Child Posture and Belt Fit in a Range of Booster Configurations



Abstract
1. Introduction
2. Materials and Methods
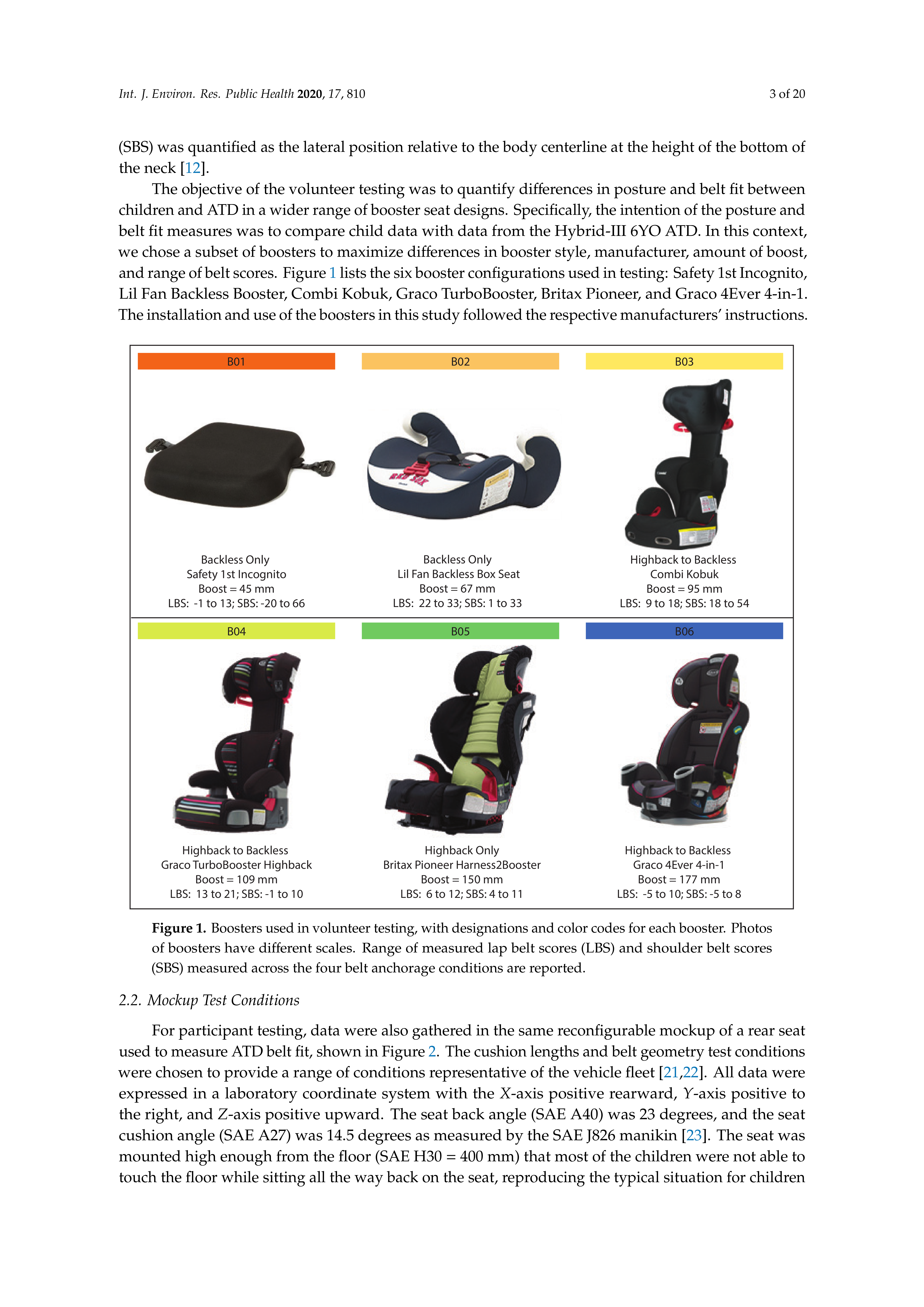
2.1. Booster Selection
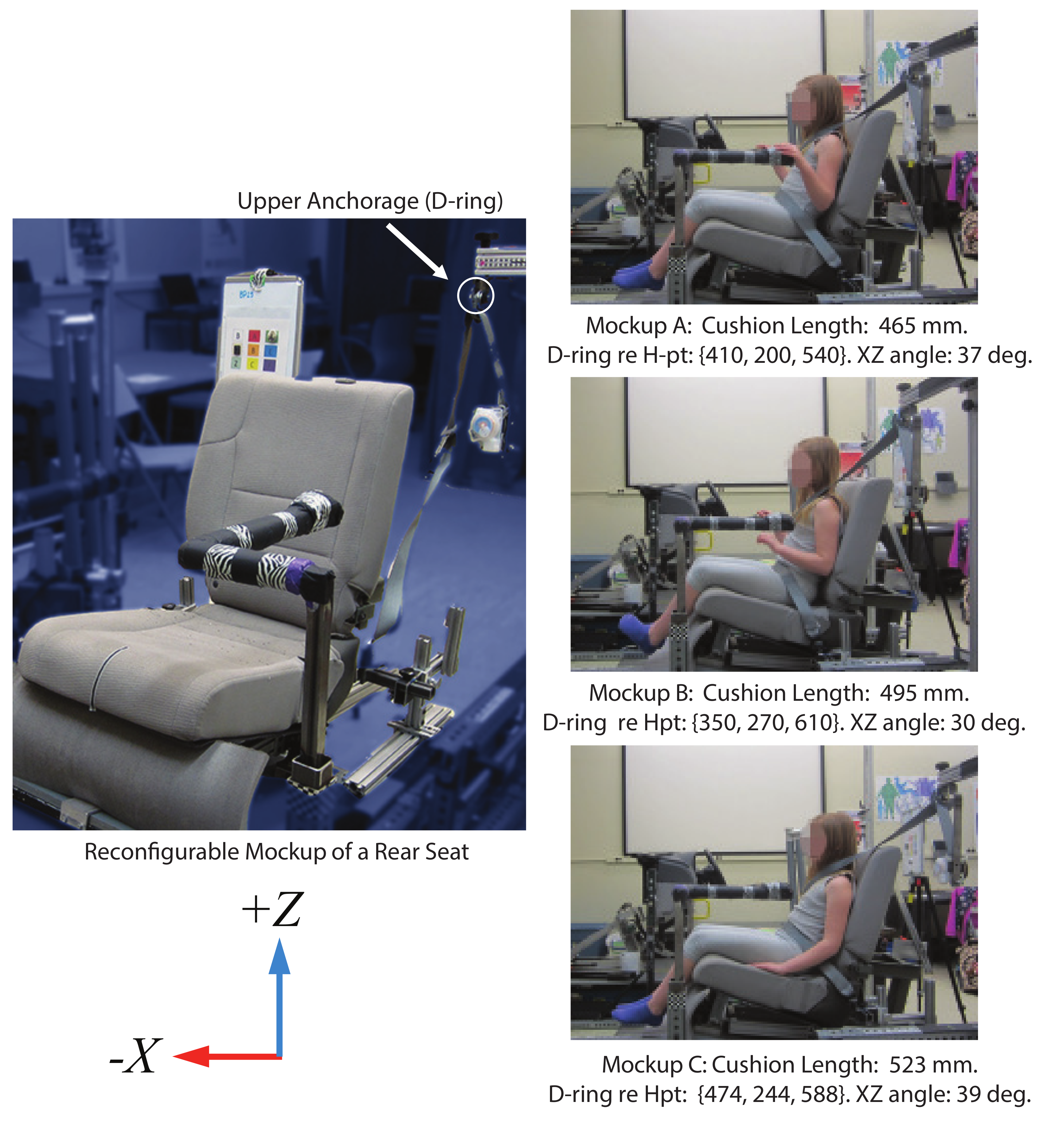
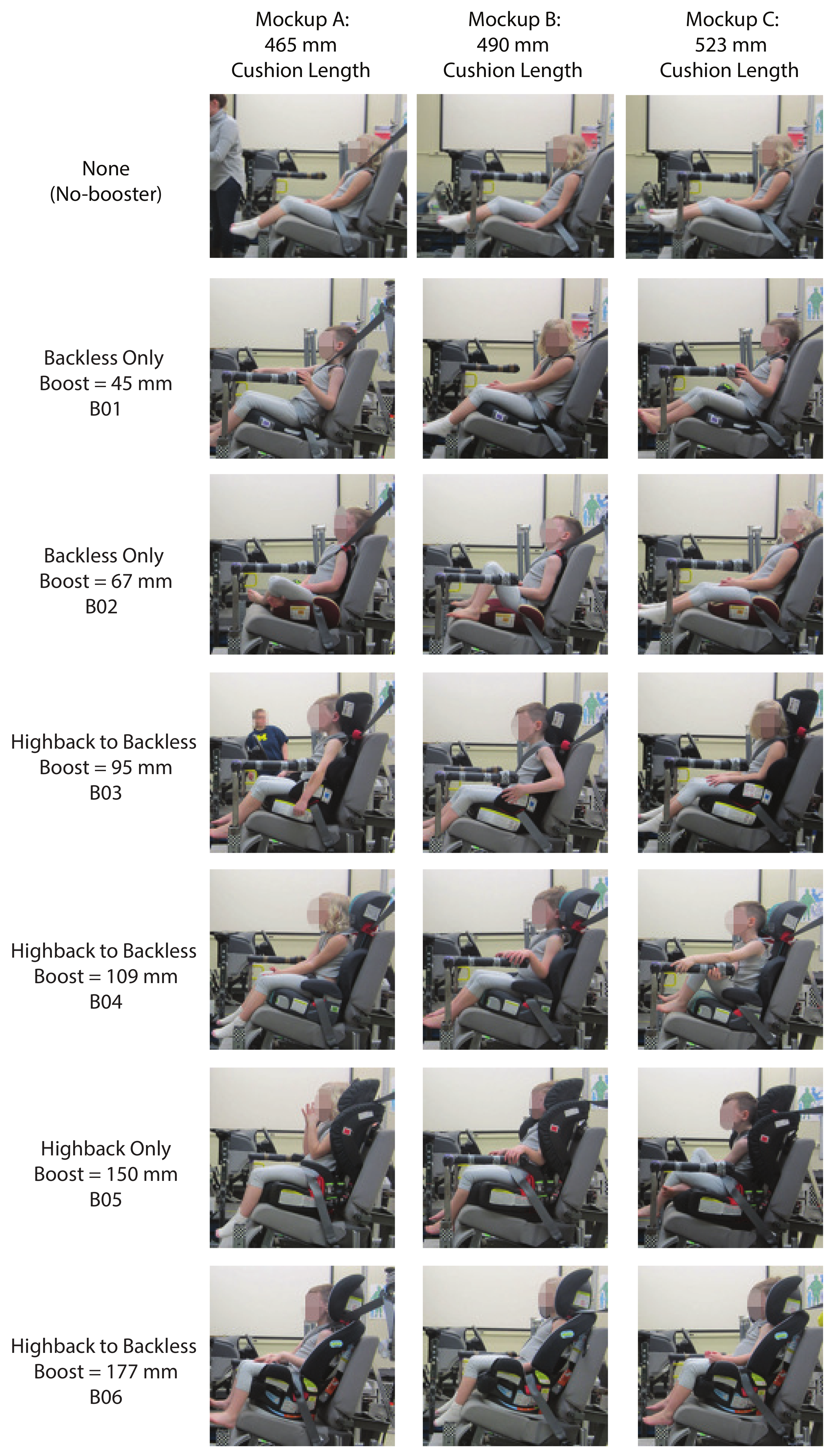
2.2. Mockup Test Conditions
2.3. Participants
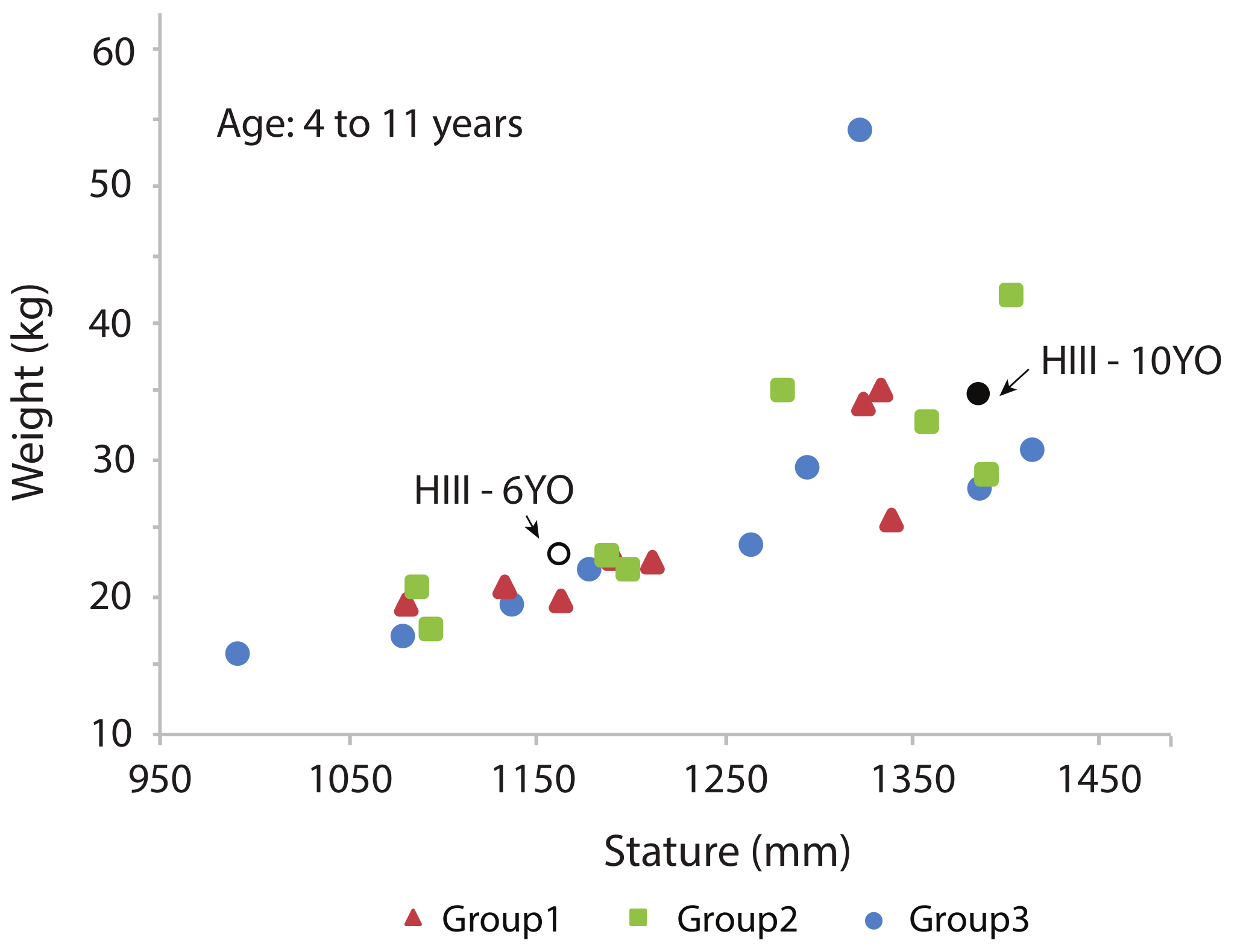
2.4. Participant Body Dimensions
2.5. Test Protocol
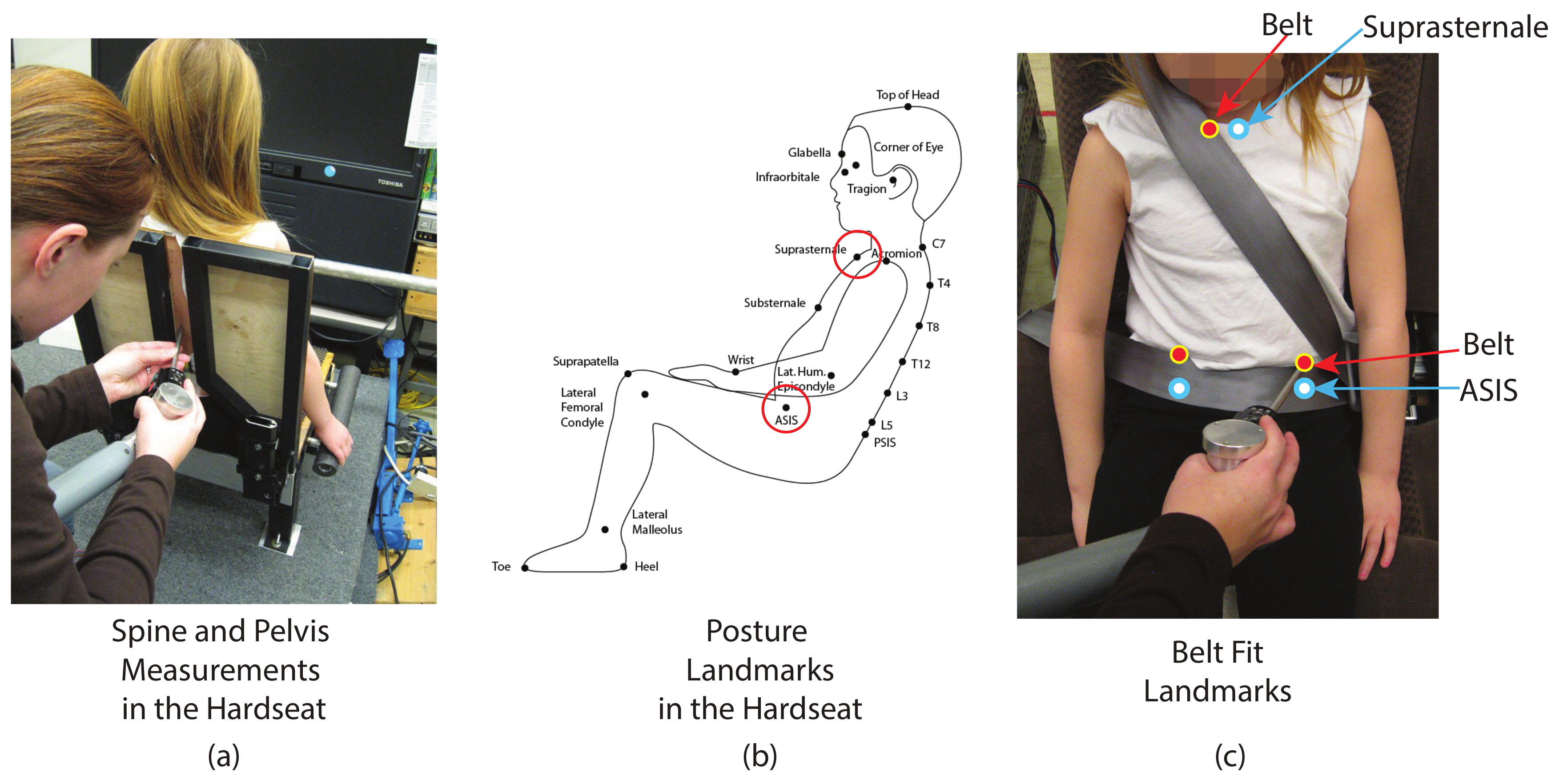
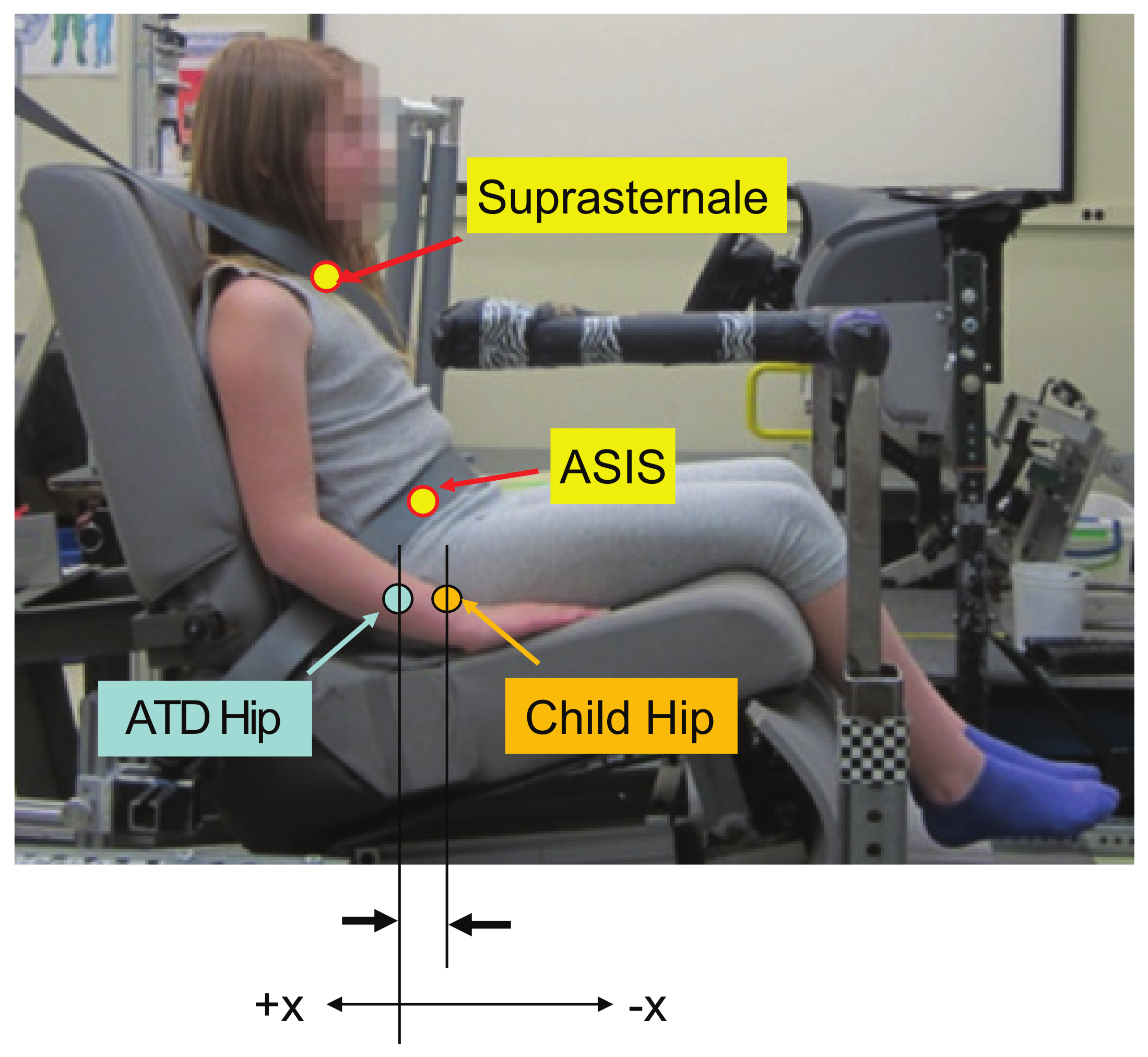
2.6. Posture and Belt Fit Measures
3. Results
3.1. Posture Measures
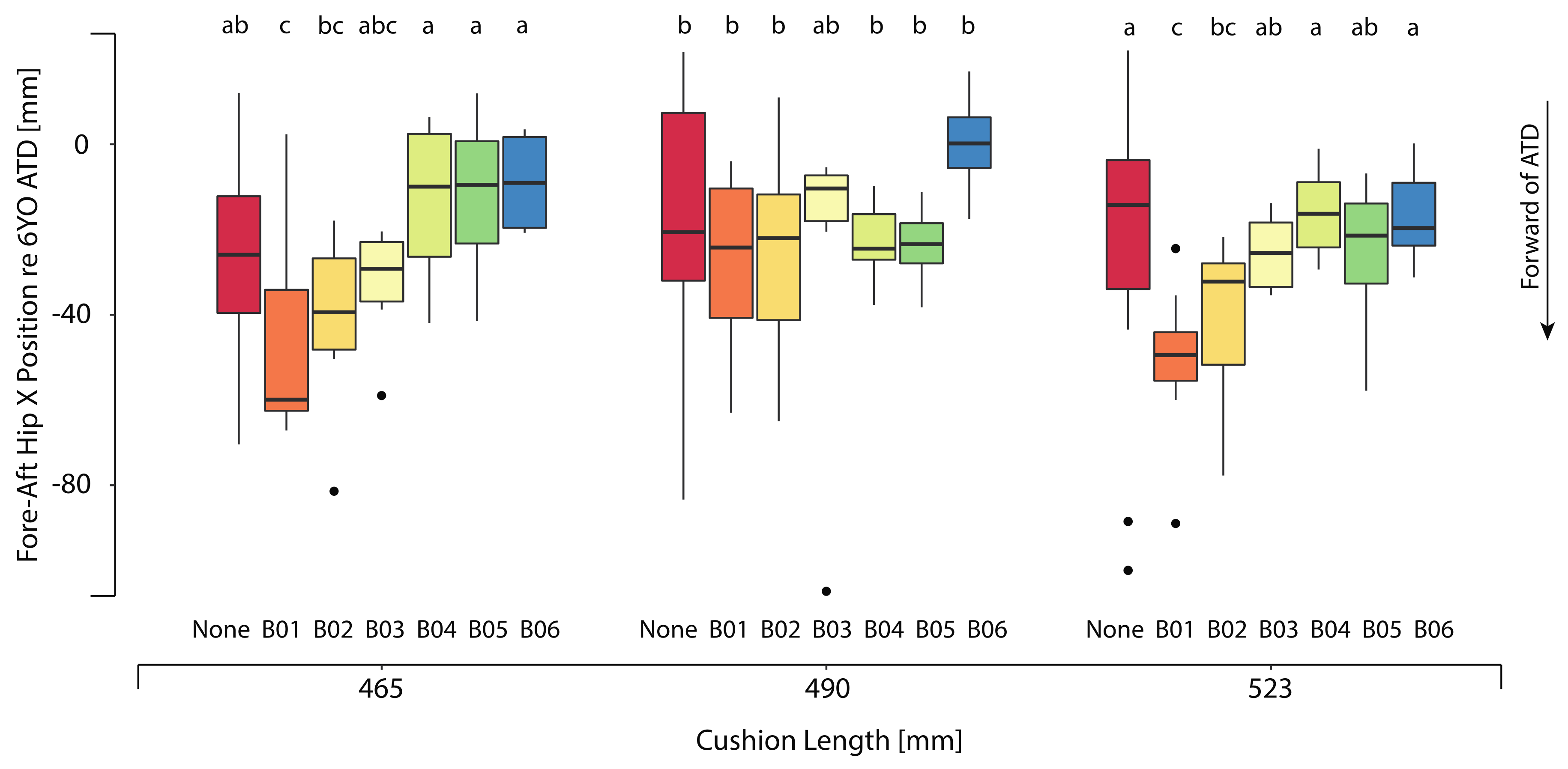
3.1.1. Hip Position vs. 6YO ATD
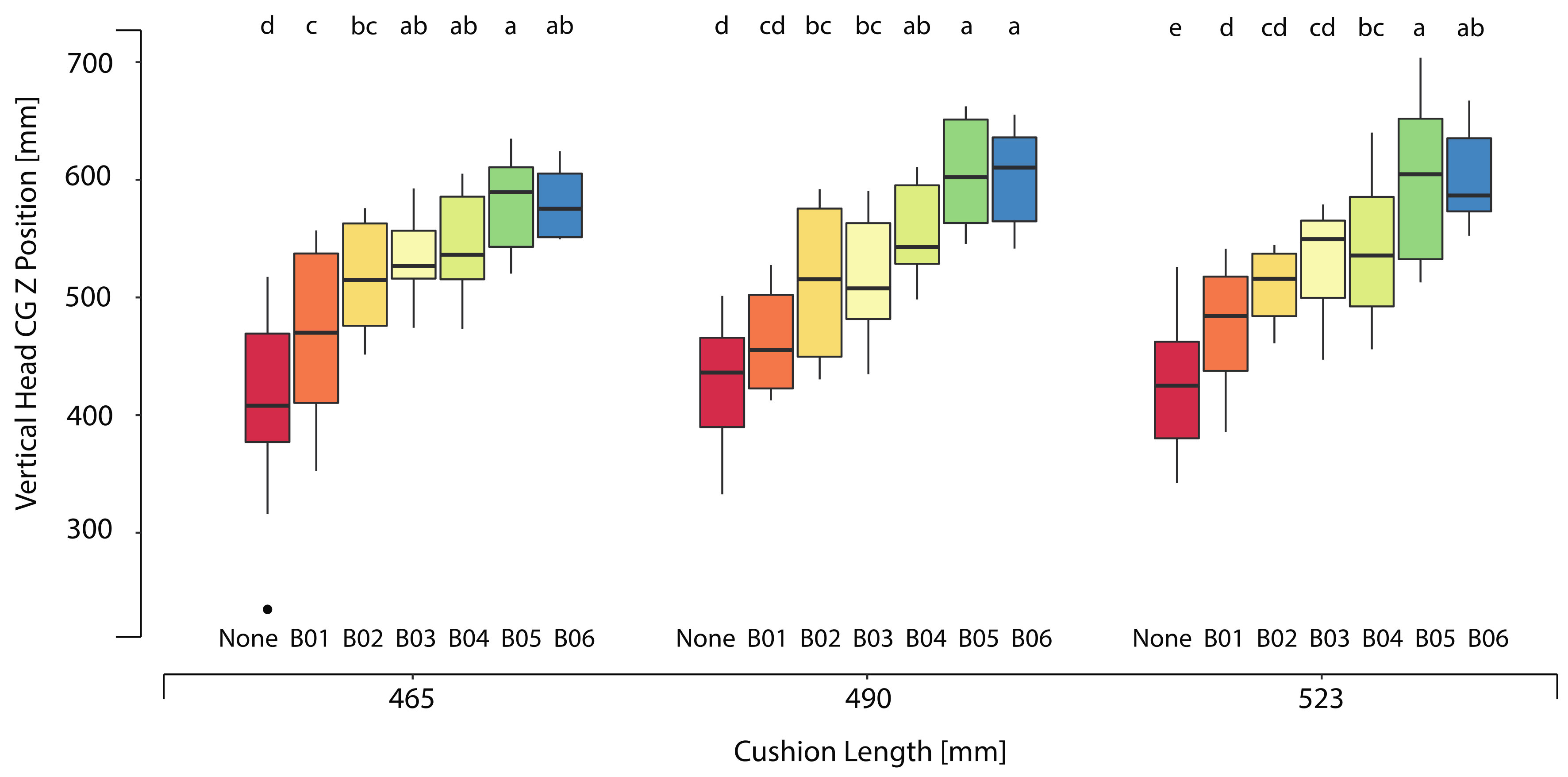
3.1.2. Head Position
3.2. Belt Fit Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A



References
- Li, H.R.; Pickrell, T.M.; KC, S. The 2015 National Survey of the Use of Booster Seats; Report No. DOT HS 812 309; National Highway Traffic Safety Administration: Washington, DC, USA, 2016. [Google Scholar]
- Klinich, K.D.; Benedetti, M.; Manary, M.A.; Flannagan, C.A. Rating child passenger safety laws relative to best practices for child occupant protection. Traffic Inj. Prev. 2016, 18, 406–411. [Google Scholar] [CrossRef]
- Benedetti, M.; Klinich, K.D.; Manary, M.A.; Flannagan, C.A. Predictors of restraint use among child occupants. Traffic Inj. Prev. 2017, 18, 866–869. [Google Scholar] [CrossRef] [PubMed]
- Arbogast, K.B.; Jermakian, J.S.; Kallan, M.F.; Durbin, D.R. Effectiveness of belt positioning booster seats: An updated assessment. Pediatrics 2009, 124, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Durbin, D.R.; Elliott, M.R.; Winston, F.K. Belt positioning booster seats and reduction in risk of injury among children in vehicle crashes. JAMA 2003, 289, 2835–2840. [Google Scholar] [CrossRef] [PubMed]
- Bilston, L.E.; Sagar, N. Geometry of rear seats and child restraints compared to child anthropometry. Stapp Car Crash J. 2007, 51, 275–298. [Google Scholar] [PubMed]
- Klinich, K.D.; Reed, M.P.; Ritchie, N.L.; Manary, M.A.; Schneider, L.W.; Rupp, J.D. Assessing Child Belt Fit, Volume II: Effect of Restraint Configuration, Booster Seat Designs, Seating Procedure, and Belt Fit on the Dynamic Response of the Hybrid III 10YO ATD in Sled Tests; UM-2008-49-2; University of Michigan: Ann Arbor, MI, USA, 2008. [Google Scholar]
- Klinich, K.D.; Reed, M.P.; Manary, M.A.; Orton, N.R.; Rupp, J.D. Optimizing Protection for Rear Seat Occupants: Assessing Booster Performance with Realistic Belt Geometry Using the Hybrid III 6YO ATD; UM-2011-40; University of Michigan: Ann Arbor, MI, USA, 2011. [Google Scholar]
- Klinich, K.D.; Reed, M.P.; Hu, J.; Rupp, J.D. Assessing the Restraint Performance of Vehicle Seats and Belt Geometry Optimized for Older Children; Report No. DOT HS 812 048, UMTRI 2012-4; National Highway Traffic Safety Administration: Washington, DC, USA, 2014. [Google Scholar]
- Reed, M.P.; Ebert-Hamilton, S.M.; Manary, M.A.; Klinich, K.D.; Schneider, L.W. A new database of child anthropometry and seated posture for automotive safety applications. Technical Paper 2005-01-1837. SAE Trans. J. Passeng. Cars Mech. Syst. 2005, 114, 2222–2235. [Google Scholar]
- Reed, M.P.; Ebert-Hamilton, S.M.; Manary, M.A.; Klinich, K.D.; Schneider, L.W. Improved positioning procedures for 6YO and 10YO ATDs based on child occupant postures. Technical Paper 2006-22-0014. Stapp Car Crash J. 2006, 50, 337–388. [Google Scholar] [PubMed]
- Reed, M.P.; Ebert, S.M.; Klinich, K.D.; Manary, M.A. Assessing Child Belt Fit, Volume I: Effects of Vehicle Seat and Belt Geometry on Belt Fit for Children with and without Belt Positioning Booster Seats; UMTRI 2008-49-1; University of Michigan: Ann Arbor, MI, USA, 2008. [Google Scholar]
- Reed, M.P.; Ebert, S.M.; Sherwood, C.P.; Klinich, K.D.; Manary, M.A. Evaluation of the static belt fit provided by belt positioning booster seats. Accid. Anal. Prev. 2009, 41, 598–607. [Google Scholar] [CrossRef] [PubMed]
- Reed, M.P.; Ebert-Hamilton, S.M.; Klinich, K.D.; Manary, M.A.; Rupp, J.D. Effects of vehicle seat and belt geometry on belt fit for children with and without belt positioning booster seats. Accid. Anal. Prev. 2013, 50, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Reed, M.P.; Klinich, K.D. Predicting Vehicle Belt Fit for Children Ages 6-12. Traffic Inj. Prev. 2016, 17, 58–64. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics. Car Seats: Product Listings for 2017. Available online: https://www.healthychildren.org/English/safety-prevention/on-the-go/Pages/Car-Safety-Seats-Product-Listing.aspx (accessed on 2 October 2017).
- Insurance Institute for Highway Safety. Booster Seat Belt Fit Evaluation Protocol (Version III); Insurance Institute for Highway Safety: Ruckersville, VA, USA. Available online: http://www.iihs.org/iihs/ratings/technical-information/boosterprotocols (accessed on 23 March 2018).
- National Highway Traffic Safety Administration. Laboratory Test Procedure for FMVSS No. 213. TP-213-10; National Highway Traffic Safety Administration: Washington, DC, USA, 2014. [Google Scholar]
- Park, J.; Ebert, S.M.; Reed, M.P.; Hallman, J.J. A statistical model including age to predict passenger postures in the rear seats of automobiles. Ergonomics 2016, 59, 796–805. [Google Scholar] [CrossRef] [PubMed]
- 49 CFR § 571.210—Standard No. 210; Seat Belt Assembly Anchorages; Code of Federal Regulations (annual edition). Title 49: Transportation. Subpart B: Federal Motor Vehicle Safety Standards; Cornell Law School: Ithaca, NY, USA, 2019.
- Huang, S.; Reed, M. Comparison of Child Body Dimensions with Rear Seat Geometry; SAE Technical Paper 2006-01-1142; University of Michigan Transportation Research Institute: Ann Arbor, MI, USA, 2006. [Google Scholar] [CrossRef]
- Reed, M.; Ebert-Hamilton, S. Distribution of belt anchorage locations in the second row of passenger cars and light trucks. Sae Int. J. Transp. Saf. 2013, 1, 25–31. [Google Scholar] [CrossRef][Green Version]
- Society of Automotive Engineers. Motor Vehicle Seat Dimensions; SAE Recommended Practice J2732; SAE International: Warrendale, PA, USA, 2008. [Google Scholar]
- NHTSA. Preliminary drawings of an upgraded standard seat assemble to evaluate child restraint systems. Available online: https://www.regulations.gov/document?D=NHTSA-2013-0055-0002 (accessed on 17 March 2015).
- Mertz, H.J.; Jarrett, K.; Moss, S.; Salloum, M.; Zhao, Y. The Hybrid III, 10-year-old dummy. Stapp Car Crash J. 2001, 45, 319–328. [Google Scholar] [PubMed]
- Reed, M.P.; Ebert-Hamilton, S.M.; Hallman, J.J. Effects of Driver Characteristics on Seat Belt Fit. Stapp Car Crash J. 2013, 57, 43–57. [Google Scholar] [PubMed]
- Cross, S.L.; Koppel, S.; Arbogast, K.B.; Bohman, K.; Rudin-Brown, C.M.; Charlton, J.L. The common characteristics and behaviors of child occupants in motor vehicle travel. Traffic Inj. Prev. 2019, 20, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Charlton, J.; Koppel, S.; Kopinathan, S.; Taranto, D. How do children really behave in restraint systems while traveling in cars? Annu. Adv. Automot. Med. 2010, 54, 181–192. [Google Scholar]
- Charlton, J.L.; Koppel, S.; Cross, S.; Kuo, J.; Rudin-Brown, C.; Arbogast, K.; Stockman, I. Naturalistic observation of children in cars: An international partnership. In Proceedings of the 1st International Conference on Protection of Children in Cars, Munchen, Germany, December 2013. [Google Scholar]
- Osvalder, A.L.; Hansson, I.; Stockman, I.; Carlsson, A.; Bohman, K.; Jakobsson, L. Older children’s sitting postures, behavior and comfort experiences during ride—A comparison between an integrated booster cushion and a high-back booster. In Proceedings of the IRCOBI Conference, Gothenburg, Sweden, 11–13 September 2013. [Google Scholar]
- Bohman, K.; Arbogast, K.B.; Loeb, H.; Charlton, J.L.; Koppel, S.; Cross, S.L. Frontal and oblique crash tests of HIII 6-year-old child ATD using real-world, observed child passenger postures. Traffic Inj. Prev. 2018, 19 (Suppl. 1), S125–S130. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| D-Ring Location Levels | X | Y | Z | Side-View (XZ) Angle (deg) | Front-View (YZ) Angle (deg) * |
|---|---|---|---|---|---|
| Fleet −1 STD | 309 | 210 | 510 | 26 | 20 |
| Fleet +1 STD | 513 | 298 | 652 | 44 | 28 |
| Mockup A | 410 | 200 | 540 | 37 | 20 |
| Mockup B | 350 | 270 | 610 | 30 | 24 |
| Mockup C | 474 | 244 | 588 | 39 | 23 |
| Lower Anchorage Location Levels | X | Y | Z | Side-View (XZ) Angle (deg) † | Front-View (YZ) Angle (deg) |
| Fleet −1 STD | 54 | 214 | −83 | 40 | 18 |
| Fleet +1 STD | 164 | 320 | −207 | 66 | 38 |
| Mockup A | 130 | 250 | −160 | 51 | 37 |
| Mockup B | 60 | 220 | −200 | 73 | 42 |
| Mockup C | 155 | 225 | −137 | 41 | 31 |
| Group 1 | Group 2 | Group 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| (4 Boys, 5 Girls) | (4 Boys, 4 Girls) | (5 Boys, 3 Girls) | |||||||
| Measurement | Mean | Min | Max | Mean | Min | Max | Mean | Min | Max |
| Age (year) | 7 | 4 | 9 | 7 | 4 | 10 | 7 | 4 | 11 |
| Stature (mm) | 1241 | 993 | 1416 | 1222 | 1080 | 1339 | 1251 | 1087 | 1405 |
| Weight (kg) | 26.9 | 15.5 | 53.9 | 25.0 | 19.5 | 35.2 | 27.5 | 17.4 | 41.7 |
| Erect Sitting Height (mm) | 666 | 567 | 765 | 651 | 594 | 693 | 664 | 592 | 726 |
| Body Mass Index (kg/m2) | 17.1 | 14.3 | 30.7 | 16.6 | 14.2 | 19.8 | 17.2 | 14.5 | 21.2 |
| Booster | Fore-Aft Hip X Position | Vertical Hip Z Position | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| re 6YO ATD (Hip X) | re 6YO ATD (Hip Z) | |||||||||||
| Mockup A | Mockup B | Mockup C | Mockup A | Mockup B | Mockup C | |||||||
| Mean (SD) | PW | Mean (SD) | PW | Mean (SD) | PW | Mean (SD) | PW | Mean (SD) | PW | Mean (SD) | PW | |
| None | −27 (24) | ab | −18 (29) | b | −20 (29) | a | 23 (18) | a | 19 (14) | a | 26 (21) | a |
| B01 | −46 (26) | c | −27 (22) | b | −51 (19) | c | 12 (15) | ab | 8 (8) | bc | 14 (11) | ab |
| B02 | −41 (20) | bc | −26 (26) | b | −42 (21) | bc | 4 (11) | b | 1 (17) | bc | 9 (10) | bc |
| B03 | −33 (14) | abc | −11 (6) | ab | −25 (9) | ab | −0 (20) | b | −5 (10) | c | 6 (9) | bc |
| B04 | −13 (19) | a | −23 (10) | b | −16 (11) | a | −2 (4) | b | 2 (17) | bc | −9 (15) | bc |
| B05 | −12 (20) | a | −24 (10) | b | −25 (17) | ab | 8 (9) | b | 11 (7) | ab | 7 (16) | c |
| B06 | −9 (13) | a | 0 (11) | a | −17 (12) | a | 0 (9) | b | 0 (7) | bc | 0 (10) | bc |
| Booster | Fore-Aft HeadCG X Position | Vertical HeadCG Z Position | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mockup A | Mockup B | Mockup C | Mockup A | Mockup B | Mockup C | |||||||
| Mean (SD) | PW | Mean (SD) | PW | Mean (SD) | PW | Mean(SD) | PW | Mean (SD) | PW | Mean (SD) | PW | |
| None | 145 (25) | a | 144 (35) | bc | 150 (37) | a | 415 (69) | d | 429 (51) | d | 420 (51) | e |
| B01 | 156 (28) | a | 187 (38) | a | 159 (33) | a | 467 (75) | c | 462 (44) | cd | 475 (57) | d |
| B02 | 160 (21) | a | 159 (25) | ab | 155 (44) | a | 517 (49) | bc | 513 (21) | bc | 509 (33) | cd |
| B03 | 108 (55) | b | 133 (25) | bcd | 118 (58) | abc | 533 (41) | ab | 505 (51) | bc | 530 (52) | cd |
| B04 | 147 (26) | a | 119 (50) | cde | 145 (54) | ab | 545 (47) | ab | 557 (44) | ab | 541 (70) | bc |
| B05 | 97 (34) | b | 90 (26) | e | 96 (51) | c | 582 (44) | a | 604 (49) | a | 600 (70) | a |
| B06 | 126 (15) | ab | 113 (16) | de | 105 (20) | bc | 581 (37) | ab | 603 (44) | a | 602 (46) | ab |
| Booster | Lap Belt X | Lap Belt Z | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mockup A | Mockup B | Mockup C | Mockup A | Mockup B | Mockup C | |||||||
| Mean (SD) | PW | Mean (SD) | PW | Mean (SD) | PW | Mean (SD) | PW | Mean (SD) | PW | Mean (SD) | PW | |
| None | −15 (11) | a | −5 (14) | a | −2 (15) | a | 19 (10) | a | 24 (9) | a | 27 (12) | a |
| B01 | −10 (14) | ab | −12 (12) | ab | −11 (13) | ab | 13 (9) | ab | 12 (11) | b | 13 (8) | bc |
| B02 | −26 (19) | c | −28 (5) | d | −28 (12) | c | 8 (9) | b | 9 (10) | b | 7 (8) | c |
| B03 | −29 (13) | c | −26 (10) | cd | −25 (14) | c | 14 (10) | ab | 9 (12) | b | 19 (9) | ab |
| B04 | −26 (18) | bc | −33 (7) | d | −25 (9) | c | 12 (11) | ab | 13 (8) | b | 11 (5) | bc |
| B05 | −26 (10) | bc | −27 (10) | cd | −28 (7) | c | 10 (7) | b | 14 (9) | b | 16 (12) | bc |
| B06 | −23 (13) | abc | −16 (11) | bc | −20 (9) | bc | 9 (7) | b | 11 (8) | b | 17 (11) | bc |
| Booster | Shoulder Belt Fit | |||||
|---|---|---|---|---|---|---|
| Mockup A | Mockup B | Mockup C | ||||
| Mean (SD) | PW | Mean (SD) | PW | Mean (SD) | PW | |
| None | −9 (15) | e | −7 (16) | e | −13 (15) | b |
| B01 | −3 (18) | e | 6 (13) | de | −3 (16) | b |
| B02 | 67 (18) | a | 31 (15) | abc | 36 (11) | a |
| B03 | 64 (30) | ab | 51 (49) | a | 35 (16) | a |
| B04 | 20 (10) | d | 24 (12) | bcd | 22 (27) | a |
| B05 | 47 (17) | bc | 43 (24) | ab | 34 (21) | a |
| B06 | 30 (31) | cd | 18 (8) | cd | 34 (26) | a |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, M.L.H.; Ebert, S.; Manary, M.A.; Reed, M.P.; Klinich, K.D. Child Posture and Belt Fit in a Range of Booster Configurations. Int. J. Environ. Res. Public Health 2020, 17, 810. https://doi.org/10.3390/ijerph17030810
Jones MLH, Ebert S, Manary MA, Reed MP, Klinich KD. Child Posture and Belt Fit in a Range of Booster Configurations. International Journal of Environmental Research and Public Health. 2020; 17(3):810. https://doi.org/10.3390/ijerph17030810
Chicago/Turabian StyleJones, Monica L.H., Sheila Ebert, Miriam A. Manary, Matthew P. Reed, and Kathleen D. Klinich. 2020. "Child Posture and Belt Fit in a Range of Booster Configurations" International Journal of Environmental Research and Public Health 17, no. 3: 810. https://doi.org/10.3390/ijerph17030810
APA StyleJones, M. L. H., Ebert, S., Manary, M. A., Reed, M. P., & Klinich, K. D. (2020). Child Posture and Belt Fit in a Range of Booster Configurations. International Journal of Environmental Research and Public Health, 17(3), 810. https://doi.org/10.3390/ijerph17030810