How the Chinese Government Has Done with Public Health from the Perspective of the Evaluation and Comparison about Public-Health Expenditure



Abstract
1. Introduction
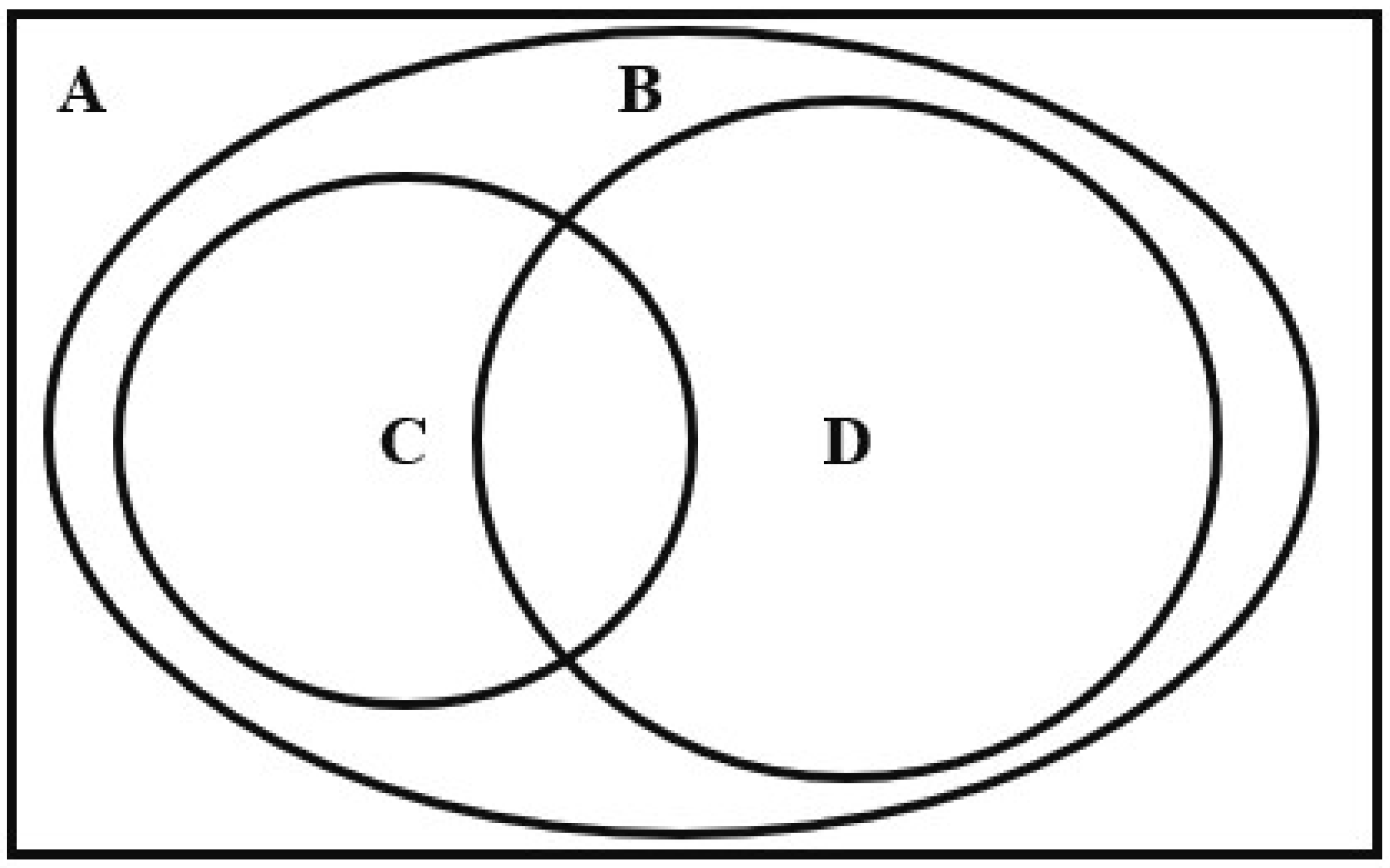
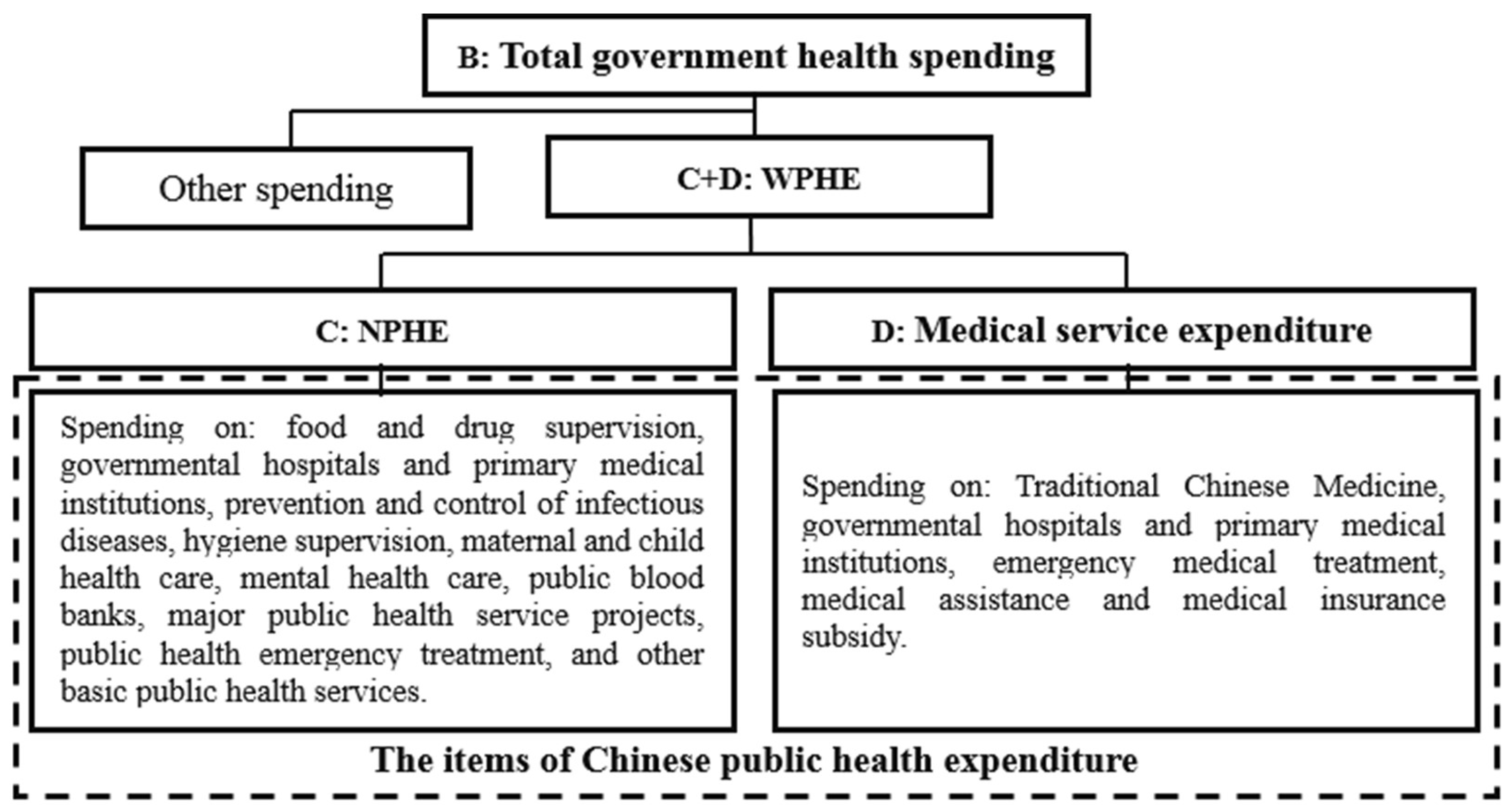
2. Chinese Public-Health Expenditure
3. The Measurement and Comparison of Chinese Public-Health Expenditure
3.1. Method and Data
3.2. The Measurement of Chinese Public-Health Expenditure
3.2.1. National Level
3.2.2. Provincial Level
3.3. The International Comparison of Public-Health Expenditure
4. The Evaluation and Analysis of Chinese Public-Health Expenditure
- (1)
- The scale of public-health expenditure in China is quite low, and pales in comparison with that in developed countries. As the 2014 data in Table 3 shows, the per capita public-health expenditure in China is 103 US dollars, about 1/40 of that in the United States, 1/28 in Japan, and 1/34 in the United Kingdom. The proportion of China’s public-health expenditure in GDP and total fiscal expenditure is also much lower than that of the United States, the United Kingdom, and Japan. In fact, public-health expenditure accounts for the highest proportion of government expenditure in Japan and the United States. But in China, the share of public-health expenditure is less than that of infrastructure construction, education, national defense, urban and rural community affairs, and so on. In addition, compared with the three developing countries, the public-health expenditure level of China is slightly better than that of India, and not as good as Russia and Thailand. The data of 2018 in Table 3 also shows a similar result, that is, the level of public-health expenditure in China is very low and much lower than that in developed countries. This similar result also implies that the Chinese government has not significantly increased its investment in public health in recent years, nor has it paid more attention to public-health affairs.
- (2)
- The Chinese government attaches less importance to public health affairs than other countries do. Firstly, the share of public-health expenditure in fiscal expenditure in China accounts for about for 1/4 of that in the United States and the United Kingdom, and 1/6 of that in Japan. It is slightly better than India, and not as good as Russia and Thailand (see Table 3). Secondly, the share of public-health expenditure in fiscal expenditure in most countries shows an upward trend, but that of China decreases by 0.26%, from 2014–2018. Thirdly, the proportion of China’s public-health expenditure in GDP is also significantly lower than that of the three developed countries, Thailand, and Russia, and has decreased slightly from 2014 to 2018. As is known to all, the tax burden, fiscal expenditure, and GDP of China have all increased sharply in recent years, but the proportion of public-health expenditure in fiscal expenditure and GDP has decreased. It implies that the Chinese government has not paid enough attention to public-health expenditure in recent years.
- (3)
- In cases where there was insufficient attention to major public health emergencies both in quantity and quality, COVID-19 took advantage of such vulnerability and swept over the masses. As is shown in Table 1, it is apparent that Chinese government spending on prevention and control of diseases, major public-health service projects, and public-health emergency treatment is quite low—especially for the public-health emergency treatment, which accounts for less than 0.1% of the public-health expenditure on average in 2014–2018. And this expenditure item shows a fluctuating decline, from 0.8 billion yuan in 2014 to 0.68 billion yuan in 2018. These data reflect the inadequacy of the spending on major public-health emergencies in quantity.
- (4)
- Chinese public-health expenditure shows an increasing trend in recent years, but the increasing rate is too low, and lower than that of GDP and fiscal expenditure. With an average annual growth rate of 8.90%, Chinese public-health expenditure has increased from 864.75 billion yuan in 2014 to 1202.05 billion yuan in 2018 (see Table 1). But the proportion of public-health expenditure in GDP and fiscal expenditure shows a trend of first rising and then decreasing, and it has decreased in general. It means that despite rapid economic growth and government spending increasing, residents in China do not enjoy most of the dividends of economic growth in public health and medical services. As mentioned above, Chinese governments have invested a lot of dividends from economic growth into infrastructure construction in order to seek higher economic growth rate. According to the experience of the COVID-19 epidemic, it is also an important way to ensure stable economic growth by improving the public-health expenditure in quantity and quality, continuously perfecting the public-health system and policy, and preventing the recurrence of such major epidemics.
- (5)
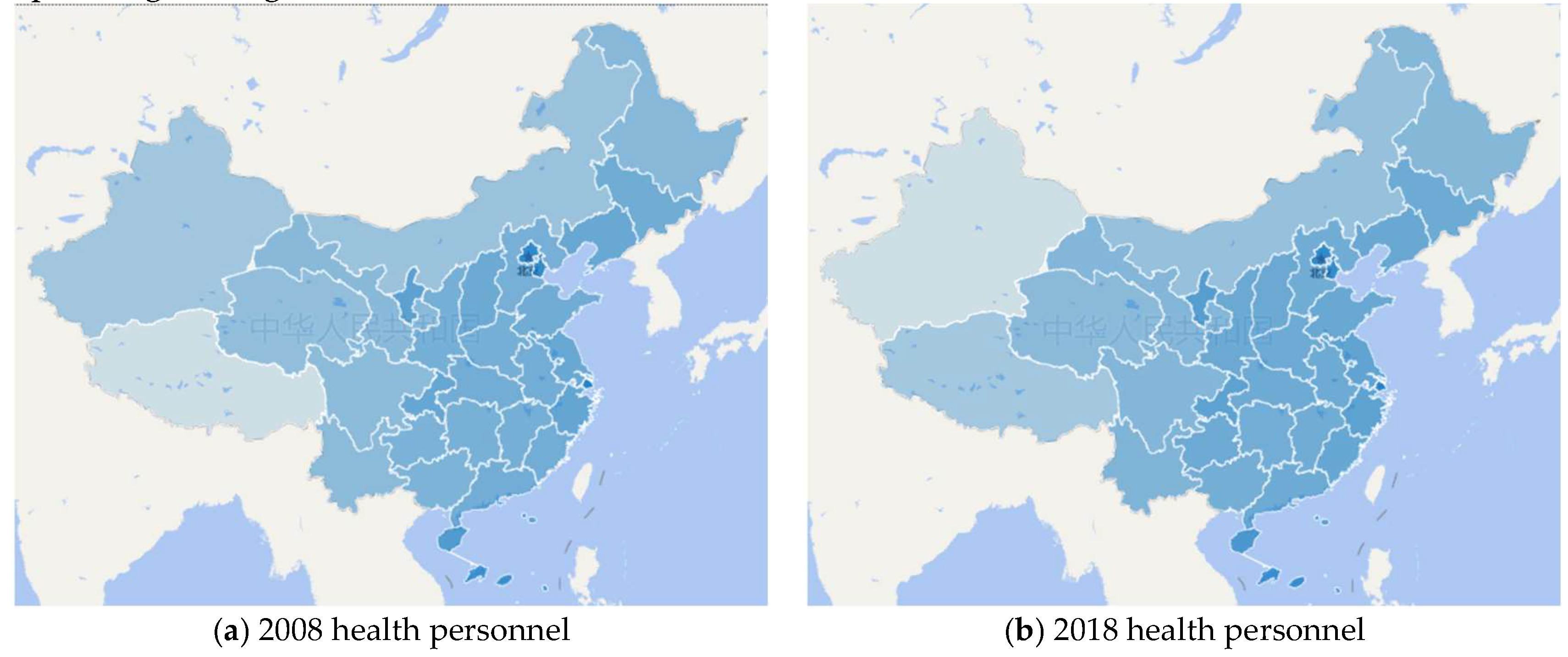
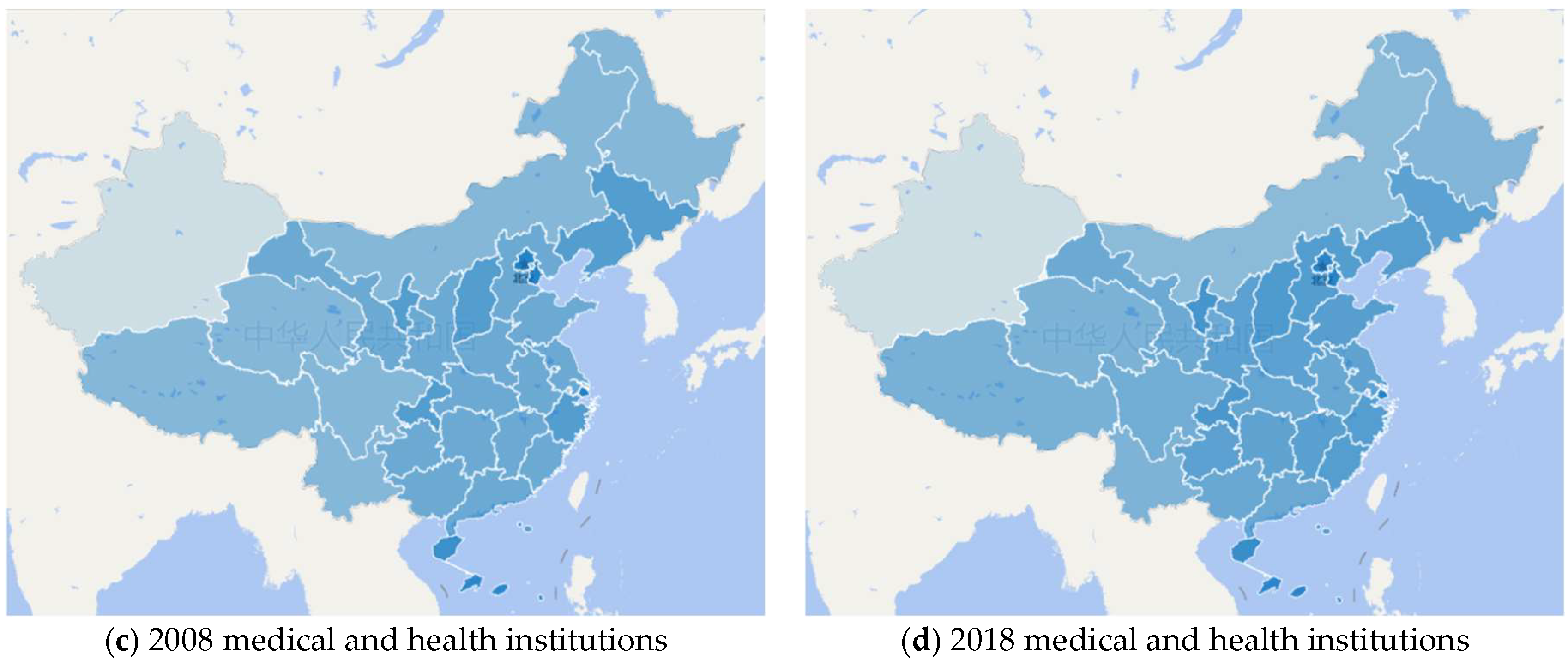
- Although the Chinese government inclines the public-health expenditure to the poor provinces in central and western regions, the imbalance and inequity in the allocation of public-health resources among regions are still expanding. China has carried out a comprehensive reform to alleviate the increasingly obvious inequities in public-health and medical services among regions, which has made public-health expenditure increase significantly in poor provinces from the central and western regions (see Table 2). The per capita public-health expenditure has increased in all 31 provinces of China since 2008. Among these provinces, Hainan, Jiangxi, Guizhou, and Guangxi are the top four provinces in terms of per capita public-health expenditure growth, with a growth rate of more than 400%, all of which are relatively poor provinces. In addition, the proportion of provincial public-health expenditure in provincial GDP and local fiscal expenditure has also increased significantly in central and western provinces. Obviously, the Chinese central government has invested a large amount of funds into the central and western provinces by transfer payment, which causes a large growth in public-health expenditure in these provinces.
- (6)
- There are a lot of wasted resources in the public-health system, which seriously reduces the efficiency of public-health expenditure in China. Although Table 3 shows that the public-health expenditure level of China is higher than that of India, it does not mean that expenditure efficiency is higher, or that the residents’ sense of gain is higher in China, because there is a huge waste of resources in China’s medical service and insurance system. The Chinese government has carried out the market-oriented reform of governmental hospitals, and requires these hospitals to be responsible for their own profits and losses. Thus, the responsibility for making profits is mainly shared by all doctors, which will lead to doctors treating minor diseases in the way of treating serious diseases, requiring patients to participate in various physical tests, prescribing a large number of safe, inefficient, and high-profit drugs, and finally making the patients and the medical insurance system pay the bill. At the same time, many governmental hospitals increase their income through economies of scale; for example, the number of beds in the First Affiliated Hospital of Zhengzhou University is more than 10,000. Such a large-scale hospital is almost unimaginable in the United Kingdom and the United States, but there are many in China. Although it brings convenience for residents to get medical services, it not only causes a great waste of resources, but also does not bring residents a higher sense of gain, because such a large hospital needs residents and the medical insurance system to bear most of the costs. The ultimate result is a great waste of resources, medical insurance fund deficit, and a low sense of patient acquisition, which all reflect the low efficiency of Chinese public-health expenditure.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Available online: http://k.sina.com.cn/article_1901036140_714f826c001015m7g.html?from=edu (accessed on 11 December 2020).
- Available online: http://mil.news.sina.com.cn/2020-02-10/doc-iimxxstf0351945.shtml (accessed on 11 December 2020).
- Sundarasen, S.; Chinna, K.; Kamaludin, K.; Nurunnabi, M.; Baloch, G.M.; Khoshaim, H.B.; Hossain, S.F.A.; Sukayt, A. Psychological Impact of COVID-19 and Lockdown among University Students in Malaysia: Implications and Policy Recommendations. Int. J. Environ. Res. Public Health 2020, 17, 6206. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Moreno, A.; Urbanos-Garrido, R.M.; Thuissard-Vasallo, I.J. Public healthcare expenditure in Spain: Measuring the impact of driving factors. Health Policy 2013, 111, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Zhang, L.; Li, F.; Zheng, X. Strategic interaction and the determinants of public health expenditures in China: A spatial panel perspective. Ann. Reg. Sci. 2013, 50, 203–221. [Google Scholar] [CrossRef]
- Musgrove, P. Public spending on health care: How are different criteria related? Health Policy 1999, 47, 207–223. [Google Scholar] [CrossRef]
- Folland, S.; Goodman, A.C.; Stano, M. The Economics of Health and Health Care; Macmillan Publishing Inc.: New York, NY, USA, 1993. [Google Scholar]
- Hayes, B.; Vandenheuvel, A. Public attitudes towards government spending on health care. Aust. J. Soc. Issues 1995, 30, 275–290. [Google Scholar] [CrossRef]
- O’Donnell, O.; Doorslaer, E.V.; Rannan-Eliya, R.P.; Somanathan, A.; Adhikari, S.R.; Harbianto, D.; Garg, C.C.; Karan, A.; Leung, G.M.; Pande, B.R.; et al. The Incidence of Public Spending on Healthcare: Comparative Evidence from Asia. World Bank Econ. Rev. 2007, 21, 93–123. [Google Scholar] [CrossRef]
- Potrafke, N. The growth of public health expenditures in OECD countries: Do government ideology and electoral motives matter? J. Health Econ. 2010, 29, 797–810. [Google Scholar] [CrossRef]
- Carrera, P. The Importance of Public Health Spending. Health Affairs 2011, 30, 2027. [Google Scholar] [CrossRef]
- Goli, S.; Moradhvaj James, K.S.; Singh, D.; Srinivasan, V. Road to family planning and RMNCHN related SDGs: Tracing the role of public health spending in India. Global Public Health 2020, 8, 1–17. [Google Scholar] [CrossRef]
- Kentikelenis, A.E.; Stubbs, T.H.; King, L.P. Structural adjustment and public spending on health: Evidence from IMF programs in low-income countries. Soc. Sci. Med. 2015, 126, 169–176. [Google Scholar] [CrossRef]
- Singh, S.R.; Young, G.J. Tax-Exempt Hospitals’ Investments in Community Health and Local Public Health Spending: Patterns and Relationships. Health Services Res. 2017, 52, 2378–2396. [Google Scholar] [CrossRef] [PubMed]
- Atems, B. Public health expenditures, taxation, and growth. Health Econ. 2019, 28, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Dominique, V.D.W. Assessing the welfare impacts of public spending. World Dev. 1998, 26, 365–379. [Google Scholar]
- Cutler, D.M.; Rosen, A.B.; Vijan, S. The value of medical spending in the United States. N. Engl. J. Med. 2006, 355, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Verma, R.; Clark, S.; Leider, J.; Bishai, D. Impact of State Public Health Spending on Disease Incidence in the United States from 1980 to 2009. Health Services Res. 2017, 52, 15–25. [Google Scholar] [CrossRef][Green Version]
- Himmelstein, D.U.; Woolhandler, S. Public Health’s Falling Share of US Health Spending. Am. J. Public Health 2015, 106, 1–2. [Google Scholar] [CrossRef]
- Matteo, L.D. The sustainability of public health expenditures: Evidence from the Canadian federation. Eur. J. Health Econ. 2010, 11, 569–584. [Google Scholar] [CrossRef]
- Clemente, J.; Lázaro-Alquézar, A.; Montañés, A. Convergence in Spanish Public health expenditure: Has the decentralization process generated disparities? Health Policy 2019, 123, 503–507. [Google Scholar] [CrossRef]
- Rahman, T. Determinants of public health expenditure: Some evidence from Indian states. Appl. Econ. Lett. 2008, 15, 853–857. [Google Scholar] [CrossRef]
- Kelly, E.; Stoye, G.; Vera-Hernández, M. Public Hospital Spending in England: Evidence from National Health Service Administrative Records. Fiscal Stud. 2016, 37, 433–459. [Google Scholar] [CrossRef]
- Wang, J.; Chen, G. Research on the content and caliber of public health expenditure in China. Public Finance Res. 2007, 8, 69–72. [Google Scholar]
- E, Q.; Liu, J. Public health function of medical institutions and its realization. Chin. J. Public Health Manag. 2005, 21, 9–10. [Google Scholar]
- Wang, J. Research on the scale of government health expenditure in China: Three misunderstandings and empirical evidence. Manag. World 2007, 2, 35–44. [Google Scholar]
- Sensenig, A.L. Refining Estimates of Public Health Spending as Measured in National Health Expenditures Accounts: The United States Experience. J. Public Health Manag. Pract. 2007, 13, 103–114. [Google Scholar] [CrossRef]
- Leider, J.P. The Problem with Estimating Public Health Spending. J. Public Health Manag. Pract. 2016, 24, 1–11. [Google Scholar] [CrossRef]
- Ho, C.S.; Gostin, L.O. The Social Face of Economic Growth: China’s Health System in Transition. JAMA 2009, 301, 1809–1811. [Google Scholar] [CrossRef]
- Newhouse, J.P. Medical-Care Expenditure: A Cross-National Survey. J. Human Res. 1977, 12, 115. [Google Scholar] [CrossRef]
- Giannoni, M.; Hitiris, T. The regional impact of health care expenditure: The case of Italy. Appl. Econ. 2002, 34, 1829–1836. [Google Scholar] [CrossRef]
- Cookson, R.; Laudicella MDonni, P.L. Measuring change in health care equity using small-area administrative data: Evidence from the English NHS 2001–2008. Soc. Sci. Med. 2020, 75, 1514–1522. [Google Scholar] [CrossRef]
- Chen, G.; Inder, B.; Lorgelly, P.; Hollingsworth, B. The cyclical behaviour of public and private health expenditure in China. Health Econ. 2013, 22, 1071–1092. [Google Scholar] [CrossRef]
- Costa-Font, J.; Pons-Novell, J. Public health expenditure and spatial interactions in a decentralized national health system. Health Econ. 2007, 16, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Kinner, K.; Pellegrini, C. Expenditures for Public Health: Assessing Historical and Prospective Trends. Am. J. Public Health 2009, 99, 1780–1791. [Google Scholar] [CrossRef]
- Gerdtham, U.G.; Jnsson, B. International Comparisons of Health Expenditure: Theory, Data and Econometric Analysis. Handb. Health Econ. 2000, 1, 11–53. [Google Scholar]
- Winslow, C.E.A. The untilled fields of public health. Science 1920, 51, 23. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.; Evans, R.G. Causes of Effective Policy Implementation: China’s public health response to SARS. J. Contemp. China 2007, 16, 195–213. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Public-Health Expenditure | 2014 | 2015 | 2016 | 2017 | 2018 | |
|---|---|---|---|---|---|---|
| Items (unit: billion CNY) | Governmental hospitals | 137.11 | 172.67 | 207.51 | 219.35 | 229.47 |
| Governmental primary medical institutions | 93.80 | 110.24 | 121.06 | 132.52 | 137.91 | |
| Prevention and control of infectious diseases | 23.64 | 28.01 | 31.29 | 34.20 | 37.34 | |
| Hygiene supervision | 6.68 | 7.71 | 8.39 | 9.31 | 10.08 | |
| Maternal and child health care | 10.95 | 13.71 | 16.65 | 19.97 | 19.40 | |
| Mental health care | 0.54 | 0.76 | 0.79 | 0.85 | 0.99 | |
| Emergency medical treatment | 1.91 | 2.26 | 2.36 | 2.71 | 3.06 | |
| Public blood banks | 4.78 | 5.59 | 6.26 | 7.36 | 7.63 | |
| Major public-health service projects | 27.59 | 27.66 | 27.76 | 28.73 | 28.80 | |
| Public health emergency treatment | 0.80 | 0.61 | 0.62 | 0.85 | 0.68 | |
| Traditional Chinese medicine | 2.44 | 3.23 | 3.86 | 4.19 | 4.95 | |
| Food and drug supervision | 24.28 | 33.67 | 39.02 | 43.63 | 45.69 | |
| Medical insurance subsidy | 462.23 | 541.65 | 595.33 | 502.41 | 548.27 | |
| Medical assistance | 21.29 | 24.06 | 26.69 | 32.09 | 46.97 | |
| Other basic public-health services | 46.73 | 59.07 | 65.65 | 71.05 | 80.81 | |
| Total public-health expenditure (unit: billion CNY) | 864.75 | 1030.87 | 1153.24 | 1109.20 | 1202.05 | |
| Per capita public-health expenditure (unit: CNY) | 632.21 | 749.93 | 834.04 | 797.94 | 861.45 | |
| Total public-health expenditure/GDP (%) | 1.35 | 1.50 | 1.56 | 1.35 | 1.34 | |
| Total public-health expenditure/fiscal expenditure (%) | 5.70 | 5.86 | 6.14 | 5.46 | 5.44 | |
| Province | Per Capita Public-Health Expenditure (Unit: CNY) | Public-Health Expenditure/GDP | Public-Health Expenditure/Total Fiscal Expenditure | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 2008 | 2014 | 2018 | 2008 | 2014 | 2018 | 2008 | 2014 | 2018 | |
| Beijing | 819.03 | 1283.63 | 1750.54 | 1.30% | 1.28% | 1.14% | 7.40% | 6.05% | 5.05% |
| Tianjin | 356.46 | 917.27 | 950.68 | 0.62% | 0.87% | 1.11% | 4.83% | 4.75% | 4.78% |
| Hebei | 172.04 | 515.91 | 703.94 | 0.75% | 1.29% | 1.64% | 6.39% | 8.12% | 6.88% |
| Shanxi | 209.62 | 569.59 | 742.87 | 0.98% | 1.62% | 1.73% | 5.44% | 6.72% | 6.45% |
| Inner Mongolia | 244.76 | 773.76 | 958.29 | 0.70% | 1.09% | 1.50% | 4.11% | 4.99% | 5.03% |
| Liaoning | 194.44 | 529.56 | 618.86 | 0.61% | 0.81% | 1.15% | 3.90% | 4.58% | 5.05% |
| Jilin | 217.70 | 637.55 | 800.17 | 0.93% | 1.27% | 1.92% | 5.04% | 6.02% | 5.71% |
| Heilongjiang | 187.45 | 521.50 | 613.79 | 0.86% | 1.33% | 1.80% | 4.65% | 5.82% | 4.95% |
| Shanghai | 571.13 | 929.44 | 1492.17 | 0.87% | 0.95% | 1.00% | 4.71% | 4.57% | 4.33% |
| Jiangsu | 191.46 | 599.59 | 807.82 | 0.48% | 0.73% | 0.70% | 4.58% | 5.63% | 5.58% |
| Zhejiang | 274.12 | 669.85 | 839.79 | 0.67% | 0.92% | 0.83% | 6.47% | 7.14% | 5.58% |
| Anhui | 169.26 | 596.28 | 762.93 | 1.17% | 1.73% | 1.42% | 6.30% | 7.74% | 7.34% |
| Fujian | 204.09 | 655.00 | 862.31 | 0.69% | 1.03% | 0.88% | 6.53% | 7.51% | 7.03% |
| Jiangxi | 174.82 | 634.56 | 969.12 | 1.10% | 1.83% | 1.98% | 6.36% | 7.41% | 7.95% |
| Shandong | 149.11 | 527.25 | 677.83 | 0.45% | 0.87% | 1.02% | 5.19% | 7.17% | 6.74% |
| Henan | 154.28 | 543.65 | 744.11 | 0.81% | 1.47% | 1.43% | 6.38% | 8.50% | 7.75% |
| Hubei | 166.49 | 587.18 | 748.63 | 0.84% | 1.25% | 1.05% | 5.76% | 6.91% | 6.10% |
| Hunan | 137.30 | 534.59 | 699.35 | 0.76% | 1.33% | 1.33% | 4.96% | 7.15% | 6.45% |
| Guangdong | 203.33 | 618.43 | 954.44 | 0.55% | 0.97% | 1.08% | 5.32% | 7.22% | 6.88% |
| Guangxi | 163.56 | 637.48 | 853.60 | 1.12% | 1.93% | 2.14% | 6.07% | 8.68% | 7.92% |
| Hainan | 194.85 | 836.12 | 1189.99 | 1.11% | 2.15% | 2.26% | 4.65% | 6.83% | 6.57% |
| Chongqing | 181.90 | 702.33 | 924.62 | 0.89% | 1.47% | 1.33% | 5.08% | 6.33% | 6.32% |
| Sichuan | 176.41 | 611.01 | 812.54 | 1.14% | 1.74% | 1.58% | 4.87% | 7.30% | 6.98% |
| Guizhou | 187.54 | 735.19 | 1029.69 | 1.89% | 2.78% | 2.41% | 6.40% | 7.27% | 7.37% |
| Yunnan | 230.22 | 637.10 | 916.60 | 1.84% | 2.34% | 2.12% | 7.11% | 6.75% | 7.29% |
| Tibet | 559.93 | 1318.02 | 2391.56 | 4.14% | 4.51% | 5.31% | 4.30% | 3.50% | 4.17% |
| Shaanxi | 210.84 | 706.59 | 906.59 | 1.07% | 1.51% | 1.46% | 5.49% | 6.72% | 6.61% |
| Gansu | 228.62 | 670.82 | 914.77 | 1.84% | 2.54% | 2.98% | 6.02% | 6.83% | 6.39% |
| Qinghai | 445.13 | 1172.96 | 1806.70 | 2.42% | 2.96% | 3.96% | 6.78% | 5.05% | 6.61% |
| Ningxia | 276.86 | 842.86 | 1180.35 | 1.42% | 2.02% | 2.31% | 5.27% | 5.54% | 5.72% |
| Xinjiang | 275.18 | 753.68 | 885.20 | 1.40% | 1.85% | 1.72% | 5.54% | 5.18% | 4.39% |
| Per capita Public-Health Expenditure (Local Currency/USD) | Public-Health Expenditure /Total Fiscal Expenditure | Public-Health Expenditure /GDP | ||||
|---|---|---|---|---|---|---|
| 2014 | 2018 | 2014 | 2018 | 2014 | 2018 | |
| The US | 4069 | 4943 | 20.94% | 22.36% | 7.44% | 7.89% |
| The UK | 2075/3415 | 2302/3071 | 19.49% | 20.22% | 7.27% | 7.23% |
| Japan | 301,314/2844 | 325,277/2946 | 36.25% | 37.23% | 7.29% | 7.37% |
| China | 632/103 | 861/130 | 5.70% | 5.44% | 1.35% | 1.34% |
| Russia | 17,278/450 | 22,815/364 | 7.83% | 9.25% | 1.35% | 3.05% |
| India | 1173/19 | — | 4.29% | — | 1.18% | — |
| Thailand | 4061/125 | 4871/151 | 11.15% | 11.31% | 2.86% | 3.03% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, H.; Qian, X. How the Chinese Government Has Done with Public Health from the Perspective of the Evaluation and Comparison about Public-Health Expenditure. Int. J. Environ. Res. Public Health 2020, 17, 9272. https://doi.org/10.3390/ijerph17249272
Jin H, Qian X. How the Chinese Government Has Done with Public Health from the Perspective of the Evaluation and Comparison about Public-Health Expenditure. International Journal of Environmental Research and Public Health. 2020; 17(24):9272. https://doi.org/10.3390/ijerph17249272
Chicago/Turabian StyleJin, Hui, and Xinyi Qian. 2020. "How the Chinese Government Has Done with Public Health from the Perspective of the Evaluation and Comparison about Public-Health Expenditure" International Journal of Environmental Research and Public Health 17, no. 24: 9272. https://doi.org/10.3390/ijerph17249272
APA StyleJin, H., & Qian, X. (2020). How the Chinese Government Has Done with Public Health from the Perspective of the Evaluation and Comparison about Public-Health Expenditure. International Journal of Environmental Research and Public Health, 17(24), 9272. https://doi.org/10.3390/ijerph17249272