Reopening Schools during the COVID-19 Pandemic: Overview and Rapid Systematic Review of Guidelines and Recommendations on Preventive Measures and the Management of Cases

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Official Documentation Released by Government Institutions
2.1.1. Data Sources and Search Strategy
2.1.2. Document Selection and Data Extraction
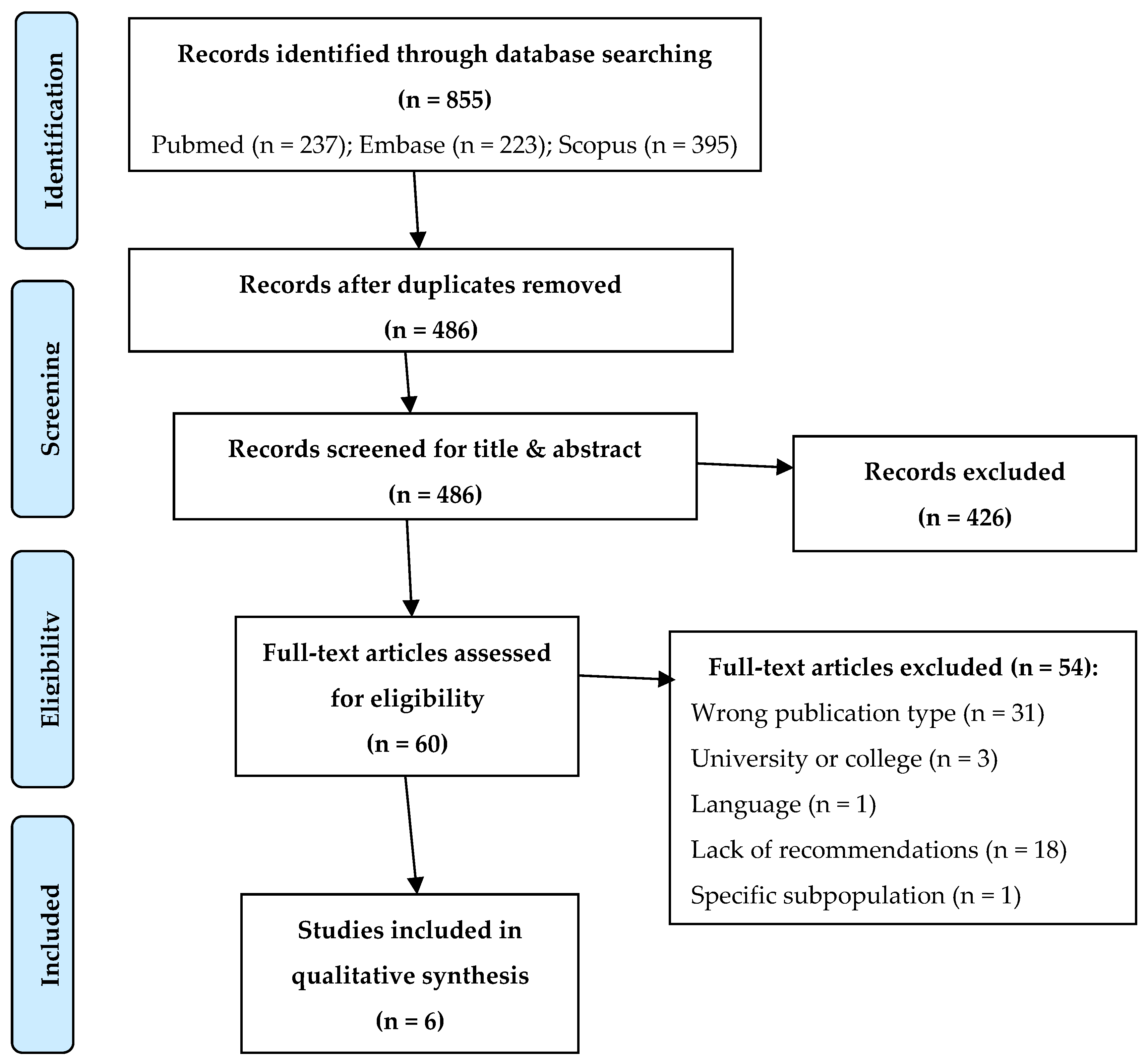
2.2. Rapid Systematic Review in Scientific Databases
2.2.1. Data Sources and Search Strategy
2.2.2. Document Selection and Data Extraction
3. Results
3.1. Preventive Measures
3.1.1. Official Documentation Released by Government Institutions
3.1.2. Rapid Systematic Review
3.2. Management of Suspected and Confirmed Cases
3.2.1. Official Documentation Released by Government Institutions
3.2.2. Rapid Systematic Review
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus Disease (COVID-19) Weekly Epidemiological Update. 5 October 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20201005-weekly-epi-update-8.pdf (accessed on 26 November 2020).
- European Centre for Disease Prevention and Control (ECDC). COVID-19 in Children and the Role of School Settings in COVID-19 Transmission; ECDC: Stockholm, Sweden, 6 August 2020; Available online: https://www.ecdc.europa.eu/sites/default/files/documents/COVID-19-schools-transmission-August%202020.pdf (accessed on 26 November 2020).
- Yonker, L.M.; Neilan, A.M.; Bartsch, Y.; Patel, A.B.; Regan, J.; Arya, P.; Gootkind, E.; Park, G.; Hardcastle, M.; St. John, A.; et al. Pediatric Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Clinical Presentation, Infectivity, and Immune Responses. J. Pediatr. 2020. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, W.; Dozier, M.; He, Y.; Kirolos, A.; Theodoratou, E. The role of children in transmission of SARS-CoV-2: A rapid review. J. Glob. Health 2020. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.M.; Russell, S.J.; Croker, H.; Packer, J.; Ward, J.; Stansfield, C.; Mytton, O.; Bonell, C.; Booy, R. School closure and management practices during coronavirus outbreaks including COVID-19: A rapid systematic review. Lancet Child Adolesc. Health 2020, 4, 397–404. [Google Scholar] [CrossRef]
- Otte Im Kampe, E.; Lehfeld, A.S.; Buda, S.; Buchholz, U.; Haas, W. Surveillance of COVID-19 school outbreaks, Germany, March to August 2020. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef]
- Stein-Zamir, C.; Abramson, N.; Shoob, H.; Libal, E.; Bitan, M.; Cardash, T.; Cayam, R.; Miskin, I. A large COVID-19 outbreak in a high school 10 days after schools’ reopening, Israel, May 2020. Eurosurveillance 2020. [Google Scholar] [CrossRef] [PubMed]
- Ehrhardt, J.; Ekinci, A.; Krehl, H.; Meincke, M.; Finci, I.; Klein, J.; Geisel, B.; Wagner-Wiening, C.; Eichner, M.; Brockmann, S.O. Transmission of SARS-CoV-2 in children aged 0 to 19 years in childcare facilities and schools after their reopening in May 2020, Baden-Württemberg, Germany. Eurosurveillance 2020. [Google Scholar] [CrossRef] [PubMed]
- Vogel, G. ‘It’s Been so, So Surreal.’ Critics of Sweden’s lax Pandemic Policies Face Fierce Backlash. 6 October 2020. Available online: https://www.sciencemag.org/news/2020/10/it-s-been-so-so-surreal-critics-sweden-s-lax-pandemic-policies-face-fierce-backlash (accessed on 19 November 2020).
- Hoffman, J.A.; Miller, E.A. Addressing the Consequences of School Closure Due to COVID-19 on Children’s Physical and Mental Well-Being. World Med. Health Policy 2020. [Google Scholar] [CrossRef] [PubMed]
- Imran, N.; Aamer, I.; Sharif, M.I.; Bodla, Z.H.; Naveed, S. Psychological burden of quarantine in children and adolescents: A rapid systematic review and proposed solutions. Pakistan J. Med. Sci. 2020, 36, 1106–1116. [Google Scholar] [CrossRef] [PubMed]
- Lee, J. Mental health effects of school closures during COVID-19. Lancet Child Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef]
- Baron, E.J.; Goldstein, E.G.; Wallace, C.T. Suffering in silence: How COVID- 19 school closures inhibit the reporting of child maltreatment. J. Public Econ. 2020, 190, 104258. [Google Scholar] [CrossRef] [PubMed]
- UNESCO. Global Monitoring of School Closures Caused by COVID-19. Available online: https://en.unesco.org/covid19/educationresponse (accessed on 19 October 2020).
- World health Organization (WHO) Regional Office for Europe. Countries. Available online: https://www.euro.who.int/en/countries (accessed on 1 September 2020).
- Khangura, S.; Konnyu, K.; Cushman, R.; Grimshaw, J.; Moher, D. Evidence summaries: The evolution of a rapid review approach. Syst. Rev. 2012, 1, 10. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Langlois, E.V.; Straus, S.E. (Eds.) Rapid Reviews to Strengthen Health Policy and Systems: A Practical Guide; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). Data on Country Response Measures to COVID-19. Available online: https://www.ecdc.europa.eu/en/publications-data/download-data-response-measures-covid-19 (accessed on 19 November 2020).
- Worldometer. Coronavirus Update (Live). Available online: https://www.worldometers.info/coronavirus/? (accessed on 19 November 2020).
- Consiglio Grande e Generale, Repubblica di San Marino. Decreto-Legge 8 Marzo 2020 n.44-Misure Urgenti di Contenimento da COVID-19 (Coronavirus). Available online: https://www.consigliograndeegenerale.sm/on-line/home/archivio-leggi-decreti-e-regolamenti/scheda17167921.html (accessed on 19 November 2020).
- Ministère de L’Éducation Nationale, de la Jeunesse et des Sports (France). Protocole Sanitaire des écoles et établissement Scolaires. 19 August 2020. Available online: https://ort-france.fr/wp-content/uploads/PROTOCOLE-SANITAIRE.pdf (accessed on 19 November 2020).
- Ministère de L’Éducation Nationale, de la Jeunesse et des Sports (France). Suspicion ou Confirmation de cas Covid-19: Ce qu’il Faut Faire. Directeurs d’école, Chefs d’établissement: Des Fiches détaillées Précisent les Procédures à Suivre dans les cas de Suspicion ou de Confirmation de cas Covid-19 dans une école, un collège ou un lycée. Mise à jour. 20 September 2020. Available online: https://www.education.gouv.fr/suspicion-ou-confirmation-de-cas-covid-19-ce-qu-il-faut-faire-305730 (accessed on 1 October 2020).
- Ministère de L’Éducation Nationale, de L’enfance et de la Jeunesse (Luxembourg). Dispositif pour la Rentrée Scolaire 2020–2021 dans le Contexte de la Crise Sanitaire COVID-19. Available online: https://gouvernement.lu/fr/actualites/toutes_actualites/articles/2020/09-septembre/04-meisch-briefing.html (accessed on 26 November 2020).
- Ministère de L’Éducation Nationale, de L’enfance et de la Jeunesse (Luxembourg). Minimal Chanchë fir de virus, Maximal Chanchë fir d’bildung. 25 September 2020. Available online: https://men.public.lu/dam-assets/catalogue-publications/sante-bien-etre/covid19/minimal-chance.pdf (accessed on 1 October 2020).
- Office of the Deputy Prime Minister Ministry for Health (Malta). Advice and Guidelines to the Educational Sector for the Re-Opening of Primary and Secondary Schools in Malta. August 2020. Available online: https://deputyprimeminister.gov.mt/en/health-promotion/covid-19/Documents/mitigation-conditions-and-guidances/Advice-and-guidelines-for-educational-sector_02Sep20.pdf (accessed on 1 October 2020).
- The Department of Education and Skills (Ireland). COVID-19 Response Plan for the Safe and Sustainable Reopening of Primary and Special Schools V2. August 2020. Available online: https://assets.gov.ie/82063/f53cc783-ed0a-4e55-bac0-18133323e90d.pdf (accessed on 1 October 2020).
- The Department of Education and Skills (Ireland). COVID-19 Response Plan for the Safe and Sustainable Reopening of Post Primary Schools V3. August 2020. Available online: https://assets.gov.ie/83312/6c36aaac-22fc-44fd-a4be-88cea4db82d6.pdf (accessed on 1 October 2020).
- The Department of Education and Skills (Ireland). Reopening Our Schools—The Roadmap for the Full Return to School. 27 July 2020. Available online: https://assets.gov.ie/82145/40753991-21a5-4715-a5a1-0f193df95ade.pdf (accessed on 1 October 2020).
- Health Service Executive, Health Protection, Office of the Clinical Director. Schools Pathway for Covid-19, the Public Health Approach. 24 August 2020. Available online: https://assets.gov.ie/86158/573fe99d-e847-4bb6-b865-456e5c03b7e4.pdf (accessed on 1 October 2020).
- Ministero dell’Istruzione (Italy). Protocollo D’intesa Per Garantire L’avvio Dell’anno Scolastico nel Rispetto Delle Regole di Sicurezza per il Contenimento Della Diffusione di Covid 19. 6 August 2020. Available online: https://www.miur.gov.it/documents/20182/2467413/Protocollo_sicurezza.pdf/292ee17f-75cd-3f43-82e0-373d69ece80f?t=1596709448986 (accessed on 1 October 2020).
- Presidenza del Consiglio dei Ministri, Dipartimento di Protezione Civile (Italy). Documento Tecnico Sull’ipotesi di Rimodulazione delle Misure Contenitive nel Settore Scolastico. Stralcio Verbale n. 82; 28 May 2020. Available online: https://www.miur.gov.it/documents/20182/0/Verbale+n.+90+riunione+CTS+del+22+giugno+2020_+STRALCIO+CTS.pdf/75993438-9abc-b6f9-5b14-37d7b7892b9b?t=1596095168730 (accessed on 1 October 2020).
- Gazzetta Ufficiale della Repubblica Italiana, Serie Generale-n. 222 7-9-2020 (Italy) “Allegato 16”. Linee Guida Per il Trasporto Scolastico Dedicato. Available online: https://www.gazzettaufficiale.it/eli/gu/2020/09/07/222/sg/pdf (accessed on 1 October 2020).
- ISS, Ministero della Salute, Ministero dell’Istruzione, INAIL, Fondazione Bruno Kessler, Regione Emilia-Romagna, Regione Veneto (Italy). Rapporto ISS COVID-19. n. 58/2020 Rev. Indicazioni Operative per la Gestione di Casi e Focolai di SARS-CoV-2 Nelle Scuole e nei Servizi Educativi Dell’infanzia. 28 August 2020. Available online: https://www.iss.it/documents/20126/0/Rapporto+ISS+COVID+58_2020+Rev.pdf/29a228fe-4b3d-c5d7-cd6a-7a86d141d440?t=1598976654944 (accessed on 1 October 2020).
- Consiglio Superiore della Pubblica Istruzione (Italy). Parere del CSPI Sullo Schema di “Ordinanza Relativa agli Alunni con Fragilità ai Sensi Dell’articolo 2, Comma 1, Lettera d-bis) del Decreto-Legge 8 Aprile 2020, n. 22”. Available online: https://www.miur.gov.it/documents/20182/0/CSPI_Parere_AlunFrag_15set_20.pdf/b056c758-7365-8b8b-fee6-f165a31ca3a0?t=1600264832398 (accessed on 1 October 2020).
- Serviço Nacional de Saúde, Direção-Geral da Saúde (Portugal). Referencial Escolas—Controlo da Transmissão de Covid-19 em Contexto Escolar. September 2020. Available online: https://www.portugal.gov.pt/download-ficheiros/ficheiro.aspx?v=%3d%3dBQAAAB%2bLCAAAAAAABAAzNDAxNgQAzLafLAUAAAA%3d (accessed on 1 October 2020).
- Direção-Geral da Saúde, Direção-Geral da Educação (Portugal). ORIENTAÇÕES. Ano letivo 2020/2021. 9 September 2020. Available online: https://www.igec.mec.pt/upload/PDF/Orienta_ano_letivo_2020_2021.pdf (accessed on 1 October 2020).
- Direção-Geral da Saúde, Direção-Geral da Educação (Portugal). Orientações para a Realização em Regime Presencial das aulas Práticas de Educação Física. 1 September 2020. Available online: https://www.dge.mec.pt/sites/default/files/orientacoes_educacao_fisica_20202021_dge_dgs.pdf (accessed on 1 October 2020).
- Department for Education (UK). Guidance for Full Opening: Schools. Update 01.10.2020. Available online: https://www.gov.uk/government/publications/actions-for-schools-during-the-coronavirus-outbreak/guidance-for-full-opening-schools (accessed on 1 October 2020).
- Department for Education (UK). What to Do If a Pupil Is Displaying Symptoms of Coronavirus (COVID-19). 17 September 2020. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/928841/Symptomatic_children_action_list_SCHOOLS_FINAL_22-10.pdf (accessed on 1 October 2020).
- Ministerio de Sanidad, Ministerio de Educación y Formación Profesional (Spain). Medidas de Prevencion, Higiene y Promocion de la Salud Frente a COVID-19 para Centros Educativos en el curso 2020–2021. 22 June 2020. Available online: https://www.educacionyfp.gob.es/dam/jcr:7e90bfc0-502b-4f18-b206-f414ea3cdb5c/medidas-centros-educativos-curso-20-21.pdf (accessed on 1 October 2020).
- Consejo Interterritorial del Sistema Nacional de Salud (Spain). Acuerdo del Consejo Interterritorial del Sistema Nacional de Salud, Adoptado en Coordinación con la Conferencia Sectorial de Educación, Sobre la Declaración de Actuaciones Coordinadas en Salud Pública Frente al Covid-19 Para Centros Educativos Durante el Curso 2020–2021. 27 August 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Acuerdo_CISNS_CSE_Actuaciones_coordinadas_en_salud_publica_para_centros_educativos_27.08.20.pdf (accessed on 1 October 2020).
- Ministerio de Sanidad (Spain). Documento Técnico-Guía de Actuación ante la Aparición de casos de COVID-19 en Centros Educativos. 24 September 2020. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Guia_actuacion_centros_educativos.pdf (accessed on 1 October 2020).
- Congresso di Stato (San Marino). Linee Guida per l’anno Scolastico 2020/2021. 17 September 2020. Available online: http://www.istruzioneecultura.sm/on-line/home/articolo20009333.html (accessed on 1 October 2020).
- Johansen, T.B.; Astrup, E.; Jore, S.; Nilssen, H.; Dahlberg, B.B.; Klingenberg, C.; Berg, A.S.; Greve-Isdahl, M. Infection prevention guidelines and considerations for paediatric risk groups when reopening primary schools during COVID-19 pandemic, Norway, April 2020. Eurosurveillance 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Ghate, S.; Parekh, B.J.; Thapar, R.K.; Nadkarni, P.R.; Sen, S.; Bansal, U.; Sambhariya, C.H.; Popat, S.; Bhattacharya, P.; Kirtani, S.; et al. Indian Academy of Pediatrics Guidelines on School Reopening, Remote Learning and Curriculum in and After the COVID-19 Pandemic. Indian Pediatr. 2020, 12, S097475591600251. [Google Scholar]
- Bonell, C.; Melendez-Torres, G.J.; Viner, R.M.; Rogers, M.B.; Whitworth, M.; Rutter, H.; Rubin, G.J.; Patton, G. An evidence-based theory of change for reducing SARS-CoV-2 transmission in reopened schools. Health Place 2020, 64, 102398. [Google Scholar] [CrossRef]
- Simon, A.; Huebner, J.; Berner, R.; Munro, A.P.S.; Exner, M.; Huppertz, H.-I.; Walger, P. Measures to maintain regular operations and prevent outbreaks of SARS-CoV-2 in childcare facilities or schools under pandemic conditions and co-circulation of other respiratory pathogens. GMS Hyg. Infect. Control 2020, 15, Doc22. [Google Scholar] [CrossRef]
- Cohen, R.; Delacourt, C.; Gras-Le Guen, C.; Launay, E. COVID-19 and schools. Guidelines of the French Pediatric Society. Arch. Pediatr. 2020, 27, 388–392. [Google Scholar] [CrossRef]
- Orscheln, R.C.; Newland, J.G.; Rosen, D.A. Practical School Algorithms for Symptomatic or SARS-CoV-2-Exposed Students Are Essential for Returning Children to In-Person Learning. J. Pediatr. 2020. [Google Scholar] [CrossRef]
- Hamilton, J.L. Returning to school in the midst of the COVID-19 pandemic for children with chronic disease and special needs. J. Pediatr. Nurs. 2020. [Google Scholar] [CrossRef]
- Hamilton, J.; Ameel, K.; Asfour, F. Returning to school in the midst of the COVID-19 pandemic for children with cystic fibrosis. Pediatr. Pulmonol. 2020, 55, 2502–2503. [Google Scholar] [CrossRef]
- Downes, K.J.; Danziger-Isakov, L.A.; Cousino, M.K.; Green, M.; Michaels, M.G.; Muller, W.J.; Orscheln, R.C.; Sharma, T.S.; Statler, V.A.; Wattier, R.L.; et al. Return to School for Pediatric Solid Organ Transplant Recipients in the United States During the Coronavirus Disease 2019 Pandemic: Expert Opinion on Key Considerations and Best Practices. J. Pediatric Infect. Dis. Soc. 2020. [Google Scholar] [CrossRef] [PubMed]
- WHO; UNESCO; UNICEF. Considerations for School-Related Public Health Measures in the Context of COVID-19 Annex to Considerations in Adjusting Public Health and Social Measures in the Context of COVID-19 14 September 2020. Available online: https://www.who.int/publications/i/item/considerations-for-school-related-public-health-measures-in-the-context-of-covid-19 (accessed on 26 November 2020).
- Smith, L.E.; Woodland, L.; Amlôt, R.; Rubin, A.; James Rubin, G. A cross-sectional survey of parental perceptions of COVID-19 related hygiene measures within schools and adherence to social distancing in journeys to and from school. BMJ Paediatr. Open 2020, 4, e000825. [Google Scholar] [CrossRef]
- Chen, X.; Ran, L.; Liu, Q.; Hu, Q.; Du, X.; Tan, X. Hand hygiene, mask-wearing behaviors and its associated factors during the COVID-19 epidemic: A cross-sectional study among primary school students in Wuhan, China. Int. J. Environ. Res. Public Health 2020, 17, 2893. [Google Scholar] [CrossRef] [PubMed]
- Kroshus, E.; Hawrilenko, M.; Tandon, P.S.; Christakis, D.A. Plans of US Parents Regarding School Attendance for Their Children in the Fall of 2020: A National Survey. JAMA Pediatr. 2020, e203864. [Google Scholar] [CrossRef] [PubMed]
- Larcher, V.; Dittborn, M.; Linthicum, J.; Sutton, A.; Brierley, J.; Payne, C.; Hardy, H. Young people’s views on their role in the COVID-19 pandemic and society’s recovery from it. Arch. Dis. Child. 2020. [Google Scholar] [CrossRef]


{kind=link}
| PICOS Strategy | |
|---|---|
| Population | Children attending primary and secondary school |
| Intervention | Prevention measures and/or management of suspected cases in school in the COVID19 pandemic |
| Comparison | None |
| Outcome | Not applicable |
| Studies | Guidelines, recommendations, protocols |
| Country | First Lockdown Measures Implemented | School Closure | School Reopening for Academic Year 2020/2021 |
|---|---|---|---|
| France [14,19,20] | 17 March 2020 | 16 March 2020 * 6633 cases 148 deaths | 1 September 2020 286,007 cases 30,661 deaths |
| Ireland [14,19,20] | 27 March 2020 | 12 March 2020 70 cases 1 death | 31 August 2020 28,811 cases 1772 deaths |
| Italy [14,19,20] | 10 March 2020 | 10 March 2020 10,156 cases 633 deaths | 14 September 2020 288,761 cases 35,624 deaths |
| Luxembourg [14,19,20] | 18 March 2020 | 16 March 2020 * 68 cases 1 death | 15 August 2020 6097 cases 123 deaths |
| Malta [14,19,20] | 12 March 2020 | 13 March 2020 12 cases 0 deaths | 28 September 2020 3006 cases 32 deaths |
| Portugal [14,19,20] | 19 March 2020 | 16 March 2020 * 7374 cases 1 death | 14 September 2020 68,208 cases 1871 deaths |
| Spain [14,19,20] | 14 March 2020 | 16 March 2020 63,386 cases 354 deaths | 7 September 2020 595,766 cases 30,585 deaths |
| United Kingdom [14,19,20] | 24 March 2020 | 20 March 2020 * 3612 cases 186 deaths | 1 September 2020 337,168 cases 41,504 deaths |
| San Marino [14,20,21] | 9 March 2020 | 24 February 2020 0 cases 0 deaths | 7 September 2020 716 cases 42 deaths |
| Country | Minimum Physical Distance | Mask at School: Staff | Mask at School: Students |
|---|---|---|---|
| France [22] | Inside school: 1 m Outside school: not mandatory | Mandatory both indoor and outdoor | Primary school: not recommended Secondary school: mandatory both indoor and outdoor |
| Ireland [27,28,29] | Between students: 1 m between desks or single students Between staff: 2 m Between staff and students: 1 m, if possible 2 m | Mandatory if 2 m distancing not possible | Primary school: not recommended >13 years: not requested but not discourage wearing if distancing is difficult to maintain |
| Italy [31,32] | Between students: 1 m Between staff: 1 m Between staff and students: 2 m between teachers’ desk and students | Mandatory for any adult entering school | >6 years: mandatory in dynamic situations and if distancing not possible |
| Luxembourg [24] | Between staff: 2 m | Mandatory between adults if distancing not possible | Primary school: facultative inside classroom and during breaks Secondary school: mandatory during breaks; at the discretion of single school inside classroom |
| Malta [26] | Between students: 1.5 m in all directions whilst sitting Between staff: 2 m Between staff and students: 2 m | Required | >3 years: children should be advised to wear masks and/or visors in common areas; not necessary within their own classrooms or cluster >11 years: recommended use of masks and/or visors at all times, including in their classroom |
| Portugal [36,37] | Between students: 1 m Between staff and students: 1 m | Mandatory | >10 years: mandatory |
| Spain [41,42] | Between students: 1.5 m Between staff: 1.5 m Between staff and students: 1.5 m | Primary school: optional within group/bubble; mandatory outside those groups if distance less than 1.5 m Secondary school: mandatory if distance less than 1.5 m | >6 years: mandatory |
| UK [39] | Between students: support to maintain distance and not touch staff and peers Between staff: 2 m Between staff and students: 2 m | Not recommended universal use of face coverings. If distancing not possible, headteachers can decide to ask staff/visitors to wear face coverings in communal areas | Primary school: not necessary If distancing not possible, headteachers can decide to ask children in years 7 and above to wear face coverings in communal areas |
| San Marino [44] | Between staff and students: 1 m | Mandatory in common areas; mandatory inside classroom if distancing not possible | Primary school: facultative Secondary school: mandatory when entering and leaving school |
| Author | Minimum Physical Distance | Mask at School: Staff | Mask at School: Students |
|---|---|---|---|
| Bonell et al. [47] | 2 m between desks | N95 surgical masks (where supplies are short should be prioritized for clinical and social care staff) | In secondary schools |
| Cohen et al. [49] | NA | Mandatory at all times | In secondary schools. Less restrictive in classes where physical distancing is possible |
| Ghate et al. [46] | Always at least 1 m for all | Compulsory for all | Compulsory for all |
| Johansen et al. [45] | At least 1 m for all | Only when pupils/staff become ill and it is not possible to maintain a distance of 2 m | Only when pupils/staff become ill and it is not possible to maintain a distance of 2 m |
| Simon et al. [48] | 1.5 m if high rates of transmission 1 | Cloth face mask if distance rules cannot be observed | >10 years: recommended 6–10 years: recommended if high rates of transmission 1 |
| Country | COVID Contact Person at School | Pre-Identified Isolation Room/Area | Student Equipment | Staff Equipment | First Call to a Doctor or Dedicated Service | Waiting for Results: Isolation of Other People | Return to School (If Not Tested Positive) |
|---|---|---|---|---|---|---|---|
| France [23] | NA | NA | If age > 6 years: mask | Mask | Home | NA | If not tested: Parents must certify they have consulted a doctor. Otherwise, after 7 days if symptoms disappeared. |
| Ireland [27,28,30] | Yes | Yes | Mask | Mask, at least 2 m | Home | Household members (removed from schools) | If tested negative: return when clinically well enough (all diarrhoea symptoms need to have been resolved for 48 h prior to return). Doctor’s certificate not required; only details as necessary for safe management are shared. |
| Italy [34] | Yes | Yes | If aged > 6 years: mask (in absence of mask: respiratory hygiene) | Mask, at least 1 m | Home | NA | If tested negative: stay home until symptoms disappearance. The doctor can decide to repeat the test after 2–3 days. Doctor’s certificate required. |
| Luxembourg [24,25] | NA | NA | NA | NA | Home | No | NA |
| Malta [26] | Yes | Yes | Mask | NA | Home | NA | Stay home until 24 h after symptoms resolve or as directed by public health authorities. Doctor’s certificate may be required. |
| Portugal [36,37] | Yes | Yes | Mask | Mask | School | Decision by Local Health Authority | NA |
| Spain [42,43] | Yes | Yes | Mask | Mask | Home | Siblings | If tested negative: return. |
| UK [39,40] | NA | Yes | NA | 2 m distancing, if not possible: suitable PPE | Home | Household members | If tested negative: return when no more symptoms. |
| Country | Return to School | Main Strategies |
|---|---|---|
| France [23] | Student cannot return before the timing defined by the doctor (as soon as possible, 7 days after the test or onset of symptoms). | Staff/students of high school in the contact list must self-isolate and be tested 7 days after the last contact to return to school. Other students in the list: isolation for 7 days, test is not mandatory. |
| Ireland [27,28,30] | NA | Public health services discuss with the school any appropriate quarantine. Every facility will be unique. Close contacts: self-isolated, tested (at day 0 and 7) (no blanket policy to quarantine/test entire classes or years). |
| Italy [34] | Student returns if no symptoms and two negative tests at 24-h intervals. | Close contacts: 14 days of quarantine starting from the last contact. Prevention Department decides the most appropriate strategies for possible tests in students/staff. |
| Luxembourg [24,25] | NA | The entire class should be tested, staff included (no later than 6 days after the last contact). No isolation but more restrictive preventive measures until the results. |
| Malta [26] | NA | Students/staff that were contacts would need to go into quarantine. |
| Portugal [36,37] | Isolation until 3 consecutive days without fever and 1 negative rRT-PCR at least 14 days from the onset of symptoms (if no hospitalization) or 2 consecutive negative rRT-PCR (if hospitalization). | Local Health Authority can decide: contacts isolation and epidemiological investigation, closure of classroom/specific areas, environmental isolation. |
| Spain [42,43] | Isolation until 3 days after the disappearance of symptoms and a minimum of 10 days from the onset of symptoms. | Close contacts: 10 days quarantine from the last contact; recommended test after 10 days from the last contact; if the test is performed before the 10th day, the quarantine must be followed until the 10th day. The classroom will be closed for 10 days if the case belonged to a bubble. If the case did not belong to bubble: quarantine of close contacts only. |
| UK [39,40] | Isolation at least 10 days from the onset of symptoms; students return only if they do not have symptoms other than cough or loss of sense of smell/taste. | Close contacts should self-isolate for 14 days from last contact. If close contacts develop symptoms in the 14 days, they should get tested: -if negative, isolation for the remainder of the 14 days; -if positive, inform their setting and isolate for at least 10 days from the onset of their symptoms and their household should self-isolate for at least 14 days from when the symptomatic person first had symptoms. |
| Author | COVID Contact Person at School | Pre-Identified Isolation Room/Area | Student Equipment | Staff Equipment | First Call to a Doctor or Dedicated Service | Waiting for Results: Isolation of Other People | Return to School (If Not Tested Positive) |
|---|---|---|---|---|---|---|---|
| Cohen et al. [49] | NA | NA | NA | NA | NA | NA | Stay home until symptoms resolve. If symptoms last for >3 days perform testing |
| Ghate et al. [46] | NA | Yes | NA | NA | NA | NA | NA |
| Johansen et al. [45] | NA | No | Age > 7: mask Age < 7: mask if pupil is comfortable | Mask if 2 m distance not possible | NA | NA | NA |
| Orscheln et al. [50] | NA | NA | NA | NA | NA | NA | If exposure to confirmed case, the student should be tested: if negative, return after 24 h without fever and symptoms improving If no exposure, evaluation by healthcare provider to get tested |
| Simon et al. [48] | Yes | NA | NA | NA | Home | NA | Stay home until 24 h symptoms resolve. Parents must confirm their child was free of symptoms for 24 h before being readmitted |
| Author | Return to School | Main Strategies |
|---|---|---|
| Cohen et al. [49] | After 7 days and possibly longer if symptoms persist. PCR monitoring is not necessary to return | Screening of entire class is only warranted if one teacher tested positive or if at least two children in the class are symptomatic and tested positive |
| Ghate et al. [46] | Notification to government authorities. Stay home for 14 days. Doctor’s certificate required | NA |
| Johansen et al. [45] | NA | NA |
| Orscheln et al. [50] | Return to school after 24 h afebrile and symptoms improving and approval of local health department. Doctor’s certificate required | Quarantine contacts of confirmed cases |
| Simon et al. [48] | Doctor’s certificate only required if child has been quarantined, a COVID-19 detection without symptoms or a close contact with a positive person. Institutions are not entitled to request a “negative test” as a condition for re-entry | Children living in the same household do not have to be necessarily tested, but remain in quarantine. This is decided by the public health department |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Moro, G.; Sinigaglia, T.; Bert, F.; Savatteri, A.; Gualano, M.R.; Siliquini, R. Reopening Schools during the COVID-19 Pandemic: Overview and Rapid Systematic Review of Guidelines and Recommendations on Preventive Measures and the Management of Cases. Int. J. Environ. Res. Public Health 2020, 17, 8839. https://doi.org/10.3390/ijerph17238839
Lo Moro G, Sinigaglia T, Bert F, Savatteri A, Gualano MR, Siliquini R. Reopening Schools during the COVID-19 Pandemic: Overview and Rapid Systematic Review of Guidelines and Recommendations on Preventive Measures and the Management of Cases. International Journal of Environmental Research and Public Health. 2020; 17(23):8839. https://doi.org/10.3390/ijerph17238839
Chicago/Turabian StyleLo Moro, Giuseppina, Tiziana Sinigaglia, Fabrizio Bert, Armando Savatteri, Maria Rosaria Gualano, and Roberta Siliquini. 2020. "Reopening Schools during the COVID-19 Pandemic: Overview and Rapid Systematic Review of Guidelines and Recommendations on Preventive Measures and the Management of Cases" International Journal of Environmental Research and Public Health 17, no. 23: 8839. https://doi.org/10.3390/ijerph17238839
APA StyleLo Moro, G., Sinigaglia, T., Bert, F., Savatteri, A., Gualano, M. R., & Siliquini, R. (2020). Reopening Schools during the COVID-19 Pandemic: Overview and Rapid Systematic Review of Guidelines and Recommendations on Preventive Measures and the Management of Cases. International Journal of Environmental Research and Public Health, 17(23), 8839. https://doi.org/10.3390/ijerph17238839