Involuntary Pregnancy Loss and Nursing Care: A Meta-Ethnography

 , , ,
, , ,
Abstract
1. Introduction
1.1. Background
1.2. Theoretical Perspective
2. Materials and Methods
2.1. Search Methods
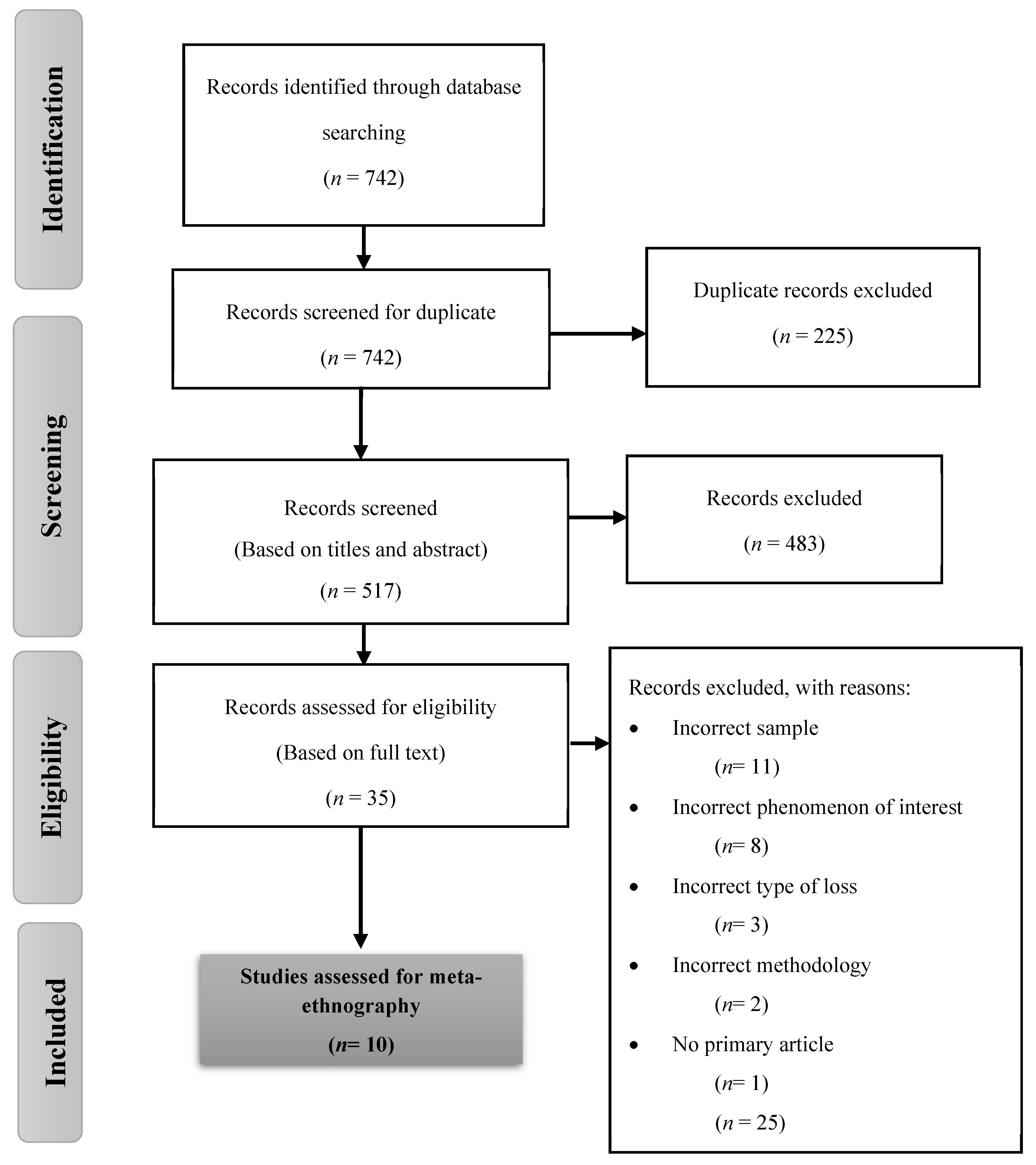
2.2. Search Outcomes
2.3. Quality Appraisal
2.4. Data Extraction and Synthesis
3. Results
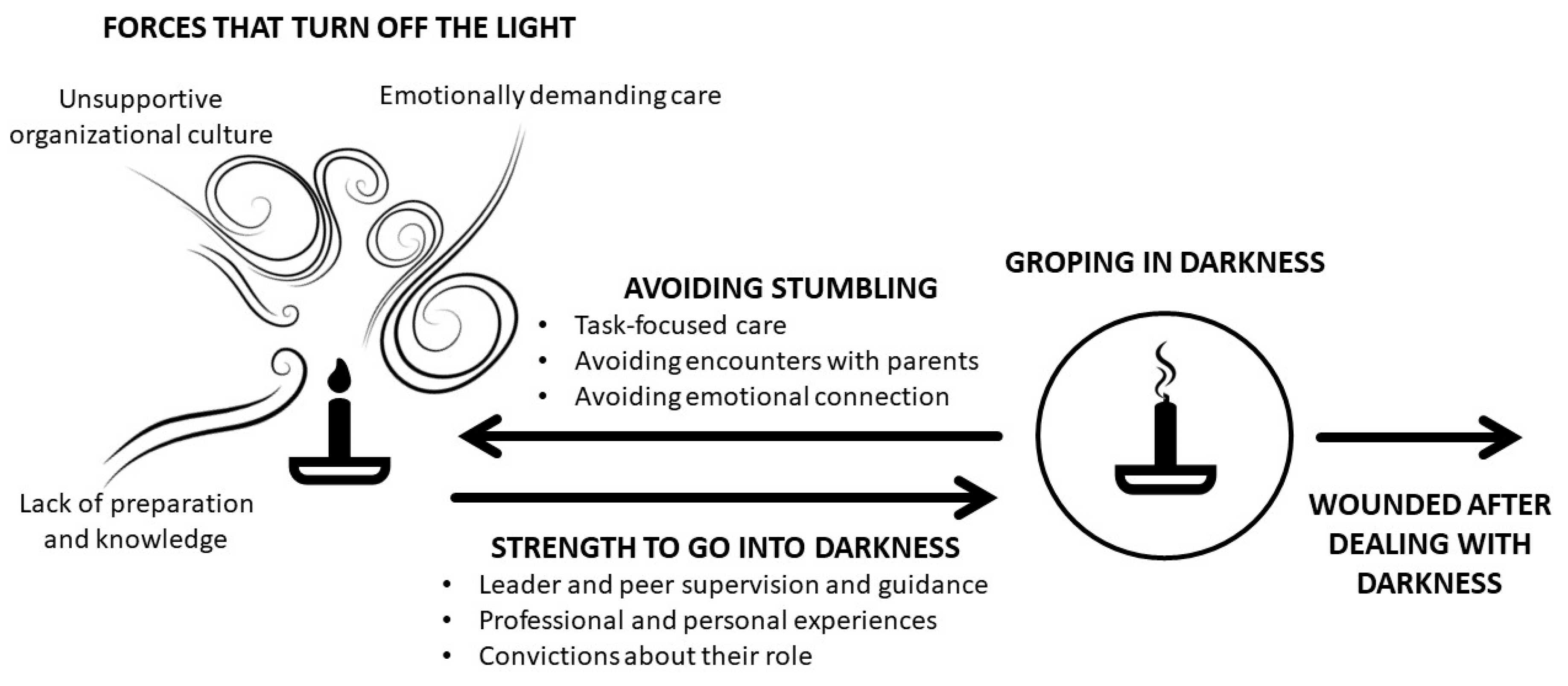
3.1. “Forces that Turn Off the Light”
3.1.1. Unsupportive Organizational Culture
3.1.2. Lack of Preparation and Knowledge
“When I started working in the operating room, I was just put into a (perinatal loss) case, and I didn’t know what to expect. I never really had any training on how to deal with the patient or with my own feelings. Unfortunately, sometimes, you are just thrown into things and you just learn.”Nurse [32].
“They really don’t recognize at all that they have had a baby, and they don’t want anything to do with either the funeral arrangements or anything like that.… To accept that their way of dealing is also normal and natural for them, there can sometimes be a bit of conflict there.”
3.1.3. Emotionally Demanding Care
“The first time I could see the parts of the baby. I was never really prepared for that. It was just shocking, and there was a moment after doing that case when I almost wanted to speak to a manager and say, ‘I may not be able to do these types of cases.’”Nurse [32].
“It’s very intense for the midwife looking after these people. There have been days when I’ve gone home and cried over different situations from here.”Midwife [29].
3.2. “Strength to Go into Darkness”
3.2.1. Leader and Peer Support and Guidance
3.2.2. Professional and Personal Experiences
3.2.3. Convictions about Care
3.3. “Avoiding Stumbling”
3.3.1. Convictions about Care
3.3.2. Avoiding Encounters with Parents
3.3.3. Avoiding Emotional Connection
3.4. “Groping in Darkness”
3.5. “Wounded after Dealing with Darkness”
4. Discussion
4.1. Strengths and Limitations
4.2. Relevance to Clinical Practice
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Criteria Headings | Pages | |
|---|---|---|
| Phase 1 Selecting meta-ethnography and getting started | 1. Rationale and context for the meta-ethnography Describe the gap in research or knowledge to be filled by the meta-ethnography and the wider context of the meta-ethnography | 1–2 |
| 2. Aim(s) of the meta-ethnography Describe the meta-ethnography aim(s) | 2 | |
| 3. Focus of the meta-ethnography Describe the meta-ethnography review question(s) (or objectives) | 2 | |
| 4. Rationale for using meta-ethnography Explain why meta-ethnography was considered the most appropriate qualitative synthesis methodology | 3, 8 | |
| Phase 2 Deciding what is relevant | 5. Search strategy Describe the rationale for the literature search strategy | 3 |
| 6. Search processes Describe how the literature searching was carried out and by whom | 3 | |
| 7. Selecting primary studies Describe the process of study screening and selection, and who was involved | 3–4 | |
| 8. Outcome of study selection Describe the results of study searches and screening | 3–4 | |
| Phase 3 Reading included studies | 9. Reading and data-extraction approach Describe the reading and data-extraction method and processes | 5 |
| 10. Presenting characteristics of included studies Describe characteristics of the included studies | 6–9 | |
| Phase 4 Determining how studies are related | 11. Process for determining how studies are related Describe the methods and processes for determining how the included studies are related: - Which aspects of studies were comparedand - How the studies were compared | 5 |
| 12. Outcome of relating studies Describe how studies relate to each other | 5 | |
| Phase 5 Translating studies into one another | 13. Process of translating studies Describe the methods of translation: • Describe steps taken to preserve the context and meaning of the relationships between concepts within and across studies • Describe how the reciprocal and refutational translations were conducted • Describe how potential alternative interpretations or explanations were considered in the translations | 5 |
| 14. Outcome of translation Describe the interpretive findings of the translation | 10–15 | |
| Phase 6 Synthesizing translations | 15. Synthesis process Describe the methods used to develop overarching concepts (“synthesized translations”), and describe how potential alternative interpretations or explanations were considered in the synthesis | 5 |
| 16. Outcome of synthesis process Describe the new theory, conceptual framework, model, configuration, or interpretation of data developed from the synthesis | 10–15 | |
| Phase 7 Expressing the synthesis | 17. Summary of findings Summarize the main interpretive findings of the translation and synthesis, and compare them to existing literature | 15 |
| 18. Strengths and limitations Reflect on and describe the strengths and limitations of the synthesis: - Methodological aspects: for example, describe how the synthesis findings were influenced by the nature of the included studies and how the meta-ethnography was conducted | 17 | |
| 19. Recommendations and conclusions Describe the implications of the synthesis | 18 | |
| Summary of Review Findings | Studies Contributing to the Review Findings | Methodological Limitations | Coherence | Relevance | Adequacy of Data | Overall CERQual Assessment of Confidence | Explanation of Decision | |
|---|---|---|---|---|---|---|---|---|
| “Forces that turn off the light” | Unsupportive organizational culture | [26,27,28,29,30,31,32,33,34] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Minor concerns regarding relevance (One study included self-employed midwives as a sample) | No concerns about adequacy of data. There were rich data to support the finding across many studies. | Minor concerns | Very minor concerns regarding coherence; no concern about adequacy of data; and minor concerns regarding methodological limitations and relevance |
| Lack of preparation and knowledge | [26,27,28,29,30,31,32,33,34,35,36] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Very minor concerns regarding relevance (All studies included nurses and midwives as a sample, focused on pregnancy loss, and were relevant to the review) | No concerns about adequacy of data. There were rich data to support the finding across all the studies. | Very minor concerns | Very minor concerns regarding coherence and relevance; no concern about adequacy of data; and minor concerns regarding methodological limitations | |
| Emotionally demanding care | [26,27,28,29,30,31,32,33,34,36] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Very minor concerns regarding relevance (All studies included nurses and midwives as a sample, focused on pregnancy loss, and were relevant to the review) | Minor concerns as the data was rich | Minor concerns | Very minor concerns regarding relevance and coherence and minor concerns regarding methodological limitations and adequacy of data | |
| “Strengths to go into darkness” | Leader and peer support and guidance | [26,27,28,30,31,32,33,34,36] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Very minor concerns regarding relevance (All studies included nurses and midwives as a sample, focused on pregnancy loss, and were relevant to the review) | Moderate concerns as the data was partially rich | Minor concerns | Very minor concerns regarding coherence and relevance; moderate concern about adequacy of data; and minor concerns regarding methodological limitations |
| Professional and personal experiences | [29,30,31,32,33,34,36] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Very minor concerns regarding relevance (All studies included nurses and midwives as a sample, focused on pregnancy loss, and were relevant to the review) | Moderate concerns as the data was partially rich | Minor concerns | Very minor concerns regarding coherence and relevance; moderate concern about adequacy of data; and minor concerns regarding methodological limitations | |
| Convictions about care | [29,30,31,32,33,34,36] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Very minor concerns regarding relevance (All studies included nurses and midwives as a sample, focused on pregnancy loss, and were relevant to the review) | Minor concerns as the data was rich | Minor concerns | Minor concerns about methodological limitations and adequacy of data and very minor concern about coherence and relevance | |
| “Avoiding stumbling” | Task-focused care | [28,31,32] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Very minor concerns regarding relevance (All studies included nurses and midwives as a sample, focused on pregnancy loss, and were relevant to the review) | Moderate concerns as the data was partially rich | Minor concerns | Minor concerns about methodological limitations; moderate concerns regarding adequacy of data; and very minor concerns about relevance and coherence |
| Avoiding encounters with parents | [26,27,31,33] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Moderate concerns regarding relevance (No studies include early pregnancy loss) | Moderate concerns as the data was partially rich | Moderate concerns | Minor concerns about methodological limitations; very minor concerns about coherence; and moderate concerns regarding adequacy of data and relevance | |
| Avoiding emotional connection | [26,27,28,29,31,32,33,34,35] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Minor concerns regarding relevance (All studies included nurses and midwives as a sample, but early pregnancy loss was not included) | Minor concerns about adequacy of data. There were rich data to support the finding across all the studies. | Minor concerns | Very minor concerns about coherence and minor concerns about methodological limitations, relevance, and adequacy of data | |
| “Groping in darkness” | [26,27,29,30,31,32,33,34,35] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Minor concerns regarding relevance (All studies included nurses and midwives as a sample, but early pregnancy loss was not included) | Minor concerns about adequacy of data. There were rich data to support the finding across all the studies. | Minor concerns | Very minor concerns about coherence and minor concerns about methodological limitations, relevance, and adequacy of data | |
| “Wounded after dealing with darkness” | [26,27,28,29,30,31,32,33,35,36] | Minor concerns regarding methodological limitations since there is lack of clarity regarding the influence of the researcher in the investigation, and vice versa | Very minor concerns regarding coherence (data very consistent within and across studies) | Very minor concerns regarding relevance (All studies included nurses and midwives as a sample, focused on pregnancy loss, and were relevant to the review) | Very minor concerns about adequacy of data. There were rich data to support the finding across many studies. | Very minor | Very minor concerns about coherence, relevance, and adequacy of data and minor concerns regarding methodological limitations | |
References
- Magnus, M.C.; Wilcox, A.J.; Morken, N.H.; Weinberg, C.R.; Håberg, S.E. Role of maternal age and pregnancy history in risk of miscarriage: Prospective register based study. BMJ 2019, 364, l869. [Google Scholar] [CrossRef]
- Blencowe, H.; Cousens, S.; Jassir, F.B.; Say, L.; Chou, D.; Mathers, C.; Hogan, D.; Shiekh, S.; Qureshi, Z.U.; You, D. National, regional, and worldwide estimates of stillbirth rates in 2015, with trends from 2000: A systematic analysis. Lancet Glob. Health 2016, 4, e98–e108. [Google Scholar] [CrossRef]
- Heazell, A.E.; Wojcieszek, A.; Graham, N.; Stephens, L. Care in pregnancies after stillbirth and perinatal death. Int. J. Birth Parent Educ. 2019, 6, 23–28. [Google Scholar]
- Kolte, A.M.; Bernardi, L.A.; Christiansen, O.B.; Quenby, S.; Farquharson, R.G.; Goddijn, M.; Stephenson, M.D. Terminology for pregnancy loss prior to viability: A consensus statement from the ESHRE early pregnancy special interest group. Hum. Reprod. 2015, 30, 495–498. [Google Scholar] [CrossRef]
- World Health Organization(WHO), Department of Reproductive Health and Research. Vaginal bleeding in early pregnancy. In Managing Complications in Pregnancy and Childbirth: A Guide for Midwives and Doctors, 2nd ed.; World Health Organization: Geneva, Switzerland, 2017; p. S10. [Google Scholar]
- World Health Organization(WHO) [Internet]. Neonatal and Perinatal Mortality Country, Regional and Global Estimates. 2006. Available online: http://whqlibdoc.who.int/publications/2006/9241563206eng.pdf (accessed on 9 January 2020).
- Fernández-Basanta, S.; Van, P.; Coronado, C.; Torres, M.; Movilla-Fernández, M.-J. Coping After Involuntary Pregnancy Loss: Perspectives of Spanish European Women. OMEGA 2019. [Google Scholar] [CrossRef]
- Hutti, M.H. Social and professional support needs of families after perinatal loss. J. Obs. Gynecol. Neonatal. Nurs. 2005, 34, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Layne, L.L. Motherhood Lost: Cultural Dimensions of Miscarriage. Women Health 1990, 16, 69–98. [Google Scholar] [CrossRef]
- McCreight, B.S. A grief ignored: Narratives of pregnancy loss from a male perspective. Sociol. Health Illn. 2004, 26, 326–350. [Google Scholar] [CrossRef]
- Murphy, F.A. The experience of early miscarriage from a male perspective. J. Clin. Nurs. 1998, 7, 325–332. [Google Scholar] [CrossRef]
- O’Leary, J.; Thorwick, C. Fathers’ perspectives during pregnancy, postperinatal loss. J. Obs. Gynecol. Neonatal. Nurs. 2006, 35, 78–86. [Google Scholar] [CrossRef]
- Ellis, A.; Chebsey, C.; Storey, C.; Bradley, S.; Jackson, S.; Flenady, V.; Alexander, H.; Dimitrios, S. Systematic review to understand and improve care after stillbirth: A review of parents’ and healthcare professionals’ experiences. BMC Pregnancy Childbirth 2016, 16. [Google Scholar] [CrossRef]
- Eriksson, K. Caring science in a new key. Nurs. Sci. Q. 2002, 15, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Ujda, R.M.; Bendiksen, R. Health care provider support and grief after perinatal loss: A qualitative study. Illn. Cris. Loss 2000, 8, 265–285. [Google Scholar] [CrossRef]
- Emond, T.; Montigny, F.; Guillaumie, L. Exploring the needs of parents who experience miscarriage in the emergency department: A qualitative study with parents and nurses. J. Clin. Nurs. 2019, 28, 1952–1965. [Google Scholar] [CrossRef] [PubMed]
- Ugwumadu, A. Management of stillbirth and perinatal loss. Obs. Gynaecol. Reprod. Med. 2015, 25, 217–221. [Google Scholar] [CrossRef]
- Fenwick, J.; Jennings, B.; Downie, J.; Butt, J.; Okanaga, M. Providing perinatal loss care: Satisfying and dissatisfying aspects for midwives. Women Birth 2007, 20, 153–160. [Google Scholar] [CrossRef]
- Lindström, U.; Lindholm, L.; Zetterlund, J.; Eriksson, K. Theory of caritative caring. In Nursing Theorists and Their Work, 6th ed.; Marriner-Tomey, A., Alligood, M., Eds.; Mosby Elsevier: St. Louis, MO, USA, 2006; pp. 191–223. [Google Scholar]
- Eriksson, K. Nursing: The caring practice “being there”. NLN Publ. 1992, 15, 201–210. [Google Scholar]
- Fernández-Basanta, S.; Coronado, C.; Movilla-Fernández, M.J. Multicultural coping experiences of parents following perinatal loss: A meta-ethnographic synthesis. J. Adv. Nurs. 2020, 76, 9–21. [Google Scholar] [CrossRef]
- Noblit, G.W.; Hare, R.D. Meta-Ethnography: Synthesizing Qualitative Studies; Sage: Newbury Park, CA, USA, 1988; Volume 11. [Google Scholar]
- France, E.F.; Cunningham, M.; Ring, N.; Uny, I.; Duncan, E.A.; Jepson, R.G.; Maxwell, M.; Roberts, R.J.; Turley, R.L.; Booth, A. Improving reporting of meta-ethnography: The eMERGe reporting guidance. BMC Med. Res. Methodol. 2019, 19, 25. [Google Scholar] [CrossRef]
- Sandelowski, M.; Barroso, J. Handbook for Synthesizing Qualitative Research; Springer Publishing Company: New York, NY, USA, 2006. [Google Scholar]
- The Joanna Briggs Institute Critical Appraisal Tools for Use in JBI Systematic Reviews Checklist for Qualitative Research. Available online: http://joannabriggs.org/research/critical-appraisal-tools.html (accessed on 9 January 2020).
- Nallen, K. Midwives’ needs in relation to the provision of bereavement support to parents affected by perinatal death. Part one. Midirs. Midwifery Dig. 2006, 16, 537–542. [Google Scholar]
- Nallen, K. Midwives’ needs in relation to the provision of bereavement support to parents affected by perinatal death. Part two. Midirs. Midwifery Dig. 2007, 17, 105–112. [Google Scholar]
- Nash, M.; Barry, M.; Bradshaw, C. Midwives’ experiences of caring for women with early pregnancy loss in an Irish maternity hospital. Br. J. Midwifery 2018, 26, 796–805. [Google Scholar] [CrossRef]
- Willis, P. Nurses’ Perspective on Caring for Women Experiencing Perinatal Loss. MCN Am. J. Matern. Child. Nurs. 2019, 44, 46–51. [Google Scholar] [CrossRef] [PubMed]
- McCreight, B.S. Perinatal grief and emotional labour: A study of nurses’ experiences in gynae wards. Int. J. Nurs. Stud. 2005, 42, 439–448. [Google Scholar] [CrossRef]
- Beaudoin, M.A.; Ouellet, N. An exploration of factors influencing nursing practice for families coping with perinatal loss. Rech. Soins. Infirm. 2018, 2, 58–69. [Google Scholar] [CrossRef]
- Hutti, M.H.; Polivka, B.; White, S.; Hill, J.; Clark, P.; Cooke, C.; Clemens, S.; Abell, H. Experiences of Nurses Who Care for Women After Fetal Loss. J. Obs. Gynecol. Neonatal. Nurs. 2016, 45, 17–27. [Google Scholar] [CrossRef]
- Roehrs, C.; Masterson, A.; Alles, R.; Witt, C.; Rutt, P. Caring for families coping with perinatal loss. J. Obs. Gynecol. Neonatal. Nurs. 2008, 37, 631–639. [Google Scholar] [CrossRef]
- Martínez-Serrano, P.; Palmar-Santos, A.M.; Solís-Muñoz, M.; Álvarez-Plaza, C.; Pedraz-Marcos, A. Midwives’ experience of delivery care in late foetal death: A qualitative study. Midwifery 2018, 66, 127–133. [Google Scholar] [CrossRef]
- Jones, K.; Smythe, L. The impact on midwives of their first stillbirth. N. Z. Coll. Midwives J. 2015, 51, 17–22. [Google Scholar] [CrossRef]
- Jonas-Simpson, C.; McMahon, E.; Watson, J.; Andrews, L. Nurses’ experiences of caring for families whose babies were born still or died shortly after birth. Int. J. Hum. Caring 2010, 14, 14–21. [Google Scholar]
- Schütz, A. Collected Papers; Martinus Nijhoff: The Hague, The Netherlands, 1962; Volume 1. [Google Scholar]
- Lewin, S.; Glenton, C.; Munthe-Kaas, H.; Carlsen, B.; Colvin, C.J.; Gülmezoglu, M.; Noyes, J.; Booth, A.; Garside, R.; Rashidian, A. Using qualitative evidence in decision making for health and social interventions: An approach to assess confidence in findings from qualitative evidence syntheses(GRADE-CERQual). PLoS Med. 2015, 12, e1001895. [Google Scholar] [CrossRef] [PubMed]
- Arman, M.; Rehnsfeldt, A. The Presence of Love in Ethical Caring. Nurs. Forum 2006, 41, 4–12. [Google Scholar] [CrossRef] [PubMed]
- McQueen, A. Nurse-patient relationships and partnership in hospital care. J. Clin. Nurs. 2000, 9, 723–731. [Google Scholar] [CrossRef]
- Maturo, A. Medicalization: Current concept and future directions in a bionic society. Mens. Sana Monogr. 2012, 10, 122–133. [Google Scholar] [CrossRef]
- Bondas, T.E. Caritative leadership: Ministering to the patients. Nurs. Adm. Q. 2003, 27, 249–253. [Google Scholar] [CrossRef]
- Bondas, T. Preparing the air for nursing care: A grounded theory study of first line nurse managers. J. Res. Nurs. 2009, 14, 351–362. [Google Scholar] [CrossRef]
- Henderson, A. Emotional labor and nursing: An under-appreciated aspect of caring work. Nurs. Inq. 2001, 8, 130–138. [Google Scholar] [CrossRef]
- Strandås, M.; Bondas, T. The nurse-patient relationship as a story of health enhancement in community care: A meta-ethnography. J. Adv. Nurs. 2018, 74, 11–22. [Google Scholar] [CrossRef]
- Smith, P. The Emotional Labour of Nursing: Its Impact on Interpersonal Relations, Management and Educational Environment; Macmillan International Higher Education LTD: London, UK, 1992. [Google Scholar] [CrossRef]
- Hochschild, A.R. The Managed Heart; University of California Press: Berkeley, CA, USA, 1983. [Google Scholar]
- Huynh, T.; Alderson, M.; Thompson, M. Emotional labour underlying caring: An evolutionary concept analysis. J. Adv. Nurs. 2008, 64, 195–208. [Google Scholar] [CrossRef]
- Phillips, S. Labouring the emotions: Expanding the remit of nursing work? J. Adv. Nurs. 1996, 24, 139–143. [Google Scholar] [CrossRef]
- Bondas, T. Nursing leadership from the perspective of clinical group supervision: A paradoxical practice. J. Nurs. Manag. 2010, 18, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Britten, N.; Campbell, R.; Pope, C.; Donovan, J.; Morgan, M.; Pill, R. Using meta ethnography to synthesise qualitative research: A worked example. J. Health Serv. Res. Policy 2002, 7, 209–215. [Google Scholar] [CrossRef] [PubMed]


| Article | Questions | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| Nallen (2006, 2007) † [26,27] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | – | ✓ | ✓ | ✓ |
| Nash (2018) [28] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | – | ✓ | ✓ | ✓ |
| Willis (2019) [29] | 🗴 | ✓ | ✓ | ✓ | ✓ | ✓ | 🗴 | ✓ | – | ✓ |
| McCreight (2005) [30] | ✓ | ✓ | ✓ | – | ✓ | ✓ | 🗴 | ✓ | ✓ | ✓ |
| Beaudoin and Ouellet (2018) [31] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 🗴 | ✓ | ✓ | ✓ |
| Hutti (2016) [32] | – | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Roehrs et al. (2008) [33] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Martinez-Serrano et al. (2018) [34] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | – | ✓ | ✓ | ✓ |
| Jones and Smythe (2015) [35] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Jonas-Simpson et al. (2010) [36] | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | – | ✓ | ✓ | ✓ |
| Authors (Year) Location | Methodology | Aim | Sample and Setting | Type of Loss | Data Collection Methods | Key Findings |
|---|---|---|---|---|---|---|
| Nallen (2006, 2007) Ireland [26,27] | Descriptive qualitative methodology | To explore midwives’ views regarding the provision of bereavement support to parents affected by perinatal death | 18 hospital midwives | Perinatal death | 3 focus groups | The findings centred on 5 major themes which emerged from the data: role recognition, prerequisites to bereavement support, perceived barriers to bereavement support, coping strategies, and spiritual support. |
| Nash et al. (2018) Ireland [28] | Descriptive qualitative design | To explore the perceptions of midwives caring for women experiencing early pregnancy loss. | 8 midwives (maternity hospital) | Early pregnancy loss (<13 gestational week) | Face-to-face semi-structured interviews | Themes identified were: “coping with the experience of early pregnancy loss”, “compassionate care for women and midwives”, and “what midwives found difficult”. |
| Willis (2019) USA [29] | Descriptive qualitative methodology | To describe the experience of caring for women with a perinatal loss from the perspective of the nurse and to determine the extent to which the response to perinatal loss reflects a process. | 9 labour and delivery nurses | Perinatal loss (>20th gestational week to 1-month post birth) | In-depth interviews | Several themes depicting nurses’ experience were identified: struggling with emotions, carrying on in the moment, being present for the patient, expressing conflict, and taking care of self. A process was identified by nurses describing their response to perinatal loss. The process began with recognition of the loss and progressed through phases including the recognition of their emotional impact, connecting with the mother, dealing with emotions, acting professionally, preparing to return to work, and never forgetting the woman. |
| McCreight (2005) Ireland [30] | Not mentioned | To collaboratively explore with gynae nurses how they constructed meanings through their narratives in relation to the professionally defined but personally experienced events of pregnancy loss. | 14 gynaecological nurses | Pregnancy loss | Semi-structured in-depth interviews | Emotion can be conceived of as a valid resource for professionals when integrated into a nurse’s matrix of professional understandings. The study also demonstrates that value should be attached to emotional work which may not be fully visible, particularly for nurses working in gynaecological units. The emotional needs of nurses need to be fully acknowledged through recognition of the importance of managed emotion in the construction of professional knowledge. |
| Beaudoin and Ouellet (2018), Canada [31] | Fourth-generation constructivist evaluative method | To explore the factors influencing the practice of nurses with families experiencing perinatal loss in a secondary obstetric care centre in the Quebec region | 7 obstetric nurses 3 managing nurses | Perinatal loss (Death of a baby during the pregnancy (>20 gestational week) or a few days to a few weeks after childbirth) | Semi-structured interviews | Five themes were identified: the quality of the relationship between the nurse and the bereaved family, the nurse’s personal characteristics, the emotions felt by the nurse, work organization on the hospital unit, and the context in which nursing care is provided to families. These themes draw attention to the importance of building a solid relationship of trust with bereaved families in which honesty, empathy, human warmth, and listening have a central place. |
| Hutti (2016) USA [32] | Not mentioned | To examine the experiences of, meaning for, and personal consequences for obstetric, emergency, and surgical nurses caring for women after foetal death and to determine how these nurses use Swanson’s caring processes in providing such care. | 28 obstetric, surgery, and emergency nurses | Foetal loss (Included miscarriages (<20 gestational week) and stillbirths (from >20 gestational week to birth)) | Focus group | Swanson’s caring processes were used as a way to describe the unified experiences of nurses who care for families after a perinatal loss. All nurses, regardless of specialty, used Swanson’s caring processes, but they used them preferentially according to situational exigencies and level of rapport developed with each patient. |
| Roehrs et al. (2008) USA [33] | Descriptive qualitative methodology | To describe support needs and comfort level of labour nurses caring for families experiencing perinatal loss. | 10 labour nurses | Perinatal loss (between >20 gestational week and 7 days old) | Online surveys and follow-up interviews | Nurses are generally comfortable but find it difficult to provide perinatal bereavement care. Strategies for coping include focusing on needed care, talking to nursing peers, and spending time with their own family members. Nurses take turns providing care depending on ‘‘who is best able to handle it that day’’ and prefer not to be assigned a labouring patient in addition to the grieving parents. Developing clinical expertise is necessary to gain the comfort level and the skills necessary to care for these vulnerable families. Orientation experiences and nursing staff debriefing would help. |
| Martinez-Serrano et al. (2018) Spain [34] | Hermeneutic-interpretative phenomenological approach | To explore the experiences of midwives regarding the attention given during labour in late foetal death. | 17 hospital midwives and 1 primary health centre midwife | Late foetal death (≥1000 g birth weight, ≥28 gestational week and ≥35 cm body length) | 3 focus groups | Two main themes were identified: professionals for life not death and organizing the work without guidelines. Midwives felt that there is a lack of social awareness related to the possibility of antepartum death that keeps the mourning hidden and affects the midwives’ practice during the late foetal death process. Midwives recognize difficulties in coping with a process that ends in death: organizations are not prepared for these events (not suitable rooms), and there is lack of training to cope with them and lack of continuity in the attention received by the parents when they are discharged. |
| Jones (2015) New Zeeland [35] | Hermeneutic interpretive phenomenology | To explore, understand, and appreciate the lived experience of midwives who have cared for parents whose baby has been stillborn. | 5 self-employed midwives | Stillbirth (the death of a baby before or during birth, from the 20 gestational week onwards, or weighing 400 grams or more at birth) | Individual interviews | Two themes were identified. This paper focused on the theme “a pocketful of grief” which is made up of three subthemes: “shockwave”, “self-protection”, and “blameworthiness”. The death of a baby is a significant event for the midwife providing care. |
| Jonas-Simpson et al. (2010) Canada [36] | Exploratory qualitative descriptive method | To explore their experience of caring for families whose babies were born still or who died shortly after birth. | 9 obstetrical nurses | Stillbirth (>20 gestational week) | In-depth face-to-face structured interview | Findings revealed that caring for bereaved families is a difficult yet meaningful experience valued by the nurses in this study. Connecting and supporting bereaved families with their babies was identified as an essential part of practice. Understanding from colleagues as well as time and space for reflection were helpful. Nurses offered mothers anticipatory guidance and described thinking about the mothers, even years later. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Basanta, S.; Movilla-Fernández, M.-J.; Coronado, C.; Llorente-García, H.; Bondas, T. Involuntary Pregnancy Loss and Nursing Care: A Meta-Ethnography. Int. J. Environ. Res. Public Health 2020, 17, 1486. https://doi.org/10.3390/ijerph17051486
Fernández-Basanta S, Movilla-Fernández M-J, Coronado C, Llorente-García H, Bondas T. Involuntary Pregnancy Loss and Nursing Care: A Meta-Ethnography. International Journal of Environmental Research and Public Health. 2020; 17(5):1486. https://doi.org/10.3390/ijerph17051486
Chicago/Turabian StyleFernández-Basanta, Sara, María-Jesús Movilla-Fernández, Carmen Coronado, Haizea Llorente-García, and Terese Bondas. 2020. "Involuntary Pregnancy Loss and Nursing Care: A Meta-Ethnography" International Journal of Environmental Research and Public Health 17, no. 5: 1486. https://doi.org/10.3390/ijerph17051486
APA StyleFernández-Basanta, S., Movilla-Fernández, M.-J., Coronado, C., Llorente-García, H., & Bondas, T. (2020). Involuntary Pregnancy Loss and Nursing Care: A Meta-Ethnography. International Journal of Environmental Research and Public Health, 17(5), 1486. https://doi.org/10.3390/ijerph17051486