Evaluation of Reablement Home Care: Effects on Care Attendants, Care Recipients, and Family Caregivers


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Needs Assessment for Setting Priorities to Establish the RHC Model
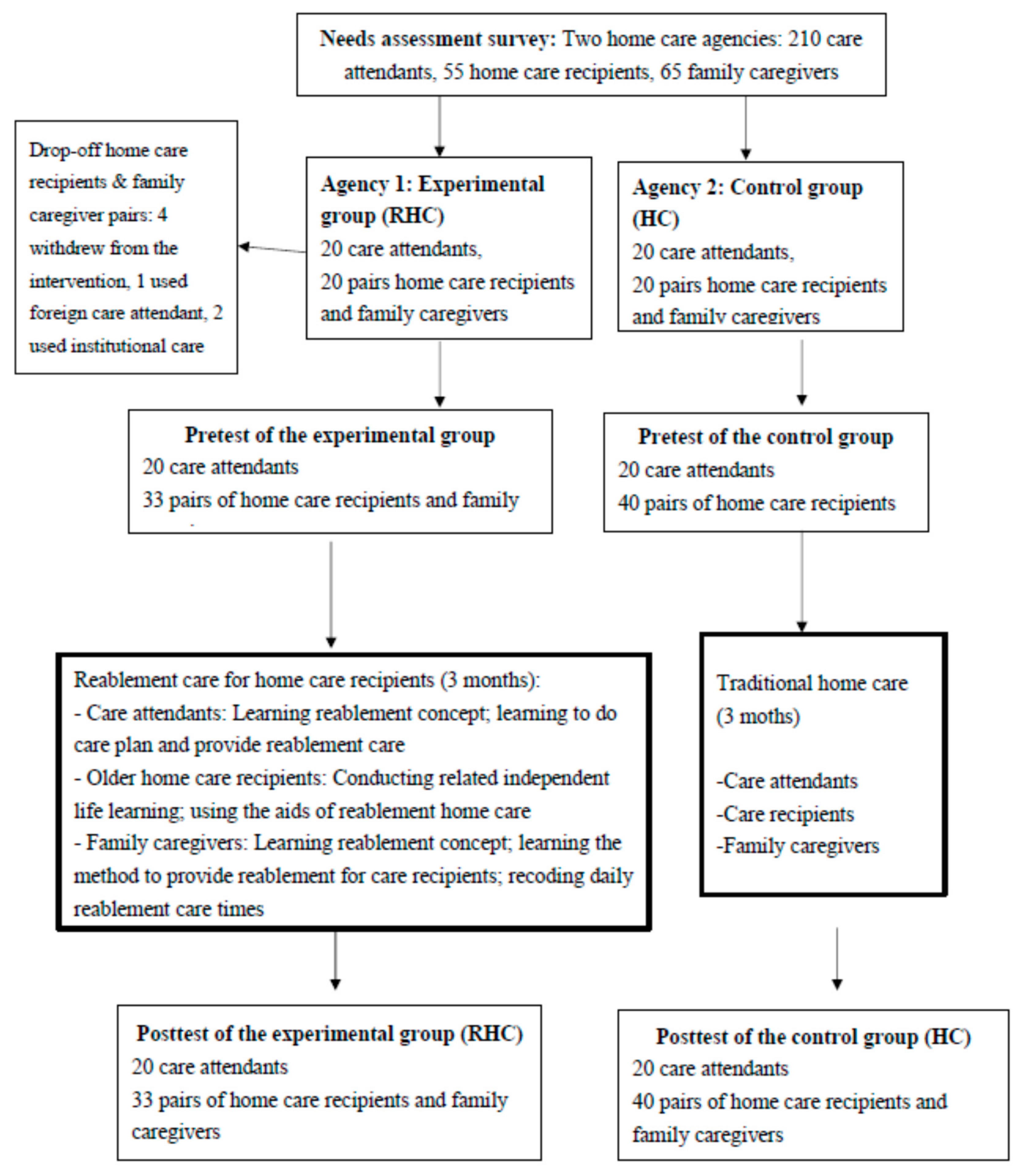
2.2. Recruitment, Implementation, and Evaluation of the Intervention
2.3. Measures
2.3.1. Main Dependent Variable: The Self-Reliance Concept on the HC Scale
2.3.2. Variables for the Care Attendants
2.3.3. Variables for the Care Recipients
2.3.4. Variables for the Family Caregivers
2.4. Analysis
3. Results
4. Discussion
4.1. Effects for Home Care Recipients
4.2. Effects for Family Caregivers
4.3. Effects for Care Attendants
4.4. Process Evaluation
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kane, R.A.; Kane, R.L. Long-Term Care: Principle, Programs, and Policies; Springer: New York, NY, USA, 1987; p. 422. [Google Scholar]
- Bookwala, J.; Zdaniuk, B.; Burton, L.; Lind, B.; Jackson, S.; Schulz, R. Concurrent and long-term predictors of older adults’ use of community-based long-term care services: The caregiver health effects study. J. Aging Health 2004, 16, 88–115. [Google Scholar] [CrossRef] [PubMed]
- Naoki, Y.; Matsuda, Y.; Maeda, I.; Kamino, H.; Kozaki, Y.; Tokoro, A.; Maki, N.; Takada, M. Association between family satisfaction and caregiver burden in cancer patients receiving outreach palliative care at home. Palliat. Support. Care 2018, 16, 260. [Google Scholar] [CrossRef] [PubMed]
- Parsons, J.G.M.; Sheridan, N.; Rouse, P.; Robinson, E.; Connolly, M. A randomized controlled trial to determine the effect of a model of restorative home care on physical function and social support among older people. Arch. Phys. Med. Rehabil. 2013, 94, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Kogan, A.C.; Wilber, K.; Mosqueda, L. Person-centered care for older adults with chronic conditions and functional impairment: A systematic literature review. J. Am. Geriatr. Soc. 2016, 64, e1–e7. [Google Scholar] [CrossRef]
- Black, K.; Hyer, K. Person-centered considerations in practice for persons with dementia and their caregivers across the continuum of care. Best Pract. Ment. Health 2010, 6, 33–46. [Google Scholar]
- Jokstad, K.; Skovdahl, K.; Landmark, B.T.; Haukelien, H. Ideal and reality; Community healthcare professionals’ experiences of user-involvement in reablement. Health Soc. Care Community 2019, 27, 907–916. [Google Scholar] [CrossRef]
- Wellin, C.; Jaffe, D.J. In search of “personal care”: Challenges to identity support in residential care for elders with cognitive illness. J. Aging Stud. 2004, 18, 275–295. [Google Scholar] [CrossRef]
- Tessier, A.; Beaulieu, M.D.; Mcginn, C.A.; Latulippe, R. Effectiveness of reablement: A systematic review. Healthc. Policy 2016, 11, 49. [Google Scholar] [CrossRef]
- Cochrane, A.; McGilloway, S.; Furlong, M.; Molloy, D.W.; Stevenson, M.; Donnelly, M. Home-care’re-ablement’services for maintaining and improving older adults’ functional independence (Protocol). Cochrane Libr. 2013, 11, 1–12. [Google Scholar] [CrossRef]
- Langeland, E.; Tuntland, H.; Folkestad, B.; Førland, O.; Jacobsen, F.F.; Kjeken, I. A multicenter investigation of reablement in Norway: A clinical controlled trial. BMC Geriatr. 2019, 19, 29. [Google Scholar] [CrossRef]
- Sims-Gould, J.; Tong, C.E.; Wallis-Mayer, L.; Ashe, M.C. Reablement, reactivation, rehabilitation and restorative interventions with odler adults in receipt of home care: A systematic review. J. Am. Med. Dir. Assoc. 2017, 18, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Hjelle, K.M.; Tuntland, H.; Førland, O.; Alvsvåg, H. Driving forces for home-based reablement; a qualitative study of older adults’ experiences. Health Soc. Care Community 2017, 25, 1581–1589. [Google Scholar] [CrossRef] [PubMed]
- Aspinal, F.; Glasby, J.; Rostgaard, T.; Tuntland, H.; Westendorn, R.G.J. New horizons: Reablement-supporting older people towards independence. Age Ageing 2016, 45, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Lewin, G.; Concanen, K.; Youens, D. The Home Independence Program with non-health professionals as care managers: An evaluation. Clin. Interv. Aging 2016, 11, 807. [Google Scholar] [CrossRef] [PubMed]
- Tuntland, H.; Aaslund, M.K.; Espehaugh, B.; Førland, O.; Kjeken, I. Reablement in community-dwelling older adults: A randomised controlled trial. BMC Geriatr. 2015, 15, 145. [Google Scholar] [CrossRef]
- Legg, L.; Gladman, J.; Drummond, A.; Davidson, A. A systematic review of the evidence on home care reablement services. Clin. Rehabil. 2015, 30, 741–749. [Google Scholar] [CrossRef]
- Parsons, M.; Senior, H.; Kerse, N.; Chen, M.H.; Jacobs, S.; Anderson, C. Randomised trial of restorative home care for frail older people in New Zealand. Nurs. Older People 2017, 29. [Google Scholar] [CrossRef]
- Lin, J.L.; Yu, Y.J. Self-supporting care for Taiwan’s practice. Long-Term Care J. 2017, 21, 15–18. (In Chinese) [Google Scholar] [CrossRef]
- Lin, Y.C.; Huang, L.H. Self-supporting care models for older adults. J. Nurs. 2018, 65, 20–26. (In Chinese) [Google Scholar] [CrossRef]
- Lewin, G.; Miguel, K.D.S.; Knuiman, M.; Alan, J.; Boldy, D.; Hendrie, D.; Vandermeulen, S. A randomized controlled trial of the home independence program, an Australian restorative home-care programme for older adults. Health Soc. Care Community 2013, 21, 69–78. [Google Scholar] [CrossRef]
- Sanerma, P.; Paavilainen, E.; Åstedt-Kurki, P. Home care services for older persons. The views of older persons and family members: A realistic evaluation. Int. J. Older People Nurs. 2020, 15, e12281. [Google Scholar] [CrossRef] [PubMed]
- Tuntland, H.; Kjeken, I.; Folkestad, B.; Førland, O.; Langeland, E. Everyday occupations prioritised by older adults participating in reablement. A cross-sectional study. Scand. J. Occup. Ther. 2020, 27, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Eklund, F.; Treschwo, A.; Ringström, A. Can reablement increase independence and reduce the need for elderly care in a Scandinavian setting? Eur. J. Public Health 2014, 24. [Google Scholar] [CrossRef]
- Cochrane, A.; Furlong, M.; McGilloway, S.; Molloy, D.W.; Stevenson, M.; Donnelly, M. Time-limited home-care reablement services for maintaining and improving the functional independence of older adults. Cochrane Database Syst. Rev. 2016, 10, CD010825. [Google Scholar] [CrossRef] [PubMed]
- Hjelle, K.M.; Alvsvåg, H.; Førland, O. The relatives’ voice: How do relatives experience participation in reablement? A qualitative study. J. Multidiscip. Healthc. 2017, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Goto, J.M. Independence Support Type Care Plan Creation Guide; Gyosei Corporation: Tokyo, Japan, 2016. (In Japanese) [Google Scholar]
- Rice, R. Home Care Nursing Practice: Concepts Application, 4th ed.; Mosby: St. Louis, MO, USA, 2006. [Google Scholar]
- Chiang, Y.H. Self-Reliance Support in Home Care: Model Establishment and Evaluation. Ph.D. Thesis, Department of Healthcare Administration, Asia University, Taichung, Taiwan, January 2019. Available online: https://hdl.handle.net/11296/z6buxu (accessed on 25 November 2020). (In Chinese).
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Yao, G.; Chung, C.W.; Yu, C.F.; Wang, J.D. Development and verification of reliability and validity of the WHOQOL-BREF Taiwan Version. J. Formos. Med. Assoc. 2002, 101, 342–351. [Google Scholar] [PubMed]
- Lin, L.N.; Wu, S.C. Measurement structure of the caregiver burden scale: Findings from a national community survey in Taiwan. Geriatr. Gerontol. Int. 2014, 14, 176–184. [Google Scholar] [CrossRef]
- Liang, K.Y.; Zeger, S.L. Longitudinal data analysis using generalized linear models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Moe, C.F.; Brinchmann, B.S. Optimising Capasity-A service user and caregiver perspective on reablement. Grounded Theory Rev. 2016, 15, 25–40. [Google Scholar]
- Ryburn, B.; Wells, Y.; Foreman, P. Enabling independence: Restorative approaches to home care provision for frail older adults. Health Soc. Care Community 2009, 17, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Moe, A.; Ingstad, K.; Brataas, H.V. Patient influence in home-based reablement for older persons: Qualitative research. BMC Health Serv. Res. 2017, 17, 736. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Care Recipients (n = 55) | Family Caregivers (n = 65) | Needs of Care Attendants (n = 210) | |||
|---|---|---|---|---|---|
| Variables | Mean (SD) or % | Variables | Mean (SD) or % | Variables | Mean (SD) or % |
| Age | 79.7 (8.9) | Age | 59.2 (11.1) | Age | 53.2 (7.2) |
| Sex | Sex | Sex | |||
| Male | 63.6% | Male | 32.3% | Male | 5.2% |
| Female | 36.4% | Female | 67.7% | Female | 94.8% |
| Years of home care use | Years of family caregiving | Working years in home care | |||
| ≤1 year | 30.9% | ≤1 year | 18.5% | <3 years | 22.9% |
| 2–3 years | 50.9% | 2–3 years | 29.2% | 4–5 years | 28.6% |
| 4–5 years | 14.5% | 4–5 years | 13.8% | 6–10 years | 34.3% |
| 6 or more years | 3.6% | 6 years or more | 38.5% | More than 10 years | 14.3% |
| Care needed in ADLs | Relationship with home care recipients | Expectation for advanced knowledge | |||
| Taking a bath | 72.7% | Spouse | 41.8% | Personal care | 4.8% |
| Dressing | 54.5% | Sons or daughters | 40.0% | Housework | 26.7% |
| Eating | 12.7% | Daughters-in-law | 7.3% | Preparing food, shopping, etc. | 1.5% |
| Transferring | 34.5% | Others | 10.9% | Emergency | 2.4% |
| Using toilet | 16.4% | Home care use items | End of care | 22.8% | |
| Walking indoors | 27.3% | Personal care (ADLs) | 83.1% | Stress coping | 12.9% |
| Care needed in IADLs | Housework | 23.1% | Occupation injury prevention | 16.6% | |
| Shopping for groceries | 67.2% | Preparing meals, accompany or shopping groceries | 41.5% | Infection prevention | 16.7% |
| Managing money | 47.3% | Accompany for rehab | 16.9% | Resource connection | 23.8% |
| Taking train/car alone | 83.6% | Others | 13.8% | Dietary nutrition | 12.4% |
| Heavy housework | 89.1% | Expectation of from home care in ADLs | Expectation to learn professional skills (top 5) | ||
| Light housework | 78.2% | Eating | 15.4% | Transferring | 33.9% |
| Making phone calls | 47.3% | Grooming | 16.9% | Passive Range or Motion Exercise | 26.7% |
| Expectation to improve in ADLs | Using toilet | 15.4% | Using assistive devices | 26.2% | |
| Taking a bath | 50.9% | Taking a bath | 55.4% | Emergency and CPR | 15.7% |
| Dressing | 41.8% | Walking | 35.4% | Baths and body cleansing | 13.3% |
| Eating | 16.4% | Going up/down stairs | 24.6% | ||
| Transferring | 27.3% | Dressing | 21.5% | ||
| Using toilet | 21.8% | Bowel control | 7.7% | ||
| Walking indoors | 27.3% | Bladder control | 3.1% | ||
| Expectation to improve in IADLS | Expectation of from home care in IADLs | ||||
| Shopping groceries | 25.5% | Shopping groceries | 20.0% | ||
| Managing money | 3.6% | Going out | 41.5% | ||
| Taking train/car alone | 27.3% | Preparing food and cooking | 38.5% | ||
| Heavy housework | 12.7% | Housework | 33.8% | ||
| Light housework | 40.0% | Laundry | 16.9% | ||
| Making phone calls | 5.5% | Making phone calls | 1.5% | ||
| Taking medicine | 13.8% | ||||
| Managing money | 1.5% | ||||
| Variables | Experimental Group (n = 20) | Control Group (n = 20) | Significance (Two Groups Baseline) |
|---|---|---|---|
| Age | 51.50 (5.93) | 55.20 (7.80) | |
| Gender | |||
| Male | 10.0% | 15.0% | |
| Female | 90.0% | 85.0% | |
| Education | |||
| Elementary school or lower | 0.0% | 15.0% | |
| Junior high school | 15.0% | 20.0% | |
| Senior high school | 65.0% | 50.0% | |
| College/university or above | 20.0% | 15.0% | |
| Marital status | |||
| Having spouse | 75.0% | 65.0% | |
| No spouse | 25.0% | 35.0% | |
| Working experience | |||
| ≤3 years | 25.0% | 15.0% | |
| 4–5 years | 40.0% | 30.0% | |
| 6–10 years | 25.0% | 30.0% | |
| ≥11 years | 10.0% | 25.0% | |
| Working hours per month | 173.50 (33.95) | 146.35 (22.94) | ** |
| Competency test (pretest) | 78.72 (3.63) | 70.30 (4.28) | *** |
| Competency test (posttest) | 93.90 (4.58) | 70.79 (3.59) | |
| Sig. (pre-post) | *** | ||
| Job satisfaction (pretest) | 39.65 (4.40) | 43.75 (3.31) | ** |
| Job satisfaction (posttest) | 44.30 (5.07) | 45.05 (3.59) | --- |
| Sig. (pre-post) | ** | * | |
| Sense of accomplishment for work (pretest) | 36.90 (3.19) | 37.55 (3.95) | |
| Sense of accomplishment for work (posttest) | 43.45 (3.97) | 38.80 (4.18) | --- |
| Sig. (pre-post) | *** | * |
| Home Care Recipients at Baseline | Family Caregivers at Baseline | ||||
|---|---|---|---|---|---|
| Variables | Experimental Group (n = 33) | Control Group (n = 40) | Variables | Experimental Group (n = 33) | Control Group (n = 40) |
| Age | 74.27 (10.1) * | 79.32 (8.0) | Age | 57.39 (13.4) | 55.38 (12.9) |
| Gender | ** | Gender | |||
| Male | 57.6% | 25.0% | Male | 39.4% | 50.0% |
| Female | 42.4% | 75.0% | Female | 60.6% | 50.0% |
| Education | Education | ||||
| Elementary school or lower | 51.5% | 55.0% | Elementary school or lower | 30.3% | 15.0% |
| Junior high school | 6.1% | 15.0% | Junior high school | 6.1% | 25.0% |
| Senior high school | 21.2% | 12.5% | Senior high school | 24.2% | 35.0% |
| College/university or above | 15.1% | 2.5% | College/university or above | 33.3% | 25% |
| Others | 6.1% | 15.0% | Others | 6.1% | 0% |
| Marital status | Marital status | ||||
| Having spouse | 48.5% | 30.0% | Having spouse | 72.7% | 67.5% |
| No spouse | 51.5% | 70% | No spouse | 27.3% | 32.5% |
| Disability level | Caregiving experience | ||||
| Mild | 24.2% | 25.0% | ≤1 year | 6.1% | 7.5% |
| Moderate | 39.4% | 32.5% | 2–3 years | 27.3% | 37.5% |
| Severe | 36.4% | 42.5% | 4–5 years | 9.1% | 7.5% |
| Self-care difficulty (pretest) | 12.45 (8.74) | 14.95 (9.67) | 6 years or more | 57.6% | 47.5% |
| Self-care difficulty (posttest) | 11.88 (8.77) | 13.00 (9.20) | Relationship | ||
| Sig. (pre-post) | * | Spouse | 30.3% | 20% | |
| Quality of life (pretest) | 76.5 (12.2) | 76.4 (11.6) | Children or daughter-in-law | 45.5% | 72.5% |
| Quality of life (posttest) | 84.61 (6.1) | 76.68 (11.4) | Brothers or sisters | 9.1% | 5.0% |
| Sig. (pre-post) | ** | Others | 15.1% | 2.5% | |
| Work | |||||
| Yes | 36.4% | 42.5% | |||
| No | 63.6% | 57.% | |||
| Caregiving burden (pretest) | 24.94 (7.6) * | 20.30 (8.5) | |||
| Caregiving burden (posttest) | 23.6 (7.7) | 21.7 (8.9) | |||
| Sig. (pre-post) | * | ||||
| Experimental Group | Control Group | |||||||
|---|---|---|---|---|---|---|---|---|
| Pretest | Care Attendants | Care Recipients | Family Caregivers | Significance | Care Attendants | Care Recipients | Family Caregivers | Significance |
| Dependence | 25.55 (1.57) | 27.06 (7.08) | 25.58 (3.20) | 23.05 (2.65) | 24.83 (3.05) | 24.65 (2.98) | ||
| Mutual-support | 43.35 (2.29) | 45.03 (4.36) | 41.21 (5.44) | ** | 47.95 (5.99) | 46.15 (6.01) | 42.65 (4.73) | ** |
| Independence | 42.05 (1.82) | 44.27 (5.45) | 43.94 (6.32) | 41.05 (4.29) | 44.13 (7.71) | 45.50 (5.40) | * | |
| Posttest | Care attendants | Care recipients | Family caregivers | Significance | Care attendants | Care recipients | Family caregivers | Significance |
| Dependence | 20.35 (2.01) *** | 24.45 (2.69) * | 24.21 (3.10) * | *** | 22.90 (2.38) | 24.48 (3.08) | 24.08 (2.91) | |
| Mutual-support | 52.25 (3.46) ** | 46.06 (4.88) | 42.18 (4.68) | *** | 47.95 (5.10) | 44.75 (4.91) | 41.25 (3.64) * | *** |
| Independence | 48.35 (4.09) ** | 44.97 (6.55) | 44.76 (5.15) | 40.60 (4.03) | 45.03 (6.70) | 39.88 (4.13) *** | ** | |
| Care Attendants | Competency Test | Job Satisfaction | Sense of Achievement | Dependence | Mutual Support | Independence | |
| Seniority | −0.41 | 0.94 | 0.79 | −0.25 | 0.31 | 0.78 | |
| Group | 8.23 *** | −3.68 ** | −0.10 | 2.39 *** | −4.46 ** | 1.35 | |
| time | 0.53 | 1.30 ** | 1.25 ** | −0.15 | −2.80 ** | −0.45 | |
| Group * time | 14.66 *** | 3.35 *** | 5.10 *** | −5.05 *** | 11.70 *** | 6.75 *** | |
| AIC | 1878.26 | 1255.32 | 1102.86 | 369.50 | 1215.00 | 1005.68 | |
| Home care recipients | Self-care difficulty | Satisfaction to home care | Satisfaction to home care agency | Dependence | Mutual support | Independence | Quality of life |
| Degree of disability | 7.32 *** | 4.91 ** | 0.95 | 0.36 | 0.75 | 0.54 | −0.24 |
| Group | −2.10 | 2.46 | −2.18 | 2.23 | −1.08 | 0.18 | 0.15 |
| time | −1.95 * | 2.20 | −1.00 | −0.35 | −8.933 × 10−17 | 0.90 | 0.33 |
| Group * time | 1.37 | −0.14 | 2.79 * | −2.23 | 1.03 | −0.20 | 7.77 ** |
| AIC | 7013.34 | 25,808.17 | 5767.84 | 2568.99 | 3751.61 | 6386.99 | 16,358.89 |
| Family caregivers | Care difficulty | Satisfaction with home care | Satisfaction to home care agency | Dependence | Mutual support | Independence | Caregiving burden |
| Degree of disability | 1.24 | −3.94 ** | −1.91 * | -.32 | −1.80 * | −1.61 | 2.68 |
| Having a job | −0.16 | −1.80 | −1.43 | −1.10 | −2.15 * | −1.74 | −2.86 |
| Group | −1.76 | −0.42 | −1.02 | 0.84 | −1.64 | −1.73 | 4.56 * |
| time | −1.05 | 0.65 | 0.20 | −0.58 | −1.40* | −5.63 *** | 1.40 * |
| Group * time | 0.32 | −0.68 | −0.05 | −0.79 | 2.37 | 6.44 *** | −2.79 *** |
| AIC | 7100.51 | 6508.59 | 2506.03 | 1283.40 | 2886.93 | 3831.04 | 8925.97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, Y.-H.; Hsu, H.-C.; Chen, C.-L.; Chen, C.-F.; Chang-Lee, S.-N.; Chen, Y.-M.; Hsu, S.-W. Evaluation of Reablement Home Care: Effects on Care Attendants, Care Recipients, and Family Caregivers. Int. J. Environ. Res. Public Health 2020, 17, 8784. https://doi.org/10.3390/ijerph17238784
Chiang Y-H, Hsu H-C, Chen C-L, Chen C-F, Chang-Lee S-N, Chen Y-M, Hsu S-W. Evaluation of Reablement Home Care: Effects on Care Attendants, Care Recipients, and Family Caregivers. International Journal of Environmental Research and Public Health. 2020; 17(23):8784. https://doi.org/10.3390/ijerph17238784
Chicago/Turabian StyleChiang, Yu-Hsien, Hui-Chuan Hsu, Chiung-Ling Chen, Chen-Fen Chen, Shu-Nu Chang-Lee, Ya-Mei Chen, and Shang-Wei Hsu. 2020. "Evaluation of Reablement Home Care: Effects on Care Attendants, Care Recipients, and Family Caregivers" International Journal of Environmental Research and Public Health 17, no. 23: 8784. https://doi.org/10.3390/ijerph17238784
APA StyleChiang, Y.-H., Hsu, H.-C., Chen, C.-L., Chen, C.-F., Chang-Lee, S.-N., Chen, Y.-M., & Hsu, S.-W. (2020). Evaluation of Reablement Home Care: Effects on Care Attendants, Care Recipients, and Family Caregivers. International Journal of Environmental Research and Public Health, 17(23), 8784. https://doi.org/10.3390/ijerph17238784