10-Year Rotavirus Infection Surveillance: Epidemiological Trends in the Pediatric Population of Perugia Province

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rotavirus. Available online: http://www.who.int/immunization/diseases/rotavirus/en/ (accessed on 22 December 2019).
- GBD 2016 Diarrhoeal Disease Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar]
- Soriano-Gabarró, M.; Mrukowicz, J.; Vesikari, T.; Verstraeten, T. Burden of rotavirus disease in European Union countries. Pediatr. Infect. Dis. J. 2006, 25, S7–S11. [Google Scholar]
- Desselberger, U. Rotaviruses. Virus Res. 2014, 190, 75–96. [Google Scholar]
- Estes, M.K.; Greenberg, H.B. Rotaviruses. In Fields Virology; Knipe, D., Howley, P., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013; pp. 1347–1401. [Google Scholar]
- Bányai, K.; Kemenesi, G.; Budinski, I.; Földes, F.; Zana, B.; Marton, S.; Varga-Kugler, R.; Oldal, M.; Kurucz, K.; Jakab, F. Candidate new rotavirus species in Schreiber’s bats, Serbia. Infect. Genet. Evol. 2017, 48, 19–26. [Google Scholar]
- Disease Factsheet about Rotavirus. Available online: https://www.ecdc.europa.eu/en/rotavirus-infection/facts (accessed on 22 December 2019).
- Epidemiology of Vaccine Preventable Diseases. Available online: https://www.cdc.gov/vaccines/pubs/pinkbook/rota.html (accessed on 22 December 2019).
- Gentsch, J.R.; Laird, A.R.; Bielfelt, B.; Griffin, D.D.; Banyai, K.; Ramachandran, M.; Jain, V.; Cunliffe, N.A.; Nakagomi, O.; Kirkwood, C.D.; et al. Serotype diversity and reassortment between human and animal rotavirus strains: Implications for rotavirus vaccine programs. J. Infect. Dis. 2005, 192 (Suppl. 1), S146–S159. [Google Scholar]
- Bányai, K.; László, B.; Duque, J.; Steele, A.D.; Nelson, E.A.S.; Gentsch, J.R.; Parashar, U.D. Systematic Review of Regional and Temporal Trends in Global Rotavirus Strain Diversity in the Pre Rotavirus Vaccine Era: Insights for Understanding the Impact of Rotavirus Vaccination Programs. Vaccine 2012, 30 (Suppl. 1), A122–A130. [Google Scholar]
- Dóró, R.; László, B.; Martella, V.; Leshem, E.; Gentsch, J.; Parashar, U.; Bányai, K. Review of global rotavirus strain prevalence data from six years post vaccine licensure surveillance: Is there evidence of strain selection from vaccine pressure? Infect. Genet. Evol. 2014, 28, 446–461. [Google Scholar]
- Mullick, S.; Mandal, P.; Nayak, M.K.; Ghosh, S.; De, P.; Rajendran, K.; Bhattacharya, M.K.; Mitra, U.; Ramamurthy, T.; Kobayashi, N.; et al. Hospital Based Surveillance and Genetic Characterization of Rotavirus Strains in Children (<5 years) with Acute Gastroenteritis in Kolkata, India, revealed Resurgence of G9 and G2 Genotypes during 2011–2013. Vaccine 2014, 32, A20–A28. [Google Scholar]
- Tiku, V.R.; Sharma, S.; Verma, A.; Kumar, P.; Raghavendhar, S.; Aneja, S.; Paul, V.K.; Bhan, M.K.; Ray, P. Rotavirus Diversity among Diarrheal Children in Delhi, India during 2007–2012. Vaccine 2014, 32 (Suppl. 1), A62–A67. [Google Scholar]
- Sharma, S.; Paul, V.K.; Bhan, M.K.; Ray, P. Genomic characterization of nontypeable rotaviruses and detection of a rare G8 strain in Delhi, India. J. Clin. Microbiol. 2009, 47, 3998–4005. [Google Scholar]
- Kaplon, J.; Grangier, N.; Pillet, S.; Minoui-Tran, A.; Vabret, A.; Wilhelm, N.; Prieur, N.; Lazrek, M.; Alain, S.; Mekki, Y.; et al. Predominance of G9P[8] rotavirus strains throughout France, 2014–2017. Clin. Microbiol. Infect. 2018, 24, 660. [Google Scholar]
- Jain, S.; Vashistt, J.; Changotra, H. Rotaviruses: Is Their Surveillance Needed? Vaccine 2014, 32, 3367–3378. [Google Scholar]
- Gasparinho, C.; Piedade, J.; Mirante, M.C.; Mendes, C.; Mayer, C.; Vaz Nery, S.; Brito, M.; Istrate, C. Characterization of rotavirus infection in children with acute gastroenteritis in Bengo province, Northwestern Angola, prior to vaccine introduction. PLoS ONE 2017, 12, e0176046. [Google Scholar]
- WHO. Meeting of the Strategic Advisory Group of Experts on immunization, October 2009—Conclusions and recommendations. Wkly. Epidemiol. Rec. 2009, 84, 517–532. [Google Scholar]
- World Health Organization. Rotavirus vaccines: WHO position paper—January 2013 = Vaccins antirotavirus: Note de synthèse de l’OMS. Wkly. Epidemiol. Rec. 2013, 88, 49–64. [Google Scholar]
- Amodio, E.; Costantino, C.; Cracchiolo, M.; Sciuto, V.; Vitale, F. Esperienze italiane ed europee sulla vaccinazione anti-rotavirus: L’esperienza della Sicilia quale regione capofila nell’introduzione della vaccinazione universale contro i rotavirus. QIJPH 2014, 3, 28–37. [Google Scholar]
- De Grazia, S.; Bonura, F.; Colomba, C.; Cascio, A.; Di Bernardo, F.; Collura, A.; Terranova, D.M.; Martella, V.; Giammanco, G.M. Data mining from a 27-years rotavirus surveillance in Palermo, Italy. Infect. Genet. Evol. 2014, 28, 377–384. [Google Scholar]
- Ianiro, G.; Micolano, R.; Di Bartolo, I.; Scavia, G.; Monini, M.; RotaNet-Italy Study Group. Group A rotavirus surveillance before vaccine introduction in Italy, September 2014 to August 2017. Euro. Surveill. 2019, 24. [Google Scholar] [CrossRef]
- Demo Istat. Available online: http://demo.istat.it/pop2019/index.html (accessed on 22 December 2019).
- National Institute of Health. Available online: http://old.iss.it/criv/?lang=1&id=363&tipo=9 (accessed on 22 December 2019).
- European Rotavirus Network. Available online: www.eurorotanet.com (accessed on 22 December 2019).
- The Pediatric ROTavirus European CommitTee (PROTECT). The paediatric burden of rotavirus disease in Europe. Epidemiol. Infect. 2006, 134, 908–916. [Google Scholar]
- Forster, J.; Guarino, A.; Parez, N.; Moraga, F.; Román, E.; Mory, O.; Tozzi, A.E.; de Aguileta, A.L.; Wahn, U.; Graham, C.; et al. Hospital-based surveillance to estimate the burden of rotavirus gastroenteritis among European children younger than 5 years of age. Pediatrics 2009, 123, e393–e400. [Google Scholar]
- Mattei, A.; Angelone, A.M.; Michetti, M.; Sbarbati, M.; Ceci, R.; Murgano, A.; di Orio, F. Epidemiological impact of RV gastroenteritis in the Abruzzo Region: SDO analysis. Ann. Ig. 2009, 21, 41–49. [Google Scholar]
- Gabutti, G.; Marsella, M.A.; Lazzara, C.; Fiumana, E.; Cavallaro, A.; Borgna-Pignatti, C. Epidemiology and burden of rotavirus-associated hospitalizations in Ferrara, Italy. J. Prev. Med. Hyg. 2007, 48, 5–9. [Google Scholar]
- Pellegrinelli, L.; Bubba, L.; Primache, V.; Chiaramonte, I.; Ruggeri, F.M.; Fiore, L.; Binda, S. Burden of pediatrics hospitalizations associated with Rotavirus gastroenteritis in Lombardy (Northern Italy) before immunization program. Ann. Ist. Super. Sanita 2015, 51, 346–351. [Google Scholar]
- Marchetti, F.; Assael, B.; Gabutti, G. Monitoring the rate of hospitalization before rotavirus immunization in Italy utilizing ICD9-CM regional databases. Hum Vaccin. 2009, 5, 1–5. [Google Scholar]
- Zuccotti, G.; Meneghin, F.; Dilillo, D.; Romanò, L.; Bottone, R.; Mantegazza, C.; Giacchino, R.; Besana, R.; Ricciardi, G.; Sterpa, A.; et al. Epidemiological and clinical features of rotavirus among children younger than 5 years of age hospitalized with acute gastroenteritis in Northern Italy. BMC Infect. Dis. 2010, 10, 218. [Google Scholar]
- De Donno, A.; Grassi, T.; Bagordo, F.; Idolo, A.; Cavallaro, A.; Gabutti, G.; Collaborative Group for the Surveillance of Rotavirus Infection. Emergence of unusual human rotavirus strains in Salento, Italy, during 2006–2007. BMC Infect. Dis. 2009, 9, 43. [Google Scholar]
- Panatto, D.; Amicizia, D.; Giacchino, R.; Tacchella, A.; Natalizia, A.R.; Melioli, G.; Bandettini, R.; Di Pietro, P.; Diana, M.C.; Gasparini, R. Burden of rotavirus infections in Liguria, Northern Italy: Hospitalisations and potential savings by vaccination. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 957–964. [Google Scholar]
- Patel, M.M.; Tate, J.E.; Selvarangan, R.; Daskalaki, I.; Jackson, M.A.; Curns, A.T.; Coffin, S.; Watson, B.; Hodinka, R.; Glass, R.I.; et al. Routine laboratory testing data for surveillance of rotavirus hospitalizations to evaluate the impact of vaccination. Pediatr. Infect. Dis. J. 2007, 26, 914–919. [Google Scholar]
- Kimura, T.; Okabe, N. Passive surveillance of rotavirus gastroenteritis-associated hospitalization using nationwide administrative databases in Japan. J. Infect. Chemother. 2019, 25, 175–181. [Google Scholar]
- Steele, A.D.; Madhi, S.A.; Cunliffe, N.A.; Vesikari, T.; Phua, K.B.; Lim, F.S.; Nelson, E.A.S.; Lau, Y.-L.; Huang, L.-M.; Karkada, N.; et al. Incidence of rotavirus gastroenteritis by age in African, Asian and European children: Relevance for timing of rotavirus vaccination. Hum. Vaccin. Immunother. 2016, 12, 2406–2412. [Google Scholar]
- Ogilvie, I.; Khoury, H.; Goetghebeur, M.M.; El Khoury, A.C.; Giaquinto, C. Burden of community-acquired and nosocomial rotavirus gastroenteritis in the pediatric population of Western Europe: A scoping review. BMC Infect. Dis. 2012, 12, 62. [Google Scholar]
- Delogu, R.; Ianiro, G.; Camilloni, B.; Fiore, L.; Rugger, F.M. Unexpected spreading of G12P[8] rotavirus strains among young children in a small area of central Italy. J. Med. Virol. 2015, 87, 1292–1302. [Google Scholar]
- Impact of Rotavirus Vaccination—Generic Study Protocol. ECDC: Stockholm. 2013. Available online: https://www.ecdc.europa.eu/sites/default/files/media/en/publications/Publications/Rotavirus-impact-vaccination-April-2013.pdf (accessed on 22 December 2019).

{kind=link}
| RV Season | 0–15 y | Males 0–15 y | Females 0–15 y | 0–5 y | Males 0–5 y | Females 0–5 y |
|---|---|---|---|---|---|---|
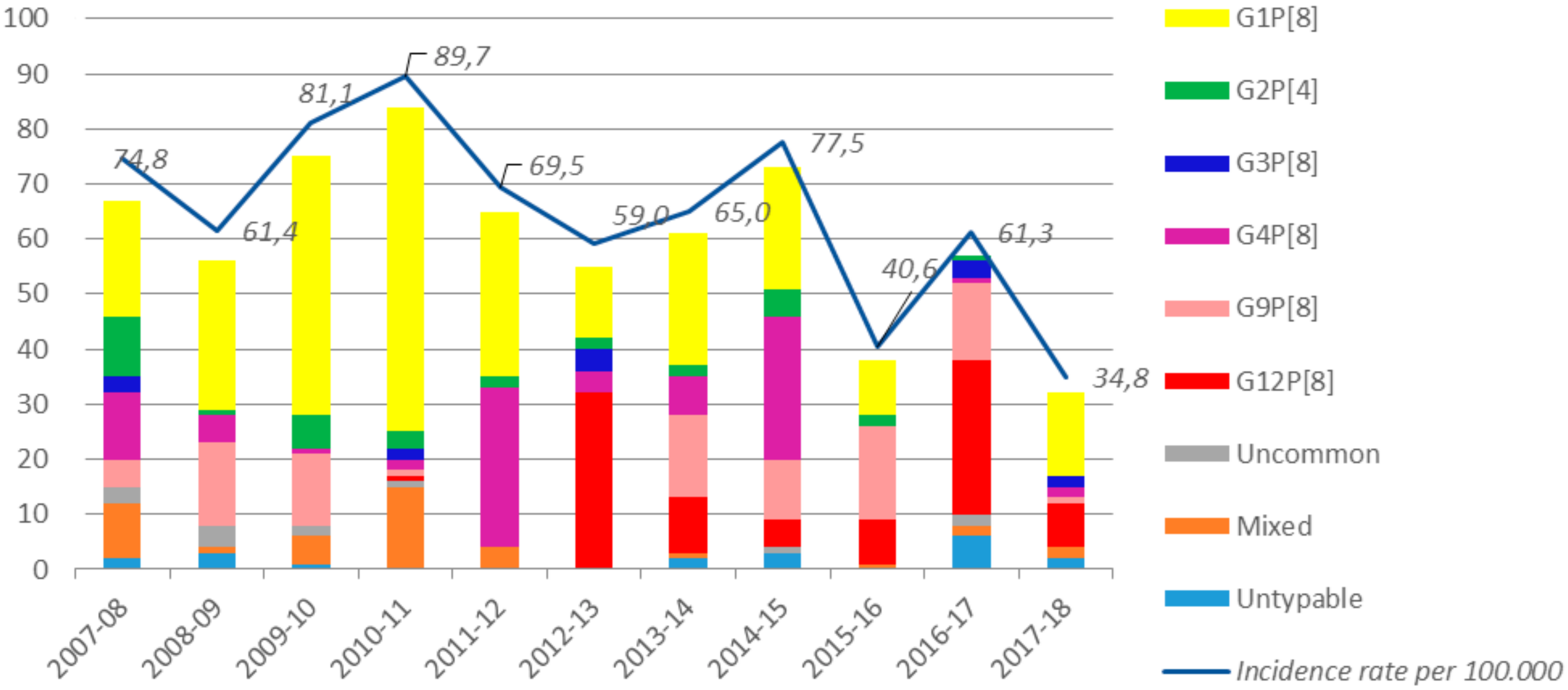
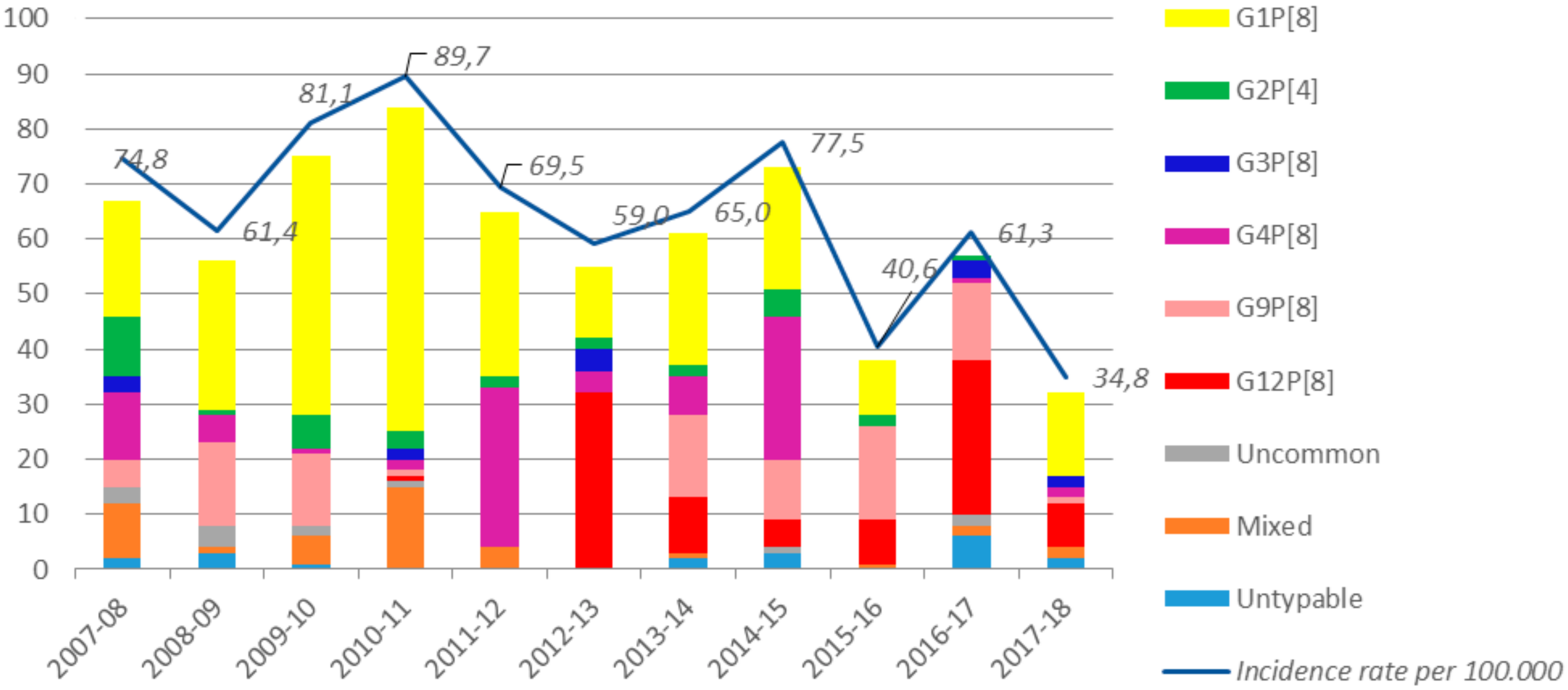
| 2007–2008 | 74.8 | 84.4 | 64.6 | 198.9 | 218.8 | 177.9 |
| 2008–2009 | 61.4 | 63.8 | 58.9 | 140.1 | 141.5 | 138.5 |
| 2009–2010 | 81.1 | 96.5 | 64.8 | 191.9 | 218.2 | 164.0 |
| 2010–2011 | 89.7 | 113.9 | 64.0 | 222.1 | 289.2 | 150.9 |
| 2011–2012 | 69.5 | 70.5 | 68.3 | 175.0 | 170.2 | 180.1 |
| 2012–2013 | 59.0 | 71.0 | 46.4 | 139.1 | 168.6 | 108.2 |
| 2013–2014 | 65.0 | 74.5 | 54.8 | 148.3 | 169.9 | 125.8 |
| 2014–2015 | 77.5 | 84.6 | 70.0 | 185.4 | 195.4 | 175.0 |
| 2015–2016 | 40.6 | 49.9 | 30.7 | 91.3 | 115.2 | 66.2 |
| 2016–2017 | 61.3 | 67.1 | 55.3 | 142.6 | 142.6 | 142.5 |
| 2017–2018 | 34.8 | 44.5 | 24.6 | 81.6 | 116.8 | 44.9 |
| RV Season | G12P[8] | G1P[8] | G2P[4] | G3P[8] | G4P[8] | G9P[8] | Uncommon | Mixed | Non-Typable | Tot ** |
|---|---|---|---|---|---|---|---|---|---|---|
| 2007–08 | 0 (0.0%) | 21 (31.3%) | 11 (16.4%) | 3 (4.5%) | 12 (17.9%) | 5 (7.5%) | 3 (4.5%) | 10 (14.9%) | 2 (3.0%) | 67 (10.1%) |
| 2008–09 | 0 (0.0%) | 27 (48.2%) | 1 (1.8%) | 0 (0.0%) | 5 (8.9%) | 15 (26.8%) | 4 (7.1%) | 1 (1.8%) | 3 (5.4%) | 56 (8.4%) |
| 2009–10 | 0 (0.0%) | 47 (62.7%) | 6 (8.0%) | 0 (0.0%) | 1 (1.3%) | 13 (17.3%) | 2 (2.7%) | 5 (6.7%) | 1 (1.3%) | 75 (11.3%) |
| 2010–11 | 1 (1.2%) | 59 (70.2%) | 3 (3.6%) | 2 (2.4%) | 2 (2.4%) | 1 (1.2%) | 1 (1.2%) | 15 (17.9%) | 0 (0.0%) | 84 (12.7%) |
| 2011–12 | 0 (0.0%) | 30 (46.2%) | 2 (3.1%) | 0 (0.0%) | 29 (44.6%) | 0 (0.0%) | 0 (0.0%) | 4 (6.2%) | 0 (0.0%) | 65 (9.8%) |
| 2012–13 | 32 (58.2%) | 13 (23.6%) | 2 (3.6%) | 4 (7.3%) | 4 (7.3%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 55 (8.3%) |
| 2013–14 | 10 (16.4%) | 24 (39.3%) | 2 (3.3%) | 0 (0.0%) | 7 (11.5%) | 15 (24.6%) | 0 (0.0%) | 1 (1.6%) | 2 (3.3%) | 61 (9.2%) |
| 2014–15 | 5 (6.8%) | 22 (30.1%) | 5 (6.8%) | 0 (0.0%) | 26 (35.6%) | 11 (15.1%) | 1 (1.4%) | 0 (0.0%) | 3 (4.1%) | 73 (11.0%) |
| 2015–16 | 8 (21.1%) | 10 (26.3%) | 2 (5.3%) | 0 (0.0%) | 0 (0.0%) | 17 (44.7%) | 0 (0.0%) | 1 (2.6%) | 0 (0.0%) | 38 (5.7%) |
| 2016–17 | 28 (49.1%) | 0 (0.0%) | 1 (1.8%) | 3 (5.3%) | 1 (1.8%) | 14 (24.6%) | 2 (3.5%) | 2 (3.5%) | 6 (10.5%) | 57 (8.6%) |
| 2017–18 | 8 (25.0%) | 15 (46.9%) | 0 (0.0%) | 2 (6.3%) | 2 (6.3%) | 1 (3.1%) | 0 (0.0%) | 2 (6.3%) | 2 (6.3%) | 32 (4.8%) |
| Tot * | 92 (13.9%) | 268 (40.4%) | 35 (5.3%) | 14 (2.1%) | 89 (13.4%) | 92 (13.9%) | 13 (2.0%) | 41 (6.2%) | 19 (2.9%) | 663 (100%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Waure, C.; Sarnari, L.; Chiavarini, M.; Ianiro, G.; Monini, M.; Alunno, A.; Camilloni, B. 10-Year Rotavirus Infection Surveillance: Epidemiological Trends in the Pediatric Population of Perugia Province. Int. J. Environ. Res. Public Health 2020, 17, 1008. https://doi.org/10.3390/ijerph17031008
de Waure C, Sarnari L, Chiavarini M, Ianiro G, Monini M, Alunno A, Camilloni B. 10-Year Rotavirus Infection Surveillance: Epidemiological Trends in the Pediatric Population of Perugia Province. International Journal of Environmental Research and Public Health. 2020; 17(3):1008. https://doi.org/10.3390/ijerph17031008
Chicago/Turabian Stylede Waure, Chiara, Laura Sarnari, Manuela Chiavarini, Giovanni Ianiro, Marina Monini, Anna Alunno, and Barbara Camilloni. 2020. "10-Year Rotavirus Infection Surveillance: Epidemiological Trends in the Pediatric Population of Perugia Province" International Journal of Environmental Research and Public Health 17, no. 3: 1008. https://doi.org/10.3390/ijerph17031008
APA Stylede Waure, C., Sarnari, L., Chiavarini, M., Ianiro, G., Monini, M., Alunno, A., & Camilloni, B. (2020). 10-Year Rotavirus Infection Surveillance: Epidemiological Trends in the Pediatric Population of Perugia Province. International Journal of Environmental Research and Public Health, 17(3), 1008. https://doi.org/10.3390/ijerph17031008