLT, mean ± sd | 36.71 ± 8.83 | 43.14 ± 10.64 | <0.001 * |
| Digit symbol, mean ± sd | 4.23 ± 1.70 | 7.28 ± 3.32 | <0.001 * |
| VR I, mean ± sd | 38.37 ± 29.92 | 59.64 ± 33.33 | <0.001 * |
| VR II, mean ± sd | 29.23 ± 32.27 | 53.41 ± 27.55 | <0.001 * |
| Frailty status (pre-frail & frailty) | 100 (100.0%) | 136 (74.7%) | <0.001 * |
| Fitness test | |||
| 2-minute step test, mean ± sd | 62.50 ± 25.81 | 73.57 ± 23.86 | <0.001 * |
| Chair stand test, mean ± sd | 9.69 ± 2.78 | 11.56 ± 2.84 | <0.001 * |
| Chair sit and reach test, mean ± sd | 1.34 ± 9.62 | 1.16 ± 9.09 | 0.876 |
| TUG test, mean ± sd | 10.91 ± 2.90 | 8.62 ± 1.99 | <0.001 * |
| Back scratch test, mean ± sd | 17.51 ± 12.28 | 9.98 ± 10.98 | <0.001 * |
| Nutrient Intake at Baseline | CF Status at 5 Years | ||
|---|---|---|---|
| N = 282 | p-Value | ||
| CF (n = 100) | Non-CF (n = 182) | ||
| Energy (kcal) | 1587 ± 411 | 1679 ± 406 | 0.080 |
| Protein (g/day) | 68.90 ± 21.14 | 70.70 ± 20.41 | 0.498 |
| Protein (% of energy) | 17.62 ± 3.96 | 17.04 ± 3.40 | 0.208 |
| Carbohydrate (g/day) | 207.22 ± 68.76 | 224.42 ± 67.90 | 0.050 |
| Carbohydrate (% of energy) | 51.65 ± 8.06 | 53.26 ± 8.28 | 0.127 |
| Fat (g/day) | 53.57 ± 16.67 | 54.41 ± 17.66 | 0.704 |
| Fat (% of energy) | 30.70 ± 7.18 | 29.28 ± 6.98 | 0.117 |
| Total Fibre (g/day) | 4.10 ± 2.42 | 5.04 ± 2.62 | 0.004 * |
| Vitamin C (mg/day) | 109.57 ± 75.51 | 145.86 ± 90.07 | 0.001 * |
| Vitamin D (mg/day) | 0.11 ± 0.32 | 0.49 ± 1.02 | <0.001 * |
| Vitamin E (mg/day) | 6.68 ± 19.16 | 5.52 ± 3.26 | 0.443 |
| Vitamin K (mg/day) | 19.39 ± 87.73 | 34.85 ± 91.24 | 0.181 |
| Alpha-Tocopherol (mg/day) | 0.26 ± 0.78 | 0.78 ± 1.34 | <0.001 * |
| Thiamin (mg/day) | 1.53 ± 3.20 | 1.61 ± 3.32 | 0.844 |
| Riboflavin (mg/day) | 1.18 ± 0.50 | 1.33± 0.44 | 0.010 |
| Niacin (mg/day) | 9.83 ± 3.35 | 10.81 ± 4.32 | 0.054 |
| Pyridoxine (mg/day) | 0.70 ± 0.32 | 0.76 ± 0.36 | 0.229 |
| Panthotenic acid (mg/day) | 0.23 ± 0.41 | 0.37 ± 0.47 | 0.011 |
| Folate (µg /day) | 93.43 ± 58.39 | 119.26 ± 68.38 | 0.002 * |
| Calcium (mg/day) | 439.35 ± 151.82 | 540.36 ± 222.90 | <0.001 * |
| Sodium (mg/day) | 1602.59 ± 992.36 | 1362.28 ± 710.87 | 0.039 |
| Iron (mg/day) | 12.98 ± 4.73 | 14.14 ± 4.63 | 0.052 |
| Zinc (mg/day) | 3.44 ± 1.78 | 3.87 ± 1.74 | 0.055 |
| Copper (mg/day) | 0.57 ± 0.33 | 0.71 ± 0.39 | 0.004 * |
| Magnesium (mg/day) | 126.32 ± 62.81 | 149.32 ± 66.98 | 0.006 * |
| Selenium (µg/day) | 25.13 ± 22.54 | 28.07 ± 17.71 | 0.242 |
| Predictor of Interest | B | ORAdj (95% CI) | p-Value |
|---|---|---|---|
| Age (years) | 0.116 | 1.123 (1.044–1.208) | 0.002 * |
| Digit symbol (scale score, continuous) | −0.403 | 0.668 (0.556–0.803) | <0.001 * |
| TUG test (continuous) | 0.209 | 1.232 (1.039–1.460) | 0.016 * |
| GDS (total score, continuous) | 0.182 | 1.200 (1.051–1.369) | 0.007 * |
| Vitamin D (µg, continuous) | −1.016 | 0.362 (0.141–0.930) | 0.035 * |
| Physical frailty (yes vs. no) | 0.769 | 2.157 (1.016–4.580) | 0.045 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivan, N.F.M.; Shahar, S.; Rajab, N.F.; Singh, D.K.A.; Che Din, N.; Mahadzir, H.; Mohamed Sakian, N.I.; Ishak, W.S.; Abd. Rahman, M.H.; Mohammed, Z.; et al. Incidence and Predictors of Cognitive Frailty Among Older Adults: A Community-based Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 1547. https://doi.org/10.3390/ijerph17051547
Rivan NFM, Shahar S, Rajab NF, Singh DKA, Che Din N, Mahadzir H, Mohamed Sakian NI, Ishak WS, Abd. Rahman MH, Mohammed Z, et al. Incidence and Predictors of Cognitive Frailty Among Older Adults: A Community-based Longitudinal Study. International Journal of Environmental Research and Public Health. 2020; 17(5):1547. https://doi.org/10.3390/ijerph17051547
Chicago/Turabian StyleRivan, Nurul Fatin Malek, Suzana Shahar, Nor Fadilah Rajab, Devinder Kaur Ajit Singh, Normah Che Din, Hazlina Mahadzir, Noor Ibrahim Mohamed Sakian, Wan Syafira Ishak, Mohd Harimi Abd. Rahman, Zainora Mohammed, and et al. 2020. "Incidence and Predictors of Cognitive Frailty Among Older Adults: A Community-based Longitudinal Study" International Journal of Environmental Research and Public Health 17, no. 5: 1547. https://doi.org/10.3390/ijerph17051547
APA StyleRivan, N. F. M., Shahar, S., Rajab, N. F., Singh, D. K. A., Che Din, N., Mahadzir, H., Mohamed Sakian, N. I., Ishak, W. S., Abd. Rahman, M. H., Mohammed, Z., & You, Y. X. (2020). Incidence and Predictors of Cognitive Frailty Among Older Adults: A Community-based Longitudinal Study. International Journal of Environmental Research and Public Health, 17(5), 1547. https://doi.org/10.3390/ijerph17051547