Implementation of KEIGAAF in Primary Schools: A Mutual Adaptation Physical Activity and Nutrition Intervention

 ,
,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
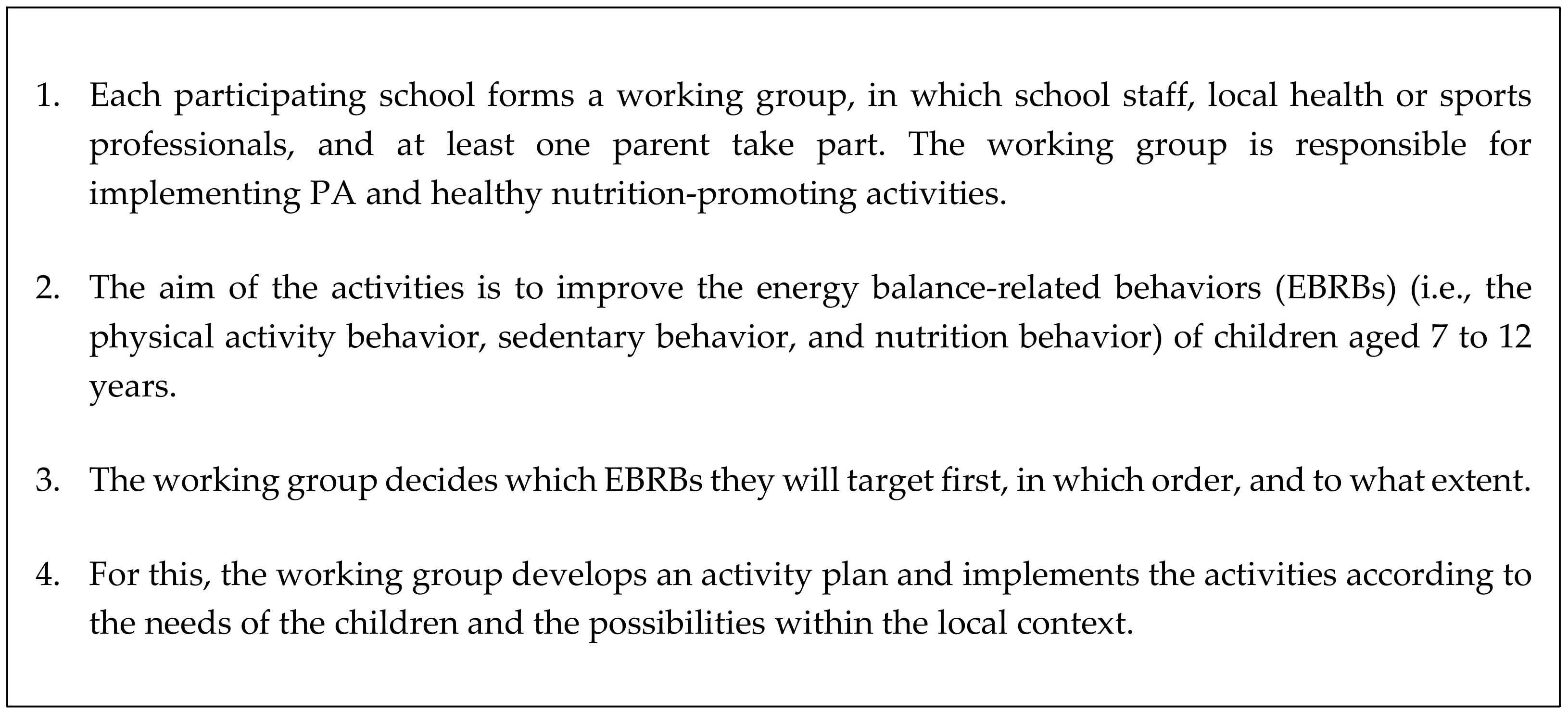
2.2. The KEIGAAF Intervention
2.3. Study Setting and Study Population
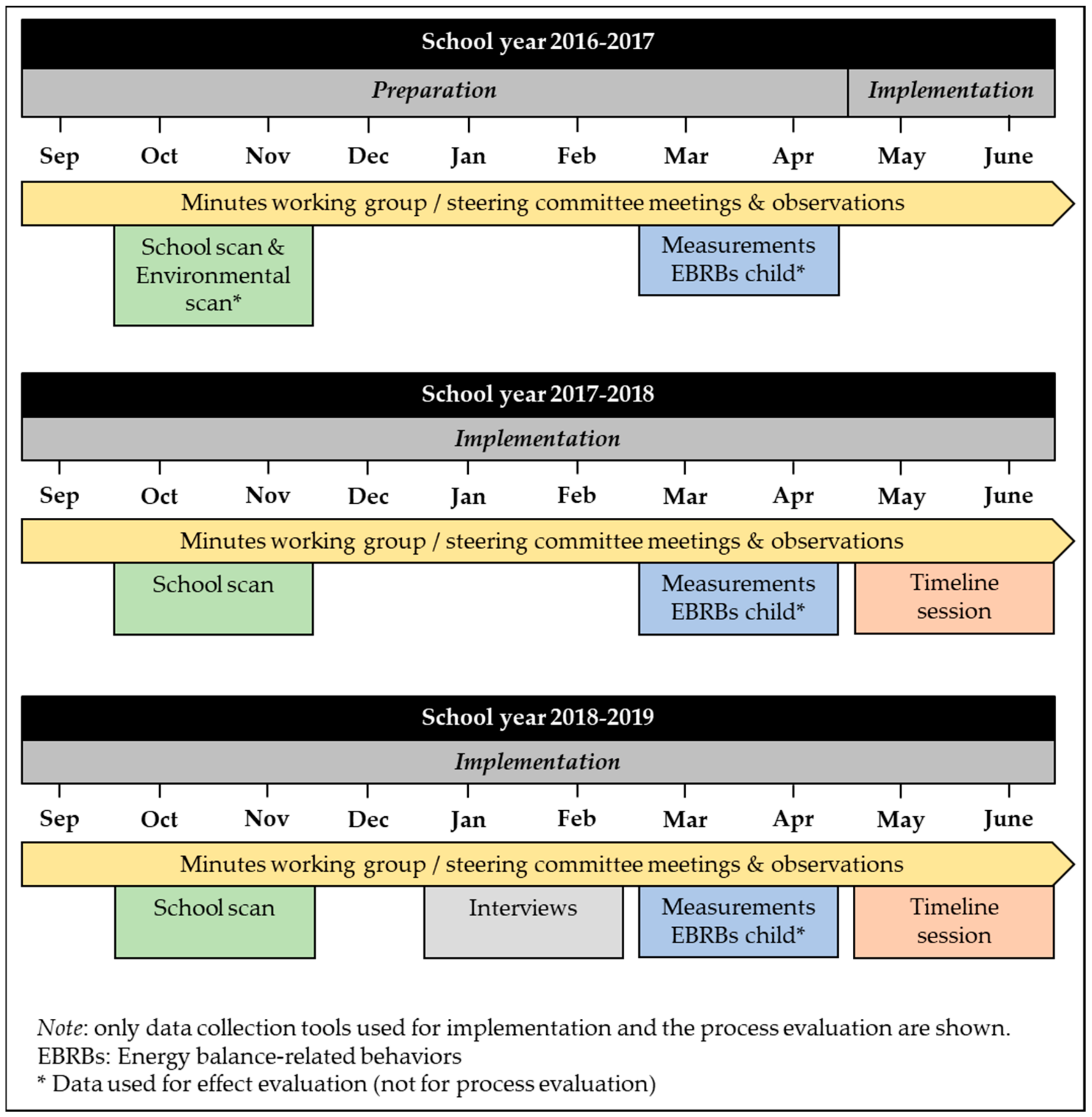
2.4. Data Collection
2.4.1. Minutes of Working Group Meetings and Participatory Observations
2.4.2. School Scan
2.4.3. Timeline Sessions
2.4.4. Semi-Structured Interviews
2.5. Data Coding and Analysis
3. Results
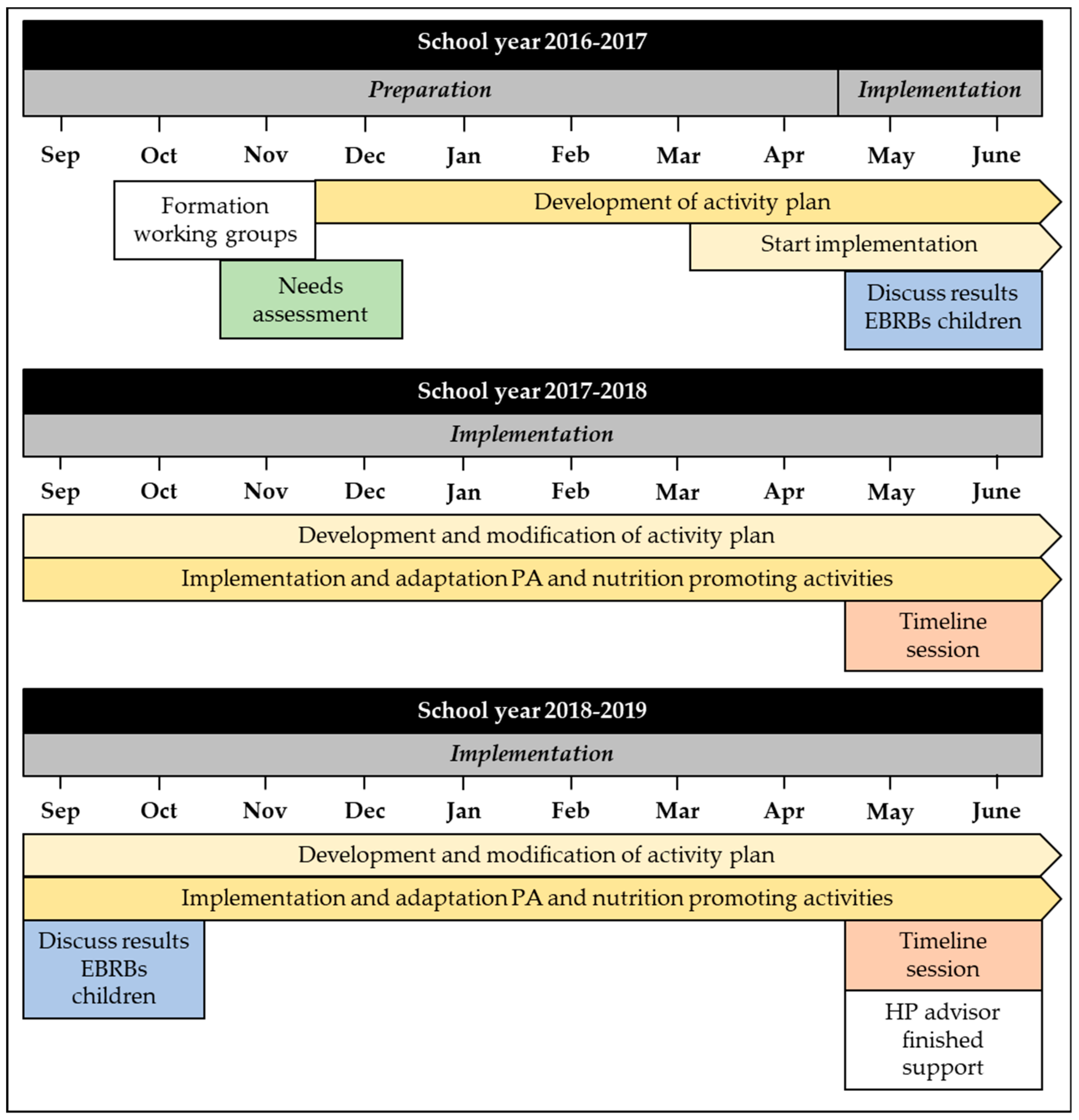
3.1. Implementation of the KEIGAAF Intervention
3.1.1. Formation of Working Group
3.1.2. Development of Activity Plans
3.1.3. Implementation of Activity Plans
3.1.4. Guarantee Sustainability
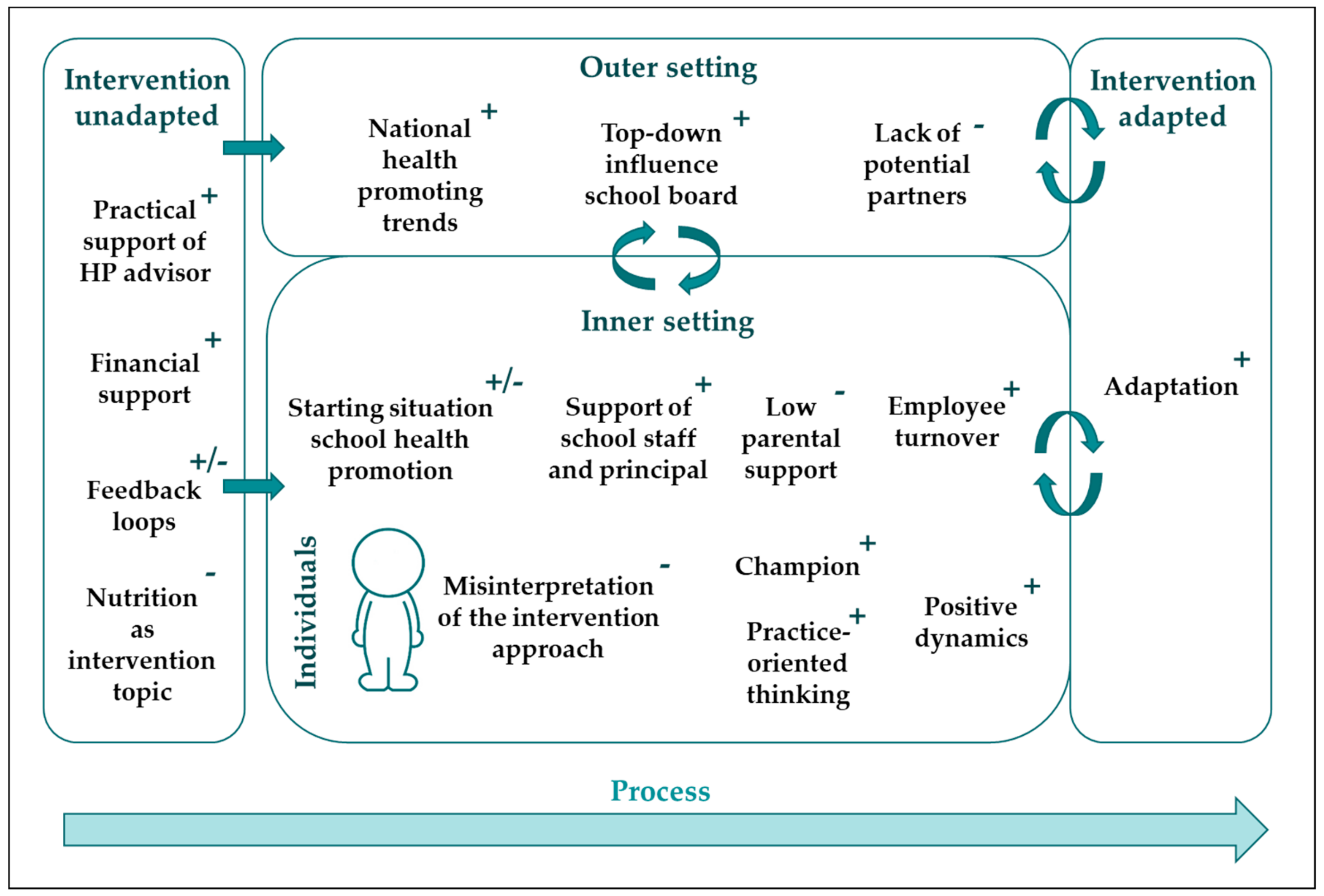
3.2. Factors Influencing the Implementation of the KEIGAAF Intervention
3.2.1. Intervention: Unadapted
Practical Support of HP Advisor and Financial Support
Feedback Loops
Nutrition as Intervention Topic
3.2.2. Outer Setting
National Health-Promoting Trends
Top-Down Influence of School Boards
Lack of Potential Partners
3.2.3. Inner Setting (Schools)
Starting Situation of Schools
Low Parental Support
Support of School Staff and Principal
Employee Turnover
3.2.4. Individuals (Working Group)
Misinterpretation of the Intervention
Practice-Oriented Thinking
Champion
Positive Dynamics
3.2.5. Intervention: Adapted
Adaptation
4. Discussion
Strengths and Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Langford, R.; Bonell, C.P.; Jones, H.E.; Pouliou, T.; Murphy, S.M.; Waters, E.; Komro, K.A.; Gibbs, L.F.; Magnus, D.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Brown, T.; Summerbell, C. Systematic review of school-based interventions that focus on changing dietary intake and physical activity levels to prevent childhood obesity: an update to the obesity guidance produced by the National Institute for Health and Clinical Excellence. Obes. Rev. 2009, 10, 110–141. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 114. [Google Scholar] [CrossRef] [PubMed]
- De Bourdeaudhuij, I.; Van Cauwenberghe, E.; Spittaels, H.; Oppert, J.M.; Rostami, C.; Brug, J.; Van Lenthe, F.; Lobstein, T.; Maes, L. School-based interventions promoting both physical activity and healthy eating in Europe: A systematic review within the HOPE project. Obes. Rev. 2011, 12, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Dobbins, M.; Husson, H.; DeCorby, K.; LaRocca, R.L. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.E.; Christian, M.S.; Cleghorn, C.L.; Greenwood, D.C.; Cade, J.E. Systematic review and meta-analysis of school-based interventions to improve daily fruit and vegetable intake in children aged 5 to 12 y. Am. J. Clin. Nutr. 2012, 96, 889–901. [Google Scholar] [CrossRef] [PubMed]
- Hersch, D.; Perdue, L.; Ambroz, T.; Boucher, J.L. The Impact of Cooking Classes on Food-Related Preferences, Attitudes, and Behaviors of School-Aged Children: A Systematic Review of the Evidence, 2003–2014. Prev. Chronic Dis. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Love, R.; Adams, J.; van Sluijs, E.M.F. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes. Rev. 2019, 20, 859–870. [Google Scholar] [CrossRef]
- Parrish, A.M.; Okely, A.D.; Stanley, R.M.; Ridgers, N.D. The effect of school recess interventions on physical activity: A systematic review. Sports Med. 2013, 43, 287–299. [Google Scholar] [CrossRef]
- Van Cauwenberghe, E.; Maes, L.; Spittaels, H.; van Lenthe, F.J.; Brug, J.; Oppert, J.M.; De Bourdeaudhuij, I. Effectiveness of school-based interventions in Europe to promote healthy nutrition in children and adolescents: Systematic review of published and ‘grey’ literature. Br. J. Nutr. 2010, 103, 781–797. [Google Scholar] [CrossRef]
- Verjans-Janssen, S.R.B.; van de Kolk, I.; Van Kann, D.H.H.; Kremers, S.P.J.; Gerards, S. Effectiveness of school-based physical activity and nutrition interventions with direct parental involvement on children’s BMI and energy balance-related behaviors—A systematic review. PLoS ONE 2018, 13, e0204560. [Google Scholar] [CrossRef] [PubMed]
- Durlak, J.A.; DuPre, E.P. Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am. J. Community Psychol. 2008, 41, 327–350. [Google Scholar] [CrossRef] [PubMed]
- Naylor, P.J.; Nettlefold, L.; Race, D.; Hoy, C.; Ashe, M.C.; Wharf Higgins, J.; McKay, H.A. Implementation of school based physical activity interventions: A systematic review. Prev. Med. 2015, 72, 95–115. [Google Scholar] [CrossRef] [PubMed]
- Langford, R.; Bonell, C.; Jones, H.; Campbell, R. Obesity prevention and the Health promoting Schools framework: Essential components and barriers to success. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 15. [Google Scholar] [CrossRef]
- Craig, P.; Di Ruggiero, E.; Frohlich, K.; On behalf of the Canadian Institutes of Health Research (CIHR) National Institute for Health Research (NIHR) Context Guidance Authors Group. Taking Account of Context in Population Health Intervention Research: Guidance for Producers, Users and Funders of Research; NIHR Evaluation, Trials and Studies Coordinating Centre: Southampton, UK, 2018; pp. 1–68. [Google Scholar] [CrossRef]
- Patton, M.Q. Developmental Evaluation: Applying Complexity Concepts to Enhance Innovation and Use; Guilford Press: New York, NY, USA, 2011; ISBN 978-1-60623-872-1. [Google Scholar]
- Hawe, P. Lessons from complex interventions to improve health. Annu. Rev. Public Health 2015, 36, 307–323. [Google Scholar] [CrossRef]
- Hawe, P.; Shiell, A.; Riley, T. Theorising interventions as events in systems. Am. J. Community Psychol. 2009, 43, 267–276. [Google Scholar] [CrossRef]
- Moore, G.F.; Evans, R.E.; Hawkins, J.; Littlecott, H.; Melendez-Torres, G.J.; Bonell, C.; Murphy, S. From complex social interventions to interventions in complex social systems: Future directions and unresolved questions for intervention development and evaluation. Evaluation 2019, 25, 23–45. [Google Scholar] [CrossRef]
- Pearson, M.; Chilton, R.; Wyatt, K.; Abraham, C.; Ford, T.; Woods, H.B.; Anderson, R. Implementing health promotion programmes in schools: A realist systematic review of research and experience in the United Kingdom. Implement. Sci. 2015, 10, 149. [Google Scholar] [CrossRef]
- Turunen, H.; Sormunen, M.; Jourdan, D.; von Seelen, J.; Buijs, G. Health Promoting Schools-a complex approach and a major means to health improvement. Health Promot. Int. 2017, 32, 177–184. [Google Scholar] [CrossRef]
- Verjans-Janssen, S.R.B.; Van Kann, D.H.H.; Gerards, S.; Vos, S.B.; Jansen, M.W.J.; Kremers, S.P.J. Study protocol of the quasi-experimental evaluation of “KEIGAAF”: A context-based physical activity and nutrition intervention for primary school children. BMC Public Health 2018, 18, 842. [Google Scholar] [CrossRef]
- Yin, R. Case Study Research: Design and Methods, 4th ed.; Sage: Los Angeles, CA, USA, 2009; Volume 5. [Google Scholar]
- Van Kann, D.H.; Jansen, M.W.; de Vries, S.I.; de Vries, N.K.; Kremers, S.P. Active Living: Development and quasi-experimental evaluation of a school-centered physical activity intervention for primary school children. BMC Public Health 2015, 15, 1315. [Google Scholar] [CrossRef] [PubMed]
- Hills, A.P.; Dengel, D.R.; Lubans, D.R. Supporting public health priorities: Recommendations for physical education and physical activity promotion in schools. Prog. Cardiovasc. Dis. 2015, 57, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [PubMed]
- Tabak, R.G.; Khoong, E.C.; Chambers, D.A.; Brownson, R.C. Bridging research and practice: Models for dissemination and implementation research. Am. J. Prev. Med. 2012, 43, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Slingerland, M.; Vervoort, J.; Verheijen, S. Brabantse Basisscholen in Beweging: Twee vliegen in 1 klap! Thomas Bulletin. 2013, 73, 39–41. [Google Scholar]
- Herens, M.; Wagemakers, A.; Vaandrager, L.; van Ophem, J.; Koelen, M. Contexts, Mechanisms, and Outcomes That Matter in Dutch Community-Based Physical Activity Programs Targeting Socially Vulnerable Groups. Eval. Health Prof. 2017, 40, 294–331. [Google Scholar] [CrossRef]
- Thomas, D.R. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- RIVM Centrum Gezond Leven; GGD GHOR; MBO Raad; PO-Raad; VO-raad. Gezonde School. Available online: https://www.gezondeschool.nl/ (accessed on 24 November 2019).
- Wageningen University & Research. EU-schoolfruit. Available online: https://www.euschoolfruit.nl/nl/schoolfruit.htm (accessed on 24 November 2019).
- Boot, N.; van Assema, P.; Hesdahl, B.; de Vries, N. Professional assistance in implementing school health policies. Health Educ. 2010, 110, 294–308. [Google Scholar] [CrossRef]
- Day, R.E.; Sahota, P.; Christian, M.S. Effective implementation of primary school-based healthy lifestyle programmes: A qualitative study of views of school staff. BMC Public Health 2019, 19, 1239. [Google Scholar] [CrossRef]
- Leo, U.; Wickenberg, P. Professional norms in school leadership: Change efforts in implementation of education for sustainable development. J. Educ. Chang. 2013, 14, 403–422. [Google Scholar] [CrossRef]
- McIsaac, J.L.; Hernandez, K.J.; Kirk, S.F.; Curran, J.A. Interventions to Support System-level Implementation of Health Promoting Schools: A Scoping Review. Int. J. Environ. Res. Public Health 2016, 13, 200. [Google Scholar] [CrossRef] [PubMed]
- Orava, T.; Manske, S.; Hanning, R. Support for healthy eating at schools according to the comprehensive school health framework: Evaluation during the early years of the Ontario School Food and Beverage Policy implementation. Health Promot. Chronic Dis. Prev. Can. 2017, 37, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Roberts, E.; McLeod, N.; Montemurro, G.; Veugelers, P.J.; Gleddie, D.; Storey, K.E. Implementing Comprehensive School Health in Alberta, Canada: The principal’s role. Health Promot. Int. 2016, 31, 915–924. [Google Scholar] [CrossRef] [PubMed]
- Samdal, O.; Rowling, L. Theoretical and empirical base for implementation components of health-promoting schools. Health Educ. 2011, 111, 367–390. [Google Scholar] [CrossRef]
- Storey, K.E.; Montemurro, G.; Flynn, J.; Schwartz, M.; Wright, E.; Osler, J.; Veugelers, P.J.; Roberts, E. Essential conditions for the implementation of comprehensive school health to achieve changes in school culture and improvements in health behaviours of students. BMC Public Health 2016, 16, 1133. [Google Scholar] [CrossRef] [PubMed]
- Wolk, C.B.; Stewart, R.E.; Eiraldi, R.; Cronholm, P.; Salas, E.; Mandell, D.S. The implementation of a team training intervention for school mental health: Lessons learned. Psychotherapy 2019, 56, 83–90. [Google Scholar] [CrossRef]
- Lucarelli, J.F.; Alaimo, K.; Mang, E.; Martin, C.; Miles, R.; Bailey, D.; Kelleher, D.K.; Drzal, N.B.; Liu, H. Facilitators to promoting health in schools: Is school health climate the key? J. Sch. Health 2014, 84, 133–140. [Google Scholar] [CrossRef]
- Rowling, L.; Samdal, O. Filling the black box of implementation for health-promoting schools. Health Educ. 2011, 111, 347–366. [Google Scholar] [CrossRef]
- McLaughlin, M.W. The Rand Change Agent Study revisited: Macro perspectives and micro realities. Educ. Res. 1990, 19, 11–16. [Google Scholar] [CrossRef]
- Evans, R.E.; Craig, P.; Hoddinott, P.; Littlecott, H.; Moore, L.; Murphy, S.; Cathain, A.; Pfadenhauer, L.; Rehfuess, E.; Segrott, J.; et al. When and how do ‘effective’ interventions need to be adapted and/or re-evaluated in new contexts? The need for guidance. J. Epidemiol. Community Health 2019, 73, 481. [Google Scholar] [CrossRef]
- Shoveller, J.; Viehbeck, S.; Di Ruggiero, E.; Greyson, D.; Thomson, K.; Knight, R. A critical examination of representations of context within research on population health interventions. Crit. Public Health 2016, 26, 487–500. [Google Scholar] [CrossRef]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verjans-Janssen, S.R.B.; Gerards, S.M.P.L.; Verhees, A.H.; Kremers, S.P.J.; Vos, S.B.; Jansen, M.W.J.; Van Kann, D.H.H. Implementation of KEIGAAF in Primary Schools: A Mutual Adaptation Physical Activity and Nutrition Intervention. Int. J. Environ. Res. Public Health 2020, 17, 751. https://doi.org/10.3390/ijerph17030751
Verjans-Janssen SRB, Gerards SMPL, Verhees AH, Kremers SPJ, Vos SB, Jansen MWJ, Van Kann DHH. Implementation of KEIGAAF in Primary Schools: A Mutual Adaptation Physical Activity and Nutrition Intervention. International Journal of Environmental Research and Public Health. 2020; 17(3):751. https://doi.org/10.3390/ijerph17030751
Chicago/Turabian StyleVerjans-Janssen, Sacha R.B., Sanne M.P.L. Gerards, Anke H. Verhees, Stef P.J. Kremers, Steven B. Vos, Maria W.J. Jansen, and Dave H.H. Van Kann. 2020. "Implementation of KEIGAAF in Primary Schools: A Mutual Adaptation Physical Activity and Nutrition Intervention" International Journal of Environmental Research and Public Health 17, no. 3: 751. https://doi.org/10.3390/ijerph17030751
APA StyleVerjans-Janssen, S. R. B., Gerards, S. M. P. L., Verhees, A. H., Kremers, S. P. J., Vos, S. B., Jansen, M. W. J., & Van Kann, D. H. H. (2020). Implementation of KEIGAAF in Primary Schools: A Mutual Adaptation Physical Activity and Nutrition Intervention. International Journal of Environmental Research and Public Health, 17(3), 751. https://doi.org/10.3390/ijerph17030751