Cross-Sectional Seroepidemiologic Study of Coronavirus Disease 2019 (COVID-19) among Close Contacts, Children, and Migrant Workers in Shanghai




Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
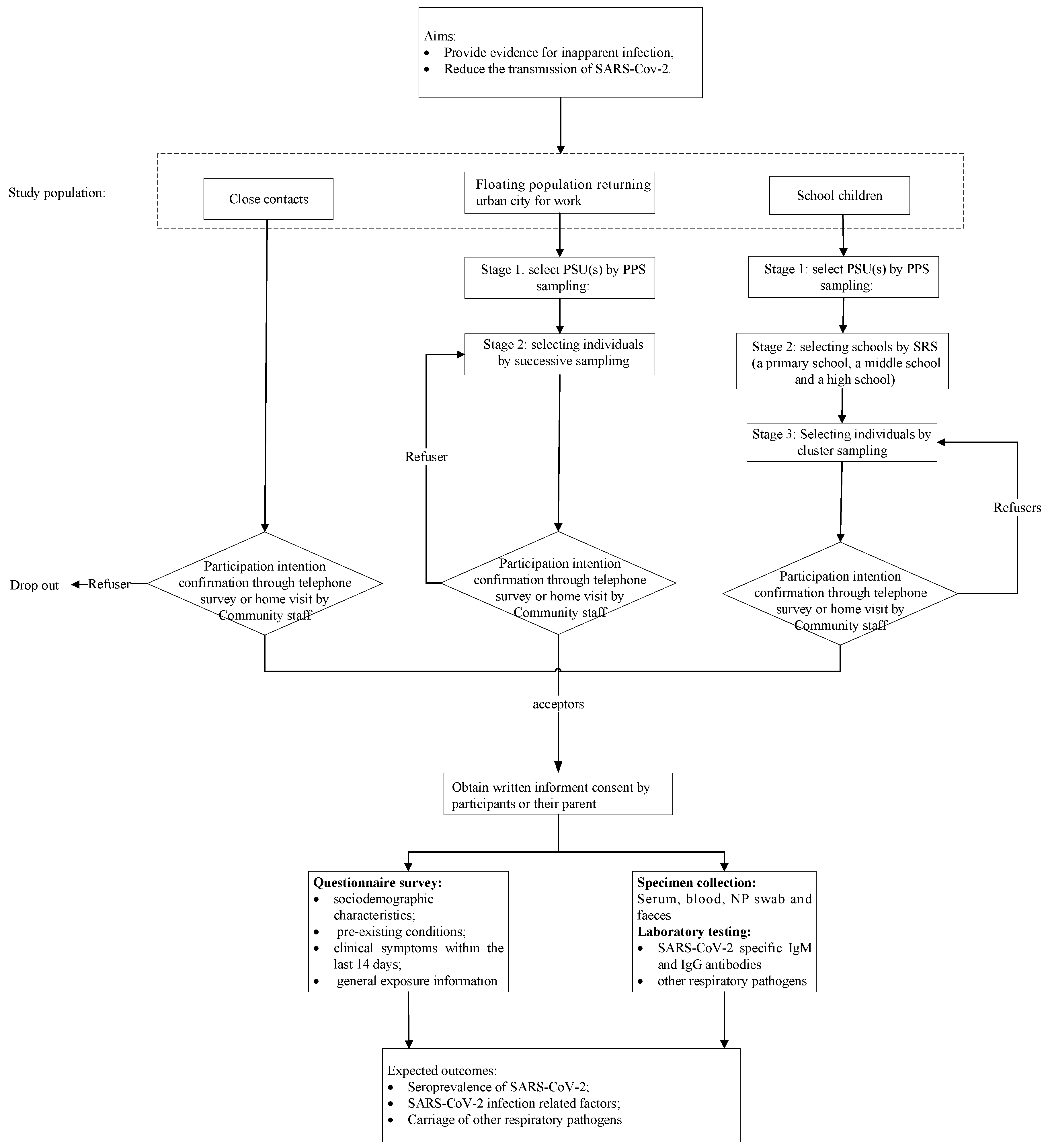
2.2. Study Objectives
2.3. Study Population
- Close contacts: The definition of “close contacts” is based on Prevention and Control of Novel Coronavirus Pneumonia (6th edition), which refers to people who had unprotected close contact (within 1 meter) with a confirmed or suspect case within two days before illness onset, or with an asymptomatic infected person within two days before sampling [10]. In China, the tracing and management of close contacts is implemented by the local Center for Disease Control and Prevention (CDC), and all identified close contacts are recorded in health administration departments.
- Volunteer to participate in the survey and provide written informed consent.
- Domestic migrant workers returning to urban areas for work:
- Aged 18 years and above;
- Unconfirmed COVID-19 cases;
- Volunteer to participate in the survey and provide signed informed consent.
- School children:
- Aged above 6 years;
- Attending primary school, middle school, or high school (non-vocational high school);
- Unconfirmed COVID-19 cases;
- Volunteer to participate in the survey and provide signed informed consent themselves and/or through their parent(s).
- Exclusion Criteria
- History of any neurologic disorders;
- Language disorders.
2.4. Study Design
2.5. Sample Size
2.6. Sampling Strategies and Study Sites
2.7. Questionnaire
- Sociodemographic characteristics: name, telephone (mobile) number, date of birth, sex, e-mail address, current address, ethnicity, job, educational level, parent employment status, educational level (only for children) and preferred mode of contact (telephone, email, or express delivery);
- Underlying conditions: pregnancy, obesity, cancer, diabetes, hypertension, heart disease, asthma requiring medication, chronic lung disease (non-asthma), chronic liver disease, chronic hematological disorder, chronic kidney disease, chronic neurological impairment/disease, and other underlying conditions. In addition, respiratory-pathogen-related vaccinations will be reviewed.
- Clinical symptoms within the last 14 days: body temperature, fever, chill, dry cough, sore throat, runny nose, shortness of breath, nausea, vomiting, diarrhea, and other symptoms.
- General exposure information: possible contact with confirmed/suspected cases, visits to medical facilities, and travel history (including destination, transfer, and duration) within the last 14 days.
2.8. Laboratory Evaluation
- Specimen collection, transportation, and storage
- Blood specimen: A 5 mL whole-blood sample will be collected with a vacutainer with no anticoagulant. Once the blood is drawn, the vacutainer should be inverted 5 or 6 times and placed at room temperature. When the blood specimen is sent to the laboratory, the vacutainer will be centrifuged for 10 min at 1500–2000 rpm at room temperature. Serum will be extracted by pipette and stored in a sterile spiral plastic tube.
- Nasopharyngeal (NP) swab: Two NP swabs will be collected for each eligible participant. The swab will be directly put in the nose parallel to the base of the NP passage. The swab should move without resistance until reaching the nasopharynx, located about one-half to two-thirds the distance from the nostril to an ear lobe. If resistance occurs, the swab will be removed, and an attempt will be made to take the sample entering through the same or the other nostril. Once the swab reaches nasopharynx, the swab will be rotated 180°, or left in place for 5 s to saturate the swab tip; and then the swab will be removed slowly. Then the swab head will be inserted into the tube containing 3.5 mL of virus preservation buffer (Virus Transport Medium (containing Hank’s balanced salt solution, polymyxin B, vancomycin, bovine serum albumin, cryoprotectant, biobuffer, etc.), Shanghai Comagal Microbial technology CO. LTD.) and swab shaft will be evenly broken at the scored line to fit in tube and replace cap tightly.
- Feces or anal swab: 3–5 mL of stool that has not been mixed with urine will be collected in a clean, dry, leak-proof container. If it is not convenient to collect fecal samples, an anal swab can be collected. The disinfectant cotton swab will be gently inserted into the anus to a depth of 3–5 cm, then it will be gently rotated pulled out, and immediately put into a 15 mL screw-capped sampling tube containing 3–5 mL virus preservation buffer. Then, the swab shaft will be evenly broken at the scored line to fit in tube and the cap will be replaced tightly.
- 2.
- Laboratory examinations
- Serological testing: The serum specimen will be available for qualitative detection of SARS-CoV-2-specific total antibodies (including IgM, IgG, IgA, and other antibody types) with Novel Coronavirus (2019-nCoV) Antibody Test Kit (chemiluminescence immunoassay method) (registered number: 20203400198), developed by Xiamen InnoDx Biotech Co., Ltd. (Xiamen, China) and which is the world’s first approved total antibody detection reagent with the double-antigen sandwich method for SARS-CoV-2. It can rapidly and simply detect specific antibodies within 29 min.
- Etiological testing: A real-time fluorescence-based reverse transcriptase-polymerase chain reaction (RT-PCR) assay will be applied to the NP specimen and feces to detect SARS-CoV-2. The primers and probes (targeting open reading frame 1ab (ORF 1ab) and nucleocapsid protein (N) in the novel coronavirus genome) used for SARS-CoV-2 detection by RT-PCR is from the Novel Coronavirus Pneumonia: Laboratory Testing Guideline, released by National Health Commission of the PRC. In addition, NP specimens will be further examined for a total of 41 respiratory pathogens (Table 4) via gene chips (Micro-Fluid Chip for Respiratory Pathogens, product number: 4398986).
2.9. Study Procedure
2.10. Data Analysis Plan
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Novel Coronavirus (2019-nCoV): Situation Report, 22. 2020; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.; Lau, E.H.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission of the People ’s Republic of China. Announcement by the National Health Commission. 20 January 2020. Available online: http://www.nhc.gov.cn/xcs/zhengcwj/202001/44a3b8245e8049d2837a4f27529cd386.shtml (accessed on 20 January 2020).
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020, 295, 200463. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Tang, J.; Wei, F. Updated understanding of the outbreak of 2019 novel coronavirus (2019-nCoV) in Wuhan, China. J. Med. Virol. 2020, 92, 441–447. [Google Scholar] [CrossRef] [PubMed]
- The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID-19)—China, 2020. China CDC Wkly. 2020, 2, 113–122. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. The Latest Status of 2019-Novel-Coronavirus (2019-nCoV) Pneumonia at 24 o’ clock, 31 July. 1 August 2020. Available online: http://www.nhc.gov.cn/xcs/yqtb/202008/96184996b6724df787ea9380dfdc88bf.shtml (accessed on 1 August 2020).
- Hu, Z.; Song, C.; Xu, C.; Jin, G.; Chen, Y.; Xu, X.; Ma, H.; Chen, W.; Lin, Y.; Zheng, Y.; et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. China Life Sci. 2020, 63, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Yu, P.; Zhu, J.; Zhang, Z.; Han, Y.; Huang, L. A Familial Cluster of Infection Associated With the 2019 Novel Coronavirus Indicating Possible Person-to-Person Transmission During the Incubation Period. J. Infect. Dis. 2020, 221, 1757–1761. [Google Scholar] [CrossRef] [PubMed]
- National Health Commission of the People’ s Republic of China. Protocol on Prevention and Control of Novel Coronavirus Pneumonia (Edition 6). 7 March 2020. Available online: http://www.nhc.gov.cn/jkj/s3577/202003/4856d5b0458141fa9f376853224d41d7/files/4132bf035bc242478a6eaf157eb0d979.pdf (accessed on 1 April 2020).
- Zhan, S. Epidemiolgy, 7th ed.; People’ s Medical Publishing House: Beijing, China, 2013. [Google Scholar]
- Leung, G.M.; Chung, P.-H.; Tsang, T.; Lim, W.; Chan, S.K.; Chau, P.; Donnelly, C.A.; Ghani, A.C.; Fraser, C.; Riley, S.; et al. SARS-CoV Antibody Prevalence in All Hong Kong Patient Contacts. Emerg. Infect. Dis. 2004, 10, 1653–1656. [Google Scholar] [CrossRef] [PubMed]
- Leung, G.M.; Lim, W.W.; Ho, L.-M.; Lam, T.-H.; Ghani, A.C.; Donnelly, C.A.; Fraser, C.; Riley, S.; Ferguson, N.M.; Anderson, R.M.; et al. Seroprevalence of IgG antibodies to SARS-coronavirus in asymptomatic or subclinical population groups. Epidemiol. Infect. 2005, 134, 211–221. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Leung, C.; Kwan, Y.-W.; Ko, P.-W.; Chiu, S.S.; Loung, P.-Y.; Fong, N.-C.; Lee, L.-P.; Hui, Y.-W.; Law, H.K.W.; Wong, W.H.-S.; et al. Severe Acute Respiratory Syndrome Among Children. Pediatrics 2004, 113, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Xuan, R.; Chen, L.; Sun, X.; Liu, X.; Liu, L.; Lin, Y.; Deng, Y.; Luo, W.; Huang, J.; Qiu, W.; et al. Epidemiological research on SARS coronavirus antibody in serum among healthy population of Qingyuan City[J]. Occup. Health 2005. Available online: http://med.wanfangdata.com.cn/Paper/Detail?id=PeriodicalPaper_zyyjk200501002&dbid=WF_QK (accessed on 2 October 2020).
- Zhao, G.; Zhao, B.; Deng, X.; Zhao, Q.; He, N.; He, J.; Wang, J.; Liu, L.; Jiang, Q. Seroepidemiological study on severe respiratory syndrome among different population in Taiyuan[J]. Chin. J. Public Health 2005, 21, 518–519. [Google Scholar]
- Shanghai Education Bureau. Statistics of Education in 2018. October 2019. Available online: http://edu.sh.gov.cn/html/xxgk/rows.list.30317.html (accessed on 10 March 2020).


{kind=link}
| District | Size of Confirmed Cases | Cumulative Sum of Confirmed Cases | Clusters Sampled |
|---|---|---|---|
| Pudong | 60 | 60 | 26 |
| Huangpu | 6 | 66 | |
| Xuhui | 18 | 84 | 83 |
| Changning | 13 | 97 | |
| Jing’an | 16 | 113 | |
| Putuo | 11 | 124 | |
| Hongkou | 7 | 131 | |
| Yangpu | 9 | 140 | 139 |
| Minhang | 19 | 159 | |
| Baoshan | 21 | 180 | |
| Jiading | 9 | 189 | |
| Jinshan | 4 | 193 | |
| Songjiang | 14 | 207 | 196 |
| Qingpu | 6 | 213 | |
| Fengxian | 9 | 222 | |
| Chongming | 4 | 226 |
| District | Size of Floating Population (Thousand) | Cumulative Sum of Floating Population (Thousand) | Clusters Sampled (Thousand) | Individuals per District |
|---|---|---|---|---|
| Pudong | 2350.90 | 2350.90 | 1125.44 | 863 |
| Huangpu | 166.30 | 2517.20 | ||
| Xuhui | 269.80 | 2787.00 | ||
| Changning | 174.80 | 2961.80 | ||
| Jing’an | 266.80 | 3228.60 | ||
| Putuo | 338.00 | 3566.60 | 3557.13 | 863 |
| Hongkou | 153.70 | 3720.30 | ||
| Yangpu | 268.60 | 3988.90 | ||
| Minhang | 1245.90 | 5234.80 | ||
| Baoshan | 834.70 | 6069.50 | 5988.83 | 863 |
| Jiading | 899.00 | 6968.50 | ||
| Jinshan | 270.00 | 7238.50 | ||
| Songjiang | 1059.51 | 8298.01 | ||
| Qingpu | 707.50 | 9005.51 | 8420.53 | 863 |
| Fengxian | 579.41 | 9584.93 | ||
| Chongming | 141.87 | 9726.79 |
| District | Size of School | Cumulative Sum of School | Clusters Sampled | Individuals per District |
|---|---|---|---|---|
| Pudong | 395 | 395 | 220 | 1960 |
| Huangpu | 76 | 471 | ||
| Xuhui | 98 | 569 | ||
| Changning | 59 | 628 | ||
| Jing’an | 115 | 743 | 696 | 1960 |
| Putuo | 105 | 848 | ||
| Hongkou | 80 | 928 | ||
| Yangpu | 107 | 1035 | ||
| Minhang | 171 | 1206 | 1172 | 1960 |
| Baoshan | 170 | 1376 | ||
| Jiading | 103 | 1479 | ||
| Jinshan | 70 | 1549 | ||
| Songjiang | 112 | 1661 | 1648 | 1960 |
| Qingpu | 71 | 1732 | ||
| Fengxian | 97 | 1829 | ||
| Chongming | 74 | 1903 |
| Pathogen | Pathogen | Pathogen |
|---|---|---|
| Adenovirus | Influenza A virus H3 (Flu-A_H3) | Rhinovirus (A, B, C) |
| Bocavirus | Influenza A virus_H1-2009 (Flu-A_H1-2009) | Streptococcus pyogenes |
| Cytomegalovirus | Influenza B virus (Flu-B) | Streptococcus pneumoniae |
| Coronavirus_229E | MERS-CoV | Bordetella_pan |
| Coronavirus_NL63 | Human Metapneumovirus 1 (hMPV-1) | Bordetella pertussis |
| Coronavirus_OC43 | Human Metapneumovirus 2 (hMPV-2) | Bordetella holmesii |
| Coronavirus_HKU-1 | Varicella-zoster virus -2 | Chlamydia pneumoniae |
| Enterovirus | Parechovirus | Coxiella burnetii |
| Epstein-Barr virus (EBV) | ParaInfuenza-1 | Legionella pneumophila |
| Herpes Simplex virus 1 (HSV-1) | ParaInfuenza-2 | Mycoplasma pneumoniae |
| Herpes Simplex virus 2 (HSV-2) | ParaInfuenza-3 | Moraxella catarrhalis |
| Human herpesvirus 6 (HHV-6) | ParaInfuenza-4 | Mumps |
| SARS-CoV | Respiratory Syncytial Viral A (RSV-A) | Measles virus |
| Influenza A virus (Flu-A) | Respiratory Syncytial Viral B (RSV-B) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, S.-F.; Lu, Y.-H.; Zhang, T.; Xiong, H.-Y.; Wang, W.-B. Cross-Sectional Seroepidemiologic Study of Coronavirus Disease 2019 (COVID-19) among Close Contacts, Children, and Migrant Workers in Shanghai. Int. J. Environ. Res. Public Health 2020, 17, 7223. https://doi.org/10.3390/ijerph17197223
Xu S-F, Lu Y-H, Zhang T, Xiong H-Y, Wang W-B. Cross-Sectional Seroepidemiologic Study of Coronavirus Disease 2019 (COVID-19) among Close Contacts, Children, and Migrant Workers in Shanghai. International Journal of Environmental Research and Public Health. 2020; 17(19):7223. https://doi.org/10.3390/ijerph17197223
Chicago/Turabian StyleXu, Shuang-Fei, Yi-Han Lu, Tao Zhang, Hai-Yan Xiong, and Wei-Bing Wang. 2020. "Cross-Sectional Seroepidemiologic Study of Coronavirus Disease 2019 (COVID-19) among Close Contacts, Children, and Migrant Workers in Shanghai" International Journal of Environmental Research and Public Health 17, no. 19: 7223. https://doi.org/10.3390/ijerph17197223
APA StyleXu, S.-F., Lu, Y.-H., Zhang, T., Xiong, H.-Y., & Wang, W.-B. (2020). Cross-Sectional Seroepidemiologic Study of Coronavirus Disease 2019 (COVID-19) among Close Contacts, Children, and Migrant Workers in Shanghai. International Journal of Environmental Research and Public Health, 17(19), 7223. https://doi.org/10.3390/ijerph17197223